
Association of the Practice of Physical Activity and Dietary Pattern with Psychological Distress before and during COVID-19 in Brazilian Adults

 ,
,  , and
, and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Sociodemographic and Health Factors
2.2. Physical Activity Practices, Food Habits and Psychological Distress
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Organização Mundial da Saúde. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19-11 March 2020. Genebra: OMS. 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 17 June 2020).
- Croda, J.H.R.; Garcia, L.P. Immediate Health Surveillance Response to COVID-19 Epidemic. Resposta imediata da Vigilância em Saúde à epidemia da COVID-19. Epidemiol. E Serv. Saude 2020, 29, e2020002. [Google Scholar] [CrossRef]
- Brasil. Ministério da Saúde, Secretaria de Vigilância em Saúde. Boletim Epidemiológico Especial COE-COVID-19. 2020. Available online: https://www.saude.gov.br/images/pdf/2020/May/29/2020-05-25---BEE17---Boletim-do-COE.pdf (accessed on 17 June 2020).
- Organização Mundial da Saúde. Coronavirus Disease (COVID-19) Pandemic; OMS: Genebra, Switzerland, 2020; Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 17 June 2020).
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [PubMed]
- Carlson, C.J. From PREDICT to prevention, one pandemic later. Lancet Microbe 2020, 1, e6–e7. [Google Scholar] [CrossRef] [PubMed]
- Belo Horizonte Prefeitura Municipal. Decreto n° 17.297, de 17 de Março de 2020. Declara Situação Anormal, Caracterizada Como Situação de Emergência em Saúde Pública, no Município de Belo Horizonte em Razão da Necessidade de Ações Para Conter a Propagação de Infecção Viral, Bem Como de Preservar a Saúde da População Contra o Coronavírus—COVID-19. 2020. Available online: https://leismunicipais.com.br/a/mg/b/belo-horizonte/decreto/2020/1730/17297/decreto-n-17297-2020-declara-situacao-anormal-caracterizada-como-situacao-de-emergencia-em-saude-publica-no-municipio-de-belo-horizonte-em-razao-da-necessidade-de-acoes-para-conter-a-propagacao-de-infeccao-viral-bem-como-de-preservar-a-saude-da-populacao-contra-o-coronavirus-covid-19 (accessed on 17 June 2020).
- Maranhão Governo do Estado. Decreto n° 35.678 de 22 de Março de 2020. Altera o Decreto n° 35.677, de 21 de Março de 2020, Que Estabelece Medidas de Prevenção do Contágio e de Combate à Propagação da Transmissão da COVID-19, Infecção Humana Causada Pelo CORONAVírus (SARS-CoV-2). 2020. Available online: https://www.tjma.jus.br/midia/cov/pagina/hotsite/500915/decretos-estaduais-ma (accessed on 17 June 2020).
- Luo, M.; Guo, L.; Yu, M.; Jiang, W.; Wang, H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public—A systematic review and meta-analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui LM, W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- Xiao, C. A Novel Approach of Consultation on 2019 Novel Coronavirus (COVID-19)-Related Psychological and Mental Problems: Structured Letter Therapy. Psychiatry Investig. 2020, 17, 175–176. [Google Scholar] [CrossRef]
- Chen, P.; Mao, L.; Nassis, G.P.; Harmer, P.; Ainsworth, B.E.; Li, F. Coronavirus disease (COVID-19): The need to maintain regular physical activity while taking precautions. J. Sport Health Sci. 2020, 9, 103–104. [Google Scholar] [CrossRef]
