
Is Maternal Carbohydrate Intake Having an Impact on Newborn Birth Weight? A Systematic Review



 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Information Sources and Search Strategy
2.3. Study Selection
2.4. Data Extraction
2.5. Quality Appraisal
2.6. Data Analysis
3. Results
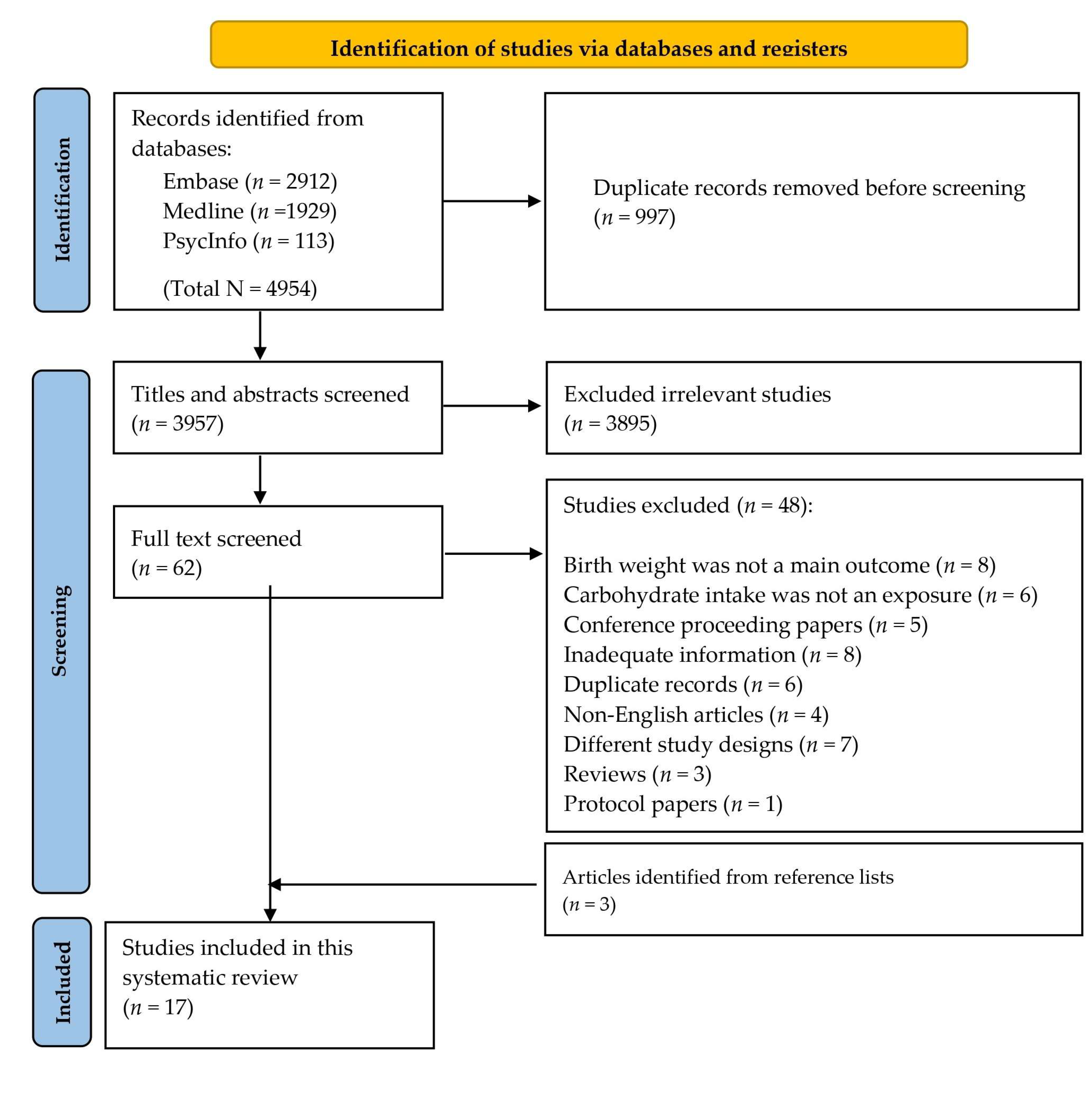
3.1. Study Selection
3.2. Characteristics of Included Studies
3.3. Characteristics of Study Participants
3.4. Reported Energy and Carbohydrate Intakes during Pregnancy
3.5. Summary of Findings Related to Carbohydrate Intake and Neonatal Birth Weight
3.6. Other Findings Related to Nutrient Intake and Neonatal Birth Weight
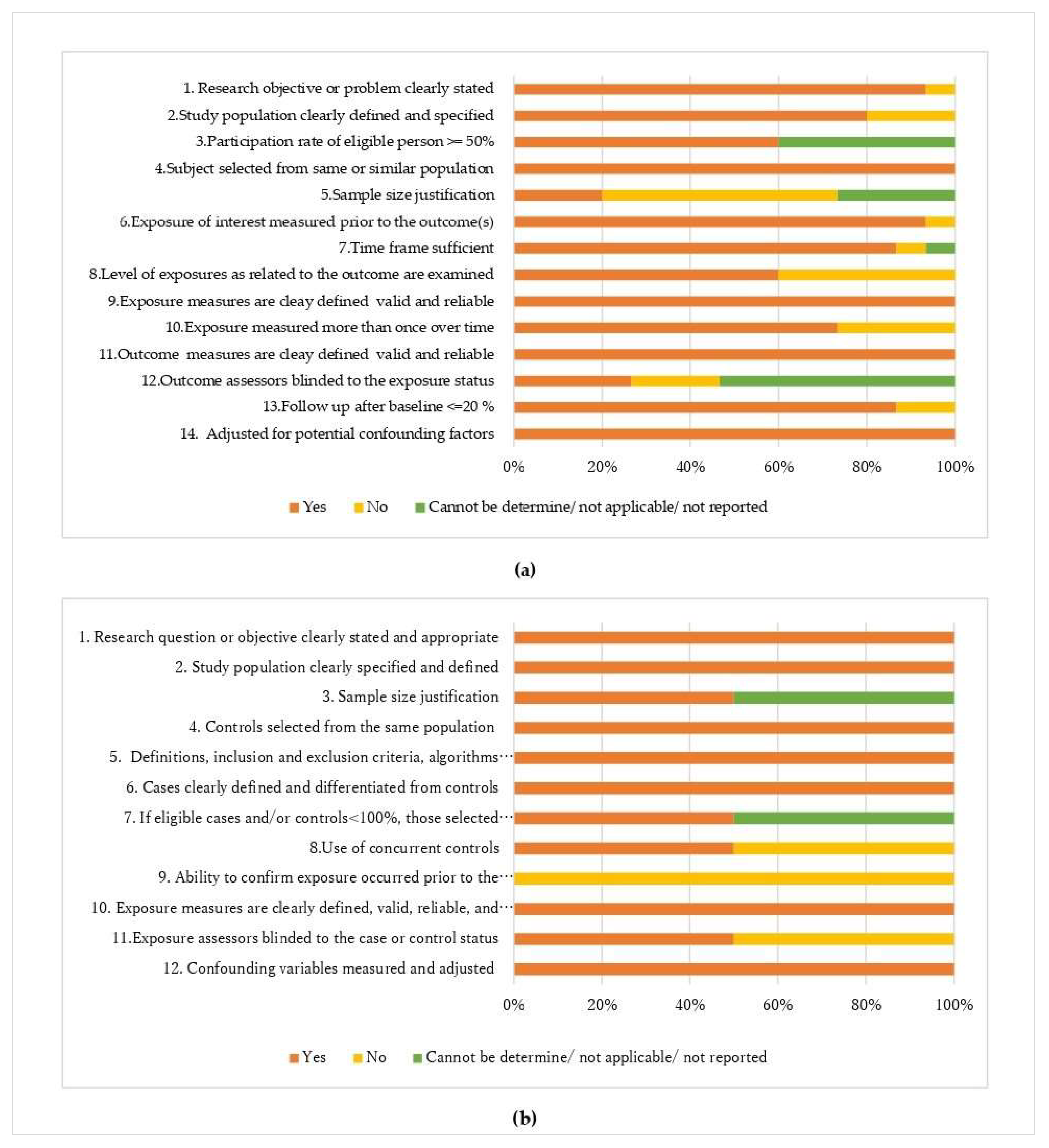
3.7. Quality Appraisal of Included Studies
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Search Items | |
|---|---|
| 1 | matern*.mp. or pregnancy/ |
| 2 | mothers/or mother*.mp. |
| 3 | pregnan*.mp. |
| 4 | (maternal adj3 carbohydrate*).mp. [mp = title, abstract, original title, name of substance word, subject heading word, floating sub-heading word, keyword heading word, organism supplementary concept word, rare disease supplementary conceptword, unique identifier, synonyms] |
| 5 | 1 OR 2 OR 3 OR 4 |
| 6 | dietary carbohydrates/or CHO.mp. |
| 7 | carbohydrates/ |
| 8 | starch.mp. or starch/ |
| 9 | sugar.mp. or sugars/ |
| 10 | 6 OR 7 OR 8 OR 9 |
| 11 | infant, newborn/or*.mp. |
| 12 | infant/or infant*.mp. |
| 13 | (baby or babies).mp. |
| 14 | birth weight/or birth?weight.mp |
| 15 | (birth?weight adj5 (neonate* or infant* or baby or babies or newborn*)).mp.[mp=title, abstract, original title, name of substance word, subject heading word, floating sub- heading word, keyword heading word, organism supplementary concept word, raredisease supplementary concept word, unique identifier, synonyms] |
| 16 | pregnancy outcomes/or pregnancy outcome*.mp. |
| 17 | 11 OR 12 OR 13 OR 14 OR 15 OR 16 |
| 18 | 5 AND 10 AND 17 |
References
