
Clinical Outcomes of the Deleterious Effects of Aluminum on Neuro-Cognition, Inflammation, and Health: A Review

 ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Study Design
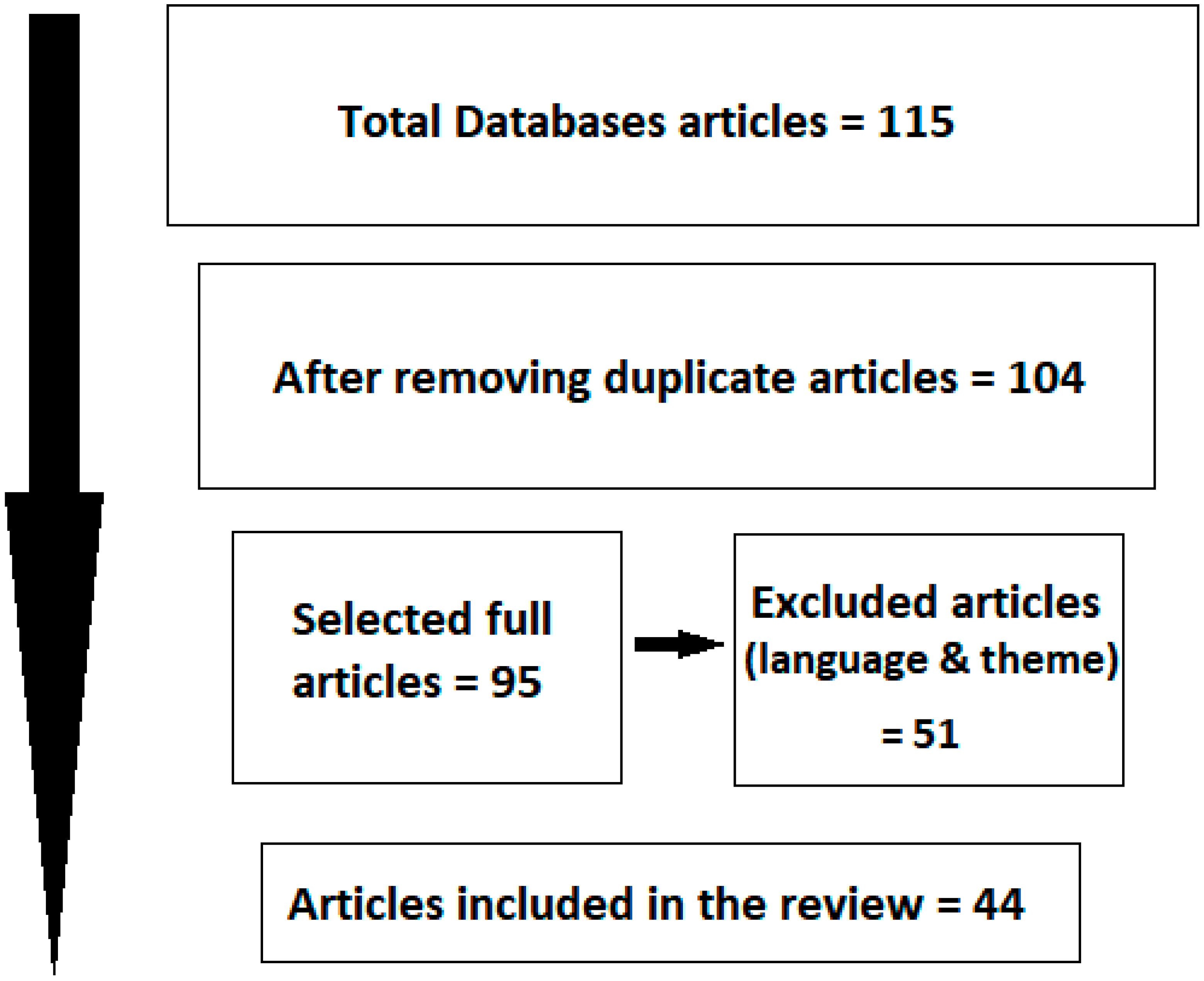
2.2. Search Strategy and Search Sources
3. Results and Discussion
3.1. Summary of Findings
3.2. Toxicity—Inflammation and Associated Impacts
3.3. Neurotoxicity and Cancer
3.4. Absorption
3.5. Diagnostic Test and Excretion
3.6. Chelation Therapy
4. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Vignal, C.; Desreumaux, P.; Body-Malapel, M. Gut: An underestimated target organ for Aluminum. Morphologie 2016, 100, 75–84. [Google Scholar] [CrossRef]
- Anonymous. Is aluminium a dementing ion? Lancet 1992, 339, 713–714. [Google Scholar] [CrossRef]
- Alasfar, R.H.; Isaifan, R.J. Aluminum environmental pollution: The silent killer. Environ. Sci. Pollut. Res. Int. 2021, 28, 44587–44597. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Huan, J.; Gao, D.; Xu, S.; Han, X.; Song, J.; Wang, L.; Zhang, H.; Niu, Q.; Lu, X. Blood pressure mediated the effects of cognitive function impairment related to aluminum exposure in Chinese aluminum smelting workers. Neurotoxicology 2022, 91, 269–281. [Google Scholar] [CrossRef]
- Niu, Q. Overview of the Relationship Between Aluminum Exposure and Health of Human Being. Adv. Exp. Med. Biol. 2018, 1091, 1–31. [Google Scholar] [CrossRef]
- Oliveira, R.B.; Barreto, F.C.; Nunes, L.A.; Custódio, M.R. Aluminum Intoxication in Chronic Kidney Disease. J. Bras. Nefrol. 2021, 43 (Suppl. S1), 660–664. [Google Scholar] [CrossRef] [PubMed]
- Berillo, D. Comparative Toxicity of Interferon Beta-1a Impurities of Heavy Metal Ions. Medicina 2022, 58, 463. [Google Scholar] [CrossRef]
