


Twelve-Week Safety and Potential Lipid Control Efficacy of Coffee Cherry Pulp Juice Concentrate in Healthy Volunteers


Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Aspects and Setting
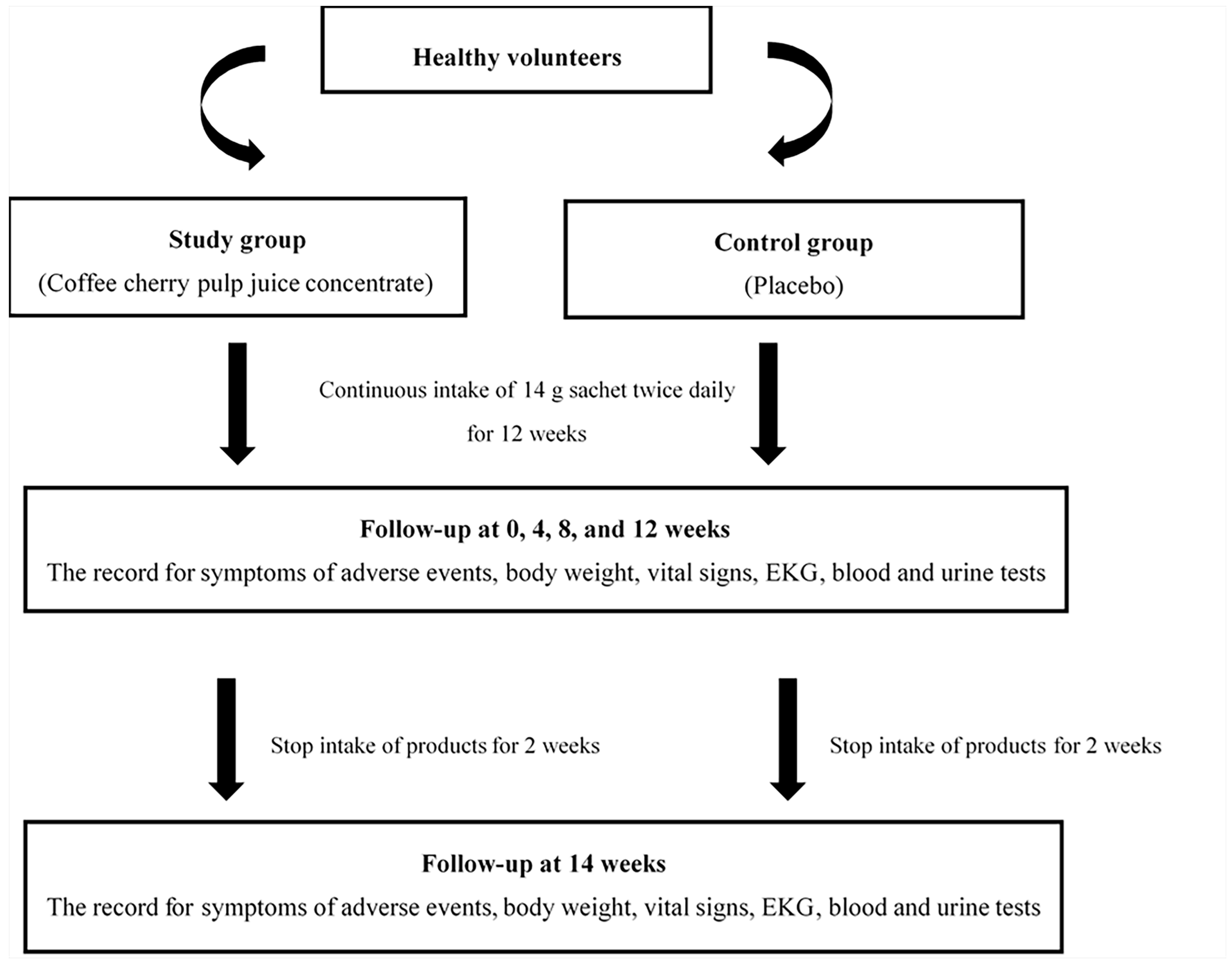
2.2. Study Design, Blinding, Random Allocation, and Concealment
2.3. Participants
2.4. Sample Size and Power
2.5. Intervention and Materials
2.6. Study Procedure
2.7. Outcome Measurement
2.8. Statistical Analysis
3. Results
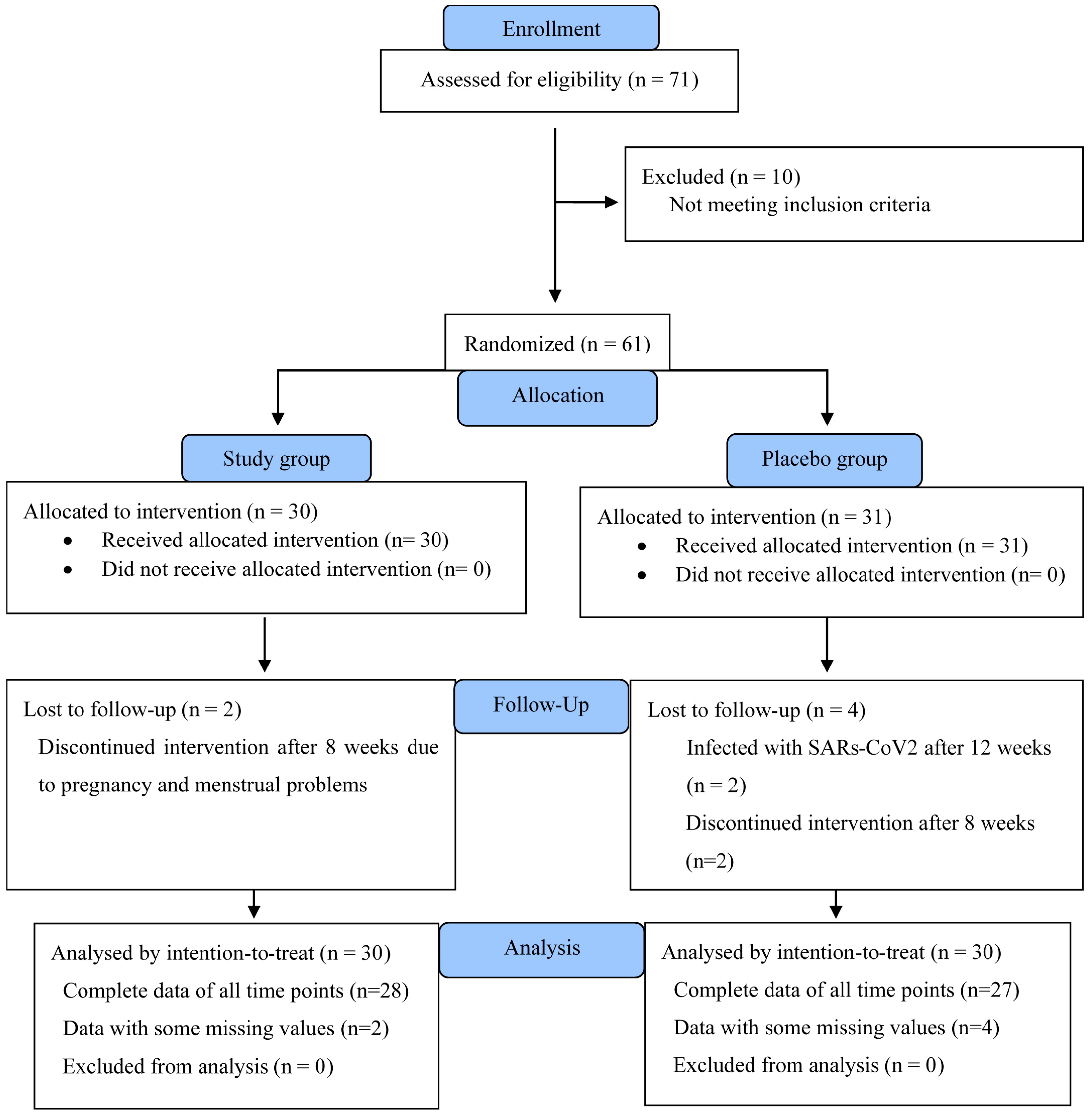
3.1. Participant Flow Chart
3.2. Baseline Demographic, Clinical Chemistry, and Hematology Characteristics of the Participants
3.3. Adverse Symptoms
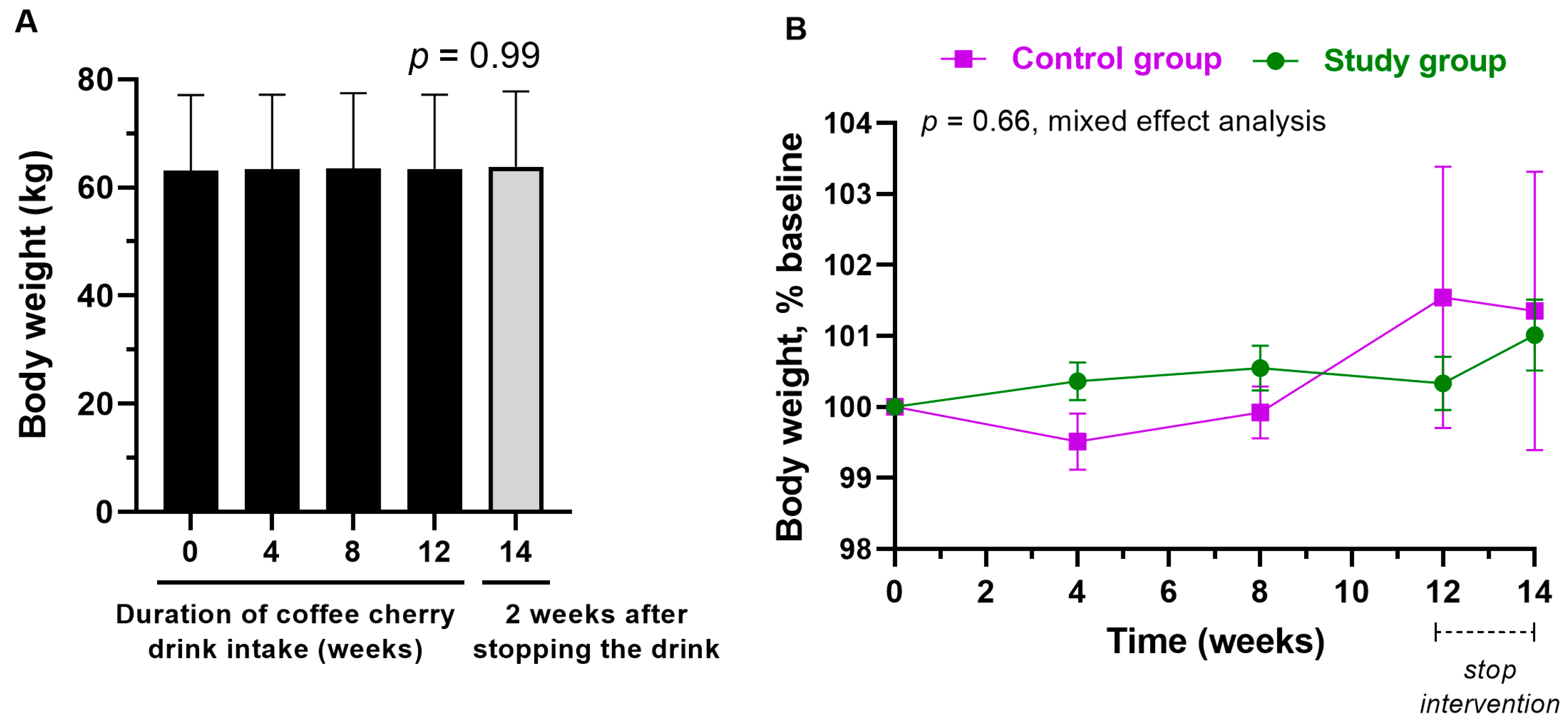
3.4. Changes in Body Weight
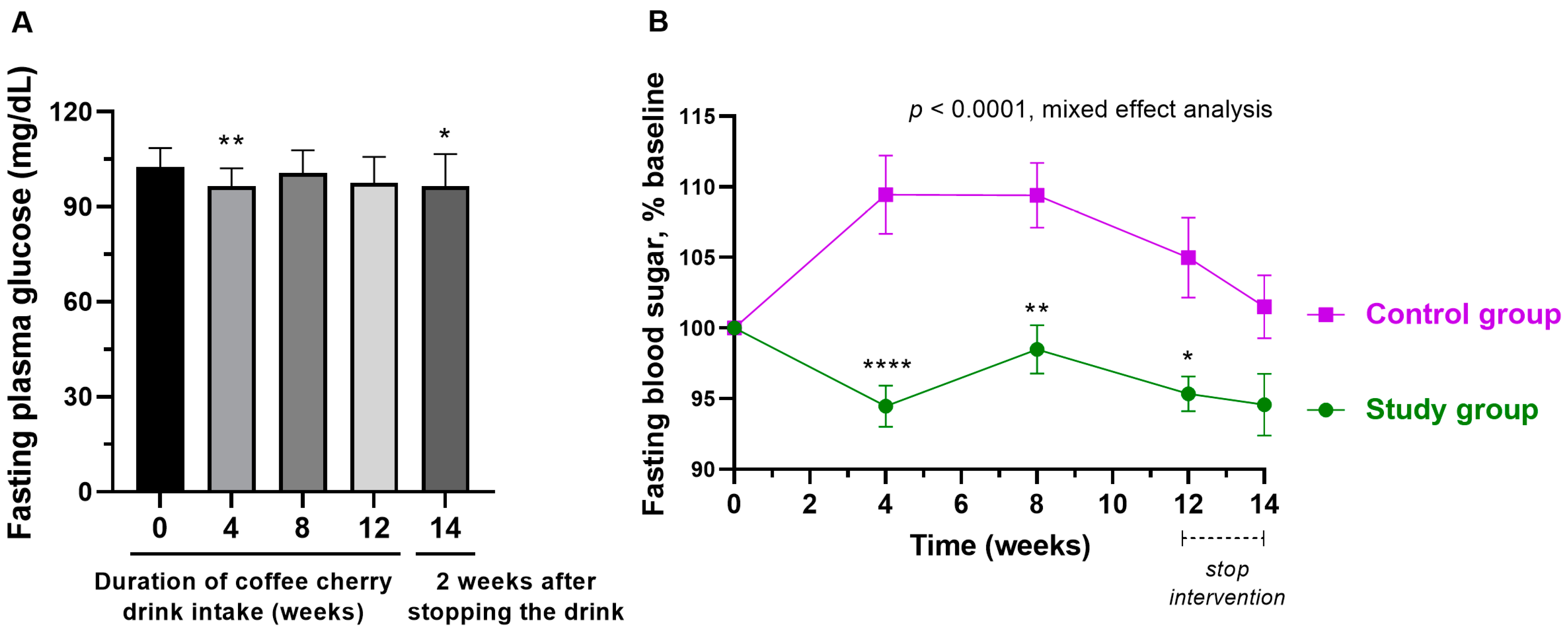
3.5. Changes in Fasting Plasma Glucose