- Hales, C.N.; Barker, D.J. The thrifty phenotype hypothesis. Br. Med. Bull. 2001, 60, 5–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barker, D.J. In utero programming of chronic disease. Clin. Sci. 1998, 95, 115–128. [Google Scholar] [CrossRef]
- Gluckman, P.D.; Hanson, M.A.; Cooper, C.; Thornburg, K.L. Effect of in utero and early-life conditions on adult health and disease. N. Engl. J. Med. 2008, 359, 61–73. [Google Scholar] [CrossRef] [Green Version]
- Hanson, M.A.; Gluckman, P.D. Early developmental conditioning of later health and disease: Physiology or pathophysiology? Physiol. Rev. 2014, 94, 1027–1076. [Google Scholar] [CrossRef]
- Batstra, L.; Elsinga, N.C.; Hadders-Algra, M. Psychiatric morbidity is related to a chain of prenatal and perinatal adversities. Early Hum. Dev. 2006, 82, 721–729. [Google Scholar] [CrossRef]
- Visentin, S.; Grumolato, F.; Nardelli, G.B.; Di Camillo, B.; Grisan, E.; Cosmi, E. Early origins of adult disease: Low birth weight and vascular remodeling. Atherosclerosis 2014, 237, 391–399. [Google Scholar] [CrossRef]
- Barker, D.J. Fetal origins of coronary heart disease. BMJ 1995, 311, 171–174. [Google Scholar] [CrossRef] [PubMed]
- Otten, J.J.; Hellwig, J.P.; Meyers, L.D. (Eds.) Institute of Medicine of the National Academies. In Dietary Reference Intakes: The Essential Guide to Nutrient Requirements; Institute of Medicine of the National Academies; The National Academies Press: Washington, DC, USA, 2006. [Google Scholar]
- Merialdi, M.; Carroli, G.; Villar, J.; Abalos, E.; Gülmezoglu, A.M.; Kulier, R.; De Onis, M. Nutritional interventions during pregnancy for the prevention or treatment of impaired fetal growth: An overview of randomized controlled trials. J. Nutr. 2003, 133, 1626S–1631S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dodd, J.M.; Deussen, A.R.; Louise, J. A randomised trial to optimise gestational weight gain and improve maternal and infant health outcomes through antenatal dietary, lifestyle and exercise advice: The OPTIMISE randomised trial. Nutrients 2019, 11, 2911. [Google Scholar] [CrossRef] [Green Version]
