
Knowledge of Dietitians on Gut Microbiota in Health—An Online Survey of the European Federation of the Associations of Dietitians (EFAD)


Highlights
- Significant positive correlations were indicated between the perceived and current knowledge of participants about the gut microbiota.
- Participants had a rather low current knowledge about probiotics and prebiotics, with dietitians tending to have a higher score compared to pre-graduate students or other professionals.
- Being a dietitian, having a higher educational level as a dietitian and working in an academic/research setting were usually associated with more knowledge about the gut microbiota.
- Being a dietitian working in an academic or research setting was an independent factor for scoring in the highest quartile in all tested sections and overall.
- The data highlighted the level and potential determinants of the current knowledge of European dietitians about parameters related to the gut microbiota, including dietary modulation.
- Areas for future educational efforts were indicated based on the detected knowledge gaps.
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Survey Questionnaire
2.3. Survey Communication Plan
2.4. Statistical Analysis
3. Results
3.1. Responses
3.2. Sociodemographic Data (Country/Region—Participants’ Characteristics)
3.3. Level of Knowledge about Gut Health in Overall Health, Nutrition as a Gut Microbiota Modulator, and Probiotics/Prebiotics in Health
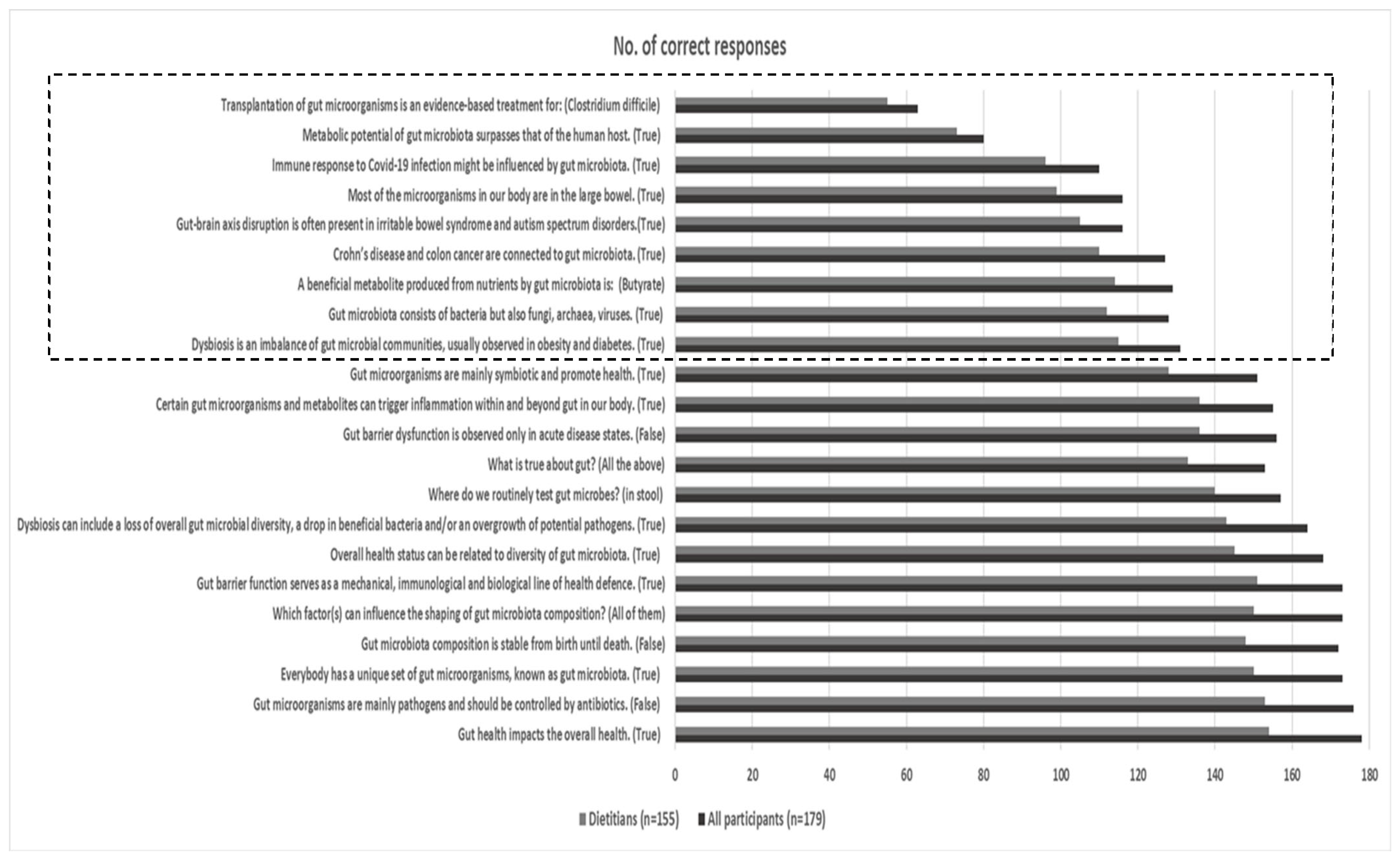
3.3.1. Section: The Role of Gut Health in Overall Health
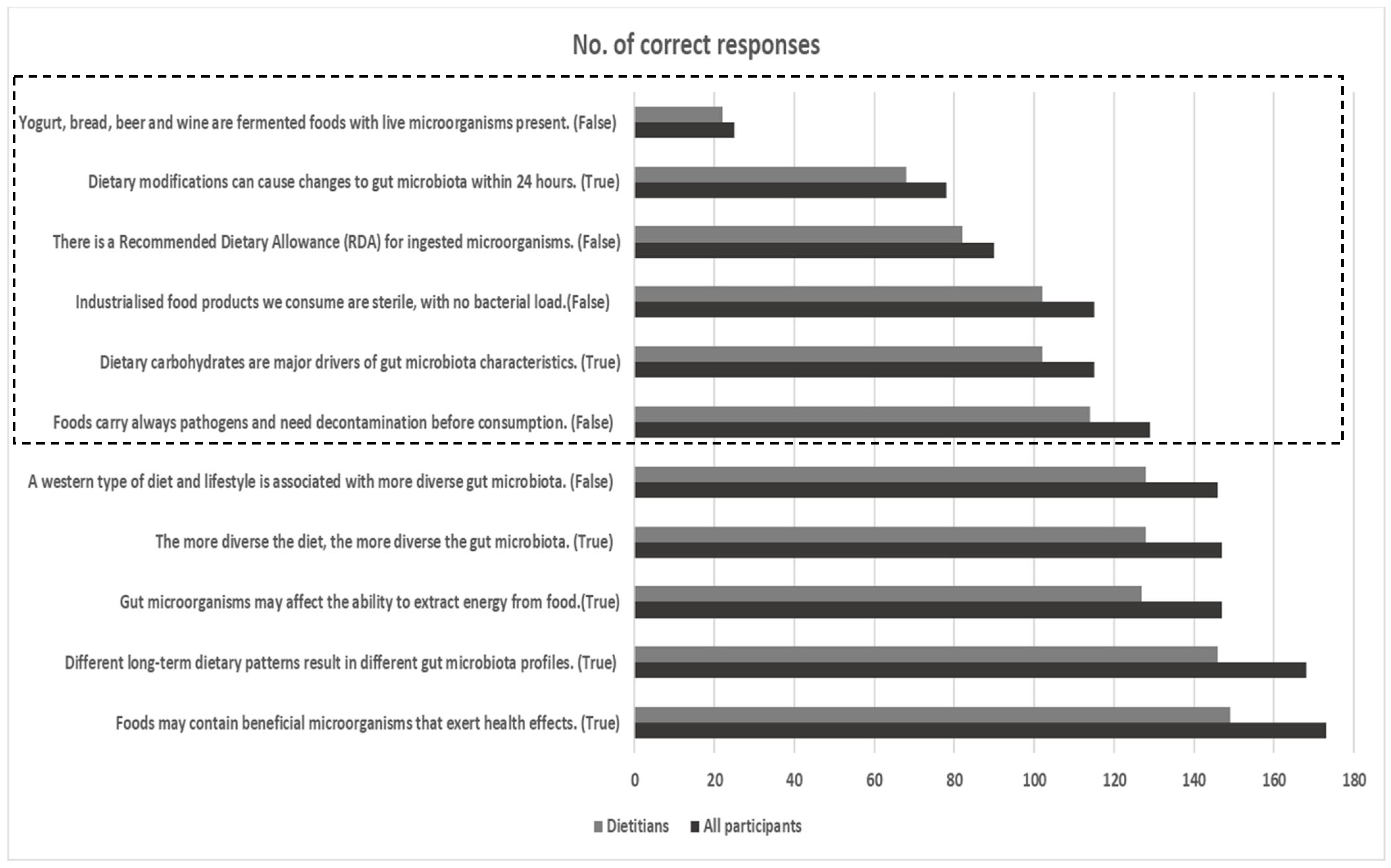
3.3.2. Section: The Role of Nutrition as Gut Microbiota Modulator
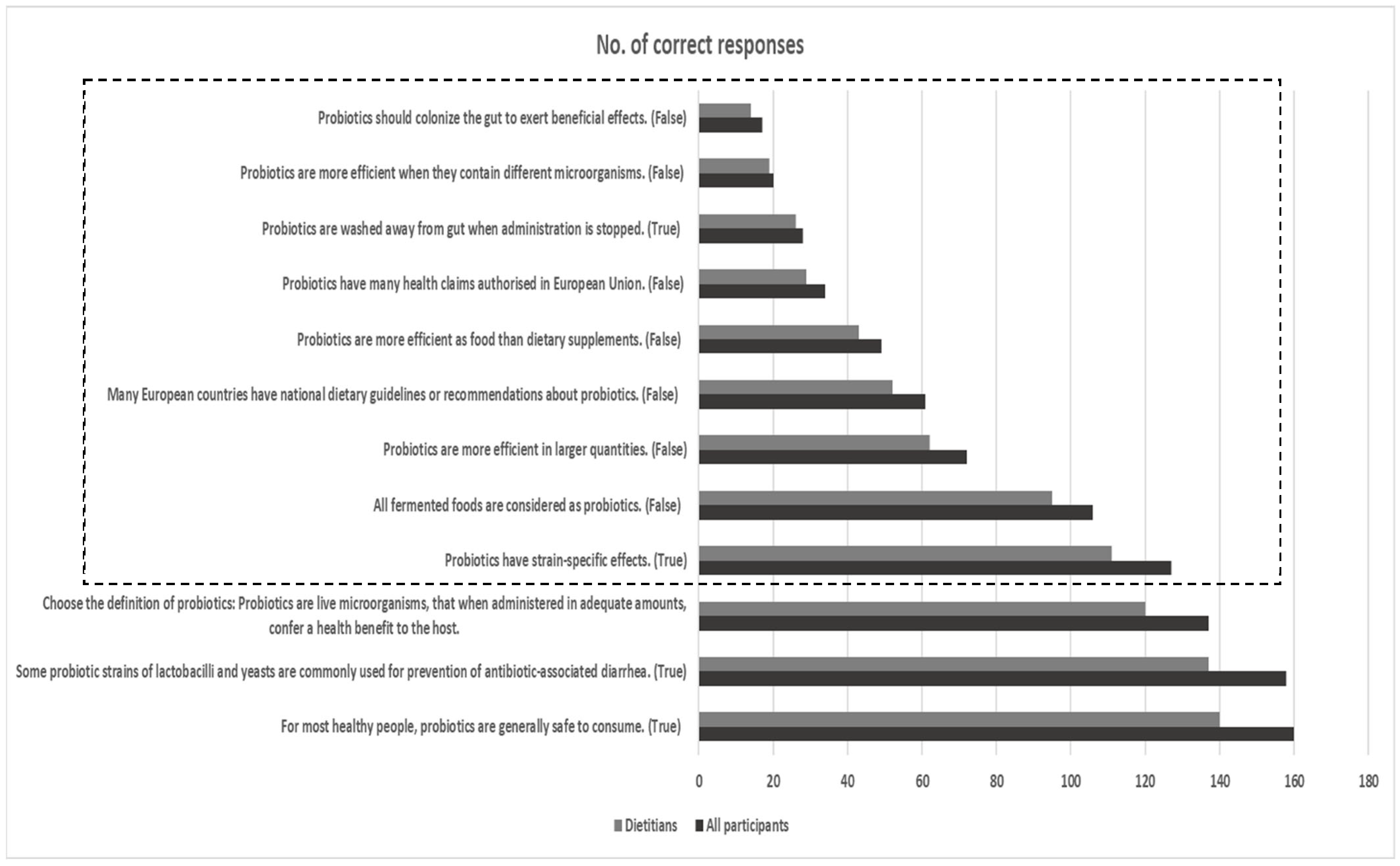
3.3.3. Section: The Role of Probiotics in Health
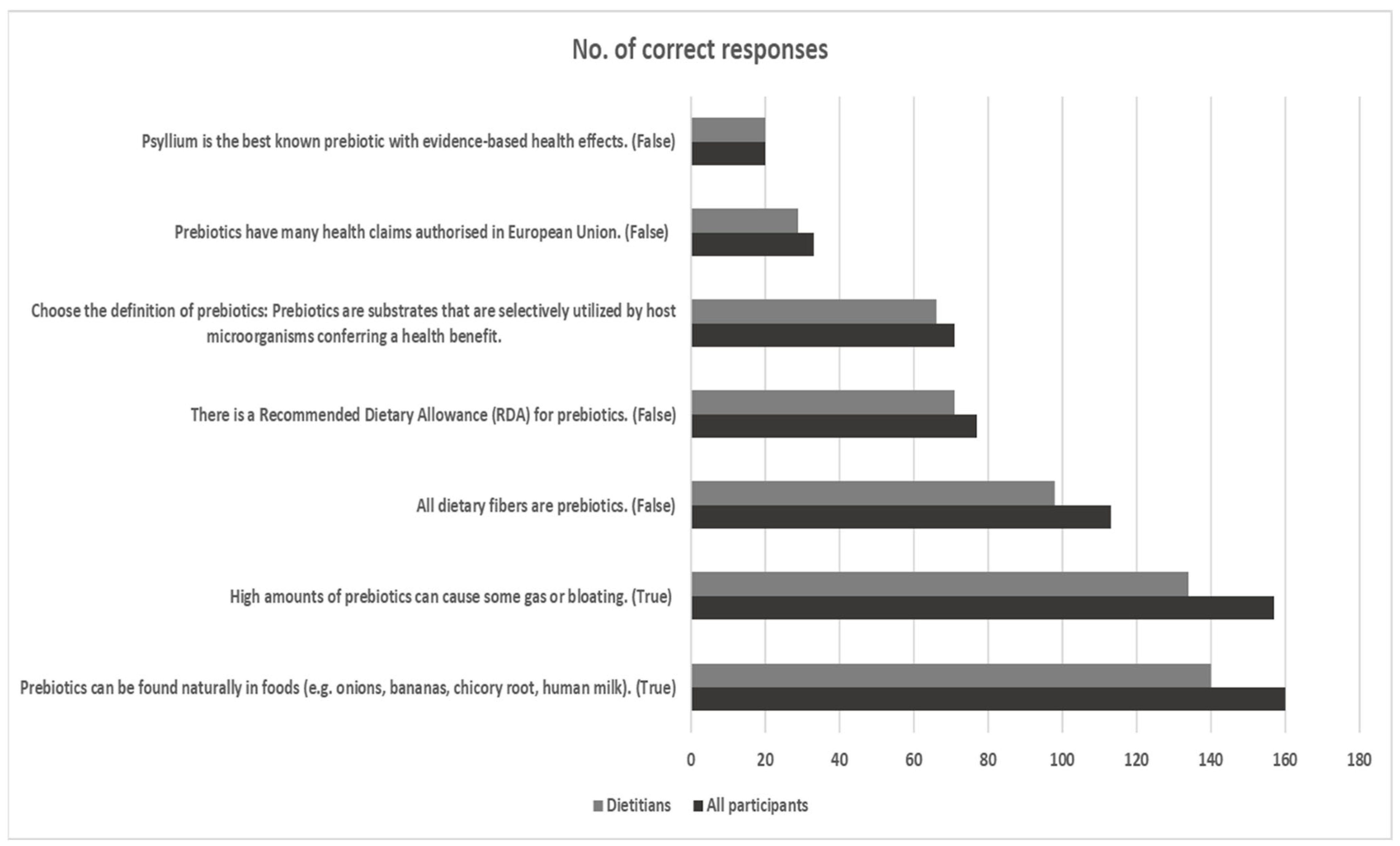
3.3.4. Section: The Role of Prebiotics in Health
3.3.5. Overall Perceived Knowledge and Total Score of Knowledge
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bischoff, S.C. ‘Gut health’: A new objective in medicine? BMC Med. 2011, 9, 24. [Google Scholar] [CrossRef] [PubMed]
- König, J.; Wells, J.; Cani, P.D.; García-Ródenas, C.L.; MacDonald, T.; Mercenier, A.; Whyte, J.; Troost, F.; Brummer, R.J. Human Intestinal Barrier Function in Health and Disease. Clin. Transl. Gastroenterol. 2016, 7, e196. [Google Scholar] [CrossRef] [PubMed]