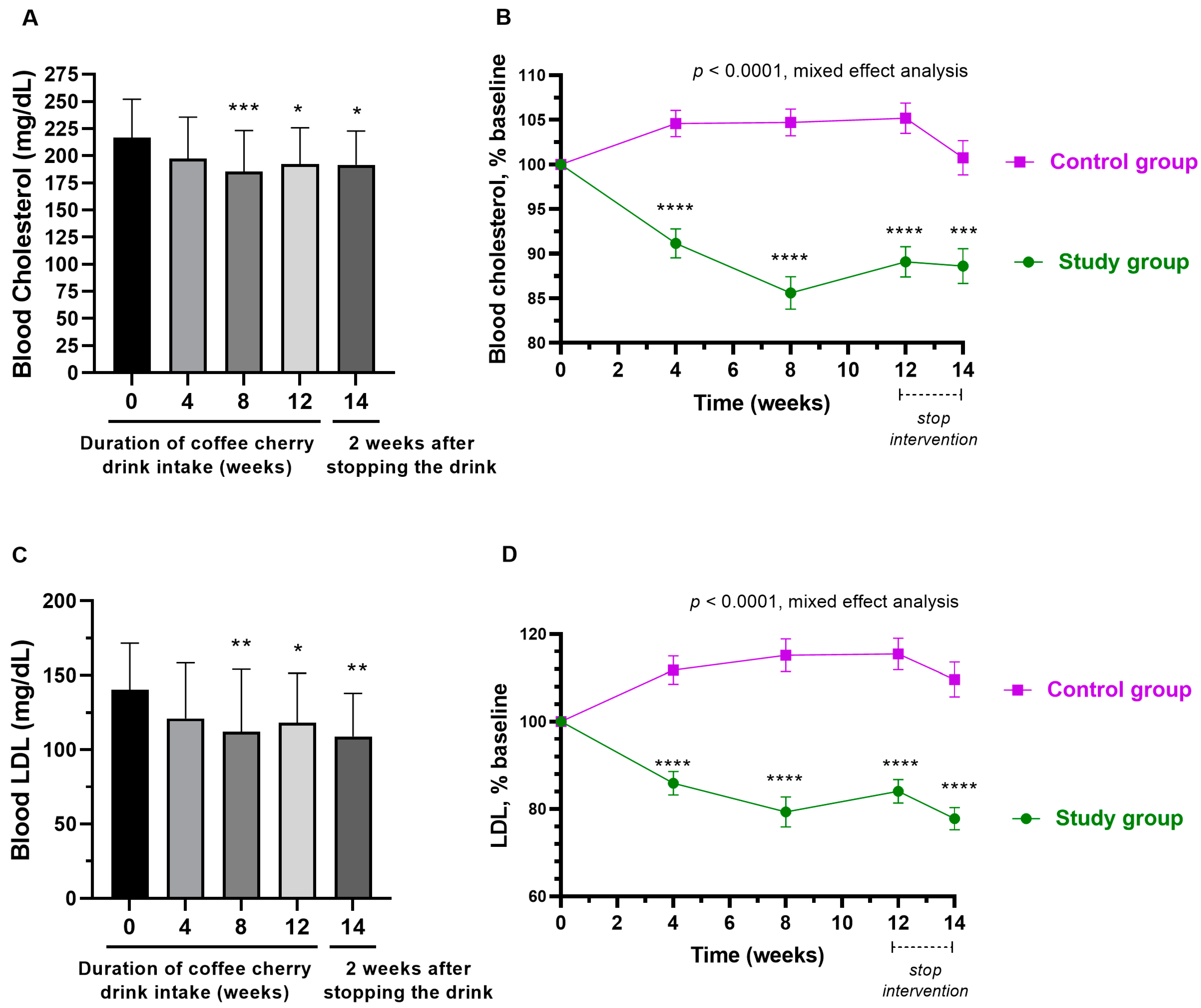
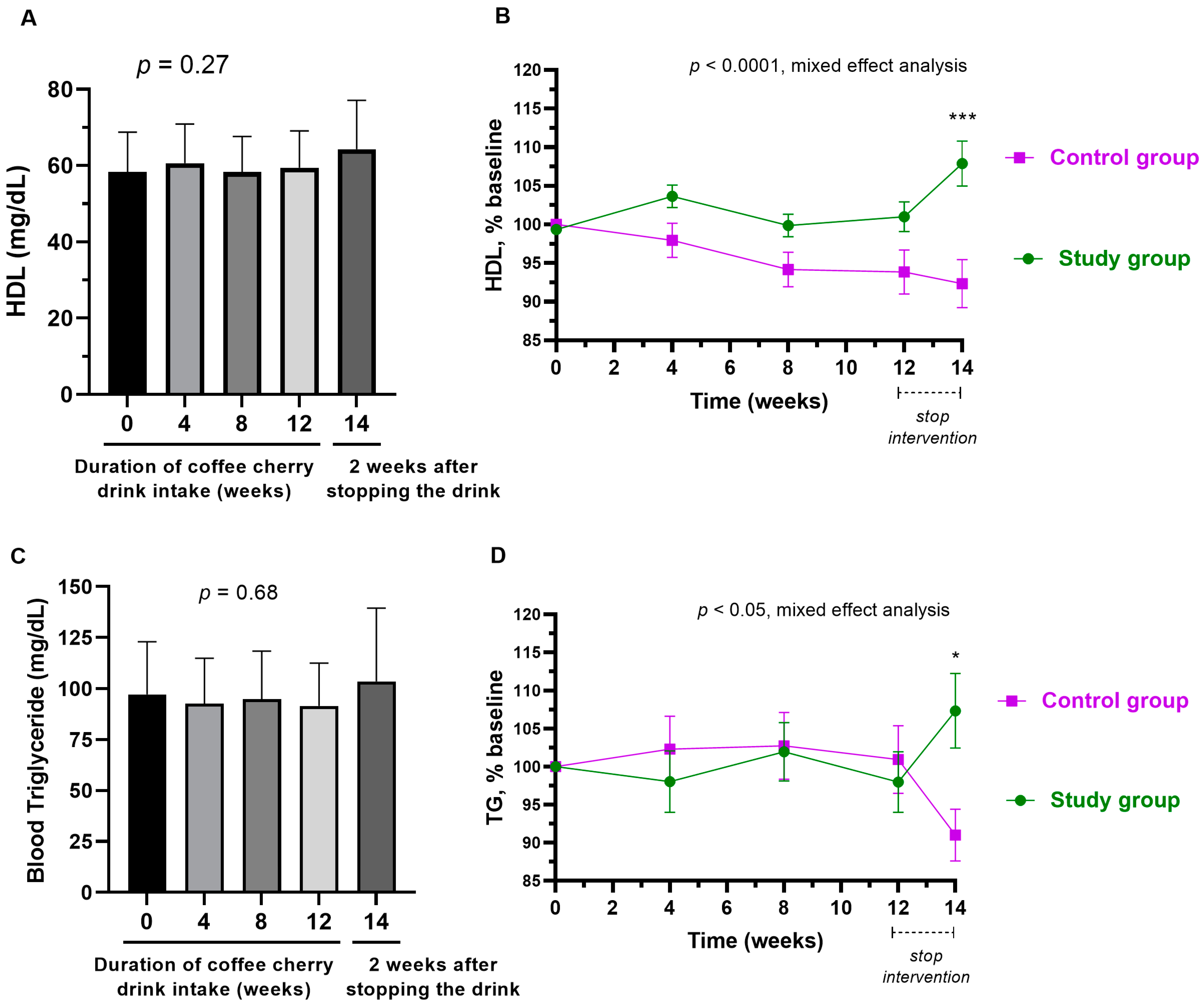
3.6. Changes in Blood Lipid Profile
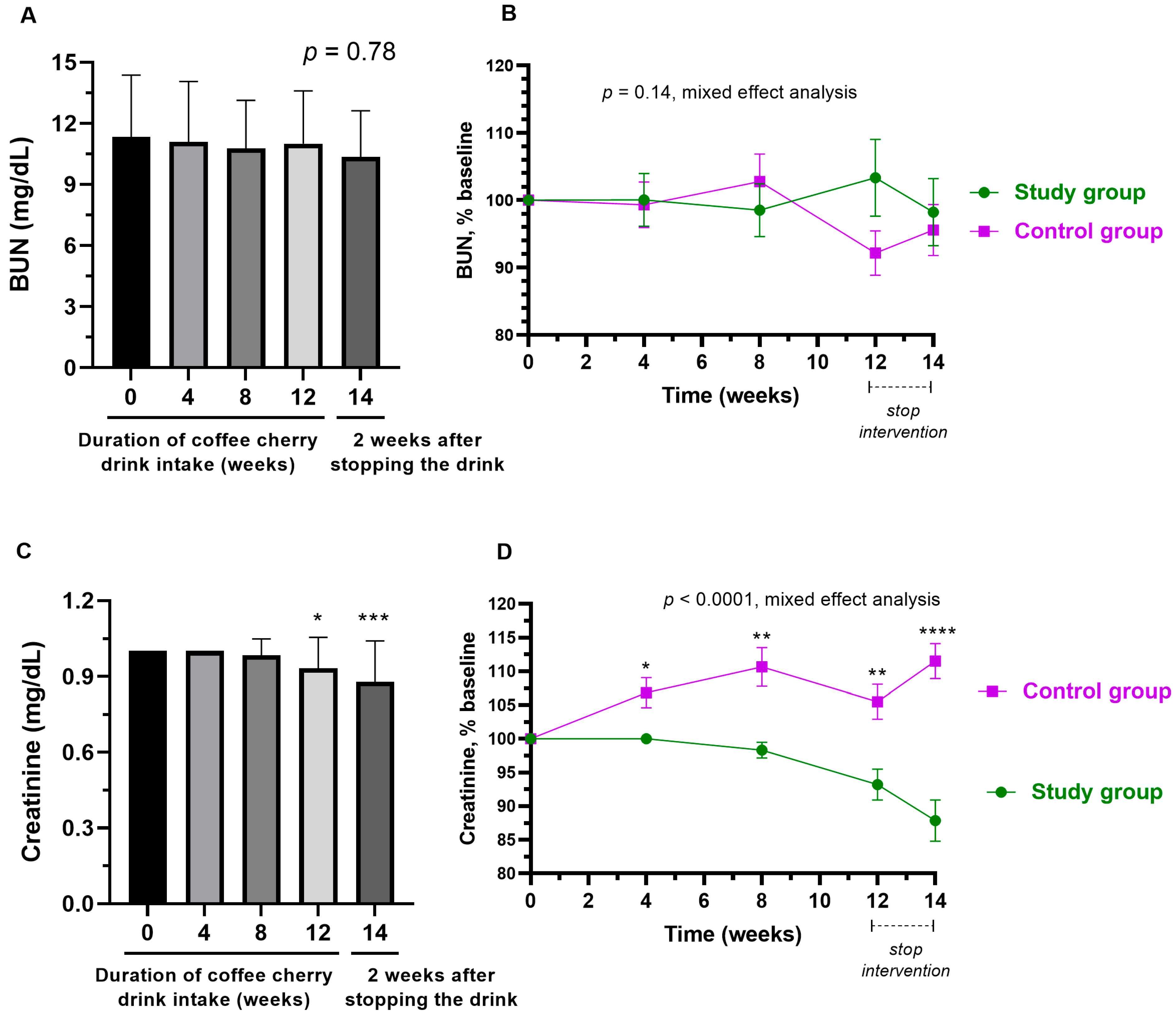
3.7. Changes in Kidney Function
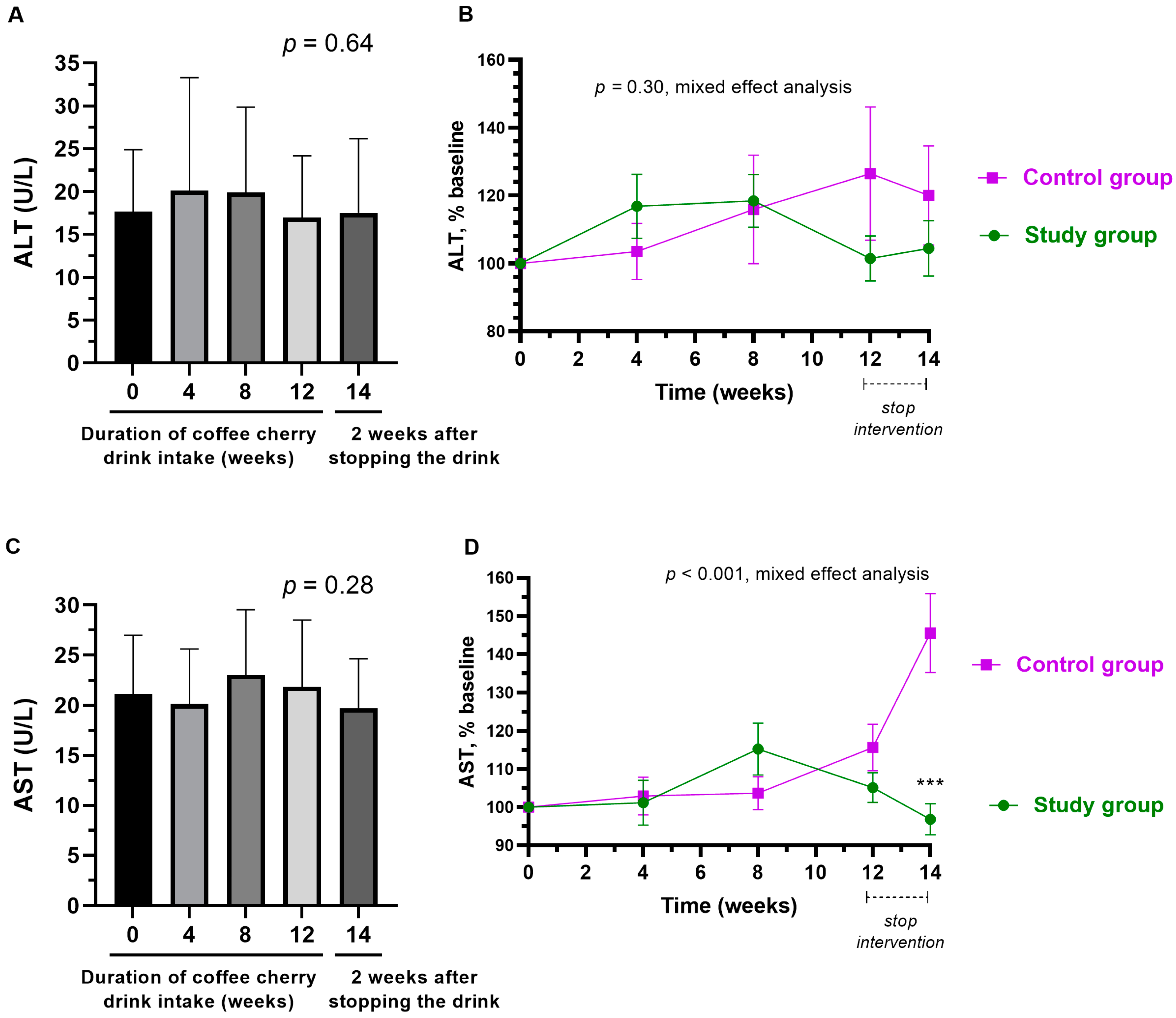
3.8. Changes in Liver Enzymes
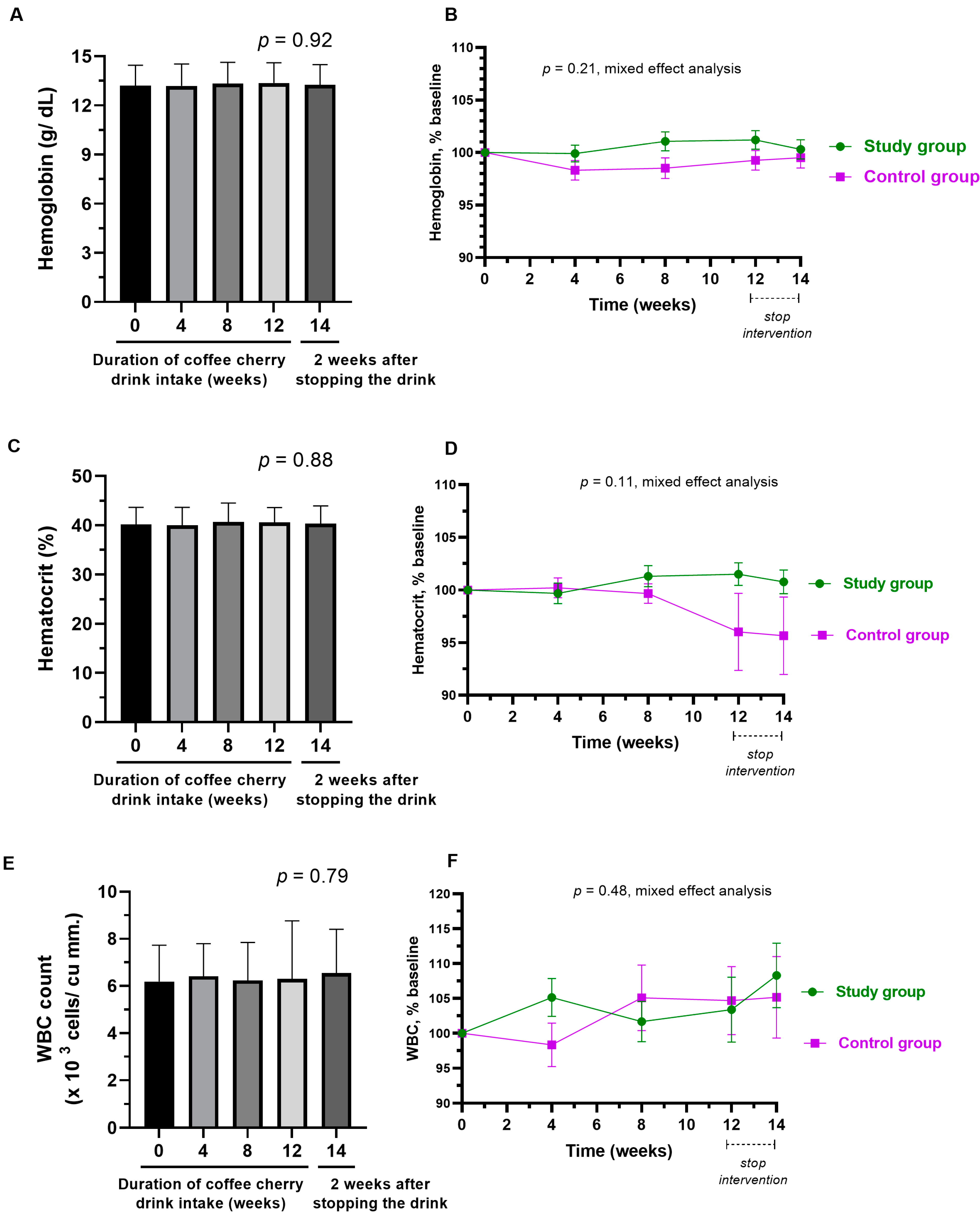
3.9. Changes in Hematological Parameter
3.10. Changes in Urinalysis
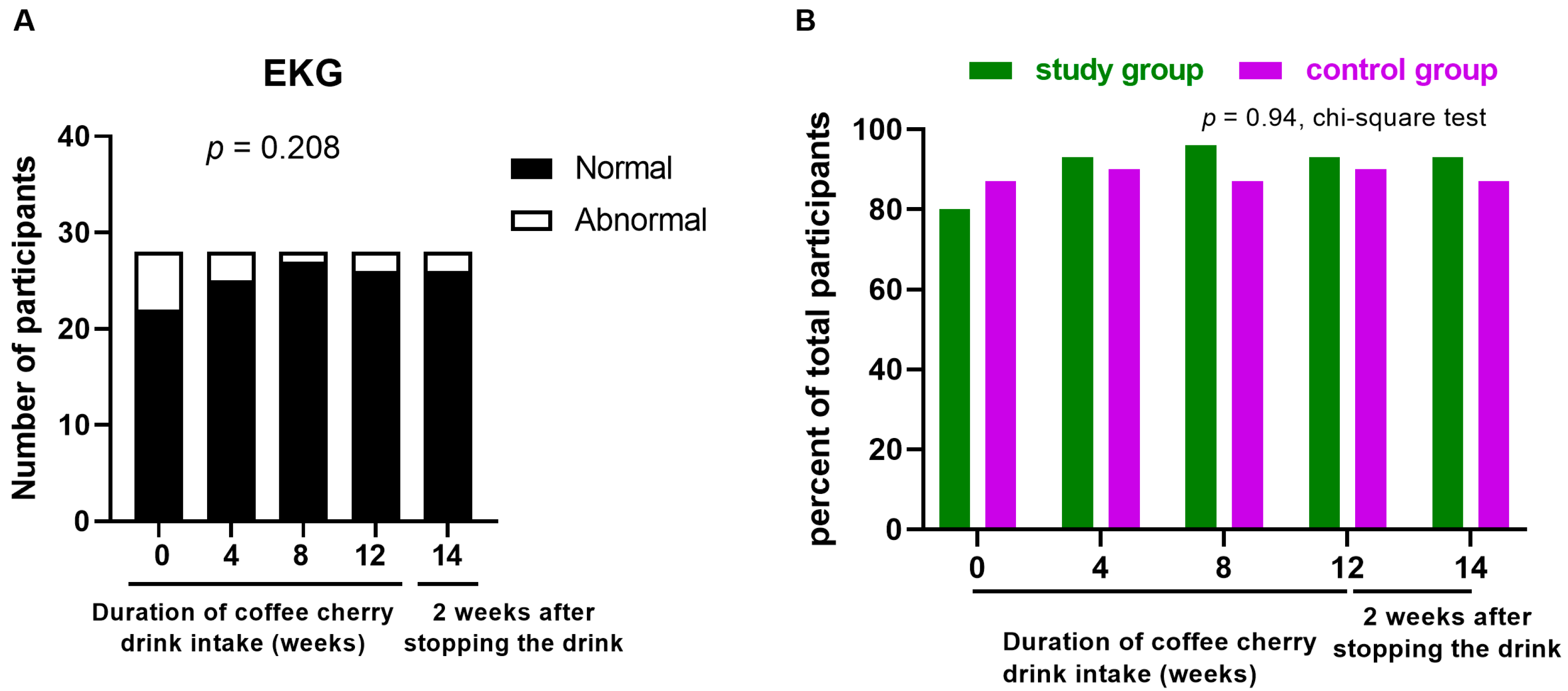
3.11. Changes in EKG
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Murthy, P.S.; Naidu, M.M. Sustainable management of coffee industry by-products and value addition—A review. Resour. Conserv. Recycl. 2012, 66, 45–58. [Google Scholar] [CrossRef]
