
The Association between Caffeine Consumption from Coffee and Tea and Sleep Health in Male and Female Older Adults: A Cross-Sectional Study

Abstract
:1. Introduction
2. Materials and Methods
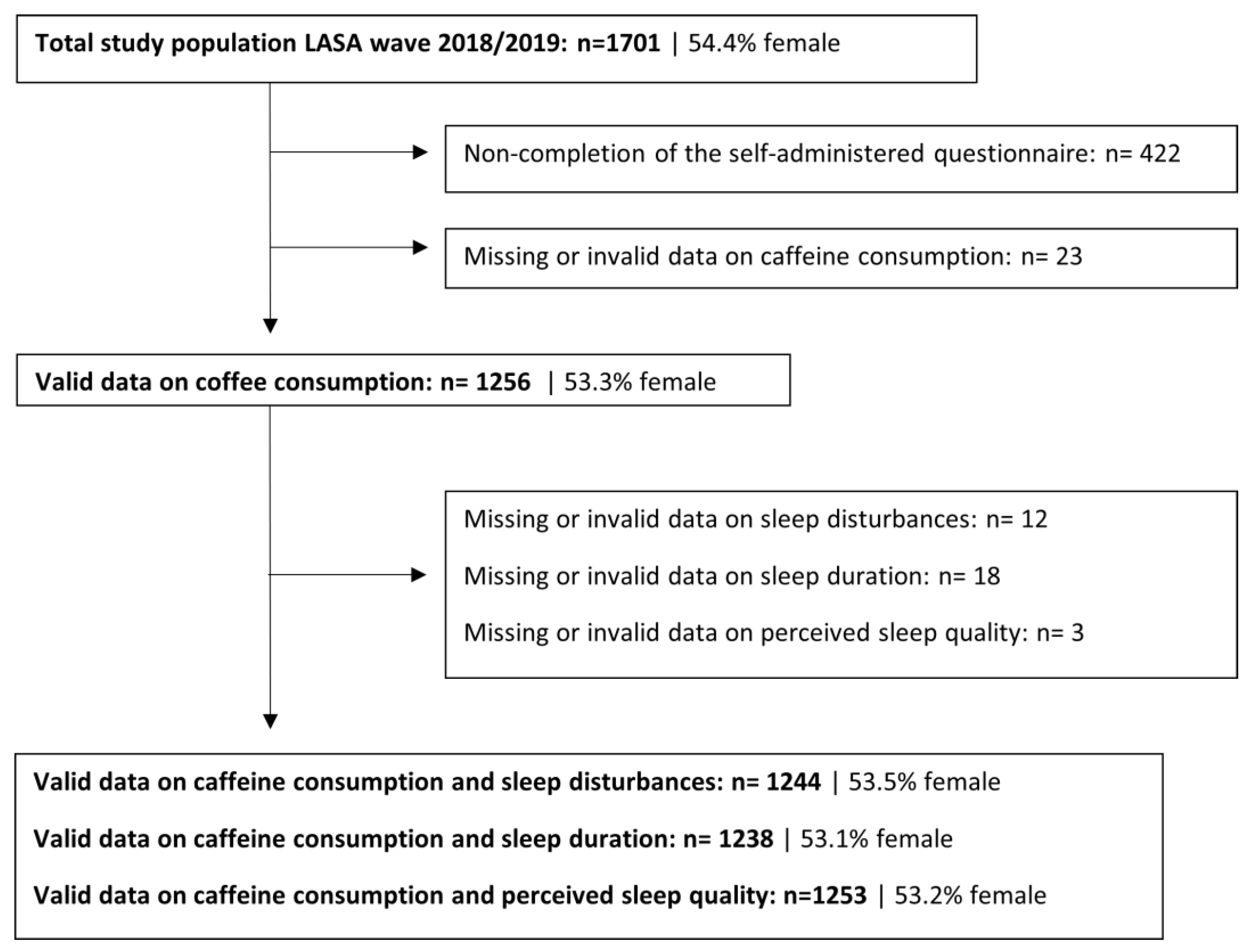
2.1. Design and Participants
2.2. Sleep Disturbances, Sleep Duration, and Perceived Sleep Quality
2.3. Caffeine Consumption from Coffee and Tea
2.4. Other Measurements
2.5. Statistical Analyses
3. Results
3.1. Sample Characteristics
3.2. Association between Caffeine Consumption and Sleep Health Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Luyster, F.S.; Strollo, P.J., Jr.; Zee, P.C.; Walsh, J.K. Boards of Directors of the American Academy of Sleep M, the Sleep Research S. Sleep: A health imperative. Sleep 2012, 35, 727–734. [Google Scholar] [CrossRef] [PubMed]
- Watson, N.F.; Badr, M.S.; Belenky, G.; Bliwise, D.L.; Buxton, O.M.; Buysse, D.; Dinges, D.F.; Gangwisch, J.; Grandner, M.A.; Kushida, C. Joint Consensus Statement of the American Academy of Sleep Medicine and Sleep Research Society on the Recommended Amount of Sleep for a Healthy Adult: Methodology and Discussion. Sleep 2015, 38, 1161–1183. [Google Scholar] [CrossRef] [PubMed]
- Foley, D.; Ancoli-Israel, S.; Britz, P.; Walsh, J. Sleep disturbances and chronic disease in older adults: Results of the 2003 National Sleep Foundation Sleep in America Survey. J. Psychosom. Res. 2004, 56, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Gulia, K.K.; Kumar, V.M. Sleep disorders in the elderly: A growing challenge. Psychogeriatrics 2018, 18, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Ohayon, M.M. Epidemiology of insomnia: What we know and what we still need to learn. Sleep. Med. Rev. 2002, 6, 97–111. [Google Scholar] [CrossRef] [PubMed]
- Kocevska, D.; Lysen, T.S.; Dotinga, A.; Koopman-Verhoef, M.E.; Luijk, M.P.; Antypa, N.; Biermasz, N.; Blokstra, A.; Brug, J.; Burk, W.J.; et al. Sleep characteristics across the lifespan in 1.1 million people from the Netherlands, United Kingdom and United States: A systematic review and meta-analysis. Nat. Hum. Behav. 2021, 5, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.E.; Ju, Y.J.; Park, E.-C.; Lee, S.Y. Effect of poor sleep quality on subjective cognitive decline (SCD) or SCD-related functional difficulties: Results from 220,000 nationwide general populations without dementia. J. Affect. Disord. 2019, 260, 32–37. [Google Scholar] [CrossRef]
- Hokett, E.; Arunmozhi, A.; Campbell, J.; Verhaeghen, P.; Duarte, A. A systematic review and meta-analysis of individual differences in naturalistic sleep quality and episodic memory performance in young and older adults. Neurosci. Biobehav. Rev. 2021, 127, 675–688. [Google Scholar] [CrossRef]
- Li, M.; Wang, N.; Dupre, M.E. Association between the self-reported duration and quality of sleep and cognitive function among middle-aged and older adults in China. J. Affect. Disord. 2022, 304, 20–27. [Google Scholar] [CrossRef]
- Robbins, R.; Quan, S.F.; Weaver, M.D.; Bormes, G.; Barger, L.K.; Czeisler, C.A. Examining sleep deficiency and disturbance and their risk for incident dementia and all-cause mortality in older adults across 5 years in the United States. Aging 2021, 13, 3254–3268. [Google Scholar] [CrossRef]