- Viggiano, D.; Ianiro, G.; Vanella, G.; Bibbò, S.; Bruno, G.; Simeone, G.; Mele, G. Gut barrier in health and disease: Focus on childhood. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 1077–1085. [Google Scholar] [PubMed]
- Kho, Z.Y.; Lal, S.K. The Human Gut Microbiome—A Potential Controller of Wellness and Disease. Front. Microbiol. 2018, 9, 1835. [Google Scholar] [CrossRef]
- Thursby, E.; Juge, N. Introduction to the human gut microbiota. Biochem. J. 2017, 474, 1823–1836. [Google Scholar] [CrossRef] [PubMed]
- Hughes, R.L.; Davis, C.D.; Lobach, A.; Holscher, H.D. An Overview of Current Knowledge of the Gut Microbiota and Low-Calorie Sweeteners. Nutr. Today 2021, 56, 105–113. [Google Scholar] [CrossRef]
- Conlon, M.A.; Bird, A.R. The impact of diet and lifestyle on gut microbiota and human health. Nutrients 2015, 7, 17–44. [Google Scholar] [CrossRef]
- Cunningham, M.; Azcarate-Peril, M.A.; Barnard, A.; Benoit, V.; Grimaldi, R.; Guyonnet, D.; Holscher, H.D.; Hunter, K.; Manurung, S.; Obis, D.; et al. Shaping the Future of Probiotics and Prebiotics. Trends Microbiol. 2021, 29, 667–685. [Google Scholar] [CrossRef]
- Fijan, S.; Frauwallner, A.; Varga, L.; Langerholc, T.; Rogelj, I.; Lorber, M.; Lewis, P.; Povalej Bržan, P. Health Professionals’ Knowledge of Probiotics: An International Survey. Int. J. Environ. Res. Public Health 2019, 16, 3128. [Google Scholar] [CrossRef]
- Jordan, D.; Johnson, N.; Thomas, L. Probiotics in primary care: A survey of health professionals. Pract. Nurs. 2015, 26, 550–554. [Google Scholar] [CrossRef]
- Oliver, L.; Rasmussen, H.; Gregoire, M.B.; Chen, Y. Health Care Provider’s Knowledge, Perceptions, and Use of Probiotics and Prebiotics. Top. Clin. Nutr. 2014, 29, 139–149. [Google Scholar] [CrossRef]
- Pettoello-Mantovani, M.; Çullu Çokuğraş, F.; Vural, M.; Mestrovic, J.; Nigri, L.; Piazzolla, R.; Giardino, I.; Conoscitore, M.; Namazova-Baranova, L. Pilot study for the understanding and use of probiotics by different paediatric healthcare professionals working in different European countries. Ital. J. Pediatr. 2019, 45, 57. [Google Scholar] [CrossRef] [PubMed]