- Blinová, L.; Sirotiak, M.; Bartošová, A.; Soldán, M. Review: Utilization of Waste from Coffee Production. Research Papers; Faculty of Materials Science and Technology Slovak University of Technology: Bratislava, Slovakia, 2017; Volume 25, pp. 91–101. [Google Scholar]
- Ramirez-Martinez, J.R. Phenolic compounds in coffee pulp: Quantitative determination by HPLC. J. Sci. Food Agric. 1988, 43, 135–144. [Google Scholar] [CrossRef]
- Ontawong, A.; Pasachan, T.; Trisuwan, K.; Soodvilai, S.; Duangjai, A.; Pongchaidecha, A.; Amornlerdpison, D.; Srimaroeng, C. Coffea arabica pulp aqueous extract attenuates oxidative stress and hepatic lipid accumulation in HepG2 cells. J. Herb. Med. 2021, 29, 100465. [Google Scholar] [CrossRef]
- Ameca, G.M.; Cerrilla, M.E.O.; Córdoba, P.Z.; Cruz, A.D.; Hernández, M.S.; Haro, J.H. Chemical composition and antioxidant capacity of coffee pulp. Ciênc. Agrotec. 2018, 42, 307–313. [Google Scholar] [CrossRef]
- Magoni, C.; Bruni, I.; Guzzetti, L.; Dell’Agli, M.; Sangiovanni, E.; Piazza, S.; Regonesi, M.E.; Maldini, M.; Spezzano, R.; Caruso, D.; et al. Valorizing coffee pulp by-products as anti-inflammatory ingredient of food supplements acting on IL-8 release. Food Res. Int. 2018, 112, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Ontawong, A.; Duangjai, A.; Muanprasat, C.; Pasachan, T.; Pongchaidecha, A.; Amornlerdpison, D.; Srimaroeng, C. Lipid-lowering effects of Coffea arabica pulp aqueous extract in Caco-2 cells and hypercholesterolemic rats. Phytomedicine 2019, 52, 187–197. [Google Scholar] [CrossRef] [PubMed]