- Jiménez-Pavón, D.; Carbonell-Baeza, A.; Lavie, C.J. Physical exercise as therapy to fight against the mental and physical consequences of COVID-19 quarantine: Special focus in older people. Prog. Cardiovasc. Dis. 2020, 63, 386–388. [Google Scholar] [CrossRef]
- GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 2022, 9, 137–150. [Google Scholar] [CrossRef]
- Schuch, F.B.; Stubbs, B.; Meyer, J.; Heissel, A.; Zech, P.; Vancampfort, D.; Rosenbaum, S.; Deenik, J.; Firth, J.; Ward, P.B.; et al. Physical activity protects from incident anxiety: A meta-analysis of prospective cohort studies. Depress. Anxiety 2019, 36, 846–858. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Firth, J.; Rosenbaum, S.; Ward, P.B.; Silva, E.S.; Hallgren, M.; Ponce De Leon, A.; Dunn, A.L.; Deslandes, A.C.; et al. Physical Activity and Incident Depression: A Meta-Analysis of Prospective Cohort Studies. Am. J. Psychiatry 2018, 175, 631–648. [Google Scholar] [CrossRef] [PubMed]
- Kandola, A.; Ashdown-Franks, G.; Hendrikse, J.; Sabiston, C.M.; Stubbs, B. Physical activity and depression: Toward understanding the antidepressant mechanisms of physical activity. Neurosci. Biobehav. Rev. 2019, 107, 525–539. [Google Scholar] [CrossRef] [PubMed]
- Sciamanna, C.N.; Smyth, J.M.; Doerksen, S.E.; Richard, B.R.; Kraschnewski, J.L.; Mowen, A.J.; Hickerson, B.D.; Rovniak, L.S.; Lehman, E.B.; Yang, C. Physical Activity Mode and Mental Distress in Adulthood. Am. J. Prev. Med. 2017, 52, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Muscogiuri, G.; Barrea, L.; Savastano, S.; Colao, A. Nutritional recommendations for CoVID-19 quarantine. Eur. J. Clin. Nutr. 2020, 74, 850–851. [Google Scholar] [CrossRef]
- Firth, J.; Marx, W.; Dash, S.; Carney, R.; Teasdale, S.B.; Solmi, M.; Stubbs, B.; Schuch, F.B.; Carvalho, A.F.; Jacka, F.; et al. The Effects of Dietary Improvement on Symptoms of Depression and Anxiety: A Meta-Analysis of Randomized Controlled Trials. Psychosom. Med. 2019, 81, 265–280. [Google Scholar] [CrossRef]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; World Health Organization: Geneva, Switzerland, 1998. [Google Scholar]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.L.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in nonspecific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef]
- Pereira, A.; Oliveira, C.A.; Bártolo, A.; Monteiro, S.; Vagos, P.; Jardim, J. Reliability and Factor Structure of the 10-item Kessler Psychological Distress Scale (K10) among Portuguese adults. Cienc. Saude Coletiva 2019, 24, 729–736. [Google Scholar] [CrossRef]
- Szuster, E.; Kostrzewska, P.; Pawlikowska, A.; Mandera, A.; Biernikiewicz, M.; Kałka, D. Mental and Sexual Health of Polish Women of Reproductive Age During the COVID-19 Pandemic—An Online Survey. Sex. Med. 2021, 9, 100367. [Google Scholar] [CrossRef]
- Ghassabian, A.; Jacobson, M.H.; Kahn, L.G.; Brubaker, S.G.; Mehta-Lee, S.S.; Trasande, L. Maternal Perceived Stress During the COVID-19 Pandemic: Pre-Existing Risk Factors and Concurrent Correlates in New York City Women. Int. J. Public Health 2022, 67, 1604497. [Google Scholar] [CrossRef]