- De Onis, M.; Villar, J.; Gülmezoglu, M. Nutritional interventions to prevent intrauterine growth retardation: Evidence from randomized controlled trials. Eur. J. Clin. Nutr. 1998, 52 (Suppl. 1), S83–S93. [Google Scholar]
- Kramer, M.S.; Kakuma, R. Energy and protein intake in pregnancy. Cochrane Database Syst. Rev. 2003, 4, Cd000032. [Google Scholar]
- Stevens, B.; Buettner, P.; Watt, K.; Clough, A.; Brimblecombe, J.; Judd, J. The effect of balanced protein energy supplementation in undernourished pregnant women and child physical growth in low- and middle-income countries: A systematic review and meta-analysis. Matern. Child Nutr. 2015, 11, 415–432. [Google Scholar] [CrossRef] [PubMed]
- Imdad, A.; Bhutta, Z.A. Effect of balanced protein energy supplementation during pregnancy on birth outcomes. BMC Public Health 2011, 11 (Suppl. 3), S17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gresham, E.; Byles, J.E.; Bisquera, A.; Hure, A.J. Effects of dietary interventions on neonatal and infant outcomes: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2014, 100, 1298–1321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Heart, Lung, and Blood Institute. Study Quality Assessment Tools. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 31 January 2023).
- Godfrey, K.; Robinson, S.; Barker, D.J.; Osmond, C.; Cox, V. Maternal nutrition in early and late pregnancy in relation to placental and fetal growth. BMJ 1996, 312, 410. [Google Scholar] [CrossRef] [Green Version]
- Mathews, F.; Yudkin, P.; Neil, A. Influence of maternal nutrition on outcome of pregnancy: Prospective cohort study. BMJ 1999, 319, 339–343. [Google Scholar] [CrossRef] [Green Version]
- Langley-Evans, A.J.; Langley-Evans, S.C. Relationship between maternal nutrient intakes in early and late pregnancy and infants weight and proportions at birth: Prospective cohort study. J. R. Soc. Promot. Health 2003, 123, 210–216. [Google Scholar] [CrossRef]