- Casagrande, M.; Forte, G.; Favieri, F.; Corbo, I. Sleep Quality and Aging: A Systematic Review on Healthy Older People, Mild Cognitive Impairment and Alzheimer’s Disease. Int. J. Environ. Res. Public Health 2022, 19, 8457. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Chen, S.J.; Ma, M.Y.; Bao, Y.P.; Han, Y.; Wang, Y.M.; Shi, J.; Vitiello, M.V.; Lu, L. Sleep disturbances increase the risk of dementia: A systematic review and meta-analysis. Sleep Med. Rev. 2018, 40, 4–16. [Google Scholar] [CrossRef]
- Sabia, S.; Fayosse, A.; Dumurgier, J.; van Hees, V.T.; Paquet, C.; Sommerlad, A.; Kivimäki, M.; Dugravot, A.; Singh-Manoux, A. Association of sleep duration in middle and old age with incidence of dementia. Nat. Commun. 2021, 12, 2289. [Google Scholar] [CrossRef] [PubMed]
- Denison, H.J.; Jameson, K.A.; Sayer, A.A.; Patel, H.P.; Edwards, M.H.; Arora, T.; Dennison, E.M.; Cooper, C.; Baird, J. Poor sleep quality and physical performance in older adults. Sleep Health 2021, 7, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Ma, T.; Yao, S.; Chen, Z.; Xu, W.-D.; Jiang, X.-Y.; Wang, X.-F. Associations of sleep quality and sleep duration with frailty and pre-frailty in an elderly population Rugao longevity and ageing study. BMC Geriatr. 2020, 20, 9. [Google Scholar] [CrossRef] [PubMed]
- Wai, J.L.; Yu, D.S. The relationship between sleep-wake disturbances and frailty among older adults: A systematic review. J. Adv. Nurs. 2020, 76, 96–108. [Google Scholar] [CrossRef] [PubMed]
- Chien, M.Y.; Chen, H.C. Poor sleep quality is independently associated with physical disability in older adults. J. Clin. Sleep Med. 2015, 11, 225–232. [Google Scholar] [CrossRef]
- Sagayadevan, V.; Abdin, E.; Binte Shafie, S.; Jeyagurunathan, A.; Sambasivam, R.; Zhang, Y.; Picco, L.; Vaingankar, J.; Chong, S.A.; Subramaniam, M. Prevalence and correlates of sleep problems among elderly Singaporeans. Psychogeriatrics 2017, 17, 43–51. [Google Scholar] [CrossRef]
- Lo, C.M.; Lee, P.H. Prevalence and impacts of poor sleep on quality of life and associated factors of good sleepers in a sample of older Chinese adults. Health Qual. Life Outcomes 2012, 10, 72. [Google Scholar] [CrossRef]
- da Silva, A.A.; de Mello, R.G.; Schaan, C.W.; Fuchs, F.D.; Redline, S.; Fuchs, S.C. Sleep duration and mortality in the elderly: A systematic review with meta-analysis. BMJ Open 2016, 6, e008119. [Google Scholar] [CrossRef]
- Zawisza, K.; Tobiasz–Adamczyk, B.; Gałaś, A.; Brzyska, M. Sleep duration and mortality among older adults in a 22-year follow-up study: An analysis of possible effect modifiers. Eur. J. Ageing 2014, 12, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Hublin, C.; Partinen, M.; Koskenvuo, M.J.; Kaprio, J.A. Sleep and mortality: A population-based 22-year follow-up study. Sleep 2007, 30, 1245–1253. [Google Scholar] [CrossRef] [PubMed]
- Pappas, J.A.; Miner, B. Sleep Deficiency in the Elderly. Clin. Chest Med. 2022, 43, 273–286. [Google Scholar] [CrossRef] [PubMed]
- Gupta, C.; Irwin, C.; Vincent, G.; Khaleesi, S. P047 Sleep and diet in older adults: What do we know and what do we need to find out? Sleep Adv. 2021, 2 (Suppl. S1), A36–A37. [Google Scholar] [CrossRef]
- Reyes, C.M.; Cornelis, M.C. Caffeine in the Diet: Country-Level Consumption and Guidelines. Nutrients 2018, 10, 1772. [Google Scholar] [CrossRef] [PubMed]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on the safety of caffeine. EFSA J. 2015, 13, 4102. [Google Scholar] [CrossRef]
- Breedveld, B.C.; Peters, J.A.C.; Netherlands Nutrition Centre. Factsheet Caffeine. Available online: www.voedingscentrum.nl (accessed on 23 November 2023).