- Valdovinos-García, L.R.; Abreu, A.T.; Valdovinos-Díaz, M.A. Probiotic use in clinical practice: Results of a national survey of gastroenterologists and nutritionists. Rev. Gastroenterol. Méx. 2019, 84, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Wilson, Z.; Whitehead, K. A cross sectional survey to assess healthcare professionals’ attitudes to and understanding of probiotics. Clin. Nutr. ESPEN 2019, 34, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Hojsak, I.; Fabiano, V.; Pop, T.L.; Goulet, O.; Zuccotti, G.V.; Çokuğraş, F.C.; Pettoello-Mantovani, M.; Kolaček, S. Guidance on the use of probiotics in clinical practice in children with selected clinical conditions and in specific vulnerable groups. Acta Paediatr. 2018, 107, 927–937. [Google Scholar] [CrossRef] [PubMed]
- Hungin, A.P.S.; Mitchell, C.R.; Whorwell, P.; Mulligan, C.; Cole, O.; Agréus, L.; Fracasso, P.; Lionis, C.; Mendive, J.; Philippart de Foy, J.M.; et al. Systematic review: Probiotics in the management of lower gastrointestinal symptoms—An updated evidence-based international consensus. Aliment. Pharmacol. Ther. 2018, 47, 1054–1070. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, Y.A.; Thompson, J.; Gulia, P.; Lomer, M.C.; IBS Dietetic Guideline Review Group on behalf of Gastroenterology Specialist Group of the British Dietetic Association. British Dietetic Association systematic review of systematic reviews and evidence-based practice guidelines for the use of probiotics in the management of irritable bowel syndrome in adults (2016 update). J. Hum. Nutr. Diet. 2016, 29, 576–592. [Google Scholar] [CrossRef]
- Su, G.L.; Ko, C.W.; Bercik, P.; Falck-Ytter, Y.; Sultan, S.; Weizman, A.V.; Morgan, R.L. AGA Clinical Practice Guidelines on the Role of Probiotics in the Management of Gastrointestinal Disorders. Gastroenterology 2020, 159, 697–705. [Google Scholar] [CrossRef]
- van den Akker, C.H.P.; van Goudoever, J.B.; Shamirm, R.; Domellöf, M.; Embleton, N.D.; Hojsak, I.; Lapillonne, A.; Mihatsch, W.A.; Berni Canani, R.; Bronsky, J.; et al. Probiotics and Preterm Infants: A Position Paper by the European Society for Paediatric Gastroenterology Hepatology and Nutrition Committee on Nutrition and the European Society for Paediatric Gastroenterology Hepatology and Nutrition Working Group for Probiotics and Prebiotics. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 664–680. [Google Scholar] [CrossRef]
- World Gastroenterology Organization. World Gastroenterology Organization Global Guidelines Probiotics and Prebiotics. 2017. Available online: https://www.worldgastroenterology.org/guidelines/probiotics-and-prebiotics/probiotics-and-prebiotics-english (accessed on 1 February 2021).
