

Exploring the Therapeutic Potential of Royal Jelly in Metabolic Disorders and Gastrointestinal Diseases

 , , ,
, , ,  , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Methodology
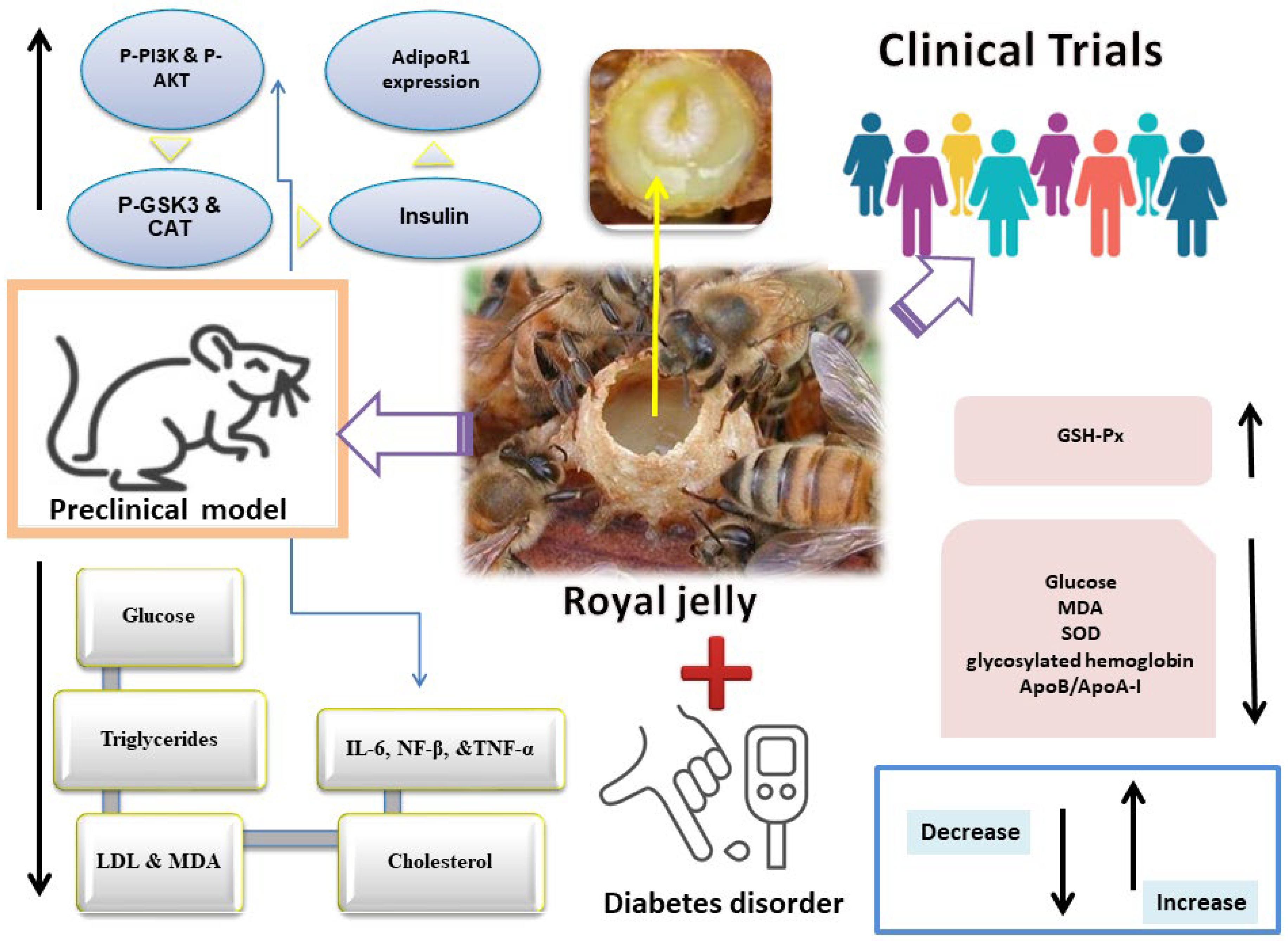
3. Royal Jelly in Diabetes
3.1. Preclinical Studies
3.2. Clinical Studies
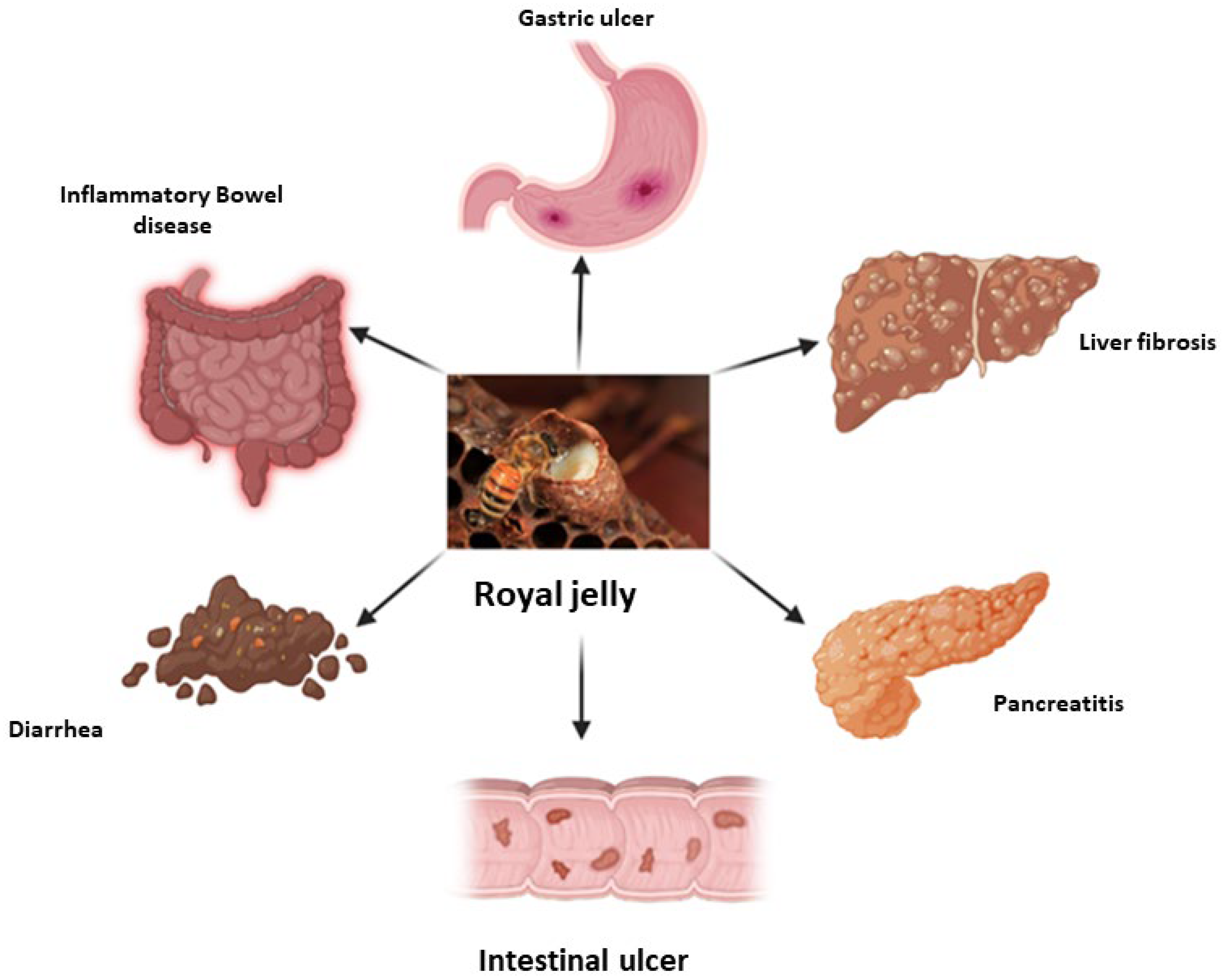
4. Royal Jelly in Gastrointestinal Diseases
4.1. Inflammatory Bowel Diseases
4.2. Lactose Intolerance
4.3. Chronic Diarrhea and Constipation
4.4. Gastrointestinal Ulcer Disease
4.5. Liver Disease
4.5.1. Preclinical Studies
4.5.2. Clinical Studies
5. Royal Jelly in Cardiovascular Disease
5.1. Antihypertensive Activity of Royal Jelly
5.1.1. Preclinical Studies
5.1.2. Clinical Studies
5.2. Hypo-Cholesterolemic Activity of Royal Jelly
6. Conclusions and Future Prospects
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Han, T.S.; Lean, M.E.J. Metabolic Syndrome. Medicine 2011, 39, 24–31. [Google Scholar] [CrossRef]
- Robbins, G.R.; Wen, H.; Ting, J.P.Y. Inflammasomes and Metabolic Disorders: Old Genes in Modern Diseases. Mol. Cell 2014, 54, 297–308. [Google Scholar] [CrossRef] [PubMed]
- Chait, A.; den Hartigh, L.J. Adipose Tissue Distribution, Inflammation and Its Metabolic Consequences, Including Diabetes and Cardiovascular Disease. Front. Cardiovasc. Med. 2020, 7, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Rinaldi, L.; Pafundi, P.C.; Galiero, R.; Caturano, A.; Morone, M.V.; Silvestri, C.; Giordano, M.; Salvatore, T.; Sasso, F.C. Mechanisms of Non-Alcoholic Fatty Liver Disease in the Metabolic Syndrome. A Narrative Review. Antioxidants 2021, 10, 270. [Google Scholar] [CrossRef] [PubMed]
- Heindel, J.J.; Blumberg, B.; Cave, M.; Machtinger, R.; Mantovani, A.; Mendez, M.A.; Nadal, A.; Palanza, P.; Panzica, G.; Sargis, R.; et al. Metabolism Disrupting Chemicals and Metabolic Disorders. Reprod. Toxicol. 2017, 68, 3–33. [Google Scholar] [CrossRef] [PubMed]
- Korivi, M.; Liu, B.R. New Strategies from Natural Materials to Fight against Diet-Induced Metabolic Disorders (Part–II). Curr. Pharm. Des. 2021, 27, 761–762. [Google Scholar] [CrossRef] [PubMed]
- Burant, C.F.; Viswanathan, P.; Marcinak, J.; Cao, C.; Vakilynejad, M.; Xie, B.; Leifke, E. TAK-875 versus Placebo or Glimepiride in Type 2 Diabetes Mellitus: A Phase 2, Randomised, Double-Blind, Placebo-Controlled Trial. Lancet 2012, 379, 1403–1411. [Google Scholar] [CrossRef] [PubMed]
- Tabatabaei-Malazy, O.; Larijani, B.; Abdollahi, M. Targeting Metabolic Disorders by Natural Products. J. Diabetes Metab. Disord. 2015, 14, 57–77. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhu, C.; Ying, Y.; Luo, L.; Huang, D.; Luo, Z. Metformin and Berberine, Two Versatile Drugs in Treatment of Common Metabolic Diseases. Oncotarget 2018, 9, 10135–10146. [Google Scholar] [CrossRef]
- Zhao, J.D.; Yu, C.J.; Li, J.Y.; Wang, S.H.; Yang, D.; Guo, C.L.; Du, X.; Zhang, W.J.; Cheng, R.D.; Diao, X.C.; et al. Effect of Berberine on Hyperglycaemia and Gut Microbiota Composition in Type 2 Diabetic Goto-Kakizaki Rats. World J. Gastroenterol. 2021, 27, 708–724. [Google Scholar] [CrossRef]
- Asgari, M.; Asle-Rousta, M.; Sofiabadi, M. Effect of Royal Jelly on Blood Glucose and Lipids in Streptozotocin Induced Type 1 Diabetic Rats. Arak Med. Univ. J. 2017, 20, 48–56. [Google Scholar]
- Pourmoradian, S.; Mahdavi, R.; Mobasseri, M.; Faramarzi, E.; Mobasseri, M. Effects of Royal Jelly Supplementation on Body Weight and Dietary Intake in Type 2 Diabetic Females. Health Promot. Perspect. 2012, 2, 231–235. [Google Scholar] [CrossRef]
- Duran, Y.; Karaboğa, İ.; Polat, F.R.; Polat, E.; Erboğa, Z.F.; Ovalı, M.A.; Öztopuz, R.Ö.; Çelikkol, A.; Yılmaz, A. Royal Jelly Attenuates Gastric Mucosal Injury in a Rat Ethanol-Induced Gastric Injury Model. Mol. Biol. Rep. 2020, 47, 8867–8879. [Google Scholar] [CrossRef]
- Miyauchi-Wakuda, S.; Kagota, S.; Maruyama-Fumoto, K.; Wakuda, H.; Yamada, S.; Shinozuka, K. Effect of Royal Jelly on Mouse Isolated Ileum and Gastrointestinal Motility. J. Med. Food 2019, 22, 789–796. [Google Scholar] [CrossRef]