- Institute of Health Metrics and Evaluation. Global Health Data Exchange (GHDx). Institute for Health Metrics and Evaluation. 2019. Available online: https://vizhub.healthdata.org/gbd-results (accessed on 7 August 2022).
- World Health Organization. Mental Disorders. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/mental-disorders (accessed on 26 July 2022).
- Heissel, A.; Heinen, D.; Brokmeier, L.L.; Skarabis, N.; Kangas, M.; Vancampfort, D.; Stubbs, B.; Firth, J.; Ward, P.B.; Rosenbaum, S.; et al. Exercise as medicine for depressive symptoms? A systematic review and meta-analysis with meta-regression. Br. J. Sports Med. 2023. [Google Scholar] [CrossRef]
- Ashdown-Franks, G.; Firth, J.; Carney, R.; Carvalho, A.F.; Hallgren, M.; Koyanagi, A.; Rosenbaum, S.; Schuch, F.B.; Smith, L.; Solmi, M.; et al. Exercise as Medicine for Mental and Substance Use Disorders: A Meta-review of the Benefits for Neuropsychiatric and Cognitive Outcomes. Sports Med. 2020, 50, 151–170. [Google Scholar] [CrossRef] [PubMed]
- McDowell, C.P.; Dishman, R.K.; Gordon, B.R.; Herring, M.P. Physical Activity and Anxiety: A Systematic Review and Meta-analysis of Prospective Cohort Studies. Am. J. Prev. Med. 2019, 57, 545–556. [Google Scholar] [CrossRef] [PubMed]
- Tárraga López, P.J.; Tárraga Marcos, A.; Panisello, J.M.; Herencia Carbayo, J.A.; Tárraga Marcos, M.L.; López-Gil, J.F. Physical activity and its association with Mediterranean diet patterns among Spanish university students. Actividad física y su asociación con los patrones de dieta mediterránea en universitarios españoles. Nutr. Hosp. 2022, 39, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Archer, T.; Josefsson, T.; Lindwall, M. Effects of physical exercise on depressive symptoms and biomarkers in depression. CNS Neurol. Disord. Drug Targets 2014, 13, 1640–1653. [Google Scholar] [CrossRef]
- Singh, B.; Olds, T.; Curtis, R.; Dumuid, D.; Virgara, R.; Watson, A.; Szeto, K.; O’Connor, E.; Ferguson, T.; Eglitis, E.; et al. Effectiveness of physical activity interventions for improving depression, anxiety and distress: An overview of systematic reviews. Br. J. Sports Med. 2023. [Google Scholar] [CrossRef]
- Sejbuk, M.; Mirończuk-Chodakowska, I.; Witkowska, A.M. Sleep Quality: A Narrative Review on Nutrition, Stimulants, and Physical Activity as Important Factors. Nutrients 2022, 14, 1912. [Google Scholar] [CrossRef]
- Liu, Q.; Liu, Y.; Zhang, C.; An, Z.; Zhao, P. Elderly mobility during the COVID-19 pandemic: A qualitative exploration in Kunming, China. J. Transp. Geogr. 2021, 96, 103176. [Google Scholar] [CrossRef]
- Liu, Q.; Liu, Z.; Lin, S.; Zhao, P. Perceived accessibility and mental health consequences of COVID-19 containment policies. J. Transp. Health 2022, 25, 101354. [Google Scholar] [CrossRef]
- Gao, Y.; Ao, H.; Hu, X.; Wang, X.; Huang, D.; Huang, W.; Han, Y.; Zhou, C.; He, L.; Lei, X.; et al. Social media exposure during COVID-19 lockdowns could lead to emotional overeating via anxiety: The moderating role of neuroticism. Applied psychology. Health Well-Being 2022, 14, 64–80. [Google Scholar] [CrossRef]