- Djouina, M.; Waxin, C.; Leprêtre, F.; Tardivel, M.; Tillement, O.; Vasseur, F.; Figeac, M.; Bongiovanni, A.; Sebda, S.; Desreumaux, P.; et al. Gene/environment interaction in the susceptibility of Crohn’s disease patients to aluminum. Sci. Total Environ. 2022, 850, 158017. [Google Scholar] [CrossRef]
- Hao, N.P.; Zhang, L.F. Research progress of epigenetic regulation in the pathogenesis of aluminum exposure. Zhonghua Yu Fang Yi Xue Za Zhi 2022, 56, 240–244. (In Chinese) [Google Scholar] [CrossRef]
- Igbokwe, I.O.; Igwenagu, E.; Igbokwe, N.A. Aluminium toxicosis: A review of toxic actions and effects. Interdiscip. Toxicol. 2019, 12, 45–70. [Google Scholar] [CrossRef]
- Paul-Ehrlich-Institut. Sicherheitsbewertung von Aluminium in Therapieallergenen. Available online: www.pei.de/DE/arzneimittelsicherheit-vigilanz/archivsicherheitsinformationen (accessed on 19 November 2022).
- Deutsche Dermatologische Gesellschaft. Definition und Therapie der Primären Hyperhidrose. S1-Leitlinie vom 15.1.2012. AWMF-Register Nr. 013/059. Available online: www.awmf.org/leitlinien (accessed on 19 November 2022).
- Willhite, C.C.; Karyakina, N.A.; Yokel, R.A.; Yenugadhati, N.; Wisniewski, T.M.; Arnold, I.M.; Momoli, F.; Krewski, D. Systematic review of potential health risks posed by pharmaceutical, occupational and consumer exposures to metallic and nanoscale aluminum, aluminum oxides, aluminum hydroxide and its soluble salts. Crit. Rev. Toxicol. 2014, 44, 1–80. [Google Scholar] [CrossRef]
- IARC (International Agency For Research On Cancer) Occupational Exposures during Aluminium Production. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. No. 100F. Lyon (FR) 2012. Available online: https://monographs.iarc.fr/ENG/Monographs/vol100F/mono100F22.pdf (accessed on 19 November 2022).
- WHO Joint FAO/WHO Expert Committee on Food Additives. Safety Evaluation of Certain Food Additives and Contaminants. Available online: http://apps.who.int/iris/bitstream/10665/44788/1/WHO_TRS_966_eng.pdf (accessed on 19 November 2022).