- Ohba, K.; Miyata, Y.; Shinzato, T.; Funakoshi, S.; Maeda, K.; Matsuo, T.; Mitsunari, K.; Mochizuki, Y.; Nishino, T.; Sakai, H. Effect of Oral Intake of Royal Jelly on Endothelium Function in Hemodialysis Patients: Study Protocol for Multicenter, Double-Blind, Randomized Control Trial. Trials 2021, 22, 950–957. [Google Scholar] [CrossRef]
- Hadi, A.; Najafgholizadeh, A.; Aydenlu, E.S.; Shafiei, Z.; Pirivand, F.; Golpour, S.; Pourmasoumi, M. Royal Jelly Is an Effective and Relatively Safe Alternative Approach to Blood Lipid Modulation: A Meta-Analysis. J. Funct. Foods 2018, 41, 202–209. [Google Scholar] [CrossRef]
- Bagameri, L.; Baci, G.-M.; Dezmirean, D.S. Royal Jelly as a Nutraceutical Natural Product with a Focus on Its Antibacterial Activity. Pharmaceutics 2022, 14, 1142. [Google Scholar] [CrossRef]
- Khalifa, S.A.M.; Elashal, M.; Kieliszek, M.; Ghazala, N.E.; Farag, M.A.; Saeed, A.; Sabir, J.S.M.; Battino, M.; Xiao, J.; Zou, X.; et al. Recent Insights into Chemical and Pharmacological Studies of Bee Bread. Trends Food Sci. Technol. 2020, 97, 300–316. [Google Scholar] [CrossRef]
- El-Seedi, H.; El-Wahed, A.A.; Yosri, N.; Musharraf, S.G.; Chen, L.; Moustafa, M.; Zou, X.; Al-Mousawi, S.; Guo, Z.; Khatib, A.; et al. Antimicrobial Properties of Apis Mellifera’s Bee Venom. Toxins 2020, 12, 451. [Google Scholar] [CrossRef] [PubMed]
- El-Wahed, A.A.A.; Farag, M.A.; Eraqi, W.A.; Mersal, G.A.M.; Zhao, C.; Khalifa, S.A.M.; El-Seedi, H.R. Unravelling the Beehive Air Volatiles Profile as Analysed via Solid-Phase Microextraction (SPME) and Chemometrics. J. King Saud Univ. Sci. 2021, 33, 101449–101456. [Google Scholar] [CrossRef]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and Regional Diabetes Prevalence Estimates for 2019 and Projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th Edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef]
- Heron, M. Deaths: Leading Causes for 2016. Natl. Vital Stat. Rep. 2018, 67, 1–77. [Google Scholar]
- Van Cauwenberghe, J.; Enzlin, P.; Nefs, G.; Ruige, J.; Hendrieckx, C.; De Block, C.; Pouwer, F. Prevalence of and Risk Factors for Sexual Dysfunctions in Adults with Type 1 or Type 2 Diabetes: Results from Diabetes MILES–Flanders. Diabet. Med. 2022, 39, e14676. [Google Scholar] [CrossRef]
- Bin Rakhis, S.A.; AlDuwayhis, N.M.; Aleid, N.; AlBarrak, A.N.; Aloraini, A.A. Glycemic Control for Type 2 Diabetes Mellitus Patients: A Systematic Review. Cureus 2022, 14, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Chamberlain, R.C.; Fleetwood, K.; Wild, S.H.; Colhoun, H.M.; Lindsay, R.S.; Petrie, J.R.; McCrimmon, R.J.; Gibb, F.; Philip, S.; Sattar, N.; et al. Foot Ulcer and Risk of LowerLimb Amputation or Death in People with Diabetes: A National Population-Based Retrospective Cohort Study. Diabetes Care 2022, 45, 83–91. [Google Scholar] [CrossRef]
- McEwan, P.; Morgan, A.R.; Boyce, R.; Bergenheim, K.; Gause-Nilsson, I.A.M.; Bhatt, D.L.; Leiter, L.A.; Johansson, P.A.; Mosenzon, O.; Cahn, A.; et al. The Cost-Effectiveness of Dapagliflozin in Treating High-Risk Patients with Type 2 Diabetes Mellitus: An Economic Evaluation Using Data from the DECLARE-TIMI 58 Trial. Diabetes Obes. Metab. 2021, 23, 1020–1029. [Google Scholar] [CrossRef] [PubMed]
- Switanek, M.; Crailsheim, K.; Truhetz, H.; Brodschneider, R. Modelling Seasonal Effects of Temperature and Precipitation on Honey Bee Winter Mortality in a Temperate Climate. Sci. Total Environ. 2017, 579, 1581–1587. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, M.; Hayashi, K.; Watadani, R.; Okano, Y.; Tanimura, K.; Kotoh, J.; Sasaki, D.; Matsumoto, K.; Maeda, A. Royal Jelly Improves Hyperglycemia in Obese/Diabetic KK-Ay Mice. J. Vet. Med. Sci. 2017, 79, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Ghanbari, E.; Nejati, V.; Khazaei, M. Antioxidant and Protective Effects of Royal Jelly on Histopathological Changes in Testis of Diabetic Rats. Int. J. Reprod. Biomed. 2016, 14, 511–518. [Google Scholar] [CrossRef]
- Ghanbari, E.; Nejati, V.; Khazaei, M. Improvement in Serum Biochemical Alterations and Oxidative Stress of Liver and Pancreas Following Use of Royal Jelly in Streptozotocin-Induced Diabetic Rat. Cell J. 2016, 18, 362–370. [Google Scholar] [PubMed]