- Tsujimoto, T.; Kajio, H.; Sugiyama, T. Association between Caffeine Intake and All-Cause and Cause-Specific Mortality: A Population-Based Prospective Cohort Study. Mayo Clin. Proc. 2017, 92, 1190–1202. [Google Scholar] [CrossRef]
- Grosso, G.; Godos, J.; Galvano, F.; Giovannucci, E.L. Coffee, Caffeine, and Health Outcomes: An Umbrella Review. Annu. Rev. Nutr. 2017, 37, 131–156. [Google Scholar] [CrossRef]
- Ferre, S. An update on the mechanisms of the psychostimulant effects of caffeine. J. Neurochem. 2008, 105, 1067–1079. [Google Scholar] [CrossRef]
- Fisone, G.; Borgkvist, A.; Usiello, A. Caffeine as a psychomotor stimulant: Mechanism of action. Cell Mol. Life Sci. 2004, 61, 857–872. [Google Scholar] [CrossRef]
- Landolt, H.P. Sleep homeostasis: A role for adenosine in humans? Biochem. Pharmacol. 2008, 75, 2070–2079. [Google Scholar] [CrossRef] [PubMed]
- Shilo, L.; Sabbah, H.; Hadari, R.; Kovatz, S.; Weinberg, U.; Dolev, S.; Dagan, Y.; Shenkman, L. The effects of coffee consumption on sleep and melatonin secretion. Sleep Med. 2002, 3, 271–273. [Google Scholar] [CrossRef] [PubMed]
- Clark, I.; Landolt, H.P. Coffee, caffeine, and sleep: A systematic review of epidemiological studies and randomized controlled trials. Sleep Med. Rev. 2017, 31, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Gardiner, C.; Weakley, J.; Burke, L.M.; Roach, G.D.; Sargent, C.; Maniar, N.; Townshend, A.; Halson, S.L. The effect of caffeine on subsequent sleep: A systematic review and meta-analysis. Sleep Med. Rev. 2023, 69, 101764. [Google Scholar] [CrossRef] [PubMed]
- Ohayon, M.M. Interactions between sleep normative data and sociocultural characteristics in the elderly. J. Psychosom. Res. 2004, 56, 479–486. [Google Scholar] [CrossRef]
- Fawale, M.B.; Ismaila, I.A.; Mustapha, A.F.; Komolafe, M.A.; Ibigbami, O. Correlates of sleep quality and sleep duration in a sample of urban-dwelling elderly Nigerian women. Sleep Health 2017, 3, 257–262. [Google Scholar] [CrossRef]
- Hu, Y.; Stephenson, K.; Klare, D. The dynamic relationship between daily caffeine intake and sleep duration in middle-aged and older adults. J. Sleep Res. 2020, 29, e12996. [Google Scholar] [CrossRef]
- Park, M.J.; Kim, K.H. What affects the subjective sleep quality of hospitalized elderly patients? Geriatr. Gerontol. Int. 2017, 17, 471–479. [Google Scholar] [CrossRef]
- Curless, R.; French, J.M.; James, O.F.W.; Wynne, H.A. Is Caffeine a Factor in Subjective Insomnia of Elderly People? Age Ageing 1993, 22, 41–45. [Google Scholar] [CrossRef]
- Robillard, R.; Bouchard, M.; Cartier, A.; Nicolau, L.; Carrier, J. Sleep is more sensitive to high doses of caffeine in the middle years of life. J. Psychopharmacol. 2015, 29, 688–697. [Google Scholar] [CrossRef]
- Carrier, J.; Paquet, J.; Fernandez-Bolanos, M.; Girouard, L.; Roy, J.; Selmaoui, B.; Filipini, D. Effects of caffeine on daytime recovery sleep: A double challenge to the sleep-wake cycle in aging. Sleep Med. 2009, 10, 1016–1024. [Google Scholar] [CrossRef] [PubMed]
- Frozi, J.; de Carvalho, H.W.; Ottoni, G.L.; Cunha, R.A.; Lara, D.R. Distinct sensitivity to caffeine-induced insomnia related to age. J. Psychopharmacol. 2018, 32, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Gahagan, J.; Gray, K.; Whynacht, A. Sex and gender matter in health research: Addressing health inequities in health research reporting. Int. J. Equity Health 2015, 14, 12. [Google Scholar] [CrossRef] [PubMed]