- Lagiou, P.; Tamimi, R.M.; Mucci, L.A.; Adami, H.O.; Hsieh, C.C.; Trichopoulos, D. Diet during pregnancy in relation to maternal weight gain and birth size. Eur. J. Clin. Nutr. 2004, 58, 231–237. [Google Scholar] [CrossRef] [Green Version]
- Moore, V.M.; Davies, M.J.; Willson, K.J.; Worsley, A.; Robinson, J.S. Dietary composition of pregnant women is related to size of the baby at birth. J. Nutr. 2004, 134, 1820–1826. [Google Scholar] [CrossRef] [Green Version]
- Denguezli, W.; Faleh, R.; Fessi, A.; Yassine, A.; Hajjaji, A.; Laajili, H.; Sakouhi, M. Risk factors of fetal macrosomia: Role of maternal nutrition. Tunis. Med. 2009, 87, 564–568. [Google Scholar]
- Bawadi, H.A.; Al-Kuran, O.; Al-Bastoni, L.A.; Tayyem, R.F.; Jaradat, A.; Tuuri, G.; Al-Beitawi, S.N.; Al-Mehaisen, L.M. Gestational nutrition improves outcomes of vaginal deliveries in Jordan: An epidemiologic screening. Nutr. Res. 2010, 30, 110–117. [Google Scholar] [CrossRef]
- Watson, P.E.; McDonald, B.W. The association of maternal diet and dietary supplement intake in pregnant New Zealand women with infant birthweight. Eur. J. Clin. Nutr. 2010, 64, 184–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crume, T.L.; Brinton, J.T.; Shapiro, A.; Kaar, J.; Glueck, D.H.; Siega-Riz, A.M.; Dabelea, D. Maternal dietary intake during pregnancy and offspring body composition: The Healthy Start Study. Am. J. Obstet. Gynecol. 2016, 215, 609.e1–609.e8. [Google Scholar] [CrossRef] [Green Version]
- Diemert, A.; Lezius, S.; Pagenkemper, M.; Hansen, G.; Drozdowska, A.; Hecher, K.; Arck, P.; Zyriax, B.C. Maternal nutrition, inadequate gestational weight gain and birth weight: Results from a prospective birth cohort. BMC Pregnancy Childbirth 2016, 16, 224. [Google Scholar] [CrossRef] [Green Version]
- Pathirathna, M.L.; Sekijima, K.; Sadakata, M.; Fujiwara, N.; Muramatsu, Y.; Wimalasiri, K.M.S. Impact of Second Trimester Maternal Dietary Intake on Gestational Weight Gain and Neonatal Birth Weight. Nutrients 2017, 9, 627. [Google Scholar] [CrossRef] [Green Version]