- Victoria-Montesinos, D.; Tárraga-Marcos, A.; Brazo-Sayavera, J.; Jiménez-López, E.; Gutiérrez-Espinoza, H.; Panisello Royo, J.M.; Tárraga-López, P.J.; López-Gil, J.F. Adherence to the Mediterranean Diet and Health-Related Quality of Life during the COVID-19 Lockdown: A Cross-Sectional Study including Preschoolers, Children, and Adolescents from Brazil and Spain. Nutrients 2023, 15, 677. [Google Scholar] [CrossRef]

{kind=link}
| (A) | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Before Pandemic | Low Stress | Moderate Stress | High Stress | Very High Stress | |||||
| Sex | n | % | n | % | n | % | n | % | p |
| Male sex | 383 | 19.1 | 275 | 13.8 | 114 | 5.7 | 36 | 1.8 | <0.001 |
| Female sex | 335 | 16.8 | 400 | 20.0 | 290 | 14.5 | 167 | 8.3 | |
| Age range | |||||||||
| ≥60 years | 51 | 2.5 | 23 | 1.1 | 7 | 0.4 | 2 | 0.1 | <0.001 |
| 50–59 years | 92 | 4.6 | 63 | 3.1 | 23 | 1.1 | 9 | 0.4 | |
| 40–49 years | 172 | 8.6 | 137 | 6.9 | 71 | 3.5 | 28 | 1.4 | |
| 30–39 years | 251 | 12.6 | 230 | 11.5 | 144 | 7.2 | 59 | 2.9 | |
| 18–29 years | 152 | 7.6 | 222 | 11.1 | 159 | 8.0 | 105 | 5.3 | |
| Body mass index | |||||||||
| Obesity | 86 | 4.3 | 85 | 4.3 | 58 | 2.9 | 33 | 1.7 | 0.667 |
| Overweight | 270 | 13.5 | 252 | 12.6 | 127 | 6.3 | 60 | 3.0 | |
| Normal weight | 351 | 17.5 | 326 | 16.3 | 210 | 10.5 | 103 | 5.1 | |
| Underweight | 11 | 0.5 | 12 | 0.6 | 9 | 0.40 | 7 | 0.4 | |
| Objective with PA | |||||||||
| Others | 42 | 2.1 | 32 | 1.6 | 36 | 1.8 | 19 | 0.9 | 0.273 |
| Sports performance | 101 | 5.1 | 69 | 3.5 | 33 | 1.7 | 22 | 1.1 | |
| Conditioning | 158 | 7.9 | 154 | 7.7 | 81 | 4.0 | 37 | 1.8 | |
| Slimming | 58 | 2.9 | 98 | 4.9 | 80 | 4.0 | 49 | 2.5 | |
| Health | 359 | 17.9 | 322 | 16.1 | 174 | 8.7 | 76 | 3.8 | |
| Activities before the pandemic | |||||||||
| Others | 169 | 8.5 | 179 | 8.9 | 110 | 5.5 | 69 | 3.5 | 0.196 |
| Race group | 35 | 1.8 | 25 | 1.3 | 14 | 0.7 | 8 | 0.4 | |
| Running advice | 57 | 2.9 | 40 | 2.0 | 20 | 1.0 | 6 | 0.3 | |
| Sport practice | 135 | 6.8 | 116 | 5.8 | 61 | 3.0 | 27 | 1.4 | |
| Gym | 322 | 16.1 | 315 | 15.8 | 199 | 10.0 | 93 | 4.7 | |
| PA frequency before distancing | |||||||||
| 6 to 7 times a week | 178 | 8.9 | 120 | 6.0 | 58 | 2.9 | 27 | 1.4 | <0.001 |
| 4 to 5 times a week | 272 | 13.6 | 252 | 11.6 | 138 | 6.9 | 71 | 3.5 | |
| 3 times a week | 140 | 7.0 | 144 | 7.2 | 84 | 4.2 | 37 | 1.8 | |
| 1 or 2 times a week | 72 | 3.6 | 96 | 4.8 | 67 | 3.4 | 35 | 1.8 | |
| I did not practice | 56 | 2.8 | 63 | 3.1 | 57 | 2.9 | 33 | 1.7 | |
| Frequency of meals before departure | |||||||||
| 5 or + meals a day | 219 | 10.9 | 184 | 9.2 | 102 | 5.1 | 58 | 2.9 | 0.032 |
| 3 to 4 meals a day | 453 | 22.7 | 449 | 22.4 | 270 | 13.5 | 122 | 6.1 | |
| 1 to 2 meals a day | 46 | 2.3 | 42 | 2.1 | 32 | 1.6 | 23 | 1.1 | |
| (B) | |||||||||
| During Pandemic | Low Stress | Moderate Stress | High Stress | Very High Stress | |||||
| Do you PA alone? | n | % | n | % | n | % | n | % | p |
| Yes | 558 | 27.9 | 495 | 24.8 | 260 | 13.0 | 117 | 5.9 | <0.001 |
| No | 160 | 8.0 | 180 | 9.0 | 144 | 7.2 | 86 | 4.3 | |
| Body mass index (during) | |||||||||
| Obesity | 87 | 4.3 | 86 | 4.3 | 63 | 3.1 | 36 | 1.8 | 0.713 |
| Overweight | 266 | 13.3 | 254 | 12.7 | 127 | 6.3 | 62 | 3.1 | |
| Normal weight | 356 | 17.8 | 325 | 16.3 | 206 | 10.3 | 98 | 4.9 | |