- Ontawong, A.; Boonphang, O.; Pasachan, T.; Duangjai, A.; Pongchaidecha, A.; Phatsara, M.; Jinakote, M.; Amornlerdpison, D.; Srimaroeng, C. Hepatoprotective effect of coffee pulp aqueous extract combined with simvastatin against hepatic steatosis in high-fat diet-induced obese rats. J. Funct. Foods 2019, 54, 568–577. [Google Scholar] [CrossRef]
- Robinson, J.L.; Hunter, J.M.; Reyes-Izquierdo, T.; Argumedo, R.; Brizuela-Bastien, J.; Keller, R.; Pietrzkowski, Z.J. Cognitive short- and long-term effects of coffee cherry extract in older adults with mild cognitive decline. Aging Neuropsychol. Cogn. 2019, 27, 918–934. [Google Scholar] [CrossRef]
- European Union. Commission Implementing Regulation (EU) 2017/2469 of 20 December 2017 Laying Down Administrative and Scientific Requirements for Applications Referred to in Article 10 of Regulation (EU) 2015/2283 of the European Parliament and of the Council on Novel Foods. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX%3A32017R2469 (accessed on 28 February 2023).
- Ministry of Public Health, Thailand. Ministry of Public Health Notification No. 376 B.E. 2559 Re: Novel Food. 2017. Available online: https://food.fda.moph.go.th/law/data/announ_moph/V.English/No.376_Re_Novel_food.pdf (accessed on 28 February 2023).
- Heimbach, J.; Marone, P.; Hunter, J.; Nemzer, B.; Stanley, S.; Kennepohl, E. Safety studies on products from whole coffee fruit. Food Chem. Toxicol. 2010, 48, 2517–2525. [Google Scholar] [CrossRef]
- Generally Recognized as Safe (GRAS). Notices GRN No.868 Coffee Fruit Extract. Available online: https://www.fda.gov/media/135526/download (accessed on 28 February 2023).