- Grandy, M.; Snowden, J.M.; Boone-Heinonen, J.; Purnell, J.Q.; Thornburg, K.L.; Marshall, N.E. Poorer maternal diet quality and increased birth weight. J. Matern. Fetal Neonatal Med. 2018, 31, 1613–1619. [Google Scholar] [CrossRef] [PubMed]
- Hjertholm, K.G.; Iversen, P.O.; Holmboe-Ottesen, G.; Mdala, I.; Munthali, A.; Maleta, K.; Shi, Z.; Ferguson, E.; Kamudoni, P. Maternal dietary intake during pregnancy and its association to birth size in rural Malawi: A cross-sectional study. Matern. Child Nutr. 2018, 14, e12433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, S.S.; Greenwood, D.C.; Simpson, N.A.B.; Cade, J.E. Is dietary macronutrient composition during pregnancy associated with offspring birth weight? An observational study. Br. J. Nutr. 2018, 119, 330–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amezcua-Prieto, C.; Martínez-Galiano, J.M.; Cano-Ibáñez, N.; Olmedo-Requena, R.; Bueno-Cavanillas, A.; Delgado-Rodríguez, M. Types of Carbohydrates Intake during Pregnancy and Frequency of a Small for Gestational Age Newborn: A Case-Control Study. Nutrients 2019, 11, 523. [Google Scholar] [CrossRef] [Green Version]
- Eshak, E.S.; Okada, C.; Baba, S.; Kimura, T.; Ikehara, S.; Sato, T.; Shirai, K.; Iso, H.; Japan Environment and Children’s Study Group. Maternal total energy, macronutrient and vitamin intakes during pregnancy associated with the offspring’s birth size in the Japan Environment and Children’s Study. Br. J. Nutr. 2020, 124, 558–566. [Google Scholar]
- Minato-Inokawa, S.; Hayashi, I.; Nirengi, S.; Yamaguchi, K.; Takakura, K.; Sakane, N.; Nagai, N. Association of Dietary Change during Pregnancy with Large-for-Gestational Age Births: A Prospective Observational Study. J. Nutr. Sci. Vitaminol. 2020, 66, 246–254. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Database on Body Mass Index. Available online: http://apps.who.int/bmi/index.jsp?introPage=intro-3.html (accessed on 1 February 2023).