| Underweight | 9 | 0.4 | 10 | 0.5 | 8 | 0.4 | 7 | 0.4 | |
| PA frequency during distancing | |||||||||
| 6 to 7 times a week | 136 | 6.8 | 72 | 3.6 | 27 | 1.4 | 10 | 0.5 | <0.001 |
| 4 to 5 times a week | 179 | 8.9 | 182 | 9.1 | 80 | 4.0 | 34 | 1.7 | |
| 3 times a week | 167 | 8.3 | 135 | 6.8 | 82 | 4.1 | 37 | 1.8 | |
| 1 or 2 times a week | 127 | 6.3 | 151 | 7.5 | 105 | 5.3 | 44 | 2.2 | |
| I did not practice | 109 | 5.5 | 135 | 6.8 | 110 | 5.5 | 78 | 3.9 | |
| PA level during distancing | |||||||||
| Increased | 127 | 6.3 | 124 | 6.2 | 62 | 3.1 | 27 | 1.4 | 0.009 |
| It remained the same | 169 | 8.5 | 139 | 7.0 | 82 | 4.1 | 36 | 1.8 | |
| Decreased | 422 | 21.1 | 412 | 20.6 | 260 | 13.0 | 140 | 7.0 | |
| Do you follow internet guidelines | |||||||||
| Yes | 309 | 15.4 | 304 | 15.2 | 179 | 8.9 | 88 | 4.4 | 0.800 |
| No | 409 | 20.4 | 371 | 18.6 | 225 | 11.3 | 115 | 5.8 | |
| Which platform | |||||||||
| Facebook® | 7 | 0.4 | 6 | 0.3 | 4 | 0.2 | 2 | 0.1 | 0.999 |
| Others | 86 | 4.3 | 80 | 4.0 | 50 | 2.5 | 17 | 0.9 | |
| YouTube® | 55 | 2.8 | 62 | 3.1 | 30 | 1.5 | 16 | 0.8 | |
| Instagram® | 72 | 3.6 | 79 | 4.0 | 56 | 2.8 | 30 | 1.5 | |
| Mobile App | 89 | 4.5 | 75 | 3.8 | 39 | 1.9 | 23 | 1.1 | |
| None | 409 | 20.4 | 373 | 18.6 | 225 | 11.3 | 115 | 5.8 | |
| Frequency of meals during distancing | |||||||||
| 5 or + meals a day | 189 | 9.4 | 196 | 9.8 | 137 | 6.9 | 75 | 3.8 | 0.043 |
| 3 to 4 meals a day | 476 | 23.8 | 440 | 22.0 | 245 | 12.3 | 99 | 5.0 | |
| 1 to 2 meals a day | 53 | 2.6 | 39 | 1.90 | 22 | 1.1 | 29 | 1.5 | |
| Greater amount of food per meal during distancing | |||||||||
| Yes | 129 | 6.5 | 189 | 9.4 | 147 | 7.3 | 82 | 4.1 | <0.001 |
| Sometimes | 192 | 9.6 | 221 | 11.1 | 137 | 6.9 | 60 | 3.0 | |
| No | 397 | 19.9 | 265 | 13.3 | 120 | 6.0 | 61 | 3.1 | |
| (A) | |||||||||
| Before Pandemic | Moderate Stress | High Stress | Very High Stress | ||||||
| Sex | OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p |
| Male sex | 1 | 1 | 1 | ||||||
| Female sex | 1.66 | 1.34–2.05 | <0.001 | 2.90 | 2.23–3.77 | <0.001 | 5.30 | 3.59–7.82 | <0.001 |
| Age range | |||||||||
| ≥60 years | 1 | 1 | 1 | ||||||
| 50–59 years | 1.82 | 0.73–4.53 | 0.198 | 1.82 | 0.73–4.53 | 0.198 | 2.49 | 0.51–11.98 | 0.254 |
| 40–49 years | 3.00 | 1.30–6.94 | 0.010 | 3.00 | 1.30–6.94 | <0.001 | 4.15 | 0.95–18.02 | 0.057 |
| 30–39 years | 4.42 | 1.84–9.45 | <0.001 | 4.18 | 1.84–9.45 | <0.001 | 5.99 | 0.41–25.32 | 0.015 |
| 18–29 years | 762 | 3.35–17.31 | <0.001 | 7.62 | 3.35–17.31 | <0.001 | 17.61 | 4.19–73.94 | <0.001 |
| Body mass index | |||||||||
| Obesity | 1 | 1 | 1 | ||||||
| Overweight | 0.94 | 0.66–1.33 | 0.745 | 0.69 | 0.47–1.03 | 0.073 | 0.57 | 0.35–0.94 | 0.029 |
| Normal weight | 0.94 | 0.67–1.31 | 0.716 | 0.88 | 0.61–1.29 | 0.531 | 0.76 | 0.48–1.20 | 0.251 |
| Underweight | 1.10 | 0.46–2.63 | 0.824 | 1.21 | 0.47–3.11 | 0.688 | 1.65 | 0.59–4.64 | 0.335 |
| Objective with PA | |||||||||
| Others | 1 | 1 | 1 | ||||||
| Sport/performance | 0.89 | 0.51–1.55 | 0.699 | 0.38 | 0.21–0.69 | <0.001 | 0.48 | 0.23–0.98 | 0.044 |
| Conditioning | 1.27 | 0.76–2.13 | 0.345 | 0.59 | 0.35–1.00 | 0.052 | 0.51 | 0.277–0.99 | 0.047 |
| Slimming | 2.21 | 1.26–3.89 | 0.006 | 1.60 | 0.92–2.81 | 0.095 | 1.86 | 0.96–3.62 | 0.064 |