- Rifat, S.L. Aluminium hypothesis lives. Lancet 1994, 343, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Klotz, K.; Weistenhöfer, W.; Neff, F.; Hartwig, A.; van Thriel, C.; Drexler, H. The Health Effects of Aluminum Exposure. Dtsch. Arztebl. Int. 2017, 114, 653–659. [Google Scholar] [CrossRef]
- Arnich, N.; Sirot, V.; Rivière, G.; Jean, J.; Noël, L.; Guérin, T.; Leblanc, J.C. Dietary exposure to trace elements and health risk assessment in the 2nd French Total Diet Study. Food Chem. Toxicol. 2012, 50, 2432–2449. [Google Scholar] [CrossRef] [PubMed]
- Al Juhaiman, L.A. Estimating Aluminum leaching from Aluminum cook wares in different meat extracts and milk. J. Saudi Chem. Soc. 2010, 14, 131–137. [Google Scholar] [CrossRef]
- Goullé, J.P.; Grangeot-Keros, L. Aluminum and vaccines: Current state of knowledge. Med. Mal. Infect. 2020, 50, 16–21. [Google Scholar] [CrossRef]
- Huat, T.J.; Camats-Perna, J.; Newcombe, E.A.; Valmas, N.; Kitazawa, M.; Medeiros, R. Metal Toxicity Links to Alzheimer’s Disease and Neuroinflammation. J. Mol. Biol. 2019, 431, 1843–1868. [Google Scholar] [CrossRef]
- Jovanova-Nesic, K.; Shoenfeld, Y.; Spector, N.H. Aluminum excytotoxicity and neuroautotoimmunity: The role of the brain expression of CD32+ (FcγRIIa), ICAM-1+ and CD3ξ in aging. Curr. Aging Sci. 2012, 5, 209–217. [Google Scholar] [CrossRef]
- Halvaei, Z.; Tehrani, H.; Soltaninejad, K.; Abdollahi, M.; Shadnia, S. Vitamin E as a novel therapy in the treatment of acute aluminum phosphide poisoning. Turk. J. Med. Sci. 2017, 47, 795–800. [Google Scholar] [CrossRef]
- Ojha, P.; Ojha, C.S.; Sharma, V.P. Influence of physico-chemical factors on leaching of chemical additives from aluminum foils used for packaging of food materials. J. Environ. Sci. Health 2007, 49, 62–66. [Google Scholar]
- Sonego, E.; Di Filippo, P.; Riccardi, C.; Pomata, D.; Bannò, A.; Simonetti, G.; Buiarelli, F. Occurrence and migration study of chemicals from baking paper and aluminium foil. Food Chem. 2023, 409, 135260. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Hao, W.; Liu, Z.; Song, Y.; Hao, C.; Wu, S.; Lu, X.; Yang, J.; Jin, C. Aluminum induces neuroinflammation via P2X7 receptor activating NLRP3 inflammasome pathway. Ecotoxicol. Environ. Saf. 2023, 249, 114373. [Google Scholar] [CrossRef] [PubMed]
- Coulson, J.M.; Hughes, B.W. Dose-response relationships in aluminium toxicity in humans. Clin. Toxicol. 2022, 60, 415–428. [Google Scholar] [CrossRef] [PubMed]
- Fulgenzi, A.; De Giuseppe, R.; Bamonti, F.; Vietti, D.; Ferrero, M.E. Efficacy of chelation therapy to remove aluminium intoxication. J. Inorg. Biochem. 2015, 152, 214–218. [Google Scholar] [CrossRef]
- Inan-Eroglu, E.; Ayaz, A. Is aluminum exposure a risk factor for neurological disorders? J. Res. Med. Sci. 2018, 23, 51. [Google Scholar] [CrossRef]
- Kilburn, K.H. Does exposure to fine aluminium dust affect the brain? Lancet 1999, 354, 1575–1577. [Google Scholar] [CrossRef]
- Abreo, K.; Faugere, M.C.; Smith, A. Prevalence and etiology of aluminum intoxication in non-dialyzed and dialyzed patients with renal failure. Kidney Int. 1983, 23, 141. [Google Scholar]
- Malluche, H.H.; Smith, A.J.; Abreo, K.; Faugere, M.C. The use of deferoxamine in the management of aluminium accumulation in bone in patients with renal failure. N. Engl. J. Med. 1984, 311, 140–144. [Google Scholar] [CrossRef]
- Ganrot, P.O. Metabolism and possible health effects of aluminum. Environ. Health Perspect. 1986, 65, 363–441. [Google Scholar] [CrossRef]