- Kroener, L.; Wang, E.T.; Pisarska, M.D. Predisposing Factors to Abnormal First Trimester Placentation and the Impact on Fetal Outcomes. Semin. Reprod. Med. 2016, 34, 27–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, G.C. First Trimester Origins of Fetal Growth Impairment. Semin. Perinatol. 2004, 28, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, D.J.; Kendall, C.W.; Augustin, L.S.; Franceschi, S.; Hamidi, M.; Marchie, A.; Jenkins, A.L.; Axelsen, M. Glycemic index: Overview of implications in health and disease. Am. J. Clin. Nutr. 2002, 76, 266s–273s. [Google Scholar]



{kind=link}
{kind=link}
| Study | Energy Intake (kcal/day) a | Carbohydrate Intake (g/day) a | % of Energy Derived from Carbohydrates a |
|---|---|---|---|
| Godfrey et al., 1996 [17] | EP: 2329 (1882, 2789); LP: 2314 (1970, 2729) | EP: 302.7 (245.7, 372.9); LP: 301.9 (254.3, 360.6) | EP: 49.4 (46.2, 53.4); LP: 49.0 (46.1, 52.2) |
| Mathews et al., 1999 [18] | EP: 2044 (1755, 2305); LP: 2197 (1824, 2660) | EP: 256.0 (218.0, 292.5); LP: 290.1 (242.5, 350.5) | EP: 47.3 (44.1, 50.4); LP: 50.1 (46.1, 53.7) |
| Langley-Evans et al., 2003 [19] | FT: 2008 (1794, 2312); TT: 2023 (1802, 2279) | Carbohydrate: FT: 262.4 (228.3, 299.6); TT: 272.7 (232.3, 302.2), Sugar: FT: 15.2 (90.3, 142.1); TT: 116.7 (93.7, 150.4), Starch: FT: 143.9 (123.0, 168.0); TT: 143.5 (122.4, 162.1) | FT: 49.0 (45.0, 52.7); TT: 48.7 (46.2, 52.5) |
| Lagiou et al., 2004 [20] | NR | NR | NR |
| Moore et al., 2004 [21] | EP: 2151.1 (1720.8, 2772.5); LP: 2198.9 (1792.5, 2700.8) | EP: 273 (213, 349); LP: 282 (230, 347) | EP: 48.3 (44.5, 53.5); LP: 49.1 (45.0, 53.3) |
| Denguezli et al., 2009 b [22] | Total: 2701.0 ± 622.0; CAs: 3124.9 ± 403.0;COs: 2626.9 ± 624.6 | Total: 413.6 ± 105.7; CAs: NR;COs: NR | NR |
| Bawadi et al., 2010 c [23] | 2603.7 ± 32.9 | 320.8 ± 3.8 | NR |
| Watson and McDonald, 2010 d [24] | 4th month: 2261.2; 7th month: 2199.8 | Carbohydrate: 4th month: 270; 7th month: 267, Glucose: 4th month: 26; 7th month: 26, Fructose: 4th month: 27; 7th month: 27, Sucrose: 4th month: 61; 7th month: 63, Lactose:4th month: 17; 7th month: 18, Maltose: 4th month: 3; 7th month: 3, Starch: 4th month: 136; 7th month: 129 | NR |
| Crume et al., 2016 [25] | 2025.0 (1789.6, 2252.6) | 242.3 (195.6, 291.6) | 47.8 (42.3, 53.2) |
| Diemert et al., 2016 b [26] | FT: 1987 ± 505; ST: 2068 ± 463;TT: 2151 ± 472 | FT: 239 ± 65; ST: 245 ± 66;TT: 254 ± 66 | 49% |
| Pathirathna et al., 2017 b [27] | ST: 2921.5 ± 687.7 | ST: 532.7 ± 133.8 | NR |
| Grandy et al., 2018 b [28] | TT: 2382 ± 556 | NR | 51 ± 8 |
| Hjertholm et al., 2018 [29] | TT: 2096.5 (1778.1, 2570.6) | TT: 377 (306, 454) | NR |
| Sharma et al., 2018 b [30] | FT: 2120 ± 692;ST: 2279 ± 634 | Carbohydrate: FT: 274 ± 99; ST: 300 ± 92, Added sugar: FT: 127 ± 73; ST: 149 ± 69, Glucose: FT: 25 ± 19; ST: 27 ± 17, Fructose: FT: 27 ± 28; ST: 30 ± 24, Sucrose: FT: 54 ± 36; ST: 64 ± 36, Maltose: FT: 2 ± 7; ST: 2 ± 3, Lactose: FT: 16 ± 13; ST: 19 ± 15, | NR |
| Amezcua-Prieto et al., 2019 [31] | NR | NR | NR |
| Eshak et al., 2020 [32] | 1620 (1311–2015) | 223.8 (182.6, 272.4) | 55.3 (50.2, 60.3) |
| Minato-Inokawa et al., 2020 b [33] | SGA group: 1444 ± 452; AGA group: 1500 ± 465; LGA group: 1506 ± 482 | Carbohydrate b,e: SGA group: 144.6 ± 23.1; AGA group: 143.0 ± 18.3; LGA group: 145.0 ± 9.6, Sucrose b,e: SGA group: 6.9 ± 3.4; AGA group: 6.4 ± 4.3; LGA group: 6.3 ± 5.9 | NR |