| Health | 1.17 | 0.72–1.91 | 0.509 | 0.56 | 0.35–0.91 | 0.020 | 0.46 | 0.25–0.84 | 0.012 |
| Activities before the pandemic | |||||||||
| Others | 1 | - | - | 1 | - | - | 1 | - | - |
| Race group | 0.67 | 0.38–1.17 | 0.164 | 0.61 | 0.31–1.19 | 0.151 | 0.56 | 0.24–1.26 | 0.164 |
| Running advice | 0.66 | 0.42–1.04 | 0.007 | 0.53 | 0.30–0.94 | 0.032 | 0.25 | 0.10–0.62 | 0.003 |
| Sport practice | 0.81 | 0.58–1.12 | 0.207 | 0.69 | 0.47–1.02 | 0.064 | 0.49 | 0.29–0.80 | 0.005 |
| Gym | 0.92 | 0.71–1.20 | 0.551 | 0.94 | 0.70–1.27 | 0.733 | 0.70 | 0.49–1.01 | 0.061 |
| PA frequency before distancing | |||||||||
| 6 to 7 times a week | 1 | 1 | 1 | ||||||
| 4 to 5 times a week | 1.37 | 0.103–1.83 | 0.031 | 1.55 | 1.08–2.23 | 0.016 | 1.72 | 1.06–2.78 | 0.027 |
| 3 times a week | 1.52 | 1.09–2.11 | 0.012 | 1.84 | 1.23–2.75 | 0.003 | 1.74 | 1.01–3.00 | 0.045 |
| 1 or 2 times a week | 1.97 | 1.34–2.90 | 0.001 | 2.85 | 1.82–4.45 | <0.001 | 3.20 | 1.80–5.67 | <0.001 |
| I did not practice | 1.66 | 1.08–2.56 | 0.019 | 3.12 | 1.94–5.01 | <0.001 | 3.88 | 2.15–7.01 | <0.001 |
| Frequency of meals before departure | |||||||||
| 5 or + meals a day | 1 | 1 | 1 | ||||||
| 3 to 4 meals a day | 1.18 | 0.93–1.49 | 0.169 | 1.28 | 0.96–1.69 | 0.083 | 1.01 | 0.71–1.44 | 0.926 |
| 1 to 2 meals a day | 1.08 | 0.68–1.72 | 0.724 | 1.49 | 0.89–2.48 | 0.122 | 1.88 | 1.05–3.36 | 0.031 |
| (B) | |||||||||
| During Pandemic | Moderate Stress | High Stress | Very High Stress | ||||||
| Do you PA alone | OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p |
| Yes | 1 | 1 | 1 | ||||||
| No | 1.26 | 0.99–1.62 | 0.057 | 1.93 | 1.47–2.52 | <0.001 | 2.56 | 1.84–3.56 | <0.001 |
| Body mass index (during) | |||||||||
| Obesity | 1 | 1 | 1 | ||||||
| Overweight | 0.96 | 0.68–1.36 | 0.966 | 0.65 | 0.44–0.97 | 0.035 | 0.56 | 0.35–0.90 | 0.018 |
| Normal weight | 0.92 | 0.66–1.29 | 0.640 | 0.79 | 0.55–1.15 | 0.231 | 0.66 | 0.42–1.04 | 0.075 |
| Underweight | 1.12 | 0.4–2.90 | 0.809 | 1.22 | 0.44–3.35 | 0.690 | 1.88 | 0.65–5.43 | 0.244 |
| PA frequency during distancing | |||||||||
| 6 to 7 times a week | 1 | 1 | 1 | ||||||
| 4 to 5 times a week | 1.92 | 1.35–2.73 | <0.001 | 2.25 | 1.37–3.67 | <0.001 | 2.58 | 1.23–5.41 | 0.012 |
| 3 times a week | 1.52 | 1.06–2.19 | 0.023 | 2.47 | 1.51–4.03 | <0.001 | 3.01 | 1.44–6.28 | 0.003 |
| 1 or 2 times a week | 2.24 | 1.55–3.25 | <0.001 | 4.16 | 2.55–6.77 | <0.001 | 4.71 | 2.27–9.75 | <0.001 |
| I did not practice | 2.33 | 1.59–3.42 | <0.001 | 5.08 | 3.11–8.30 | <0.001 | 9.73 | 4.80–19.69 | <0.001 |
| PA level during distancing | |||||||||
| Increased | 1 | 1 | 1 | ||||||
| It remained the same | 0.84 | 0.60–1.17 | 0.314 | 0.99 | 0.66–1.48 | 0.976 | 1.00 | 0.57–1.73 | 0.994 |
| Decreased | 1.00 | 0.75–1.32 | 1.000 | 1.262 | 0.89–1.77 | 0.181 | 1.56 | 0.98–2.46 | 0.056 |
| Do you follow internet guidelines | |||||||||
| Yes | 1 | 1 | 1 | ||||||
| No | 0.92 | 0.74–1.13 | 0.452 | 0.95 | 0.74–1.21 | 0.680 | 0.98 | 0.72–1.35 | 0.937 |
| Which platform | |||||||||
| Facebook® | 1 | 1 | 1 | ||||||
| Others | 1.09 | 0.35–3.36 | 0.887 | 1.01 | 0.28–3.64 | 0.979 | 0.69 | 0.13–3.62 | 0.663 |