- Ostojic, S.M.; Stojanovic, M.D.; Djordjevic, B.; Jourkesh, M.; Vasiljevic, N. The effects of a 4-week coffeeberry supplementation on antioxidant status, endurance, and anaerobic performance in college athletes. Res. Sport. Med. 2008, 16, 281–294. [Google Scholar] [CrossRef]
- Klingel, T.; Kremer, J.I.; Gottstein, V.; De Rezende, T.R.; Schwarz, S.; Lachenmeier, D.W. A Review of Coffee By-Products Including Leaf, Flower, Cherry, Husk, Silver Skin, and Spent Grounds as Novel Foods within the European Union. Foods 2020, 9, 665. [Google Scholar] [CrossRef]
- Carmen, M.-T.; Lorena, Z.-C.; Alexander, V.-A.; Amandio, V.; Raúl, S. Coffee Pulp: An Industrial By-product with Uses in Agriculture, Nutrition and Biotechnology. Rev. Agric. Sci. 2020, 8, 323–342. [Google Scholar] [CrossRef] [PubMed]
- Rolz, C.; Menchú, J.F.; Arriola, M.D.C.D.; de Micheo, F. Pressing of coffee pulp. Agric. Wastes 1980, 2, 207–214. [Google Scholar] [CrossRef]
- Rungraung, N.; Muangpracha, N.; Trachootham, D. A Dose-Escalation Study for Identifying Safe Doses of Coffee Cherry Pulp Juice Concentrate in Healthy Subjects. Thai J. Toxicol. 2022, 37, 57–78. [Google Scholar]
- Zhou, D.; Liu, X.; Lo, K.; Huang, Y.; Feng, Y. The effect of total cholesterol/high-density lipoprotein cholesterol ratio on mortality risk in the general population. Front. Endocrinol. 2022, 13, 1012383. [Google Scholar] [CrossRef]
- He, G.-D.; Liu, X.-C.; Liu, L.; Yu, Y.-L.; Chen, C.-L.; Huang, J.-Y.; Lo, K.; Huang, Y.-Q.; Feng, Y.-Q. A nonlinear association of total cholesterol with all-cause and cause-specific mortality. Nutr. Metab. 2021, 18, 25. [Google Scholar] [CrossRef]
- Kang, H. Sample size determination and power analysis using the G*Power software. J. Educ. Eval. Health Prof. 2021, 18, 17. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Public Health, Thailand. Ministry of Public Health Notification No. 355 B.E. 2556 Regarding to the Food in a Hermetically Sealed Container. 2013. Available online: https://food.fda.moph.go.th/law/data/announ_moph/V.English/P355_E.pdf (accessed on 8 February 2023).
- Lau, K.Q.; Sabran, M.R.; Shafie, S.R. Utilization of Vegetable and Fruit by-products as Functional Ingredient and Food. Front. Nutr. 2021, 8, 661693. [Google Scholar] [CrossRef]
- Zarbà, C.; Chinnici, G.; Hamam, M.; Bracco, S.; Pecorino, B.; D’Amico, M. Driving Management of Novel Foods: A Network Analysis Approach. Front. Sustain. Food Syst. 2022, 5, 531. [Google Scholar] [CrossRef]
- Ramirez-Coronel, M.A.; Marnet, N.; Kolli, V.K.; Roussos, S.; Guyot, S.; Augur, C. Characterization and estimation of proanthocyanidins and other phenolics in coffee pulp (Coffea arabica) by thiolysis—high-performance liquid chromatography. J. Agric. Food Chem. 2004, 52, 1344–1349. [Google Scholar] [CrossRef]
- Heeger, A.; Kosińska-Cagnazzo, A.; Cantergiani, E.; Andlauer, W. Bioactives of coffee cherry pulp and its utilisation for production of Cascara beverage. Food Chem. 2017, 221, 969–975. [Google Scholar] [CrossRef] [PubMed]
- Eckhardt, S.; Franke, H.; Schwarz, S.; Lachenmeier, D.W. Risk Assessment of Coffee Cherry (Cascara) Fruit Products for Flour Replacement and Other Alternative Food Uses. Molecules 2022, 27, 8435. [Google Scholar] [CrossRef]
- Su, X.; Cheng, Y.; Zhang, G.; Wang, B. Novel insights into the pathological mechanisms of metabolic related dyslipidemia. Mol. Biol. Rep. 2021, 48, 5675–5687. [Google Scholar] [CrossRef] [PubMed]
- Su, X.; Peng, H.; Chen, X.; Wu, X.; Wang, B. Hyperlipidemia and hypothyroidism. Clin. Chim. Acta 2022, 527, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Meng, S.; Cao, J.; Feng, Q.; Peng, J.; Hu, Y. Roles of Chlorogenic Acid on Regulating Glucose and Lipids Metabolism: A Review. Evid.-Based Complement. Altern. Med. 2013, 2013, 801457. [Google Scholar] [CrossRef] [Green Version]
- Reis, C.E.; Dórea, J.G.; da Costa, T.H. Effects of coffee consumption on glucose metabolism: A systematic review of clinical trials. J. Tradit. Complement. Med. 2019, 9, 184–191. [Google Scholar] [CrossRef]
- Bhandarkar, N.S.; Mouatt, P.; Majzoub, M.E.; Thomas, T.; Brown, L.; Panchal, S.K. Coffee Pulp, a By-Product of Coffee Production, Modulates Gut Microbiota and Improves Metabolic Syndrome in High-Carbohydrate, High-Fat Diet-Fed Rats. Pathogens 2021, 10, 1369. [Google Scholar] [CrossRef]
- Cañas, S.; Rebollo-Hernanz, M.; Braojos, C.; Benítez, V.; Ferreras-Charro, R.; Dueñas, M.; Aguilera, Y.; Martín-Cabrejas, M.A. Understanding the Gastrointestinal Behavior of the Coffee Pulp Phenolic Compounds under Simulated Conditions. Antioxidants 2022, 11, 1818. [Google Scholar] [CrossRef]
- Franczyk, B.; Gluba-Brzózka, A.; Ciałkowska-Rysz, A.; Ławiński, J.; Rysz, J. The Impact of Aerobic Exercise on HDL Quantity and Quality: A Narrative Review. Int. J. Mol. Sci. 2023, 24, 4653. [Google Scholar] [CrossRef]
- Jomard, A.; Osto, E. High Density Lipoproteins: Metabolism, Function, and Therapeutic Potential. Front. Cardiovasc. Med. 2020, 7, 39. [Google Scholar] [CrossRef]
- Qiu, C.; Zhao, X.; Zhou, Q.; Zhang, Z. High-density lipoprotein cholesterol efflux capacity is inversely associated with cardiovascular risk: A systematic review and meta-analysis. Lipids Health Dis. 2017, 16, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Kaur, N.; Pandey, A.; Negi, H.; Shafiq, N.; Reddy, S.; Kaur, H.; Chadha, N.; Malhotra, S. Effect of HDL-Raising Drugs on Cardiovascular Outcomes: A Systematic Review and Meta-Regression. PLoS ONE 2014, 9, e94585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Liu, Q.; Pan, Y.; Chen, S.; Zhao, Y.; Hu, Y. New insights into the role of dietary triglyceride absorption in obesity and metabolic diseases. Front. Pharmacol. 2023, 14, 1097835. [Google Scholar] [CrossRef]