| Study | Trimester/Period Studied | Method of Dietary Assessment | Confounders/Covariates | Significant Findings Related to Carbohydrate Intake and Birth Weight | Significant Findings Related to Other Nutrient Components and Birth Weight |
|---|---|---|---|---|---|
| Godfrey et al., 1996 [17] | Early pregnancy and late pregnancy (Median durations 15.3 and 32.7 weeks) | FFQ | Gestational age at delivery; newborn gender | A higher intake of carbohydrates in early pregnancy was associated with lower birth weight, especially if combined with low dairy protein intake in late pregnancy. | None |
| Mathews et al., 1999 [18] | First trimester and third trimester | 7 day food diary, FFQ | Maternal smoking, height, nutrient intake, gestational age at delivery, gender of the newborn | None | Birth weight was positively associated with early maternal intake of vitamin C. |
| Langley-Evans et al., 2003 [19] | First trimester and third trimester | 5 day food diary | Social class based on partner’s occupation, maternal weight at booking, maternal smoking, gestational age at delivery, gender of the newborn | None | None |
| Lagiou et al., 2004 [20] | Second trimester | FFQ | Maternal age, height, pre-pregnancy BMI, education, parity, pre-gravid oral contraceptive use, maternal smoking, gestational age at delivery, gender of the newborn | None | None |
| Moore et al., 2004 [21] | Early pregnancy and late pregnancy (before 16 weeks and 30–34 weeks gestation) | FFQ | Maternal smoking, alcohol consumption, height, pre-pregnancy weight, parity, use of recreational drugs, gestational age at delivery | None | The percentage of energy derived from protein in early pregnancy was positively associated with birth weight. |
| Denguezli et al., 2009 [22] | Third trimester: the last 24 h before delivery | FFQ | Pre-pregnancy BMI, parity, term | None | None |
| Bawadi et al., 2010 [23] | Retrospectively collected data during 1–2 days postpartum focusing on the dietary intake during gestation | FFQ | Maternal pre-pregnancy BMI, parity, gestational weight gain | None | Birth weight was positively associated with maternal calcium and vitamin A intake. |
| Watson and McDonald, 2010 [24] | Month 4 and month 7 of pregnancy | 24 HDR, 3 day food diary | Maternal height, weight, smoking, number of preschoolers, number of other adults in the house, gestational age at delivery (modified for over term babies), gender of the newborn | A quadratic relationship was established between birth weight and the percentage of total energy from carbohydrates, fat, and protein throughout pregnancy; birth weight was greatest when the percentage of total energy from carbohydrates was 48%, along with 35% fat and 17% protein. | Birth weight was greatest when the percentage of total energy from carbohydrates was 48%, along with 35% fat and 17% protein. |
| Crume et al., 2016 [25] | Throughout pregnancy | 24 HDR | Maternal age, pre-pregnancy BMI, gravidity, race/ethnicity, smoking at any time during pregnancy, postnatal age at air displacement plethysmography measurement, physical activity levels during pregnancy, gestational age at delivery, gender of the newborn | None | None |
| Diemert et al., 2016 [26] | First trimester (12 + 0 to 14 + 6 weeks); second trimester (22 + 0 to 24 + 6 weeks); third trimester (34 + 0 to 36 + 6 weeks gestation) | 24 HDR | Maternal age, pre-pregnancy BMI, level of education, gestational age at delivery | None | None |
| Pathirathna et al., 2017 [27] | Second trimester | FFQ | Gestational age at delivery, average monthly income, area of residence, history of low-birth-weight delivery | The newborns of women with low carbohydrate intake during pregnancy second trimester were lighter than those of women with a moderate carbohydrate intake. | None |