- Day, S.; Mason, R.; Lagosky, S.; Rochon, P.A. Integrating and evaluating sex and gender in health research. Health Res. Policy Syst. 2016, 14, 75. [Google Scholar] [CrossRef] [PubMed]
- Huisman, M.; Poppelaars, J.; van der Horst, M.; Beekman, A.T.; Brug, J.; van Tilburg, T.G.; Deeg, D.J. Cohort Profile: The Longitudinal Aging Study Amsterdam. Int. J. Epidemiol. 2011, 40, 868–876. [Google Scholar] [CrossRef] [PubMed]
- Hoogendijk, E.O.; Deeg, D.J.H.; de Breij, S.; Klokgieters, S.S.; Kok, A.A.L.; Stringa, N.; Timmermans, E.J.; van Schoor, N.M.; van Zutphen, E.M.; van der Horst, M.; et al. The Longitudinal Aging Study Amsterdam: Cohort update 2019 and additional data collections. Eur. J. Epidemiol. 2020, 35, 61–74. [Google Scholar] [CrossRef] [PubMed]
- Hoogendijk, E.O.; Deeg, D.J.; Poppelaars, J.; van der Horst, M.; Broese van Groenou, M.I.; Comijs, H.C.; Pasman, H.R.; van Schoor, N.M.; Suanet, B.; Thomése, F.; et al. The Longitudinal Aging Study Amsterdam: Cohort update 2016 and major findings. Eur. J. Epidemiol. 2016, 31, 927–945. [Google Scholar] [CrossRef]
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Hillard, P.J.; Katz, E.S.; et al. National Sleep Foundation’s updated sleep duration recommendations: Final report. Sleep Health 2015, 1, 233–243. [Google Scholar] [CrossRef]
- Den Dulk, C.J.; Van De Stadt, H.; Vliegen, J.M. A new measure for degree of urbanization: The address density of the surrounding area. Maandstat. Bevolk. 1992, 40, 14–27. [Google Scholar]
- Hunt, S.M.; McEwen, J.; McKenna, S.P. Measuring health status: A new tool for clinicians and epidemiologists. J. R. Coll. Gen. Pract. 1985, 35, 185–188. [Google Scholar]
- Radloff, L.S. The CES-D Scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Reinhard, O.P.M.; Rood-Bakker, D.S. Alcoholgebruik in Beeld. Standaardmeetlat; Nederlands Economisch Instituut: Rotterdam, The Netherlands, 1998. [Google Scholar]
- Stel, V.S.; Smit, J.H.; Pluijm, S.M.; Visser, M.; Deeg, D.J.; Lips, P. Comparison of the LASA Physical Activity Questionnaire with a 7-day diary and pedometer. J. Clin. Epidemiol. 2004, 57, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Haskell, W.L.; Leon, A.S.; Jacobs, D.R., Jr.; Montoye, H.J.; Sallis, J.F.; Paffenbarger, R.S., Jr. Compendium of physical activities: Classification of energy costs of human physical activities. Med. Sci. Sports Exerc. 1993, 25, 71–80. [Google Scholar] [CrossRef]
- Caspersen, C.J.; Bloemberg, B.P.; Saris, W.H.; Merritt, R.K.; Kromhout, D. The prevalence of selected physical activities and their relation with coronary heart disease risk factors in elderly men: The Zutphen Study, 1985. Am. J. Epidemiol. 1991, 133, 1078–1092. [Google Scholar] [CrossRef] [PubMed]
- Dager, S.R.; Layton, M.E.; Strauss, W.; Richards, T.L.; Heide, A.; Friedman, S.D.; Artru, A.A.; Hayes, C.E.; Posse, S. Human brain metabolic response to caffeine and the effects of tolerance. Am. J. Psychiatry 1999, 156, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Lovallo, W.R.; Whitsett, T.L.; Al’absi, M.; Sung, B.H.; Vincent, A.S.; Wilson, M.F. Caffeine stimulation of cortisol secretion across the waking hours in relation to caffeine intake levels. Psychosom. Med. 2005, 67, 734–739. [Google Scholar] [CrossRef]
- Hindmarch, I.; Rigney, U.; Stanley, N.; Quinlan, P.; Rycroft, J.; Lane, J. A naturalistic investigation of the effects of day-long consumption of tea, coffee and water on alertness, sleep onset and sleep quality. Psychopharmacology 2000, 149, 203–216. [Google Scholar] [CrossRef]