- Khoshpey, B.; Djazayeri, S.; Amiri, F.; Malek, M.; Hosseini, A.F.; Hosseini, S.; Shidfar, S.; Shidfar, F. Effect of Royal Jelly Intake on Serum Glucose, Apolipoprotein A-I (ApoA-I), Apolipoprotein B (ApoB) and ApoB/ApoA-I Ratios in Patients with Type 2 Diabetes: A Randomized, Double-Blind Clinical Trial Study. Can. J. Diabetes 2016, 40, 324–328. [Google Scholar] [CrossRef]
- Pourmoradian, S.; Mahdavi, R.; Mobasseri, M.; Faramarzi, E.; Mobasseri, M. Effects of Royal Jelly Supplementation on Glycemic Control and Oxidative Stress Factors in Type 2 Diabetic Female: A Randomized Clinical Trial. Chin. J. Integr. Med. 2014, 20, 347–352. [Google Scholar] [CrossRef]
- Ghanbari, E.; Nejati, V.; Najafi, G.; Khazaei, M.; Babaei, M. Study on the Effect of Royal Jelly on Reproductive Parameters in Streptozotocin-Induced Diabetic Rats. Int. J. Fertil. Steril. 2015, 9, 113–120. [Google Scholar]
- Karaca, T.; Demirtaş, S.; Karaboğa, İ.; Ayvaz, S. Protective Effects of Royal Jelly against Testicular Damage in Streptozotocin-Induced Diabetic Rats. Turk. J. Med. Sci. 2015, 45, 27–32. [Google Scholar] [CrossRef]
- Nohair, S.F. Al Antidiabetic Efficacy of a Honey-Royal Jelly Mixture: Biochemical Study in Rats. Int. J. Health Sci. 2021, 15, 4–9. [Google Scholar]
- Macadangdang, R.R., Jr.; Orodio, A.L.T.; Calabio, A.G.T.; Miciano, K.B.V.; Coleen, A.L.T. Hypoglycemic Effect of Moringa Oliefera Lam. Seed Oil Extract and Royal Jelly Composite Mixture in Alloxan-Induced Diabetes in Male Albino Wistar Rats. Asian, J. Biol. Life Sci. 2021, 10, 159–164. [Google Scholar] [CrossRef]
- Yoneshiro, T.; Kaede, R.; Nagaya, K.; Aoyama, J.; Saito, M.; Okamatsu-Ogura, Y.; Kimura, K.; Terao, A. Royal Jelly Ameliorates Diet-Induced Obesity and Glucose Intolerance by Promoting Brown Adipose Tissue Thermogenesis in Mice. Obes. Res. Clin. Pract. 2016, 10, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Watadani, R.; Kotoh, J.; Sasaki, D.; Someya, A.; Matsumoto, K.; Maeda, A. 10-Hydroxy-2-Decenoic Acid, a Natural Product, Improves Hyperglycemia and Insulin Resistance in Obese/Diabetic KK-Ay Mice, but Does Not Prevent Obesity. J. Vet. Med. Sci. 2017, 79, 1596–1602. [Google Scholar] [CrossRef]
- Hu, X.; Liu, Z.; Lu, Y.; Chi, X.; Han, K.; Wang, H.; Wang, Y.; Ma, L.; Xu, B. Glucose Metabolism Enhancement by 10-Hydroxy- 2-Decenoic Acid via the PI3K/AKT Signaling Pathway in High-Fat-Diet/Streptozotocin Induced Type 2 Diabetic Mice. Food Funct. 2022, 13, 9931–9946. [Google Scholar] [CrossRef]
- You, S.; Xiang, Y.; Qi, X.; Mao, R.; Cai, E.; Lan, Y.; Lu, H.; Shen, J.; Deng, H. Harnessing a Biopolymer Hydrogel Reinforced by Copper / Tannic Acid Nanosheets for Treating Bacteria-Infected Diabetic Wounds. Mater. Today Adv. 2022, 15, 100271–100286. [Google Scholar] [CrossRef]
- Zhou, J.; Wang, Z.; Yang, C.; Zhang, H.; Yan, W.; Wang, K. A Carrier-Free, Dual-Functional Hydrogel Constructed of Antimicrobial Peptide Jelleine-1 and 8Br-CAMP for MRSA Infected Diabetic Wound Healing. Acta Biomater. J. 2022, 151, 223–234. [Google Scholar] [CrossRef]
- Jayaraman, R.; Subramani, S.; Sheik Abdullah, S.H.; Udaiyar, M. Antihyperglycemic Effect of Hesperetin, a Citrus Flavonoid, Extenuates Hyperglycemia and Exploring the Potential Role in Antioxidant and Antihyperlidemic in Streptozotocin-Induced Diabetic Rats. Biomed. Pharmacother. 2018, 97, 98–106. [Google Scholar] [CrossRef]
- López-Gutiérrez, N.; Aguilera-Luiz, M.D.M.; Romero-González, R.; Vidal, J.L.M.; Garrido Frenich, A. Fast Analysis of Polyphenols in Royal Jelly Products Using Automated TurboFlowTM-Liquid Chromatography-Orbitrap High Resolution Mass Spectrometry. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2014, 973, 17–28. [Google Scholar] [CrossRef]
- Singh, P.; Bansal, S.; Kuhad, A.; Kumar, A.; Chopra, K. Naringenin Ameliorates Diabetic Neuropathic Pain by Modulation of Oxidative-Nitrosative Stress, Cytokines and MMP-9 Levels. Food Funct. 2020, 11, 4548–4560. [Google Scholar] [CrossRef] [PubMed]