- Jana, S.; Mitra, P.; Roy, S. Proficient Novel Biomarkers Guide Early Detection of Acute Kidney Injury: A Review. Diseases 2022, 11, 8. [Google Scholar] [CrossRef] [PubMed]
- McGill, M.R. The past and present of serum aminotransferases and the future of liver injury biomarkers. EXCLI J. 2016, 15, 817–828. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Group (n = 30) | Control Group (n = 31) | p-Value (1) | |
| Parameter | N (%) | N (%) | |
| Gender | |||
| Female | 22 (73.33) | 21 (67.74) | 0.78 (1) |
| Male | 8 (26.67) | 10 (32.26) | |
| Systemic diseases | |||
| None Allergic rhinitis | 27 3 | 29 2 | 0.67 |
| Smoking | 0 | 0 | >0.99 |
| Alcohol drinking | 1 (3.33) | 2 (6.45) | >0.99 |
| Study Group (n = 30) | Control Group (n = 31) | p-Value (2) | |
| Parameter | Mean ± SD | Mean ± SD | |
| Age (years) | 32.43 ± 6.82 | 30.87 ± 7.39 | 0.42 |
| BMI (kg/m2) | 23.7 ± 4.48 | 23.09 ± 4.13 | 0.49 |
| Systolic blood pressure (mmHg) | 116.93 ± 11.33 | 118.2 ± 14.1 | 0.72 |
| Diastolic blood pressure (mmHg) | 78.57 ± 10.98 | 74.9 ± 9.8 | 0.17 |
| Pulse rate (beats/min) | 77.57 ± 8.48 | 74.43 ± 12.98 | 0.28 |
| Parameter | Study Group (n = 30) | Control Group (n = 31) | p-Value |
|---|---|---|---|
| WBC (cells/cu.mm) | 6.37 ± 1.45 × 103 | 6.34 ± 1.18 × 103 | 0.55 |
| RBC (million cells/cu.mm) | 4.83 ± 0.43 × 106 | 4.56 ± 0.35 × 106 | 0.42 |
| Hemoglobin (g/dL) | 13.46 ± 0.95 | 13.31 ± 1.19 | 0.89 |
| Hematocrit value (%) | 40.82 ± 3.2 | 40.69 ± 3.32 | 0.96 |
| MCV (fL) | 86.07 ± 3.83 | 84.6 ± 6.94 | 0.27 |
| MCH (pg) | 29.01 ± 1.46 | 27.9 ± 2.72 | 0.30 |
| MCHC (g/dL) | 33.51 ± 0.42 | 33 ± 0.82 | 0.69 |
| RBDW (%) | 13.15 ± 0.84 | 12.89 ± 0.96 | 0.06 |
| Platelet count (cells/cu.mm) | 290,900 ± 74,118.89 | 279,709.68 ± 63,507.59 | 0.46 |
| Neutrophils (%) | 55.37 ± 8.45 | 44.94 ± 12.17 | 0.43 |
| Lymphocytes (%) | 32.54 ± 6.22 | 32.18 ± 20.44 | 0.28 |
| Monocytes (%) | 6.13 ± 1.23 | 15.23 ± 15.49 | 0.53 |
| Eosinophil (%) | 2.64 ± 1.77 | 3.54 ± 3.41 | 0.24 |
| Basophil (%) | 0.77 ± 0.43 | 1.56 ± 1.66 | 0.59 |
| Fasting plasma glucose (mg/dL) | 104.33 ± 6.91 | 90.68 ± 10.14 | *** |
| HbA1C (%) | 5.27 ± 0.31 | 5.10 ± 0.41 | 0.08 |
| Total cholesterol (mg/dL) | 218 ± 35.00 | 194.30 ± 28.01 | ** |
| Triglyceride (mg/dL) | 100.3 ± 32.49 | 97.42 ± 26.07 | 0.70 |
| HDL cholesterol (mg/dL) | 58.07 ± 11.23 | 68.00 ± 13.00 | ** |
| LDL cholesterol (mg/dL) | 141.03 ± 30.00 | 105.89 ± 24.04 | **** |
| BUN (mg/dL) | 11.37 ± 2.92 | 11.21 ± 2.98 | 0.73 |
| Creatinine (mg/dL) | 0.64 ± 0.11 | 0.71 ± 0.09 | *** |
| eGFR (mL/min/1.73 m2) | 121.63 ± 8.85 | 110.75 ± 10.62 | *** |
| AST (U/L) | 21.20 ± 5.87 | 18.33 ± 4.79 | * |
| ALT (U/L) | 18.87 ± 8.85 | 15.57 ± 8.76 | * |
| Total bilirubin (mg/dL) | 0.52 ± 0.12 | 0.44 ± 0.23 | 0.09 |
| Sodium level (mg/dL) | 136.6 ± 2.49 | 134.33 ± 6.66 | 0.08 |
| Potassium level (mg/dL) | 4.14 ± 0.28 | 4.16 ± 0.35 | 0.61 |
| Chloride level (mg/dL) | 100.27 ± 1.66 | 100.41 ± 1.96 | 0.93 |
| Carbon dioxide level (mg/dL) | 19.53 ± 2.10 | 20.27 ± 1.39 | 0.13 |
| Variables | Study Group (n = 30) | Control Group (n = 31) |
|---|---|---|
| Participants with any AEs | 0 | 0 |
| Specific AEs | 0 | 0 |
| Burning mouth | 0 | 0 |
| Nausea | 0 | 0 |
| Vomiting | 0 | 0 |
| Abdominal pain | 0 | 0 |
| Headache | 0 | 0 |
| Parameter | Normal Range | Study Group (n = 30) | Placebo Group (n = 31) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Week 4 | Week 8 | Week 12 | Week 14 | Baseline | Week 4 | Week 8 | Week 12 | Week 14 | ||
| Color | Colorless | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Appearance | Clear | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Specific gravity | 1.003–1.030 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| pH | 5.0–8.0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Leukocyte | Negative | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Nitrite | Negative | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Glucose | Negative | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Protein | Negative | 1 (1+) | 0 | 1 (2+) | 0 | 1 | 1 (2+) | 0 | 0 | 0 | 0 |
| Bilirubin | Negative | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Ketone | Negative | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Urobilinogen | Normal | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Blood | Negative | 0 | 1 (4+) | 0 | 0 | 0 | 1 (4+) | 2 (4+, 4+) | 0 | 0 | 0 |
| WBC | 0–1 cell/HP | 0 | 1 (2–3) | 0 | 0 | 0 | 1 (2–3) | 2 (2–3, 2–3) | 0 | 0 | 0 |
| RBC | 0–1 cell/HP | 0 | 2 (3–5, 3–5) | 0 | 0 | 1 (3–5) | 1 (3–5) | 2 (3–5, 3–5) | 0 | 0 | 0 |
| Squamous epithelial cell | 0–1 cell/HP | 1 (3–5) | 2 (3–5, 3–5) | 0 | 0 | 0 | 0 | 2 (3–5, 3–5) | 0 | 0 | 0 |
| Bacteria | Few | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rungraung, N.; Muangpracha, N.; Trachootham, D. Twelve-Week Safety and Potential Lipid Control Efficacy of Coffee Cherry Pulp Juice Concentrate in Healthy Volunteers. Nutrients 2023, 15, 1602. https://doi.org/10.3390/nu15071602
Rungraung N, Muangpracha N, Trachootham D. Twelve-Week Safety and Potential Lipid Control Efficacy of Coffee Cherry Pulp Juice Concentrate in Healthy Volunteers. Nutrients. 2023; 15(7):1602. https://doi.org/10.3390/nu15071602
Chicago/Turabian StyleRungraung, Numphung, Niramol Muangpracha, and Dunyaporn Trachootham. 2023. "Twelve-Week Safety and Potential Lipid Control Efficacy of Coffee Cherry Pulp Juice Concentrate in Healthy Volunteers" Nutrients 15, no. 7: 1602. https://doi.org/10.3390/nu15071602
APA StyleRungraung, N., Muangpracha, N., & Trachootham, D. (2023). Twelve-Week Safety and Potential Lipid Control Efficacy of Coffee Cherry Pulp Juice Concentrate in Healthy Volunteers. Nutrients, 15(7), 1602. https://doi.org/10.3390/nu15071602