- Yang, A.; Palmer, A.A.; de Wit, H. Genetics of caffeine consumption and responses to caffeine. Psychopharmacology 2010, 211, 245–257. [Google Scholar] [CrossRef]
- Retey, J.V.; Adam, M.; Khatami, R.; Luhmann, U.F.; Jung, H.H.; Berger, W.; Landolt, H.P. A genetic variation in the adenosine A2A receptor gene (ADORA2A) contributes to individual sensitivity to caffeine effects on sleep. Clin. Pharmacol. Ther. 2007, 81, 692–698. [Google Scholar] [CrossRef]
- Drake, C.; Roehrs, T.; Shambroom, J.; Roth, T. Caffeine effects on sleep taken 0, 3, or 6 hours before going to bed. J. Clin. Sleep Med. 2013, 9, 1195–1200. [Google Scholar] [CrossRef]
- Soroko, S.; Chang, J.; Barrett-Connor, E. Reasons for changing caffeinated coffee consumption: The Rancho Bernardo Study. J. Am. Coll. Nutr. 1996, 15, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Lauderdale, D.S.; Knutson, K.L.; Yan, L.L.; Liu, K.; Rathouz, P.J. Self-Reported and Measured Sleep Duration: How Similar Are They? Epidemiology 2008, 19, 838–845. [Google Scholar] [CrossRef] [PubMed]
- Vitiello, M.V.; Larsen, L.H.; Moe, K.E. Age-related sleep change: Gender and estrogen effects on the subjective-objective sleep quality relationships of healthy, noncomplaining older men and women. J. Psychosom. Res. 2004, 56, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Danker-Hopfe, H.; Hornung, O.; Regen, F.; Hansen, M.L.; Albrecht, N.; Heuser, I. Subjective sleep quality in noncomplaining elderly subjects: Results of a follow-up study. Anthr. Anz. 2006, 64, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Zilli, I.; Ficca, G.; Salzarulo, P. Factors involved in sleep satisfaction in the elderly. Sleep Med. 2009, 10, 233–239. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; 3rd Monk, T.H.; Hoch, C.C.; Yeager, A.L.; Kupfer, D.J. Quantification of subjective sleep quality in healthy elderly men and women using the Pittsburgh Sleep Quality Index (PSQI). Sleep 1991, 14, 331–338. [Google Scholar]
- Åkerstedt, T.; Schwarz, J.; Gruber, G.; Lindberg, E.; Theorell-Haglöw, J. The relation between polysomnography and subjective sleep and its dependence on age—Poor sleep may become good sleep. J. Sleep Res. 2016, 25, 565–570. [Google Scholar] [CrossRef]
- Schönknecht, P.; Pantel, J.; Kruse, A.; Schröder, J. Prevalence and natural course of aging-associated cognitive decline in a population-based sample of young-old subjects. Am. J. Psychiatry 2005, 162, 2071–2077. [Google Scholar] [CrossRef]
- Ambrosini, G.L.; van Roosbroeck, S.A.; Mackerras, D.; Fritschi, L.; de Klerk, N.H.; Musk, A.W. The reliability of ten-year dietary recall: Implications for cancer research. J. Nutr. 2003, 133, 2663–2668. [Google Scholar] [CrossRef]
- Krall, E.A.; Dwyer, J.T.; Ann Coleman, K. Factors influencing accuracy of dietary recall. Nutr. Res. 1988, 8, 829–841. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; 3rd Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep. Med. 2001, 2, 297–307. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Males | Females | |||||||
|---|---|---|---|---|---|---|---|---|
| Characteristics | Excluded Cases (n = 455) | Analytical Sample (n = 1256) | Total (n = 587) | No Caffeine (n = 39) | Caffeine (n = 548) | Total (n = 669) | No Caffeine (n = 61) | Caffeine (n = 608) |
| Caffeine consumption | ||||||||
| Total caffeine (mg/day) | ||||||||
| Mean ± SD | - | 263 ± 167 | 286 ± 175 | - | 306 ± 164 | 244 ± 156 | - | 268 ± 143 |
| Categories of caffeine, N (%) a | ||||||||