- Wojnar, W.; Zych, M.; Kaczmarczyk-Sedlak, I. Antioxidative Effect of Flavonoid Naringenin in the Lenses of Type 1 Diabetic Rats. Biomed. Pharmacother. 2018, 108, 974–984. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Andrade, R.R.; Sánchez-Salgado, J.C.; Navarrete-Vázquez, G.; Webster, S.P.; Binnie, M.; García-Jiménez, S.; León-Rivera, I.; Cigarroa-Vázquez, P.; Villalobos-Molina, R.; Estrada-Soto, S. Antidiabetic and Toxicological Evaluations of Naringenin in Normoglycaemic and NIDDM Rat Models and Its Implications on Extra-Pancreatic Glucose Regulation. Diabetes Obes. Metab. 2008, 10, 1097–1104. [Google Scholar] [CrossRef]
- Kumar, B.; Gupta, S.K.; Srinivasan, B.P.; Nag, T.C.; Srivastava, S.; Saxena, R. Hesperetin Ameliorates Hyperglycemia Induced Retinal Vasculopathy via Anti-Angiogenic Effects in Experimental Diabetic Rats. Vascul. Pharmacol. 2012, 57, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Jia, Q.; Mehmood, S.; Ma, S.; Liu, X. Genistein Ameliorates Inflammation and Insulin Resistance through Mediation of Gut Microbiota Composition in Type 2 Diabetic Mice. Eur. J. Nutr. 2021, 60, 2155–2168. [Google Scholar] [CrossRef]
- Fu, Z.; Zhang, W.; Zhen, W.; Lum, H.; Nadler, J.; Bassaganya-Riera, J.; Jia, Z.; Wang, Y.; Misra, H.; Liu, D. Genistein Induces Pancreatic β-Cell Proliferation through Activation of Multiple Signaling Pathways and Prevents Insulin-Deficient Diabetes in Mice. Endocrinology 2010, 151, 3026–3037. [Google Scholar] [CrossRef]
- Li, R.Z.; Ding, X.W.; Geetha, T.; Al-Nakkash, L.; Broderick, T.L.; Babu, J.R. Beneficial Effect of Genistein on Diabetes-Induced Brain Damage in the OB/OB Mouse Model. Drug Des. Devel. Ther. 2020, 14, 3325–3336. [Google Scholar] [CrossRef]
- Qnais, E.; Alqudah, A.; Wedyan, M.; Gammoh, O.; Alkhateeb, H.; Alnoaimi, M. Formononetin Suppresses Hyperglycaemia through Activation of GLUT4-AMPK Pathway. Pharmacia 2023, 70, 527–536. [Google Scholar] [CrossRef]
- Oza, M.J.; Kulkarni, Y.A. Formononetin Ameliorates Diabetic Neuropathy by Increasing Expression of SIRT1 and NGF. Chem. Biodivers. 2020, 17, e2000162. [Google Scholar] [CrossRef] [PubMed]
- Zywno, H.; Bzdega, W.; Kolakowski, A.; Kurzyna, P.; Harasim-Symbor, E.; Sztolsztener, K.; Chabowski, A.; Konstantynowicz-Nowicka, K. The Influence of Coumestrol on Sphingolipid Signaling Pathway and Insulin Resistance Development in Primary Rat Hepatocytes. Biomolecules 2021, 11, 268. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.M.; Imm, J.Y. The Effect of Chrysin-Loaded Phytosomes on Insulin Resistance and Blood Sugar Control in Type 2 Diabetic Db/Db Mice. Molecules 2020, 25, 5503. [Google Scholar] [CrossRef] [PubMed]
- Salama, A.; Asaad, G.; Shaheen, A. Chrysin Ameliorates STZ-Induced Diabetes in Rats: Possible Impact of Modulation of TLR4/NF-Κβ Pathway. Res. Pharm. Sci. 2022, 17, 1–11. [Google Scholar] [CrossRef]
- Honda, Y.; Araki, Y.; Hata, T.; Ichihara, K.; Ito, M.; Tanaka, M.; Honda, S. 10-Hydroxy-2-Decenoic Acid, the Major Lipid Component of Royal Jelly, Extends the Lifespan of Caenorhabditis Elegans through Dietary Restriction and Target of Rapamycin Signaling. J. Aging Res. 2015, 2015, 425261. [Google Scholar] [CrossRef]
- Shidfar, F.; Jazayeri, S.; Mousavi, S.N.; Malek, M.; Hosseini, A.F.; Khoshpey, B. Does Supplementation with Royal Jelly Improve Oxidative Stress and Insulin Resistance in Type 2 Diabetic Patients? Iran. J. Public Health 2015, 44, 797–803. [Google Scholar]
- Siavash, M.; Shokri, S.; Haghighi, S.; Mohammadi, M.; Shahtalebi, M.A.; Farajzadehgan, Z. The Efficacy of Topical Royal Jelly on Diabetic Foot Ulcers Healing: A Case Series. J. Res. Med. Sci. 2011, 16, 904–909. [Google Scholar]
- Boukraĝ, L.; Meslem, A.; Benhanifia, M.; Hammoudi, S.M. Synergistic Effect of Starch and Royal Jelly against Staphylococcus Aureus and Escherichia Coli. J. Altern. Complement. Med. 2009, 15, 755–757. [Google Scholar] [CrossRef]
- Yakoot, M.; Abdelatif, M.; Helmy, S. Efficacy of a New Local Limb Salvage Treatment for Limb-Threatening Diabetic Foot Wounds–A Randomized Controlled Study. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 1659–1665. [Google Scholar] [CrossRef]
- Aljafary, M.A.; Al-suhaimi, E.A. Adiponectin System (Rescue Hormone): The Missing Link between Metabolic and Cardiovascular Diseases. Pharmaceutics 2022, 14, 1430. [Google Scholar] [CrossRef]