- StataCorp. Stata Statistical Software: Release 15; StataCorp LLC.: College Station, TX, USA, 2017. [Google Scholar]
- Evans, J.R.; Mathur, A. The value of online surveys: A look back and a look ahead. Internet Res. 2018, 28, 854–887. [Google Scholar] [CrossRef]
- Agus, A.; Clément, K.; Sokol, H. Gut microbiota-derived metabolites as central regulators in metabolic disorders. Gut 2021, 70, 1174–1182. [Google Scholar] [CrossRef]
- Cani, P.D.; Osto, M.; Geurts, L.; Everard, A. Involvement of gut microbiota in the development of low-grade inflammation and type 2 diabetes associated with obesity. Gut Microbes 2012, 3, 279–288. [Google Scholar] [CrossRef]
- Clapp, M.; Aurora, N.; Herrera, L.; Bhatia, M.; Wilen, E.; Wakefield, S. Gut microbiota’s effect on mental health: The gut-brain axis. Clin. Pract. 2017, 7, 987. [Google Scholar] [CrossRef]
- Singh, R.; Zogg, H.; Wei, L.; Bartlett, A.; Ghoshal, U.C.; Rajender, S.; Ro, S. Gut Microbial Dysbiosis in the Pathogenesis of Gastrointestinal Dysmotility and Metabolic Disorders. J. Neurogastroenterol. Motil. 2021, 27, 19–34. [Google Scholar] [CrossRef]
- Yeoh, Y.K.; Zuo, T.; Lui, G.C.; Zhang, F.; Liu, Q.; Li, A.Y.; Chung, A.C.; Cheung, C.P.; Tso, E.Y.; Fung, K.S.; et al. Gut microbiota composition reflects disease severity and dysfunctional immune responses in patients with COVID-19. Gut 2021, 70, 698–706. [Google Scholar] [CrossRef] [PubMed]
- Sbahi, H.; Di Palma, J.A. Faecal microbiota transplantation: Applications and limitations in treating gastrointestinal disorders. BMJ Open Gastroenterol. 2016, 3, e000087. [Google Scholar] [CrossRef] [PubMed]
- Clancy, A.K.; Gunaratne, A.W.; Borody, T.J. Dietary Management for Faecal Microbiota Transplant: An International Survey of Clinical and Research Practice, Knowledge and Attitudes. Front. Nutr. 2021, 8, 653653. [Google Scholar] [CrossRef]
- Aaliya, B.; Valiyapeediyekkal Sunooj, K.; Navaf, M.; Parambil Akhila, P.; Sudheesh, C.; Ahmad Mir, S.; Sabu, S.; Sasidharan, A.; Theingi Hlaing, M.; George, J. Recent trends in bacterial decontamination of food products by hurdle technology: A synergistic approach using thermal and non-thermal processing techniques. Food Res. Int. 2021, 147, 110514. [Google Scholar] [CrossRef] [PubMed]
- Jumpertz, R.; Le, D.S.; Turnbaugh, P.J.; Trinidad, C.; Bogardus, C.; Gordon, J.I.; Krakoff, J. Energy-balance studies reveal associations between gut microbes, caloric load, and nutrient absorption in humans. Am. J. Clin. Nutr. 2011, 94, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.K.; Chang, H.W.; Yan, D.; Lee, K.M.; Ucmak, D.; Wong, K.; Abrouk, M.; Farahnik, B.; Nakamura, M.; Zhu, T.H.; et al. Influence of diet on the gut microbiome and implications for human health. J. Transl. Med. 2017, 15, 73. [Google Scholar] [CrossRef] [PubMed]
- Leeming, E.R.; Johnson, A.J.; Spector, T.D.; Le Roy, C.I. Effect of Diet on the Gut Microbiota: Rethinking Intervention Duration. Nutrients 2019, 11, 2862. [Google Scholar] [CrossRef]
- Marco, M.L.; Sanders, M.E.; Gänzle, M.; Arrieta, M.C.; Cotter, P.D.; De Vuyst, L.; Hill, C.; Holzapfel, W.; Lebeer, S.; Merenstein, D.; et al. The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on fermented foods. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 196–208. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on the substantiation of health claims related to live yoghurt cultures and improved lactose digestion (ID 1143, 2976) pursuant to Article 13(1) of Regulation (EC) No 1924/2006. EFSA J. 2010, 8, 1763. [Google Scholar] [CrossRef]
- Hill, C. RDA for microbes—Are you getting your daily dose? Biochemist 2018, 40, 22–25. [Google Scholar] [CrossRef]
- Marco, M.L.; Hill, C.; Hutkins, R.; Slavin, J.; Tancredi, D.J.; Merenstein, D.; Sanders, M.E. Should There Be a Recommended Daily Intake of Microbes? J. Nutr. 2020, 150, 3061–3067. [Google Scholar] [CrossRef] [PubMed]
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. Expert consensus document. The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 506–514. [Google Scholar] [CrossRef] [PubMed]
- Binda, S.; Hill, C.; Johansen, E.; Obis, D.; Pot, B.; Sanders, M.E.; Tremblay, A.; Ouwehand, A.C. Criteria to Qualify Microorganisms as “Probiotic” in Foods and Dietary Supplements. Front. Microbiol. 2020, 11, 1662. [Google Scholar] [CrossRef] [PubMed]
- Soni, R.; Tank, K.; Jain, N. Knowledge, attitude and practice of health professionals about probiotic use in Ahmedabad, India. Nutr. Food Sci. 2018, 48, 125–135. [Google Scholar] [CrossRef]