| None | - | 100 (8.0) | 39 (6.6) | 39 (100) | - | 61 (9.1) | 61 (100) | - |
| Low | - | 289 (23.0) | 120 (20.4) | - | 120 (21.9) | 169 (25.3) | - | 169 (27.8) |
| Moderate | - | 289 (23.0) | 126 (21.5) | - | 126 (23.0) | 163 (24.4) | - | 163 (26.8) |
| High | - | 300 (23.9) | 153 (26.1) | - | 152 (27.9) | 147 (22.0) | - | 147 (24.2) |
| Very high | - | 278 (22.1) | 149 (25.4) | - | 149 (27.2) | 129 (19.3) | - | 129 (21.2) |
| Caffeine from coffee (mg/day) b | ||||||||
| Median (IQR) | - | 220 (194) | 220 (187) | - | 223 (220) | 167 (220) | - | 200 (182) |
| Caffeine from tea (mg/day) c | ||||||||
| Median (IQR) | - | 36 (102) | 26 (75) | - | 33.6 (78) | 50 (116) | - | 62 (123) |
| Demographics | ||||||||
| Age in years | n = 445 | |||||||
| Mean ± SD | 76.3 ± 9.9 | 72.8 ± 7.5 | 72.5 ± 7.3 | 77.3 ± 10.2 | 72.2 ± 6.9 | 73.1 ± 7.7 | 75.9 ± 8.8 | 72.8 ± 7.5 |
| Level of attained education, N (%) | n = 445 | |||||||
| Low | 199 (44.7) | 386 (30.7) | 159 (27.1) | 13 (33.3) | 146 (26.6) | 227 (33.9) | 28 (45.9) | 199 (32.7) |
| Intermediate | 162 (36.4) | 487 (38.8) | 202 (34.4) | 16 (41.0) | 186 (33.9) | 285 (42.6) | 23 (37.7) | 262 (43.1) |
| High | 84 (18.9) | 383 (30.5) | 226 (38.5) | 10 (25.6) | 216 (39.4) | 157 (23.5) | 10 (16.4) | 147 (24.2) |
| Partner status, N (%) | n = 443 | |||||||
| Living alone | 212 (47.9) | 408 (32.5) | 125 (21.3) | 8 (20.5) | 117 (21.4) | 283 (42.3) | 29 (47.5) | 254 (41.8) |
| Living with partner | 231 (52.1) | 848 (67.5) | 462 (78.7) | 31 (79.5) | 431 (78.6) | 386 (57.7) | 32 (52.5) | 354 (58.2) |
| Level of urbanization, N (%) * | n = 441 | |||||||
| Sparsely populated (<1000) | 173 (39.2) | 520 (41.5) | 240 (41.0) | 22 (56.4) | 218 (39.9) | 280 (41.9) | 29 (47.5) | 251 (41.4) |
| Densely populated (≥1000) | 268 (60.8) | 733 (58.5) | 345 (59.0) | 17 (43.6) | 328 (60.1) | 388 (58.1) | 32 (52.5) | 356 (58.6) |
| Health related factors | ||||||||
| Number of chronic diseases d | n = 137 | |||||||
| Mean ± SD | 2.8 ± 1.7 | 2.2 ± 1.4 | 2.1 ± 1.4 | 2.4 ± 1.6 | 2.1 ± 1.4 | 2.3 ± 1.4 | 2.5 ± 1.5 | 2.3 ± 1.4 |
| Depressive symptoms (CES-D) * | n = 137 | |||||||
| Median (IQR) | 10 (12) | 5.0 (8.0) | 5.0 (7.0) | 5.0 (6.0) | 4.0 (7.0) | 6.0 (8.0) | 8.0 (10) | 6.0 (8.0) |
| Body mass index (kg/m2) * | n = 103 | |||||||
| Mean ± SD | 27.2 ± 4.7 | 27.3 ± 4.7 | 27.4 ± 4.2 | 27.0 ± 5.2 | 27.5 ± 4.1 | 27.2 ± 5.2 | 28.3 ± 5.8 | 27.1 ± 5.1 |
| Subjective pain * | ||||||||
| Mean ± SD | - | 5.8 ± 1.4 | 5.6 ± 1.2 | 5.8 ± 1.2 | 5.6 ± 1.2 | 6.0 ± 1.6 | 6.4 ± 1.9 | 6.0 ± 1.5 |
| Behavioural factors | ||||||||
| Smoking status, N (%) * | n = 107 | |||||||
| Never smoked | 26 (24.3) | 304 (24.9) | 116 (20.3) | 7 (18.4) | 109 (20.5) | 188 (28.9) | 20 (33.3) | 168 (28.5) |
| Former smoker | 66 (61.7) | 812 (66.5) | 410 (71.8) | 30 (78.9) | 380 (71.3) | 402 (61.8) | 35 (58.3) | 367 (62.6) |
| Current smoker | 15 (14.0) | 105 (8.6) | 45 (7.9) | 1 (2.6) | 44 (8.3) | 60 (9.2) | 5 (8.3) | 55 (9.3) |
| Alcohol use, N (%) * | n = 107 | |||||||
| No use | 35 (32.7) | 172 (14.1) | 56 (9.8) | 7 (18.4) | 49 (9.2) | 116 (17.8) | 19 (31.7) | 97 (16.4) |
| Moderate use | 67 (62.6) | 925 (75.8) | 467 (81.8) | 31 (81.6) | 436 (81.8) | 458 (70.5) | 38 (63.3) | 420 (71.2) |
| Above moderate use | 5 (4.7) | 124 (10.2) | 48 (8.4) | - | 48 (9.0) | 76 (11.7) | 3 (5.0) | 73 (12.4) |
| Physical activity (MET-hrs./wk.) * | n = 136 | |||||||
| Median (IQR) | 35.7 (49.1) | 52.0 (45.3) | 45.2 (40.6) | 37.3 (43.2) | 45.6 (40.2) | 58.6 (45.2) | 51.0 (41.1) | 59.3 (45.5) |