- Geagea, A.G.; Mallat, S.; Matar, C.F.; Zerbe, R.; Filfili, E.; Francis, M.; Haidar, H.; Jurjus, A. Adiponectin and Inflammation in Health and Disease: An Update. Open Med. J. 2018, 5, 20–32. [Google Scholar] [CrossRef]
- Maleki, V.; Jafari-Vayghan, H.; Saleh-Ghadimi, S.; Adibian, M.; Kheirouri, S.; Alizadeh, M. Effects of Royal Jelly on Metabolic Variables in Diabetes Mellitus: A Systematic Review. Complement. Ther. Med. 2019, 43, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Joshi, T.; Singh, A.K.; Haratipour, P.; Sah, A.N.; Pandey, A.K.; Naseri, R.; Juyal, V.; Farzaei, M.H. Targeting AMPK Signaling Pathway by Natural Products for Treatment of Diabetes Mellitus and Its Complications. J. Cell. Physiol. 2019, 234, 17212–17231. [Google Scholar] [CrossRef] [PubMed]
- Ananthakrishnan, A.N.; Xavier, R.J. Gastrointestinal Diseases. In Hunter’s Tropical Medicine and Emerging Infectious Diseases; Elsevier: Amsterdam, The Netherlands, 2020; pp. 16–26. [Google Scholar]
- Sperber, A.D.; Bangdiwala, S.I.; Drossman, D.A.; Ghoshal, U.C.; Simren, M.; Tack, J.; Whitehead, W.E.; Dumitrascu, D.L.; Fang, X.; Fukudo, S.; et al. Worldwide Prevalence and Burden of Functional Gastrointestinal Disorders, Results of Rome Foundation Global Study. Gastroenterology 2021, 160, 99–114.e3. [Google Scholar] [CrossRef] [PubMed]
- De Filippo, C.; Di Paola, M.; Ramazzotti, M.; Albanese, D.; Pieraccini, G.; Banci, E.; Miglietta, F.; Cavalieri, D.; Lionetti, P. Diet, Environments, and Gut Microbiota. A Preliminary Investigation in Children Living in Rural and Urban Burkina Faso and Italy. Front. Microbiol. 2017, 8, 1979–1983. [Google Scholar] [CrossRef] [PubMed]
- Rizzello, F.; Spisni, E.; Giovanardi, E.; Imbesi, V.; Salice, M.; Alvisi, P.; Valerii, M.C.; Gionchetti, P. Implications of the Westernized Diet in the Onset and Progression of IBD. Nutrients 2019, 11, 1033. [Google Scholar] [CrossRef]
- Vona, R.; Pallotta, L.; Cappelletti, M.; Severi, C.; Matarrese, P. The Impact of Oxidative Stress in Human Pathology: Focus on Gastrointestinal Disorders. Antioxidants 2021, 10, 201. [Google Scholar] [CrossRef]
- Proestos, C. Superfoods: Recent Data on Their Role in the Prevention of Diseases. Curr. Res. Nutr. Food Sci. 2018, 6, 576–593. [Google Scholar] [CrossRef]
- Mostafa, R.E.; El-Marasy, S.A.; Abdel Jaleel, G.A.; Bakeer, R.M. Protective Effect of Royal Jelly against Diclofenac-Induced Hepato-Renal Damage and Gastrointestinal Ulcerations in Rats. Heliyon 2020, 6, e03330. [Google Scholar] [CrossRef]
- Ahmad, S.; Campos, M.G.; Fratini, F.; Altaye, S.Z.; Li, J. New Insights into the Biological and Pharmaceutical Properties of Royal Jelly. Int. J. Mol. Sci. 2020, 21, 382. [Google Scholar] [CrossRef]
- Li, S.; Tao, L.; Yu, X.; Zheng, H.; Wu, J.H.F. Royal Jelly Proteins and Their Derived Peptides: Preparation, Properties, and Biological Activities. J. Agric. Food Chem. 2021, 69, 14415–14427. [Google Scholar] [CrossRef]
- Jairath, V.; Feagan, B.G. Global Burden of Inflammatory Bowel Disease. Lancet Gastroenterol. Hepatol. 2020, 5, 2–3. [Google Scholar] [CrossRef]
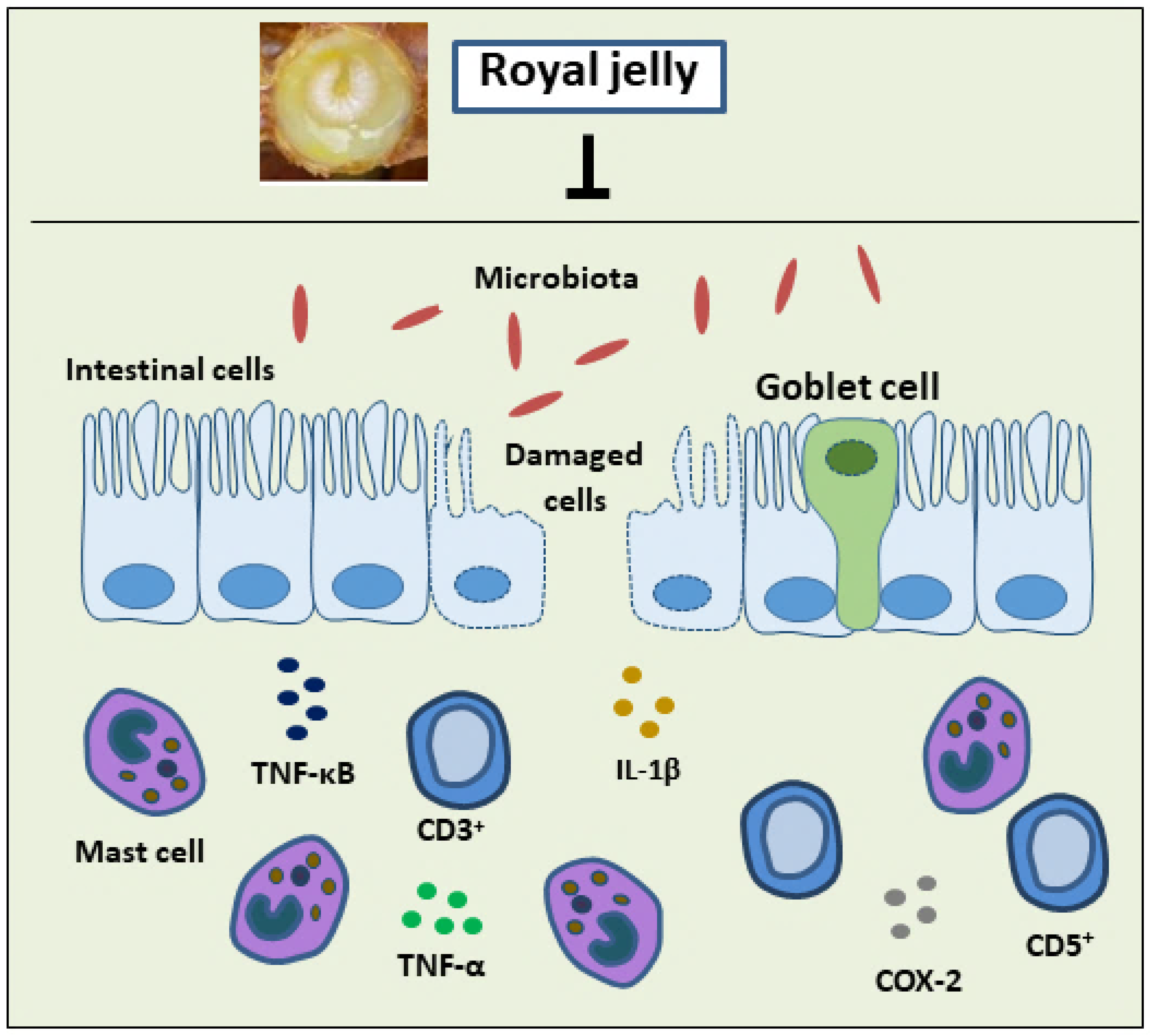
- Karaca, T.; Uz, Y.H.; Demirtas, S.; Karaboga, I.; Can, G. Protective Effect of Royal Jelly in 2,4,6 Trinitrobenzene Sulfonic Acid-Induced Colitis in Rats. Iran. J. Basic Med. Sci. 2015, 18, 370–379. [Google Scholar]
- Karaca, T.; Bayiroglu, F.; Yoruk, M.; Kaya, M.S.; Uslu, S.; Comba, B.; Mis, L. Effect of Royal Jelly on Experimental Colitis Induced by Acetic Acid and Alteration of Mast Cell Distribution in the Colon of Rats. Eur. J. Histochem. 2010, 54, 158–161. [Google Scholar] [CrossRef]
- Karaca, T.; Şimşek, N.; Uslu, S.; Kalkan, Y.; Can, I.; Kara, A.; Yörük, M. The Effect of Royal Jelly on CD3+, CD5+, CD45+ T-Cell and CD68+ Cell Distribution in the Colon of Rats with Acetic Acid-Induced Colitis. Allergol. Immunopathol. 2012, 40, 357–361. [Google Scholar] [CrossRef]