- Ciorba, M.A. A gastroenterologist’s guide to probiotics. Clin. Gastroenterol. Hepatol. 2012, 10, 960–968. [Google Scholar] [CrossRef]
- Suez, J.; Zmora, N.; Segal, E.; Elinav, E. The pros, cons, and many unknowns of probiotics. Nat. Med. 2019, 25, 716–729. [Google Scholar] [CrossRef] [PubMed]
- Sniffen, J.C.; McFarland, L.V.; Evans, C.T.; Goldstein, E.J.C. Choosing an appropriate probiotic product for your patient: An evidence-based practical guide. PLoS ONE 2018, 13, e0209205. [Google Scholar] [CrossRef]
- Glanville, J.; King, S.; Guarner, F.; Hill, C.; Sanders, M.E. A review of the systematic review process and its applicability for use in evaluating evidence for health claims on probiotic foods in the European Union. Nutr. J. 2015, 14, 16. [Google Scholar] [CrossRef] [PubMed]
- Ebner, S.; Smug, L.N.; Kneifel, W.; Salminen, S.J.; Sanders, M.E. Probiotics in dietary guidelines and clinical recommendations outside the European Union. World J. Gastroenterol. 2014, 20, 16095–16100. [Google Scholar] [CrossRef] [PubMed]
- Smug, L.N.; Salminen, S.; Sanders, M.E.; Ebner, S. Yoghurt and probiotic bacteria in dietary guidelines of the member states of the European Union. Benef. Microbes 2014, 5, 61–66. [Google Scholar] [CrossRef]
- Betz, M.; Uzueta, A.; Rasmussen, H.; Gregoire, M.; Vanderwall, C.; Witowich, G. Inpatient knowledge and use of probiotics and prebiotics. Nutr. Diet. 2015, 72, 261–266. [Google Scholar] [CrossRef]
- Khalesi, S.; Vandelanotte, C.; Thwaite, T.; Russell, A.M.T.; Dawson, D.; Williams, S.L. Awareness and Attitudes of Gut Health, Probiotics and Prebiotics in Australian Adults. J. Diet. Suppl. 2021, 18, 418–432. [Google Scholar] [CrossRef] [PubMed]
- Precup, G.; Pocol, C.B.; Teleky, B.E.; Vodnar, D.C. Awareness, Knowledge, and Interest about Prebiotics-A Study among Romanian Consumers. Int. J. Environ. Res. Public Health 2022, 19, 1208. [Google Scholar] [CrossRef]
- Guarino, M.P.L.; Altomare, A.; Emerenziani, S.; Di Rosa, C.; Ribolsi, M.; Balestrieri, P.; Iovino, P.; Rocchi, G.; Cicala, M. Mechanisms of Action of Prebiotics and Their Effects on Gastro-Intestinal Disorders in Adults. Nutrients 2020, 12, 1037. [Google Scholar] [CrossRef]
- Gibson, G.R.; Hutkins, R.; Sanders, M.E.; Prescott, S.L.; Reimer, R.A.; Salminen, S.J.; Scott, K.; Stanton, C.; Swanson, K.S.; Cani, P.D.; et al. Expert consensus document: The International Scientific Association for Probiotics and Prebiotics (ISAPP) consensus statement on the definition and scope of prebiotics. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 491–502. [Google Scholar] [CrossRef]
- Wilson, B.; Whelan, K. Prebiotic inulin-type fructans and galacto-oligosaccharides: Definition, specificity, function, and application in gastrointestinal disorders. J. Gastroenterol. Hepatol. 2017, 32 (Suppl. S1), 64–68. [Google Scholar] [CrossRef]
- Jalanka, J.; Major, G.; Murray, K.; Singh, G.; Nowak, A.; Kurtz, C.; Silos-Santiago, I.; Johnston, J.M.; de Vos, W.M.; Spiller, R. The Effect of Psyllium Husk on Intestinal Microbiota in Constipated Patients and Healthy Controls. Int. J. Mol. Sci. 2019, 20, 433. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on the substantiation of a health claim related to “native chicory inulin” and maintenance of normal defecation by increasing stool frequency pursuant to Article 13.5 of Regulation (EC) No 1924/2006. EFSA J. 2015, 13, 3951. [Google Scholar] [CrossRef]
- Barqawi, H.J.; Adra, S.F.; Ramzi, H.R.; Abouaggour, M.A.; Almehairi, S.K. Evaluating the knowledge, attitudes and practices of the UAE community on microbiota composition and the main factors affecting it: A cross-sectional study. BMJ Open 2021, 11, e047869. [Google Scholar] [CrossRef] [PubMed]
- Alamri, A.; AlKhater, S.A. Evaluating the knowledge on microbiome and dysbiosis in allergic diseases among medical sciences students in Saudi Arabia. Clin. Mol. Allergy 2022, 20, 2. [Google Scholar] [CrossRef] [PubMed]
- Leeming, E.R.; Louca, P.; Gibson, R.; Menni, C.; Spector, T.D.; Le Roy, C.I. The complexities of the diet-microbiome relationship: Advances and perspectives. Genome Med. 2021, 13, 10. [Google Scholar] [CrossRef] [PubMed]
- Peregrin, T. The inside tract: What RDs need to know about the gut microbiome. J. Acad. Nutr. Diet. 2013, 113, 1019–1023. [Google Scholar] [CrossRef] [PubMed]
- Biocodex Microbiota Institute. The International Microbiota Observatory, 2023 Results. Available online: https://www.biocodexmicrobiotainstitute.com/en/international-microbiota-observatory (accessed on 30 November 2023).