| YouTube® | 1.31 | 0.41–4.15 | 0.640 | 0.95 | 0.25–3.52 | 0.944 | 1.01 | 0.19–5.39 | 0.983 |
| Instagram® | 1.28 | 0.41–3.98 | 0.670 | 1.36 | 0.38–4.88 | 0.636 | 0.15 | 0.28–7.42 | 0.650 |
| Mobile App | 0.98 | 0.31–0.31 | 0.977 | 0.76 | 0.21–2.77 | 0.686 | 0.90 | 0.17–4.64 | 0.904 |
| None | 1.06 | 0.35–3.19 | 0.912 | 0.96 | 0.27–3.32 | 0.952 | 0.98 | 0.20–4.80 | 0.984 |
| Frequency of meals during distancing | |||||||||
| 5 or more meals a day | 1 | 1 | 1 | ||||||
| 3 to 4 meals a day | 0.89 | 0.70–1.13 | 0.344 | 0.71 | 0.54–0.92 | 0.012 | 0.52 | 0.37–0.73 | <0.001 |
| 1 to 2 meals a day | 0.71 | 0.44–1.12 | 0.143 | 0.57 | 0.33–0.98 | 0.044 | 1.37 | 0.81–2.33 | 0.231 |
| Greater amount of food per meal during distancing | |||||||||
| Yes | 1 | 1 | 1 | ||||||
| Sometimes | 0.78 | 0.58–1.05 | 0.110 | 0.62 | 0.45–0.86 | 0.004 | 0.49 | 0.32–0.73 | <0.001 |
| No | 0.45 | 0.34–0.59 | <0.001 | 0.26 | 0.19–0.36 | <0.001 | 0.24 | 0.16–0.35 | <0.001 |
| (A) | |||||||||
| Before Pandemic | Moderate Stress | High Stress | Very High Stress | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Sex a | OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p |
| Male sex | 1 | 1 | 1 | ||||||
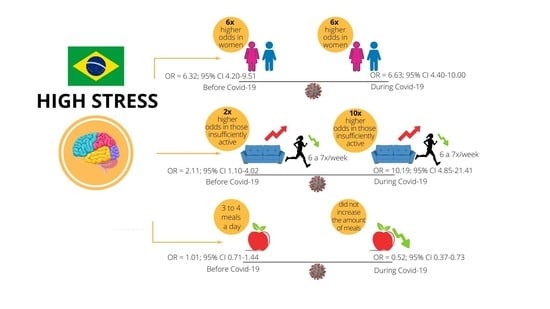
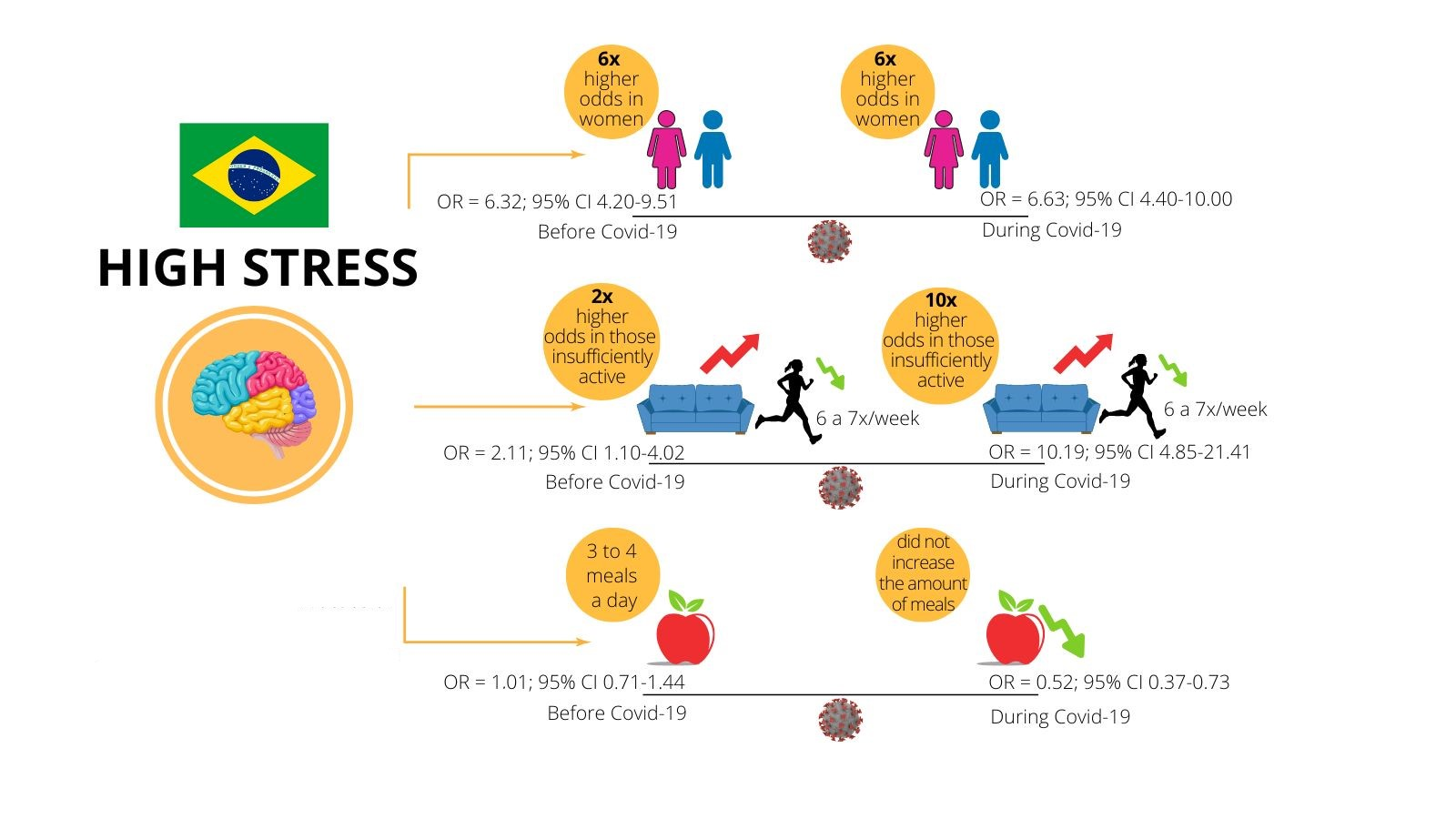
| Female sex | 1.81 | 1.45–2.27 | <0.001 | 3.25 | 2.46–4.29 | <0.001 | 6.32 | 4.20–9.51 | <0.001 |
| Objective with PA b | |||||||||
| Others | 1 | 1 | 1 | ||||||
| Sports performance | 1.05 | 0.60–1.86 | 0.843 | 0.52 | 0.28–0.97 | 0.041 | 0.81 | 0.37–1.73 | 0.591 |
| Conditioning | 1.33 | 0.79–2.25 | 0.274 | 0.68 | 0.39–1.17 | 0.166 | 0.67 | 0.34–1.35 | 0.270 |
| Slimming | 1.77 | 0.99–3.18 | 0.052 | 1.16 | 0.64–2.11 | 0.616 | 1.24 | 0.60–2.55 | 0.554 |
| Health | 1.28 | 0.78–2.10 | 0.325 | 0.66 | 0.40–1.09 | 0.110 | 0.62 | 0.33–1.17 | 0.144 |
| Activities before the pandemic b | |||||||||
| Others | 1 | 1 | 1 | ||||||
| Race group | 0.86 | 0.48–1.52 | 0.610 | 0.92 | 0.46–1.85 | 0.828 | 1.03 | 0.43–2.46 | 0.941 |
| Running advice | 0.88 | 0.55–1.41 | 0.612 | 0.90 | 0.50–1.63 | 0.743 | 0.57 | 0.22–1.44 | 0.239 |
| Sport practice | 0.87 | 0.62–1.22 | 0.419 | 0.81 | 0.54–1.23 | 0.334 | 0.63 | 0.36–1.07 | 0.890 |
| Gym | 0.97 | 0.73–1.27 | 0.830 | 1.08 | 0.79–1.49 | 0.612 | 0.86 | 0.58–1.27 | 0.463 |
| PA frequency before distancing b | |||||||||
| 6 to 7 times a week | 1 | 1 | 1 | ||||||
| 4 to 5 times a week | 1.34 | 0.99–1.81 | 0.053 | 1.50 | 1.02–2.19 | 0.036 | 1.69 | 1.01–2.82 | 0.044 |
| 3 times a week | 1.41 | 1.00–2.01 | 0.050 | 1.62 | 1.05–2.49 | 0.028 | 1.52 | 0.85–2.73 | 0.157 |
| 1 or 2 times a week | 1.81 | 1.20–2.72 | 0.004 | 2.42 | 1.49–3.91 | <0.001 | 2.55 | 1.37–4.74 | 0.003 |
| I did not practice | 1.34 | 0.85–2.12 | 0.205 | 2.05 | 1.23–3.43 | 0.006 | 2.11 | 1.10–4.02 | 0.023 |
| (B) | |||||||||
| During Pandemic | Moderate Stress | High Stress | Very High Stress | ||||||
| Sex a | OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p |
| Male sex | 1 | 1 | 1 | ||||||
| Female sex | 1.82 | 1.45–2.28 | <0.001 | 3.28 | 2.48–4.32 | <0.001 | 6.63 | 4.40–10.00 | <0.001 |
| Do you PA alone b | |||||||||
| Yes | 1 | 1 | 1 | ||||||
| No | 1.23 | 0.95–1.58 | 0.107 | 1.83 | 1.37–2.43 | <0.001 | 2.18 | 1.52–3.11 | <0.001 |