| Sleep parameters | ||||||||
| Sleep duration(h/day), N (%) * | ||||||||
| Mean ± SD | - | 7.4 ± 1.1 | 7.5 ± 1.1 | 7.8 ± 1.0 | 7.5 ± 1.1 | 7.3 ± 1.1 | 6.9 ± 1.3 | 7.3 ± 1.1 |
| Recommended (7–8 h) | - | 795 (64.2) | 402 (69.2) | 27 (71.1) | 375 (69.1) | 393 (59.8) | 24 (42.9) | 369 (61.4) |
| Short (< 7 h) | - | 272 (22.0) | 99 (17.0) | 5 (13.2) | 94 (17.3) | 173 (26.3) | 25 (44.6) | 148 (24.6) |
| Long (>8 h) | - | 171 (13.8) | 80 (13.8) | 6 (15.8) | 74 (13.6) | 91 (13.9) | 7 (12.5) 84 (14.0) | |
| Sleep disturbances, N (%) e * | ||||||||
| Median (IQR) | - | 6.0 (3.0) | 5.0 (3.0) | 6.0 (2.0) | 5.0 (3.0) | 6.0 (3.0) | 7.0 (3.0) | 6.0 (3.0) |
| No disturbances (3) | - | 154 (12.4) | 101 (17.4) | 2 (5.1) | 99 (18.3) | 53 (8.0) | 2 (3.3) | 51 (8.4) |
| Some disturbances (4–6) | - | 652 (52.4) | 329 (56.8) | 25 (64.1) | 304 (56.3) | 323 (48.6) | 23 (37.7) | 300 (49.7) |
| Several disturbances (7–9) | - | 376 (30.2) | 131 (22.6) | 12 (30.8) | 119 (22.0) | 245 (36.8) | 29 (47.5) | 216 (35.8) |
| Many disturbances (10–12) | - | 62 (5.0) | 18 (3.1) | - | 18 (3.3) | 44 (6.6) | 7 (11.5) | 37 (6.1) |
| Perceived sleep quality, N (%) * | ||||||||
| Good | - | 1028 (82.0) | 511 (87.2) | 36 (92.3) | 475 (86.8) | 517 (77.5) | 44 (72.1) | 473 (78.1) |
| Poor | - | 225 (18.0) | 75 (12.8) | 3 (7.7) | 72 (13.2) | 150 (22.5) | 17 (27.9) | 133 (21.9) |
| Males (n = 579) | Females (n = 665) | |||||
|---|---|---|---|---|---|---|
| β | 95% CI | p-Value | β | 95% CI | p-Value | |
| Categories of caffeine a | ||||||
| Crude model | ||||||
| None | 0.12 | −0.58–0.82 | 0.737 | 0.80 | 0.20–1.40 | 0.009 |
| Low (ref.) | - | - | - | - | - | - |
| Moderate | −0.27 | −0.76–0.21 | 0.267 | 0.06 | −0.38–0.51 | 0.776 |
| High | −0.54 | −1.00–−0.07 | 0.024 | −0.23 | −0.68–0.23 | 0.326 |
| Very high | −0.21 | −0.68–0.26 | 0.382 | −0.14 | −0.61–0.33 | 0.561 |
| Adjusted model c | ||||||
| None | 0.23 | −0.44–0.90 | 0.500 | 0.61 | 0.04–1.17 | 0.035 |
| Low (ref.) | - | - | - | - | - | - |
| Moderate | −0.17 | −0.63–0.29 | 0.467 | 0.08 | −0.34–0.50 | 0.713 |
| High | −0.35 | −0.80–0.09 | 0.122 | −0.12 | −0.55–0.31 | 0.572 |
| Very high | −0.12 | −0.58–0.33 | 0.597 | −0.12 | −0.57–0.32 | 0.587 |
| Caffeine vs. no caffeine | ||||||
| Crude model | ||||||
| Caffeine (ref.) | - | - | - | - | - | - |
| No caffeine | 0.39 | −0.24–1.02 | 0.222 | 0.87 | 0.33–1.41 | 0.002 |
| Adjusted model c | ||||||
| Caffeine (ref.) | - | - | - | - | - | - |
| No caffeine | 0.39 | −0.21–1.00 | 0.205 | 0.64 | 0.13–1.15 | 0.014 |
| Males (n = 581) | Females (n = 657) | |||||
|---|---|---|---|---|---|---|
| OR b | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Short sleep duration (<7 h ) a | ||||||
| Categories of caffeine c | ||||||
| Crude model | ||||||
| None | 0.78 | 0.27–2.29 | 0.651 | 2.45 | 1.26–4.75 | 0.008 |
| Low (ref.) | - | - | - | - | - | - |
| Moderate | 0.91 | 0.45–1.84 | 0.791 | 0.93 | 0.55–1.55 | 0.767 |
| High | 1.20 | 0.63–2.29 | 0.587 | 1.00 | 0.59–1.69 | 0.997 |
| Very high | 1.08 | 0.56–2.08 | 0.812 | 0.83 | 0.48–1.45 | 0.511 |
| Adjusted model d | ||||||
| None | 0.93 | 0.30–2.87 | 0.903 | 2.18 | 1.09–4.37 | 0.028 |
| Low (ref.) | - | - | - | - | - | - |
| Moderate | 0.94 | 0.45–1.96 | 0.867 | 0.97 | 0.56–1.66 | 0.899 |
| High | 1.24 | 0.62–2.47 | 0.537 | 1.10 | 0.63–1.91 | 0.744 |
| Very high | 1.00 | 0.49–2.02 | 0.989 | 0.80 | 0.45–1.44 | 0.454 |
| Caffeine vs. no caffeine | ||||||
| Crude model | ||||||
| Caffeine (ref.) | - | - | - | - | - | - |