- Williams, G.M.; Tapsell, L.C.; Beck, E.J. Dietitians’ perspectives on the role of dietetics practice in ‘gut health’. Nutr. Diet 2023, 80, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Arshad, M.S.; Saqlain, M.; Majeed, A.; Imran, I.; Saeed, H.; Saleem, M.U.; Abrar, M.A.; Islam, M.; Hashmi, F.; Akbar, M.; et al. Cross-sectional study to assess the healthcare professionals’ knowledge, attitude and practices about probiotics use in Pakistan. BMJ Open 2021, 11, e047494. [Google Scholar] [CrossRef]
- van der Geest, A.M.; Flach, J.; Claassen, E.; Sijlmans, A.W.; van de Burgwal, L.H.M.; Larsen, O.F.A. European General Practitioners perceptions on probiotics: Results of a multinational survey. PharmaNutrition 2020, 11, 100178. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants’ Characteristics | Variable Categories | Central and Eastern Europe | Northern Europe | Southern Europe | Western Europe | Total | Overall p |
|---|---|---|---|---|---|---|---|
| Age group (years) | 20–24 | 3 | 2 | 26 | 2 | 33 | <0.001 |
| 25–29 | 8 | 3 | 33 | 4 | 48 | ||
| 30–34 | 0 | 2 | 17 | 7 | 26 | ||
| 35–39 | 1 | 2 | 7 | 4 | 14 | ||
| 40–44 | 0 | 1 | 6 | 9 | 16 | ||
| 45–49 | 2 | 2 | 5 | 7 | 16 | ||
| 50–54 | 0 | 3 | 4 | 10 | 17 | ||
| 55–59 | 0 | 2 | 1 | 1 | 4 | ||
| 60–65 | 0 | 0 | 0 | 1 | 1 | ||
| Status | Dietitian | 12 | 14 | 88 | 39 | 153 | 0.274 |
| Other professional | 0 | 2 | 2 | 4 | 8 | ||
| Pre-graduate dietetic student | 2 | 1 | 9 | 2 | 14 | ||
| Educational level (dietitians) † | Dietitian, BTS | 0 | 0 | 0 | 4 | 4 | 0.130 |
| Dietitian, pre-BSc | 0 | 0 | 4 | 1 | 5 | ||
| Dietitian, BSc | 6 | 5 | 30 | 17 | 58 | ||
| Dietitian, MSc | 5 | 8 | 39 | 12 | 64 | ||
| Dietitian, PhD | 1 | 1 | 15 | 5 | 22 | ||
| Workplace † | Clinical setting | 4 | 10 | 20 | 18 | 52 | 0.058 |
| Community service | 0 | 2 | 4 | 2 | 8 | ||
| Industry | 1 | 0 | 4 | 1 | 6 | ||
| Academia/Research | 2 | 1 | 26 | 9 | 38 | ||
| Freelancer | 3 | 0 | 29 | 9 | 41 | ||
| Other | 2 | 3 | 7 | 4 | 16 | ||
| Years in practice as a dietitian † | 0–4 | 8 | 5 | 50 | 7 | 70 | 0.003 |
| 5–9 | 2 | 4 | 17 | 10 | 33 | ||
| 10–19 | 0 | 3 | 15 | 11 | 29 | ||
| 20 or more | 2 | 2 | 6 | 11 | 21 |
| Participants’ Characteristics | Variable Categories | Gut Health in Overall Health | Nutrition as Gut Microbiota Modulator | Probiotics in Health | Prebiotics in Health | Overall Perceived Knowledge |
|---|---|---|---|---|---|---|
| European region † | Central and Eastern (n = 14) | 0/6/7/1 | 0/4/9/1 | 0/5/8/1 | 0/3/10/1 | 0/4/9/1 |
| Northern (n = 17) | 1/6/7/3 | 1/8/5/3 | 2/9/4/2 | 3/8/3/3 | 1/9/4/3 | |
| Southern (n = 99) | 15/46/35/3 | 13/47/35/4 | 18/47/30/4 | 17/49/30/3 | 14/48/33/4 | |
| Western (n = 45) | 8/15/19/3 | 4/19/19/3 | 9/22/12/2 | 10/19/14/2 | 5/19/19/2 | |
| overall p | 0.439 | 0.260 | 0.428 | 0.022 | 0.149 | |
| Age group (years) | 20–24 (n = 33) | 7/16/10/0 | 7/17/9/0 | 6/20/7/0 | 7/20/6/0 | 7/18/8/0 |
| 25–29 (n = 51) | 8/26/14/3 | 6/20/24/1 | 8/21/21/1 | 8/19/23/1 | 6/22/22/1 | |
| 30–34 (n = 27) | 1/11/11/4 | 1/16/5/5 | 1/17/5/4 | 2/15/7/3 | 1/15/6/5 | |
| 35–39 (n = 14) | 2/5/7/0 | 1/6/7/0 | 3/8/3/0 | 2/6/6/0 | 1/7/6/0 | |
| 40–44 (n = 16) | 2/6/6/2 | 2/6/6/2 | 3/8/5/0 | 3/10/2/1 | 2/7/6/1 | |
| 45–49 (n = 16) | 2/5/9/0 | 1/5/9/1 | 4/4/7/1 | 4/5/6/1 | 2/4/9/1 | |
| 50–54 (n = 17) | 2/5/8/2 | 0/8/6/3 | 2/6/6/3 | 3/5/6/3 | 1/7/6/3 | |
| 55–59 (n = 4) | 0/2/2/0 | 0/3/1/0 | 2/2/0/0 | 1/2/1/0 | 0/3/1/0 | |
| 60–65 (n = 1) | 0/0/1/0 | 0/0/1/0 | 0/0/1/0 | 0/0/1/0 | 0/0/1/0 | |
| overall p | 0.768 | 0.235 | 0.054 | 0.215 | 0.147 | |
| Status | Dietitian (n = 155) | 20/63/61/11 | 15/67/61/12 | 21/75/50/9 | 22/69/55/9 | 16/69/59/11 |
| Other professional (n = 9) | 1/5/3/0 | 1/4/4/0 | 3/4/2/0 | 3/5/1/0 | 1/5/3/0 | |
| Pre-graduate dietetic student (n = 15) | 3/8/4/0 | 2/10/3/0 | 5/7/3/0 | 5/8/2/0 | 3/9/3/0 | |
| overall p | 0.852 | 0.712 | 0.290 | 0.135 | 0.546 | |
| Educational level (dietitians) † | Dietitian, BTS (n = 4) | 1/1/2/0 | 1/2/1/0 | 1/2/1/0 | 1/2/1/0 | 1/2/1/0 |
| Dietitian, pre-BSc (n = 5) | 2/3/0/0 | 2/3/0/0 | 2/3/0/0 | 3/1/1/0 | 2/3/0/0 | |
| Dietitian, BSc (n = 58) | 11/26/16/5 | 7/25/21/5 | 9/26/19/4 | 10/25/18/5 | 8/25/20/5 | |
| Dietitian, MSc (n = 65) | 5/26/30/4 | 5/27/29/4 | 8/33/22/2 | 7/30/25/3 | 4/30/28/3 | |
| Dietitian, PhD (n = 23) | 1/7/13/2 | 0/10/10/3 | 1/11/8/3 | 1/11/10/1 | 1/9/10/3 | |
| overall p | <0.001 | 0.487 | 0.586 | 0.304 | 0.327 | |
| Workplace † | Clinical setting (n = 52) | 7/19/20/6 | 5/22/20/5 | 8/26/15/3 | 8/22/17/5 | 5/22/20/5 |
| Community service (n = 8) | 1/5/1/1 | 1/4/2/1 | 3/3/1/1 | 3/4/0/1 | 1/5/1/1 | |
| Industry (n = 6) | 2/2/2/0 | 1/3/2/0 | 1/2/3/0 | 1/3/2/0 | 1/2/3/0 | |