- Pineau, A.; Guillard, O.; Fauconneau, B.; Favreau, F.; Marty, M.H.; Gaudin, A.; Vincent, C.M.; Marrauld, A.; Marty, J.P. In vitro study of percutaneous absorption of aluminum from antiperspirants through human skin in the Franz™ diffusion cell. Inorg. Biochem. 2012, 110, 21–26. [Google Scholar] [CrossRef]
- Wechphanich, S.; Thammarat, P. A survey of metal contamination in blood collection tubes on toxicology assays. Bangk. Med. J. 2017, 13, 5. [Google Scholar] [CrossRef]
- Ogawa, M.; Kayama, F. A study of the association between urinary aluminum concentration and pre-clinical findings among aluminum-handling and non-handling workers. J. Occup. Med. Toxicol. 2015, 10, 13–17. [Google Scholar] [CrossRef]
- Krewski, D.; Yokel, R.A.; Nieboer, E.; Borchelt, D.; Cohen, J.; Harry, J.; Kacew, S.; Lindsay, J.; Mahfouz, A.M.; Rondeau, V. Human health risk assessment for aluminium, aluminium oxide, and aluminium hydroxide. J. Toxicol. Environ. Health B Crit. Rev. 2007, 10 (Suppl. S1), 1–269. [Google Scholar] [CrossRef] [PubMed]
- Berthon, G. Aluminium speciation in relation to aluminium bioavailability, metabolism and toxicity. Coord. Chem. Rev. 2002, 228, 319–341. [Google Scholar] [CrossRef]
- Singh, P.; Mitra, P.; Goyal, T.; Sharma, S.; Purohit, P.; Sharma, P. Levels of lead, aluminum, and zinc in occupationally exposed workers of North-Western India. J. Basic Clin. Physiol. Pharmacol. 2021, 33, 191–197. [Google Scholar] [CrossRef]
- Schifman, R.B.; Luevano, D.R. Aluminum toxicity: Evaluation of 16-year trend among 14 919 patients and 45 480 results. Arch. Pathol. Lab. Med. 2018, 142, 742–746. [Google Scholar] [CrossRef]
- Exley, C. Human exposure to aluminium. Environ. Sci. Process. Impacts 2013, 15, 1807–1816. [Google Scholar] [CrossRef]
- Kusanagi, E.; Takamura, H.; Hoshi, N.; Chen, S.J.; Adachi, M. Levels of Toxic and Essential Elements and Associated Factors in the Hair of Japanese Young Children. Int. J. Environ. Res. Public Health 2023, 20, 1186. [Google Scholar] [CrossRef]
- Abubakar, M.G.; Taylor, A.; Ferns, G.A. The effects of aluminium and selenium supplementation on brain and liver antioxidant status in the rat. Afr. J. Biotechnol. 2004, 3, 88–93. [Google Scholar]
- Cheng, D.; Zhang, X.; Xu, L.; Li, X.; Hou, L.; Wang, C. Protective and prophylactic effects of chlorogenic acid on aluminum-induced acute hepatotoxicity and hematotoxicity in mice. Chem. Biol. Interact. 2017, 273, 125–132. [Google Scholar] [CrossRef]
- Fyiad, A. Aluminium toxicity and oxidative damage reduction by melatonin in rats. Res. J. Appl. Sci. 2007, 3, 1210–1217. [Google Scholar]
- Al-Qayim, M.A.J.; Ghali, L.S.; Al-Azwai, T.S. Comparative effects of propolis and malic acid on hematological parameters of aluminum exposed male rats. Glob. J. Bio-Sci. Biotechnol. 2014, 3, 6–11. [Google Scholar]
- Turkez, H.; Yousef, M.I.; Geyikoglu, F. Propolis prevents aluminium-induced genetic and hepatic damages in rat liver. Food. Chem. Toxicol. 2010, 48, 2741–2746. [Google Scholar] [CrossRef] [PubMed]
- Omar, H.M.; Hassan, K.A.; KH, A.E.S.; EA, A. Aluminium toxicity in rats: The role of tannic acid as antioxidant. Ass. Univ. Bull. Environ. Res. 2003, 6, 1–14. [Google Scholar]
- Sharma, D.R.; Wani, W.Y.; Sunkaria, A.; Kandimalla, R.J.; Sharma, R.K.; Verma, D.; Bal, A.; Gill, K.D. Quercetin attenuates neuronal death against aluminum-induced neurodegeneration in the rat hippocampus. Neuroscience 2006, 324, 163–176. [Google Scholar] [CrossRef]