| No caffeine | 0.74 | 0.28–1.97 | 0.545 | 2.60 | 1.44–4.69 | 0.002 |
| Adjusted model d | ||||||
| Caffeine (ref.) | - | - | - | - | - | - |
| No caffeine | 0.90 | 0.32–2.48 | 0.833 | 2.26 | 1.22–4.20 | 0.010 |
| Long sleep duration (>8 h) a | ||||||
| Categories of caffeine c | ||||||
| Crude model | ||||||
| None | 0.94 | 0.34–2.59 | 0.898 | 1.28 | 0.49–3.33 | 0.612 |
| Low (ref.) | - | - | - | - | - | - |
| Moderate | 0.81 | 0.40–1.67 | 0.574 | 1.07 | 0.56–2.01 | 0.847 |
| High | 0.91 | 0.46–1.79 | 0.781 | 1.06 | 0.55–2.05 | 0.862 |
| Very high | 0.64 | 0.31–1.33 | 0.231 | 0.86 | 0.43–1.73 | 0.666 |
| Adjusted model d | ||||||
| None | 0.73 | 0.24–2.17 | 0.564 | 1.19 | 0.44–3.18 | 0.735 |
| Low (ref.) | - | - | - | - | - | - |
| Moderate | 0.89 | 0.42–1.90 | 0.761 | 1.08 | 0.55–2.10 | 0.827 |
| High | 1.19 | 0.57–2.46 | 0.646 | 1.17 | 0.59–2.34 | 0.657 |
| Very high | 0.82 | 0.38–1.78 | 0.622 | 0.97 | 0.46–2.02 | 0.925 |
| Caffeine vs. no caffeine | ||||||
| Crude model | ||||||
| Caffeine (ref.) | - | - | - | - | - | - |
| No caffeine | 1.13 | 0.45–2.82 | 0.800 | 1.28 | 0.53–3.07 | 0.579 |
| Adjusted model d | ||||||
| Caffeine (ref.) | - | - | - | - | - | - |
| No caffeine | 0.75 | 0.28–2.03 | 0.567 | 1.13 | 0.46–2.80 | 0.788 |
| Males (n = 586) | Females (n = 667) | |||||
|---|---|---|---|---|---|---|
| OR a | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Categories of caffeine b | ||||||
| Crude model | ||||||
| None | 0.58 | 0.16–2.13 | 0.415 | 1.42 | 0.73–2.77 | 0.308 |
| Low (ref.) | - | - | - | - | - | - |
| Moderate | 0.96 | 0.45–2.05 | 0.905 | 1.09 | 0.65–1.83 | 0.758 |
| High | 0.82 | 0.39–1.73 | 0.598 | 0.90 | 0.52–1.56 | 0.710 |
| Very high | 1.48 | 0.75–2.94 | 0.263 | 1.16 | 0.67–2.00 | 0.595 |
| Adjusted model c | ||||||
| None | 0.86 | 0.22–3.47 | 0.837 | 1.25 | 0.60–2.58 | 0.556 |
| Low (ref.) | - | - | - | - | - | - |
| Moderate | 1.18 | 0.50–2.77 | 0.711 | 1.04 | 0.59–1.82 | 0.903 |
| High | 1.03 | 0.45–2.40 | 0.938 | 0.97 | 0.54–1.76 | 0.917 |
| Very high | 1.97 | 0.89–4.39 | 0.095 | 1.11 | 0.61–2.02 | 0.738 |
| Caffeine vs. no caffeine | ||||||
| Crude model | ||||||
| Caffeine (ref.) | - | - | - | - | - | - |
| No caffeine | 0.55 | 0.17–1.83 | 0.330 | 1.37 | 0.76–2.48 | 0.293 |
| Adjusted model c | ||||||
| Caffeine (ref.) | - | - | - | - | - | - |
| No caffeine | 0.67 | 0.19–2.41 | 0.543 | 1.21 | 0.64–2.32 | 0.558 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van der Linden, M.; Olthof, M.R.; Wijnhoven, H.A.H. The Association between Caffeine Consumption from Coffee and Tea and Sleep Health in Male and Female Older Adults: A Cross-Sectional Study. Nutrients 2024, 16, 131. https://doi.org/10.3390/nu16010131
van der Linden M, Olthof MR, Wijnhoven HAH. The Association between Caffeine Consumption from Coffee and Tea and Sleep Health in Male and Female Older Adults: A Cross-Sectional Study. Nutrients. 2024; 16(1):131. https://doi.org/10.3390/nu16010131
Chicago/Turabian Stylevan der Linden, Mette, Margreet R. Olthof, and Hanneke A. H. Wijnhoven. 2024. "The Association between Caffeine Consumption from Coffee and Tea and Sleep Health in Male and Female Older Adults: A Cross-Sectional Study" Nutrients 16, no. 1: 131. https://doi.org/10.3390/nu16010131
APA Stylevan der Linden, M., Olthof, M. R., & Wijnhoven, H. A. H. (2024). The Association between Caffeine Consumption from Coffee and Tea and Sleep Health in Male and Female Older Adults: A Cross-Sectional Study. Nutrients, 16(1), 131. https://doi.org/10.3390/nu16010131