| Academia/ Research (n = 39) | 2/11/23/3 | 1/14/20/4 | 3/16/17/3 | 2/16/20/1 | 1/15/20/3 | |
| Freelancer (n = 42) | 7/21/13/1 | 7/19/14/2 | 6/22/13/1 | 7/21/13/1 | 7/20/14/1 | |
| Other (n = 17) | 2/10/5/0 | 1/9/7/0 | 3/10/3/1 | 4/8/4/1 | 2/10/4/1 | |
| overall p | 0.271 | 0.046 | 0.648 | 0.295 | 0.564 | |
| Years in practice as a dietitian † | 0–4 (n = 71) | 12/35/21/3 | 11/29/29/2 | 11/33/25/2 | 13/28/28/2 | 11/30/28/2 |
| 5–9 (n = 33) | 5/12/12/4 | 3/17/10/3 | 5/17/8/3 | 5/17/8/3 | 3/18/8/4 | |
| 10–19 (n = 30) | 3/8/16/3 | 1/13/12/4 | 4/16/10/0 | 3/16/10/1 | 2/13/13/2 | |
| 20 or more (n = 21) | 0/8/12/1 | 0/8/10/3 | 1/9/7/4 | 1/8/9/3 | 0/8/10/3 | |
| overall p | 0.234 | 0.393 | 0.186 | 0.310 | 0.190 |
| Score of Current Knowledge | ||||
|---|---|---|---|---|
| Participants’ Characteristics | Variable Categories | Median | Q1–Q3 | Overall p |
| European region † | Central and Eastern Europe | 18.00 | 17.25–20.00 | 0.792 |
| Northern Europe | 19.00 | 15.00–21.00 | ||
| Southern Europe | 18.00 | 16.00–20.00 | ||
| Western Europe | 18.00 | 16.00–19.00 | ||
| Age group (yrs) ‡ | 20–24 | 18.00 | 16.00–20.00 | 0.411 |
| 25–29 | 18.00 | 16.00–19.00 | ||
| 30–34 | 18.00 | 15.00–20.00 | ||
| 35–39 | 19.00 | 18.75–20.00 | ||
| 40–44 | 17.50 | 16.00–19.00 | ||
| 45–49 | 17.50 | 15.25–19.00 | ||
| 50–54 | 20.00 | 14.00–21.00 | ||
| 55–59 | 19.00 | 19.00–20.50 | ||
| Status | Dietitian | 18.00 | 16.00–20.00 | 0.173 |
| Other professional | 17.00 | 15.50–19.00 | ||
| Pre-graduate dietetic student | 16.00 | 15.00–19.00 | ||
| Educational level (dietitians) † | Dietitian, BTS | 16.50 | 13.75–18.50 | 0.139 |
| Dietitian, pre-BSc | 15.00 | 12.50–19.00 | ||
| Dietitian, BSc | 18.00 | 15.00–20.00 | ||
| Dietitian, MSc | 19.00 | 17.00–20.00 | ||
| Dietitian, PhD | 19.00 | 16.00–20.00 | ||
| Workplace † | Clinical setting | 18.00 | 16.25–20.00 | 0.035 |
| Community service | 16.50 | 10.50–19.00 | ||
| Industry | 17.00 | 11.75–18.00 | ||
| Academia/Research | 19.00 | 17.00–20.00 | ||
| Freelancer | 18.00 | 15.00–20.00 | ||
| Other | 18.00 | 15.50–19.50 | ||
| Years in practice as a dietitian † | 0–4 | 18.00 | 16.00–20.00 | 0.554 |
| 5–9 | 18.00 | 16.00–20.00 | ||
| 10–19 | 19.00 | 17.00–20.00 | ||
| 20 or more | 19.00 | 14.50–20.00 | ||
| Score of Current Knowledge | ||||
|---|---|---|---|---|
| Participants’ Characteristics | Variable Categories | Median | Q1–Q3 | Overall p |
| European region † | Central and Eastern Europe | 7.00 | 6.00–9.25 | 0.168 |
| Northern Europe | 8.00 | 7.00–9.00 | ||
| Southern Europe | 7.00 | 6.00–8.00 | ||
| Western Europe | 8.00 | 6.00–9.00 | ||
| Age group (yrs) ‡ | 20–24 | 7.00 | 6.00–9.00 | 0.348 |
| 25–29 | 7.00 | 6.00–9.00 | ||
| 30–34 | 8.00 | 7.00–8.00 | ||
| 35–39 | 8.50 | 7.75–9.00 | ||
| 40–44 | 8.00 | 7.00–9.00 | ||
| 45–49 | 8.50 | 6.00–9.75 | ||
| 50–54 | 8.00 | 6.50–9.00 | ||
| 55–59 | 7.50 | 6.25–8.75 | ||
| Status | Dietitian | 8.00 | 6.00–9.00 | 0.006 |
| Other professional | 8.00 | 7.50–9.00 | ||
| Pre-graduate dietetic student | 7.00 | 5.00–7.00 | ||
| Educational level (dietitians) † | Dietitian, BTS | 7.50 | 6.00–9.00 | 0.078 |
| Dietitian, pre-BSc | 6.00 | 4.50–7.00 | ||
| Dietitian, BSc | 8.00 | 6.00–9.00 | ||
| Dietitian, MSc | 8.00 | 6.00–9.00 | ||
| Dietitian, PhD | 8.00 | 8.00–9.00 | ||
| Workplace † | Clinical setting | 8.00 | 7.00–9.00 | 0.034 |
| Community service | 7.00 | 4.50–8.00 | ||
| Industry | 8.00 | 5.25–8.75 | ||
| Academia/Research | 8.00 | 8.00–9.00 | ||
| Freelancer | 7.00 | 6.00–9.00 | ||
| Other | 7.00 | 5.50–9.00 | ||
| Years in practice as a dietitian † | 0–4 | 8.00 | 6.00–9.00 | 0.227 |
| 5–9 | 7.00 | 6.00–9.00 | ||
| 10–19 | 8.00 | 7.00–9.00 | ||
| 20 or more | 8.00 | 6.00–9.50 | ||
| Score of Current Knowledge | ||||
|---|---|---|---|---|
| Participants’ Characteristics | Variable Categories | Median | Q1–Q3 | Overall p |
| European region † | Central and Eastern Europe | 5.00 | 4.75–7.25 | 0.655 |
| Northern Europe | 6.00 | 4.00–7.00 | ||
| Southern Europe | 5.00 | 4.00–6.00 | ||
| Western Europe | 6.00 | 4.00–7.00 | ||
| Age group (yrs) ‡ | 20–24 | 5.00 | 4.00–6.00 | 0.622 |
| 25–29 | 6.00 | 5.00–7.00 | ||
| 30–34 | 6.00 | 4.00–7.00 | ||
| 35–39 | 6.00 | 4.00–7.00 | ||
| 40–44 | 5.00 | 3.25–6.75 | ||
| 45–49 | 5.50 | 4.25–6.75 | ||
| 50–54 | 5.00 | 4.00–7.50 | ||
| 55–59 | 5.00 | 4.25–7.25 | ||
| Status | Dietitian | 6.00 | 4.00–7.00 | 0.137 |
| Other professional | 5.00 | 5.00–7.00 | ||
| Pre-graduate dietetic student | 5.00 | 3.00–6.00 | ||
| Educational level (dietitians) † | Dietitian, BTS | 5.00 | 3.50–8.00 | 0.183 |
| Dietitian, pre-BSc | 5.00 | 3.50–5.50 | ||