| Grandy et al., 2018 [28] | Third trimester (37–38 weeks gestation) | 24 HDR | Maternal age, pre-pregnancy BMI, parity, total energy intake | None | None |
| Hjertholm et al., 2018 [29] | Third trimester | 3 day repeated interactive multi-pass 24 HDR, 4 day repeated single-pass 24 HDR | Maternal age, weight, height, gestational age at delivery, literacy, marital status, household assets, parity, total energy intake, gender of the newborn | None | Birth weight was positively associated with vitamin C and the frequency of milk intake. |
| Sharma et al., 2018 [30] | First trimester, second trimester | 24 HDR | Alcohol and smoking consumption status | The first-trimester maternal carbohydrate intake was positively associated with neonatal birth weight, while second-trimester maternal glucose and lactose intake were positively associated with neonatal birth weight. | Birth weight was negatively associated with early pregnancy maternal fat consumption and higher intake of PUFAs. |
| Amezcua-Prieto et al., 2019 [31] | Retrospective collection of data during 1–2 days of postpartum focusing on the dietary intake during the previous year | FFQ | Maternal level of education, pre-pregnancy BMI, parity, history of low-birth-weight delivery, history of preterm delivery, total energy intake, maternal smoking | Consumption of brown bread >75 g/day was inversely correlated with SGA, while industrial sweets more than once a day or even 2–6 times a week increased the risk of SGA births. | None |
| Eshak et al., 2020 [32] | Throughout pregnancy | FFQ | Maternal age, height, pre-pregnancy BMI, education, parity, household income, use of folate supplements, maternal smoking, alcohol consumption, gestational weight gain, gestational age at delivery, gender of the newborn | None | Birth weight was positively associated with maternal intake of total energy, dietary fiber, folate. and vitamins A, K, E, D, and C. |
| Minato-Inokawa et al., 2020 [33] | First trimester, second trimester, third trimester | BDHQ | Total energy intake | Mothers with LGA showed larger changes in plant oil and sucrose consumption from the first to the second trimester of pregnancy. | None |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pathirathna, M.L.; Nandasena, H.M.R.K.G.; Samarasekara, B.P.P.; Dasanayake, T.S.; Weerasekara, I.; Haruna, M. Is Maternal Carbohydrate Intake Having an Impact on Newborn Birth Weight? A Systematic Review. Nutrients 2023, 15, 1649. https://doi.org/10.3390/nu15071649
Pathirathna ML, Nandasena HMRKG, Samarasekara BPP, Dasanayake TS, Weerasekara I, Haruna M. Is Maternal Carbohydrate Intake Having an Impact on Newborn Birth Weight? A Systematic Review. Nutrients. 2023; 15(7):1649. https://doi.org/10.3390/nu15071649
Chicago/Turabian StylePathirathna, Malshani L., Hapugahapitiye M. R. K. G. Nandasena, Buddhini P. P. Samarasekara, Thakshila S. Dasanayake, Ishanka Weerasekara, and Megumi Haruna. 2023. "Is Maternal Carbohydrate Intake Having an Impact on Newborn Birth Weight? A Systematic Review" Nutrients 15, no. 7: 1649. https://doi.org/10.3390/nu15071649
APA StylePathirathna, M. L., Nandasena, H. M. R. K. G., Samarasekara, B. P. P., Dasanayake, T. S., Weerasekara, I., & Haruna, M. (2023). Is Maternal Carbohydrate Intake Having an Impact on Newborn Birth Weight? A Systematic Review. Nutrients, 15(7), 1649. https://doi.org/10.3390/nu15071649