- Chi, X.; Liu, Z.; Wang, H.; Wang, Y.; Xu, B.; Wei, W. Regulation of a New Type of Selenium-Rich Royal Jelly on Gut Microbiota Profile in Mice. Biol. Trace Elem. Res. 2022, 200, 1763–1775. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Ma, B.; Wang, Z.; Chen, Y.; Tian, W.; Dong, Y. Royal Jelly Protected against Dextran-Sulfate-Sodium-Induced Colitis by Improving the Colonic Mucosal Barrier and Gut Microbiota. Nutrients 2022, 14, 2069. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Zhang, W.; Wang, C.; Yu, Q.; Dai, R.; Pei, X. Lactococcus Lactis Expressing Food-Grade β-Galactosidase Alleviates Lactose Intolerance Symptoms in Post-Weaning Balb/c Mice. Appl. Microbiol. Biotechnol. 2012, 96, 1499–1506. [Google Scholar] [CrossRef] [PubMed]
- Kavas, N. Functional Probiotic Yoghurt Production with Royal Jelly Fortification and Determination of Some Properties. Int. J. Gastron. Food Sci. 2022, 28, 100519. [Google Scholar] [CrossRef]
- Oak, S.J.; Jha, R. The Effects of Probiotics in Lactose Intolerance: A Systematic Review–The Effects of Probiotics in Lactose Intolerance: A Systematic Review. Crit. Rev. Food Sci. Nutr. 2018, 8398, 1425977. [Google Scholar] [CrossRef]
- Hassan, A.A.M.; Elenany, Y.E.; Nassrallah, A.; Cheng, W.; Abd El-Maksoud, A.A. Royal Jelly Improves the Physicochemical Properties and Biological Activities of Fermented Milk with Enhanced Probiotic Viability. LWT 2022, 155, 112912. [Google Scholar] [CrossRef]
- Vazhacharickal, J.P. A Review on Health Benefits and Biological Action of Honey, Propolis and Royal Jelly. J. Med. Plants Stud. 2021, 9, 1–13. [Google Scholar]
- Ali, M.W.; Sabir, A.M.; Gadour, M.O. Gum Arabic in Treatment of Functional Constipation in Children in Sudan. Sudan JMS 2012, 8, 73–76. [Google Scholar]
- Postali, E.; Peroukidou, P.; Giaouris, E.; Papachristoforou, A. Investigating Possible Synergism in the Antioxidant and Antibacterial Actions of Honey and Propolis from the Greek Island of Samothrace through Their Combined Application. Foods 2022, 11, 2041. [Google Scholar] [CrossRef]
- Guo, J.; Wang, Z.; Chen, Y.; Cao, J.; Tian, W.; Ma, B.; Dong, Y. Active Components and Biological Functions of Royal Jelly. J. Funct. Foods 2021, 82, 104514. [Google Scholar] [CrossRef]
- Bílikova, K.; Huang, S.-C.; Lin, I.-P.; Šimuth, J.; Peng, C.-C. Structure and Antimicrobial Activity Relationship of Royalisin, an Antimicrobial Peptide from Royal Jelly of Apis Mellifera. Peptides 2015, 86, 190–196. [Google Scholar] [CrossRef]
- Chantawannakul, P. From Entomophagy to Entomotherapy. Front. Biosci. 2020, 25, 179–200. [Google Scholar] [CrossRef]
- Sofiabadi, M.; Samiee-Rad, F. Royal Jelly Accelerates Healing of Acetate Induced Gastric Ulcers in Male Rats. Gastroenterol. Hepatol. Bed Bench 2020, 13, 18–22. [Google Scholar] [CrossRef]
- Abd El-Naeem, A. Effect of Nicotine on the Structure of Gastric Mucosa of Adult Male Albino Rats and the Possible Protective Effect of Royal Jelly (Light and Scanning Electron Microscopic Study). Egypt. J. Histol. 2021, 45, 404–415. [Google Scholar] [CrossRef]
- Ahmed, W.M.S.; Khalaf, A.A.; Moselhy, W.A.; Safwat, G.M. Royal Jelly Attenuates Azathioprine Induced Toxicity in Rats. Environ. Toxicol. Pharmacol. 2014, 37, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Felemban, A.H.; Alshammari, G.M.; Yagoub, A.E.G.A.; Al-Harbi, L.N.; Alhussain, M.H.; Yahya, M.A. Activation of AMPK Entails the Protective Effect of Royal Jelly against High-Fat-Diet-Induced Hyperglycemia, Hyperlipidemia, and Non-Alcoholic Fatty Liver Disease in Rats. Nutrients 2023, 15, 1471. [Google Scholar] [CrossRef] [PubMed]
- Fang, C.; Pan, J.; Qu, N.; Lei, Y.; Han, J.; Zhang, J.; Han, D. The AMPK Pathway in Fatty Liver Disease. Front. Physiol. 2022, 13, 970292. [Google Scholar] [CrossRef]
- Bahaaldin-Beygi, M.; Kariminik, A.; Arababadi, M.K. Royal Jelly Significantly Alters Inflammasome Pathways in Patients with Chronic Hepatitis B. Indian J. Exp. Biol. 2022, 60, 875–879. [Google Scholar]
- Ezzati, M.; Obermeyer, Z.; Tzoulaki, I.; Mayosi, B.M.; Elliott, P.; Leon, D.A. Contributions of Risk Factors and Medical Care to Cardiovascular Mortality Trends. Nat. Rev. Cardiol. 2015, 12, 508–530. [Google Scholar] [CrossRef] [PubMed]
- Townsend, N.; Kazakiewicz, D.; Lucy Wright, F.; Timmis, A.; Huculeci, R.; Torbica, A.; Gale, C.P.; Achenbach, S.; Weidinger, F.; Vardas, P. Epidemiology of Cardiovascular Disease in Europe. Nat. Rev. Cardiol. 2022, 19, 133–143. [Google Scholar] [CrossRef]