- Zhu, Y.; Hu, C.; Zheng, P.; Miao, L.; Yan, X.; Li, H.; Wang, Z.; Gao, B.; Li, Y. Ginsenoside Rb1 alleviates aluminum chloride-induced rat osteoblasts dysfunction. Toxicology 2016, 368, 183–188. [Google Scholar] [CrossRef]
- Ferreira, A.O.; Freire, É.S.; Polonini, H.C.; Da Silva, P.J.L.C.; Brandão, M.A.F.; Raposo, N.R.B. Anti-Aging Effects of Monomethylsilanetriol and Maltodextrin-Stabilized Orthosilicic Acid on Nails, Skin and Hair. Cosmetics 2018, 5, 41. [Google Scholar] [CrossRef]
- Farooq, M.A.; Dietz, K.J. Silicon as Versatile Player in Plant and Human Biology: Overlooked and Poorly Understood. Front. Plant Sci. 2015, 6, 994. [Google Scholar] [CrossRef]
- Jugdaohsingh, R.; Hui, M.; Anderson, S.H.; Kinrade, S.D.; Powell, J.J. The silicon supplement ‘Monomethylsilanetriol’ is safe and increases the body pool of silicon in healthy Pre-menopausal women. Nutr. Metab. 2013, 10, 37. [Google Scholar] [CrossRef]
- Rahimzadeh, M.R.; Rahimzadeh, M.R.; Kazemi, S.; Amiri, R.J.; Pirzadeh, M.; Moghadamnia, A.A. Aluminum Poisoning with Emphasis on Its Mechanism and Treatment of Intoxication. Emerg. Med. Int. 2022, 2022, 1480553. [Google Scholar] [CrossRef]


{kind=link}
| Detrimental Effects | References |
|---|---|
| Oxidative stress and lipid peroxidation | Willhite, 2014 [13]; Zhang et al., 2022 [4] |
| Protein denaturation and disturbance | Igbokwe, 2019 [10]; Paul-ehrlich-institut, 2022 [11] |
| Enzymatic/Receptor function disturbance: stimulation or inhibition | Zhu, 2023 [26] |
| Amyloidogenic and anti-amyloidolytic action | Huat, 2019 [21] |
| Metalloestrogen action: promoting augmented proliferation and migration of breast cancer cells | IARC, 2012 [14] |
| Disrupts receptor function and cell membrane | Willhite, 2014 [13] |
| Increases osteoclastic activity and reduces osteoblastic activity, inhibiting bone formation and mineralization | Coulson, 2022 [27] |
| Alter gastrointestinal tract homeostasis (permeability regulation, gut microbiota, and gut immune function) | Vignal et al., 2016 [1] |
| Induces arterial hypertension (systolic and arterial) | Zhang et al., 2022 [4] |
| Parameter | Levels |
|---|---|
| Daily dietary intake of Al | 1.6–13 mg (0.2–1.5 mg/kg BW/week) (Igbokwe, et al., 2019) [10] |
| Absorption | 0.1% of the total Al orally ingested absorbed by GIT (Igbokwe, et al., 2019) [10] |
| Tolerable weekly intake | 1 mg Al/kg body weight (EFSA) [33] |
| Diagnostic tests: urine blood serum | 55 μg/g of creatinine (Oliveira, et al., 2021) [6] 10 mcg/L or 60 mcg/L (dialytic patients) (Oliveira, et al., 2021) [6] |
| Toxicity tests: urine blood serum | ranging from 100–108 to 162 mcg/L (Wechphanich & Thammarat. 2007) [35] concentrations higher than 100 mcg/L (Ogawa & Kayama. 2015) [36] |
| Main Excretion mechanisms: urine Bile | 95–99% (Krewski, 2007) [37] 1–2% (Berthon, 2002) [38] |
| Antioxidant/Chelant | Physiological Effects |
|---|---|
| Chow supplemented with 1 mg/kg selenium as sodium selenite daily (Abubakar, et al., 2004) [43]. | Treatment with a selenium-rich diet was associated with a significant reduction of Al in the liver and brain of animal models after infusion of an aqueous solution with Al at a dose of 5 mg/kg per day, five times a week for three weeks. |
| Injected (i.p.) CGA (2 h after Al-treatment, a single dose of 100 mg/kg) and CGA (administered to mice daily for 5 days at 30 mg/kg before Al-treatment) (Cheng, et al., 2017) [44]. | CGA (5-O-caffeoylquinic acid) prevented induced oxidative damaging effects, hepatotoxicity and hematotoxicity of single injection (i.p.) of 25 mg AlCl3 in mice. |