| PA frequency during distancing b | |||||||||
| 6 to 7 times a week | 1 | 1 | 1 | ||||||
| 4 to 5 times a week | 2.02 | 1.41–2.90 | <0.001 | 2.53 | 1.52–4.21 | <0.001 | 3.18 | 1.47–6.86 | 0.003 |
| 3 times a week | 1.66 | 1.14–2.43 | 0.008 | 2.98 | 1.78–4.96 | <0.001 | 4.16 | 1.93–8.94 | <0.001 |
| 1 or 2 times a week | 2.30 | 1.57–3.38 | <0.001 | 4.45 | 2.67–7.40 | <0.001 | 5.19 | 2.43–11.09 | <0.001 |
| I did not practice | 2.44 | 1.64–3.63 | <0.001 | 5.50 | 3.28–9.22 | <0.001 | 10.19 | 4.85–21.41 | <0.001 |
| PA level during distancing b | |||||||||
| Increased | 1 | 1 | 1 | ||||||
| It remained the same | 0.93 | 0.66–1.31 | 0.707 | 1.18 | 0.77–1.80 | 0.435 | 1.27 | 0.71–2.27 | 0.421 |
| Decreased | 1.13 | 0.85–1.51 | 0.388 | 1.59 | 1.11–2.28 | 0.010 | 2.28 | 1.40–3.71 | <0.001 |
| Do you follow internet guidelines b | |||||||||
| Yes | 1 | 1 | 1 | ||||||
| No | 1.05 | 0.84–1.31 | 0.665 | 1.22 | 0.94–1.59 | 0.130 | 1.31 | 0.93–1.85 | 0.114 |
| Which platform b | |||||||||
| Facebook® | 1 | 1 | 1 | ||||||
| Others | 1.03 | 0.32–3.25 | 0.957 | 0.84 | 0.22–0.31 | 0.806 | 0.48 | 0.08–2.78 | 0.418 |
| YouTube® | 1.15 | 0.35–3.69 | 0.813 | 0.68 | 0.17–2.66 | 0.590 | 0.62 | 0.10–3.61 | 0.595 |
| Instagram® | 1.14 | 0.36–3.61 | 0.823 | 1.00 | 0.26–3.79 | 0.990 | 0.91 | 0.16–5.10 | 0.915 |
| Mobile app | 0.92 | 0.29–2.91 | 0.889 | 0.62 | 0.16–2.35 | 0.483 | 0.63 | 0.11–3.58 | 0.605 |
| None | 1.11 | 0.36–3.40 | 0.847 | 0.97 | 0.27–3.52 | 0.971 | 0.88 | 0.16–4.70 | 0.881 |
| Greater amount of food per meal during distancing b | |||||||||
| Yes | 1 | 1 | 1 | ||||||
| Sometimes | 0.74 | 0.54–1.00 | 0.051 | 0.57 | 0.41–0.80 | <0.001 | 0.41 | 0.27–0.64 | <0.001 |
| No | 0.49 | 0.37–0.65 | <0.001 | 0.31 | 0.22–0.43 | <0.001 | 0.28 | 0.18–0.43 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Camargo, E.M.; López-Gil, J.F.; Piola, T.S.; Pechnicki dos Santos, L.; de Borba, E.F.; de Campos, W.; Gregorio da Silva, S. Association of the Practice of Physical Activity and Dietary Pattern with Psychological Distress before and during COVID-19 in Brazilian Adults. Nutrients 2023, 15, 1926. https://doi.org/10.3390/nu15081926
de Camargo EM, López-Gil JF, Piola TS, Pechnicki dos Santos L, de Borba EF, de Campos W, Gregorio da Silva S. Association of the Practice of Physical Activity and Dietary Pattern with Psychological Distress before and during COVID-19 in Brazilian Adults. Nutrients. 2023; 15(8):1926. https://doi.org/10.3390/nu15081926
Chicago/Turabian Stylede Camargo, Edina Maria, José Francisco López-Gil, Thiago Silva Piola, Letícia Pechnicki dos Santos, Edilson Fernando de Borba, Wagner de Campos, and Sergio Gregorio da Silva. 2023. "Association of the Practice of Physical Activity and Dietary Pattern with Psychological Distress before and during COVID-19 in Brazilian Adults" Nutrients 15, no. 8: 1926. https://doi.org/10.3390/nu15081926
APA Stylede Camargo, E. M., López-Gil, J. F., Piola, T. S., Pechnicki dos Santos, L., de Borba, E. F., de Campos, W., & Gregorio da Silva, S. (2023). Association of the Practice of Physical Activity and Dietary Pattern with Psychological Distress before and during COVID-19 in Brazilian Adults. Nutrients, 15(8), 1926. https://doi.org/10.3390/nu15081926