- Aslan, A.; Beyaz, S.; Gok, O.; Can, M.I.; Parlak, G.; Ozercan, I.H.; Gundogdu, R. Royal Jelly Abrogates Flouride-Induced Oxidative Damage in Rat Heart Tissue by Activating of the Nrf-2/NF-ΚB and Bcl-2/Bax Pathway. Toxicol. Mech. Methods 2021, 31, 644–654. [Google Scholar] [CrossRef]
- Fan, P.; Han, B.; Feng, M.; Fang, Y.; Zhang, L.; Hu, H.; Hao, Y.; Qi, Y.; Zhang, X.; Li, J. Functional and Proteomic Investigations Reveal Major Royal Jelly Protein 1 Associated with Anti-Hypertension Activity in Mouse Vascular Smooth Muscle Cells. Sci. Rep. 2016, 6, 30230–30241. [Google Scholar] [CrossRef]
- Matsui, T.; Yukiyoshi, A.; Doi, S.; Sugimoto, H.; Yamada, H.; Matsumoto, K. Gastrointestinal Enzyme Production of Bioactive Peptides from Royal Jelly Protein and Their Antihypertensive Ability in SHR. J. Nutr. Biochem. 2002, 13, 80–86. [Google Scholar] [CrossRef]
- Lin, N.; Chen, S.; Zhang, H.; Li, J.; Fu, L. Quantification of Major Royal Jelly Protein 1 in Fresh Royal Jelly by Ultraperformance Liquid Chromatography-Tandem Mass Spectrometry. J. Agric. Food Chem. 2018, 66, 1270–1278. [Google Scholar] [CrossRef]
- Feng, M.; Fang, Y.; Han, B.; Xu, X.; Fan, P.; Hao, Y.; Qi, Y.; Hu, H.; Huo, X.; Meng, L.; et al. In-Depth N-Glycosylation Reveals Species-Specific Modifications and Functions of the Royal Jelly Protein from Western (Apis mellifera) and Eastern Honeybees (Apis cerana). J. Proteome Res. 2015, 14, 5327–5340. [Google Scholar] [CrossRef]
- Escamilla, K.I.A.; Ordóñez, Y.B.M.; Sandoval-Peraza, V.M.; Fernández, J.J.A.; Ancona, D.A.B. Anti-Hypertensive Activity in Vitro and in Vivo on Royal Jelly Produced by Different Diets. Emir. J. Food Agric. 2022, 34, 9–15. [Google Scholar] [CrossRef]
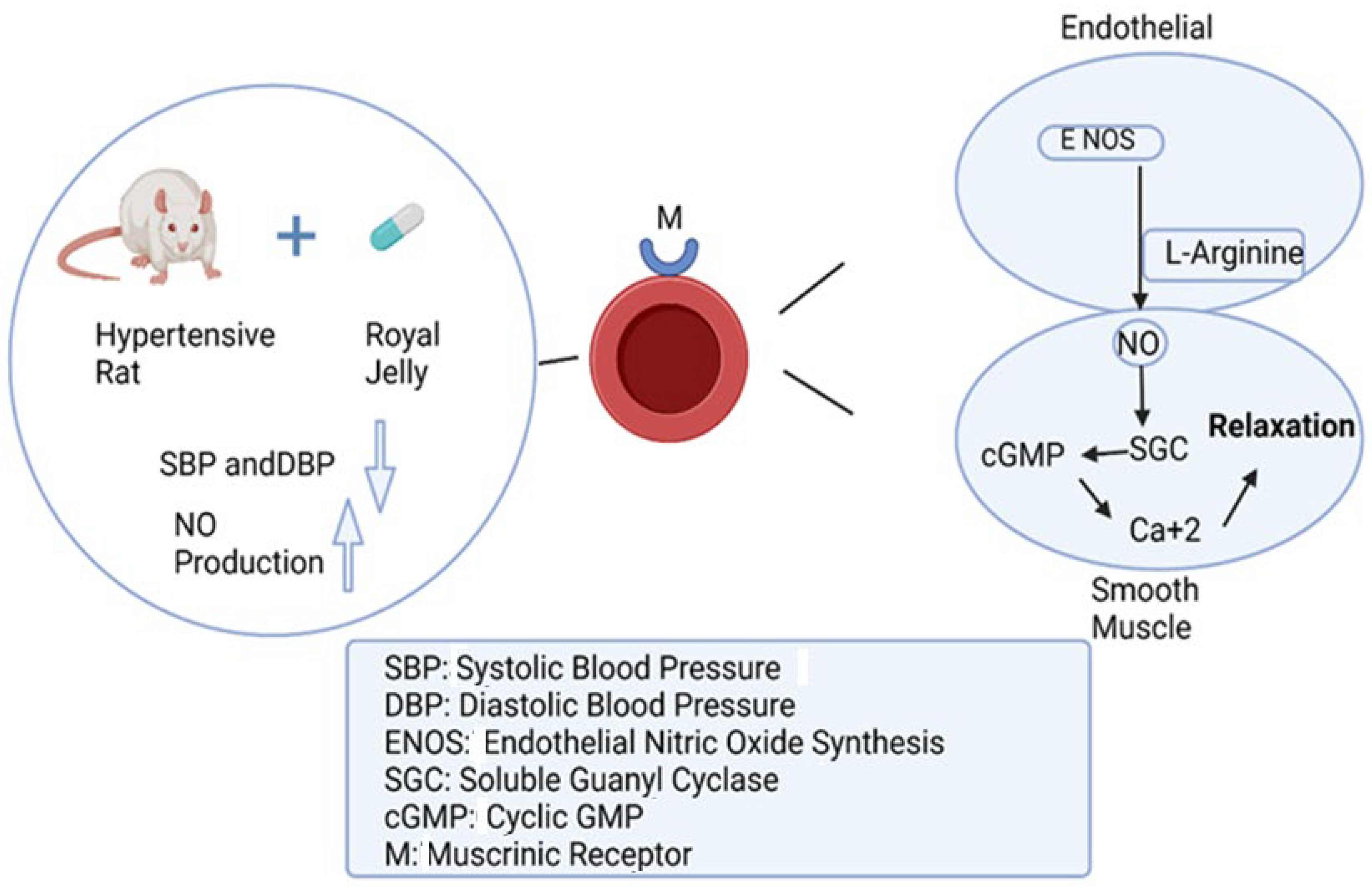
- Pan, Y.; Rong, Y.; You, M.; Ma, Q.; Chen, M.; Hu, F. Royal Jelly Causes Hypotension and Vasodilation Induced by Increasing Nitric Oxide Production. Food Sci. Nutr. 2019, 7, 1361–1370. [Google Scholar] [CrossRef]
- Wei, W.; Wei, M.; Kang, X.; Deng, H.; Lu, Z. A Novel Method Developed for Acetylcholine Detection in Royal Jelly by Using Capillary Electrophoresis Coupled with Electrogenerated Chemiluminescence Based on a Simple Reaction. Electrophoresis 2009, 30, 1949–1952. [Google Scholar] [CrossRef]
- Fujisue, K.; Yamamoto, E.; Sueta, D.; Arima, Y.; Hirakawa, K.; Tabata, N.; Ishii, M.; Ito, M.; Yamanaga, K.; Hanatani, S.; et al. A Randomized, Double-Blind Comparison Study of Royal Jelly to Augment Vascular Endothelial Function in Healthy Volunteers. J. Atheroscler. Thromb. 2022, 29, 1285–1294. [Google Scholar] [CrossRef] [PubMed]
- Roman, W.A.; Piato, A.L.; Conterato, G.M.M.; Wildner, S.M.; Marcon, M.; Mocelin, R.; Emanuelli, M.P.; Emanuelli, T.; Nepel, A.; Barison, A.; et al. Hypolipidemic Effects of Solidago Chilensis Hydroalcoholic Extract and Its Major Isolated Constituent Quercetrin in Cholesterol-Fed Rats. Pharm. Biol. 2015, 53, 1488–1495. [Google Scholar] [CrossRef] [PubMed]
- Kamakura, M.; Moriyama, T.; Sakaki, T. Changes in Hepatic Gene Expression Associated with the Hypocholesterolaemic Activity of Royal Jelly. J. Pharm. Pharmacol. 2010, 58, 1683–1689. [Google Scholar] [CrossRef]
- Kashima, Y.; Kanematsu, S.; Asai, S.; Kusada, M.; Watanabe, S.; Kawashima, T.; Nakamura, T.; Shimada, M.; Goto, T.; Nagaoka, S. Identification of a Novel Hypocholesterolemic Protein, Major Royal Jelly Protein 1, Derived from Royal Jelly. PLoS ONE 2014, 9, e105073–e105084. [Google Scholar] [CrossRef] [PubMed]
- Chiu, H.F.; Chen, B.K.; Lu, Y.Y.; Han, Y.C.; Shen, Y.C.; Venkatakrishnan, K.; Golovinskaia, O.; Wang, C.K. Hypocholesterolemic Efficacy of Royal Jelly in Healthy Mild Hypercholesterolemic Adults. Pharm. Biol. 2017, 55, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Bălan, A.; Moga, M.A.; Dima, L.; Toma, S.; Neculau, A.E.; Anastasiu, C.V. Royal Jelly–A Traditional and Natural Remedy for Postmenopausal Symptoms and Aging-Related Pathologies. Molecules 2020, 25, 3291. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
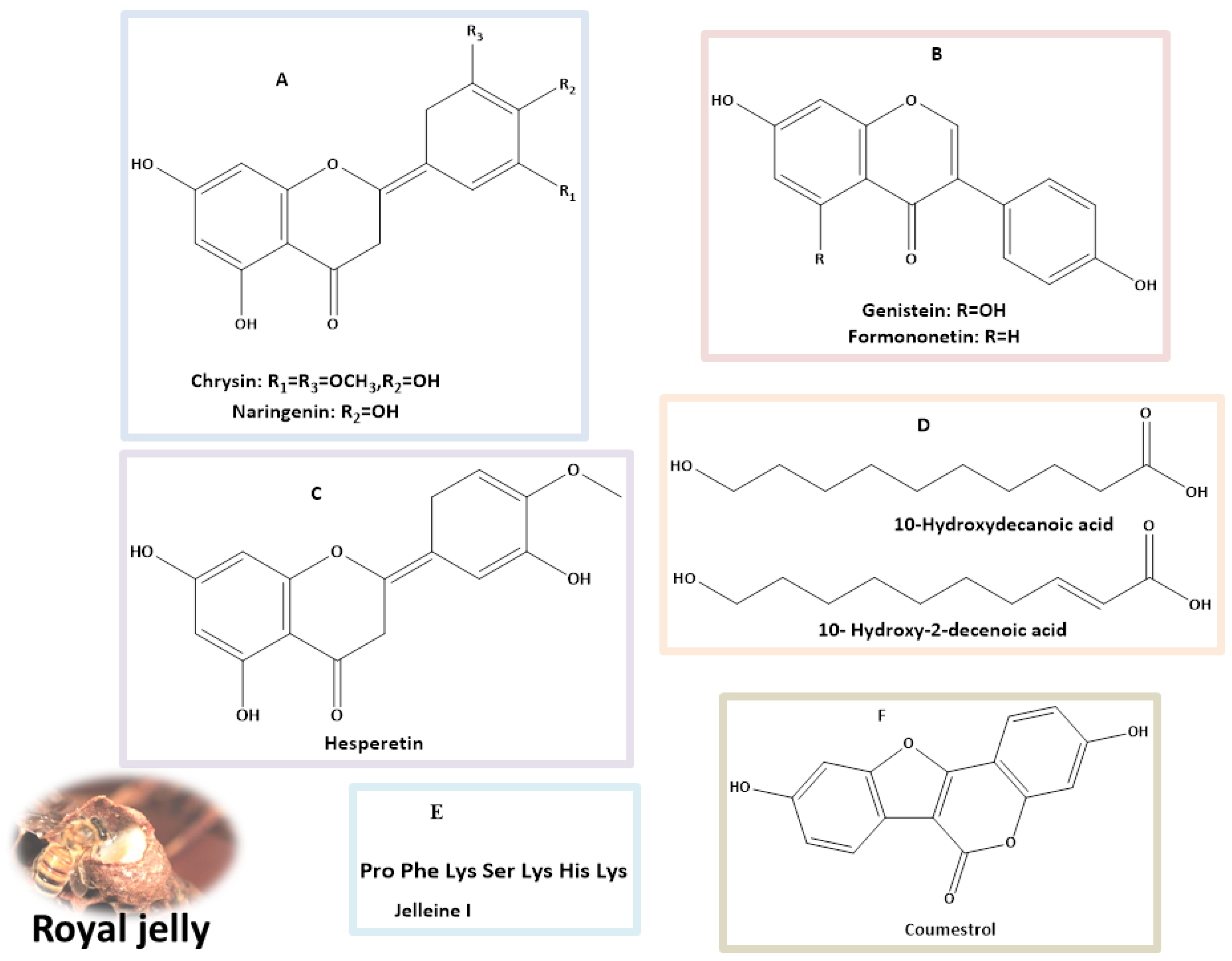
| Identified Compounds | Dosage | Biological Activity (In Vitro/In Vivo) | References |
|---|---|---|---|