| Pretreatment (30min before AlCl3) with oral melatonin (200 μg/kg body weight) (Fyiad, et al., 2007) [45]. | Melatonin (200 μg/kg body weight) 30 min prior to aluminum chloride AlCl3 orally (8.5 mg/kg body weight for eight weeks) was associated with a decline in all abnormal changes observed in AlCl3 treated rats-oxidative damage and Al-toxicity induced injury to liver, kidney and brain. |
| Oral propolis (50 mg/kg body weight) (Al-Qayim et al., 2014) [46]. | Propolis reduced the significant negative elevation of kidney function parameters in rats presented by the oral AlCl3 (50 mg /kg body weight) for 60 days. |
| Oral propolis (50 mg/kg body weight) (Turkez, et al., 2010) [47]. | Propolis significantly modulated the hepatic toxic effects of oral AlCl3 (34 mg/kg body weight) 30 days in rats. |
| Oral acid malic (45 mg/kg body weight) (Al-Qayim et al., 2014) [46]. | Acid malic reduced the significant negative elevation of kidney function parameters in rats presented by the oral AlCl3 (50 mg /kg body weight) for 60 days. |
| Oral tannic acid (50 mg/kg body weight) (Omar, et al., 2003) [48]. | Tannic acid partially improves the moderate toxicity on liver, kidneys and spleen of treated rats with oral AlCl3 (50 mg /kg body weight) for 80 days. |
| Oral quercetin (10 mg/kg body body weight) (Sharma, et al., 2016) [49]. | Quercetin attenuates neuronal death against oral Al lactate-induced (10 mg /kg body weight) neurodegeneration in rats for 12 weeks. |
| Cell culture added ginsenoside Rb1 (0.0145 mg/Ml) (Zhu, et al., 2016) [50]. | After 24 h of culture, ginsenoside Rb1 alleviates AlCl3-induced (0.126 mg/mL) rat osteoblasts dysfunction. |
| Human studies | |
| Vitamin E (400 mg/BD/intra muscular) (Halvaei et al., 2017) [23]. | DL-alpha tocopheryl acetate significantly decreased the plasma MDA level. |
| Oral monomethysilanetriol (10mg/day) (Ferreira, et al., 2018) [51]. | The supplementation of MMST can lead to a decrease of 53% in aluminum levels 150 days in humans. |
| Intravenous EDTA (2 g/10 mL diluted in 500 mL physiological saline administered in 2 h) (Fulgenzi, 2015) [28]. | EDTA removes Al in urine samples collected from patients over 12h after the procedure. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Renke, G.; Almeida, V.B.P.; Souza, E.A.; Lessa, S.; Teixeira, R.L.; Rocha, L.; Sousa, P.L.; Starling-Soares, B. Clinical Outcomes of the Deleterious Effects of Aluminum on Neuro-Cognition, Inflammation, and Health: A Review. Nutrients 2023, 15, 2221. https://doi.org/10.3390/nu15092221
Renke G, Almeida VBP, Souza EA, Lessa S, Teixeira RL, Rocha L, Sousa PL, Starling-Soares B. Clinical Outcomes of the Deleterious Effects of Aluminum on Neuro-Cognition, Inflammation, and Health: A Review. Nutrients. 2023; 15(9):2221. https://doi.org/10.3390/nu15092221
Chicago/Turabian StyleRenke, Guilherme, Vanessa Borges Pinheiro Almeida, Everton Almeida Souza, Suzana Lessa, Raila Linhares Teixeira, Leticia Rocha, Pamela Lopes Sousa, and Bernardo Starling-Soares. 2023. "Clinical Outcomes of the Deleterious Effects of Aluminum on Neuro-Cognition, Inflammation, and Health: A Review" Nutrients 15, no. 9: 2221. https://doi.org/10.3390/nu15092221
APA StyleRenke, G., Almeida, V. B. P., Souza, E. A., Lessa, S., Teixeira, R. L., Rocha, L., Sousa, P. L., & Starling-Soares, B. (2023). Clinical Outcomes of the Deleterious Effects of Aluminum on Neuro-Cognition, Inflammation, and Health: A Review. Nutrients, 15(9), 2221. https://doi.org/10.3390/nu15092221