| Dietitian, BSc | 5.00 | 4.00–7.00 | ||
| Dietitian, MSc | 5.00 | 4.00–7.00 | ||
| Dietitian, PhD | 6.00 | 5.00–7.00 | ||
| Workplace † | Clinical setting | 5.00 | 4.00–7.00 | 0.061 |
| Community service | 5.50 | 2.75–7.00 | ||
| Industry | 3.50 | 3.00–6.50 | ||
| Academia/Research | 6.00 | 5.00–7.00 | ||
| Freelancer | 5.00 | 5.00–7.00 | ||
| Other | 5.00 | 3.00–6.00 | ||
| Years in practice as a dietitian † | 0–4 | 5.00 | 4.00–7.00 | 0.738 |
| 5–9 | 6.00 | 4.00–7.00 | ||
| 10–19 | 5.00 | 4.00–7.00 | ||
| 20 or more | 6.00 | 5.00–6.50 | ||
| Score of Current Knowledge | ||||
|---|---|---|---|---|
| Participants’ Characteristics | Variable Categories | Median | Q1–Q3 | Overall p |
| European region † | Central and Eastern Europe | 3.50 | 2.00–5.00 | 0.620 |
| Northern Europe | 3.00 | 2.00–4.00 | ||
| Southern Europe | 3.00 | 3.00–4.00 | ||
| Western Europe | 4.00 | 3.00–4.50 | ||
| Age group (yrs) ‡ | 20–24 | 3.00 | 2.00–4.00 | 0.742 |
| 25–29 | 3.00 | 3.00–5.00 | ||
| 30–34 | 3.00 | 2.00–4.00 | ||
| 35–39 | 3.00 | 2.75–4.25 | ||
| 40–44 | 3.00 | 2.25–4.75 | ||
| 45–49 | 4.00 | 2.25–4.00 | ||
| 50–54 | 4.00 | 3.00–5.00 | ||
| 55–59 | 3.00 | 2.25–3.75 | ||
| Status | Dietitian | 4.00 | 3.00–4.00 | 0.108 |
| Other professional | 3.00 | 2.00–4.00 | ||
| Pre-graduate dietetic student | 3.00 | 2.00–4.00 | ||
| Educational level (dietitians) † | Dietitian, BTS | 3.50 | 3.00–4.75 | 0.023 |
| Dietitian, pre-BSc | 3.00 | 1.50–3.00 | ||
| Dietitian, BSc | 3.00 | 2.00–4.00 | ||
| Dietitian, MSc | 4.00 | 3.00–4.00 | ||
| Dietitian, PhD | 4.00 | 3.00–5.00 | ||
| Workplace † | Clinical setting | 4.00 | 3.00–4.00 | 0.007 |
| Community service | 2.50 | 2.00–4.00 | ||
| Industry | 3.00 | 2.75–3.25 | ||
| Academia/Research | 4.00 | 3.00–5.00 | ||
| Freelancer | 3.00 | 2.00–4.00 | ||
| Other | 3.00 | 2.00–4.00 | ||
| Years in practice as a dietitian † | 0–4 | 3.00 | 2.00–4.00 | 0.217 |
| 5–9 | 4.00 | 3.00–4.00 | ||
| 10–19 | 3.00 | 2.75–4.00 | ||
| 20 or more | 4.00 | 3.00–5.00 | ||
| Score of Current Knowledge | ||||
|---|---|---|---|---|
| Participants’ Characteristics | Variable Categories | Median | Q1–Q3 | Overall p |
| European region † | Central and Eastern Europe | 34.00 | 29.75–41.00 | 0.601 |
| Northern Europe | 36.00 | 29.00–40.50 | ||
| Southern Europe | 34.00 | 29.00–38.00 | ||
| Western Europe | 36.00 | 29.00–39.00 | ||
| Age group (yrs) ‡ | 20–24 | 33.00 | 28.00–37.50 | 0.677 |
| 25–29 | 33.00 | 30.00–38.00 | ||
| 30–34 | 35.00 | 29.00–38.00 | ||
| 35–39 | 36.50 | 34.25–39.00 | ||
| 40–44 | 33.00 | 28.00–37.75 | ||
| 45–49 | 35.50 | 29.00–38.75 | ||
| 50–54 | 37.00 | 28.50–41.00 | ||
| 55–59 | 34.50 | 31.50–37.50 | ||
| Status | Dietitian | 35.00 | 30.00–39.00 | 0.030 |
| Other professional | 33.00 | 29.00–37.00 | ||
| Pre-graduate dietetic student | 29.00 | 28.00–34.00 | ||
| Educational level (dietitians) † | Dietitian, BTS | 31.00 | 29.00–39.00 | 0.029 |
| Dietitian, pre-BSc | 27.00 | 23.50–34.00 | ||
| Dietitian, BSc | 35.00 | 28.00–38.00 | ||
| Dietitian, MSc | 36.00 | 31.50–38.50 | ||
| Dietitian, PhD | 38.00 | 33.00–42.00 | ||
| Workplace † | Clinical setting | 35.50 | 30.25–38.00 | 0.004 |
| Community service | 34.00 | 20.25–36.75 | ||
| Industry | 28.00 | 27.00–33.50 | ||
| Academia/Research | 38.00 | 35.00–41.00 | ||
| Freelancer | 33.50 | 29.00–37.25 | ||
| Other | 33.00 | 26.50–39.00 | ||
| Years in practice as a dietitian † | 0–4 | 34.00 | 28.00–38.00 | 0.411 |
| 5–9 | 35.00 | 30.00–39.00 | ||
| 10–19 | 36.00 | 31.75–38.25 | ||
| 20 or more | 38.00 | 30.00–41.00 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitsou, E.K.; Katsagoni, C.N.; Janiszewska, K. Knowledge of Dietitians on Gut Microbiota in Health—An Online Survey of the European Federation of the Associations of Dietitians (EFAD). Nutrients 2024, 16, 621. https://doi.org/10.3390/nu16050621
Mitsou EK, Katsagoni CN, Janiszewska K. Knowledge of Dietitians on Gut Microbiota in Health—An Online Survey of the European Federation of the Associations of Dietitians (EFAD). Nutrients. 2024; 16(5):621. https://doi.org/10.3390/nu16050621
Chicago/Turabian StyleMitsou, Evdokia K., Christina N. Katsagoni, and Katarzyna Janiszewska. 2024. "Knowledge of Dietitians on Gut Microbiota in Health—An Online Survey of the European Federation of the Associations of Dietitians (EFAD)" Nutrients 16, no. 5: 621. https://doi.org/10.3390/nu16050621
APA StyleMitsou, E. K., Katsagoni, C. N., & Janiszewska, K. (2024). Knowledge of Dietitians on Gut Microbiota in Health—An Online Survey of the European Federation of the Associations of Dietitians (EFAD). Nutrients, 16(5), 621. https://doi.org/10.3390/nu16050621