| Hesperetin | 40 mg/kg body weight (BW) for 45 days | Reduces high blood sugar and lipid levels by enhancing insulin secretion (in vivo). | [42,43] |
| Naringenin | (25, 50, 100 mg/kg) for 4 weeks | The therapy significantly enhanced the control of blood glucose levels and also contributed to the recovery of BWin diabetic rats, in contrast to those that received a vehicle treatment (in vivo). | [43,44] |
| 50 mg/kg for 4 weeks | Adequate to mitigate the alterations in the lenses caused by diabetes-related oxidative stress (in vivo). | [45] | |
| 50 mg/kg/day for 5 days | Significant decrease in blood glucose and triglyceride levels in diabetic rats (in vivo). | [46] | |
| 100 mg/kg BW /day for 4 weeks | Restored the serum insulin and C-peptide levels, replenished liver glycogen, and reduced glucose-6-phosphatase and glycogen phosphorylase activity in the liver. Additionally, it improved the serum lipid profile and strengthened the liver’s antioxidant defense system (in vivo). | [47] | |
| Genistein | (20 and 40 mg/kg) for 8 weeks. | Improved glucose tolerance, blood glucose levels, insulin, glucagon, lipid profiles, and pro-inflammatory factors. It also improved liver function, reduced inflammation in the liver and colon, and positively altered gut microbiota composition (in vivo). | [43,48] |
| 25–200 mg/day | Improved hyperglycemia, glucose tolerance, and blood insulin levels, along with enhancing islet beta-cell proliferation, survival, and mass (in vivo). | [49] | |
| 600 mg/kg for 4 weeks | Enhanced insulin sensitivity and increased expression of neurotrophic factors, such as nerve growth factor (NGF) and brain-derived neurotrophic factors (BDNF) (in vivo). | [50] | |
| Formononetin | 20 mg/kg for 28 days | Reduced serum glucose levels and increased serum insulin compared to the control group. It also decreased insulin resistance and reduced fasting glucose (C57BL/6 mice, in vivo). | [43,51] |
| 40 mg/kg/day for 16 weeks | Decreased insulin resistance and regulated hypoglycemia in male rats with diabetes (in vivo). | [52] | |
| Coumestrol | 50 µM | Improved hepatic insulin resistance in primary at hepatocyte (in vivo). | [43,53] |
| Chrysin | 100 mg/kg | It resulted in a reduction of fasting blood glucose and insulin levels in db/db mice when compared to the control group (in vivo). | [43,54] |
| 80 mg/kg BW for 10 days | Anti-diabetic effects via increasing insulin levels, reducing oxidative stress, and regulating the inflammatory pathway (in vivo). | [55] | |
| 10-Hydroxy-2-decenoic acid | 100 mg per kg BW/Daily for 4 weeks. | Decreased fasting blood glucose and increased insulin levels in diabetic mice. Enhanced activity of crucial antioxidants in the livers of diabetic mice, such as superoxide dismutase, catalase, and glutathione peroxidase (in vivo). | [39,56] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El-Seedi, H.R.; Salama, S.; El-Wahed, A.A.A.; Guo, Z.; Di Minno, A.; Daglia, M.; Li, C.; Guan, X.; Buccato, D.G.; Khalifa, S.A.M.; et al. Exploring the Therapeutic Potential of Royal Jelly in Metabolic Disorders and Gastrointestinal Diseases. Nutrients 2024, 16, 393. https://doi.org/10.3390/nu16030393
El-Seedi HR, Salama S, El-Wahed AAA, Guo Z, Di Minno A, Daglia M, Li C, Guan X, Buccato DG, Khalifa SAM, et al. Exploring the Therapeutic Potential of Royal Jelly in Metabolic Disorders and Gastrointestinal Diseases. Nutrients. 2024; 16(3):393. https://doi.org/10.3390/nu16030393
Chicago/Turabian StyleEl-Seedi, Hesham R., Suzy Salama, Aida A. Abd El-Wahed, Zhiming Guo, Alessandro Di Minno, Maria Daglia, Chuan Li, Xiao Guan, Daniele Giuseppe Buccato, Shaden A. M. Khalifa, and et al. 2024. "Exploring the Therapeutic Potential of Royal Jelly in Metabolic Disorders and Gastrointestinal Diseases" Nutrients 16, no. 3: 393. https://doi.org/10.3390/nu16030393
APA StyleEl-Seedi, H. R., Salama, S., El-Wahed, A. A. A., Guo, Z., Di Minno, A., Daglia, M., Li, C., Guan, X., Buccato, D. G., Khalifa, S. A. M., & Wang, K. (2024). Exploring the Therapeutic Potential of Royal Jelly in Metabolic Disorders and Gastrointestinal Diseases. Nutrients, 16(3), 393. https://doi.org/10.3390/nu16030393