

The Role of Probiotics in the Prevention of Clostridioides difficile Infection in Patients with Chronic Kidney Disease

Abstract
:1. Introduction
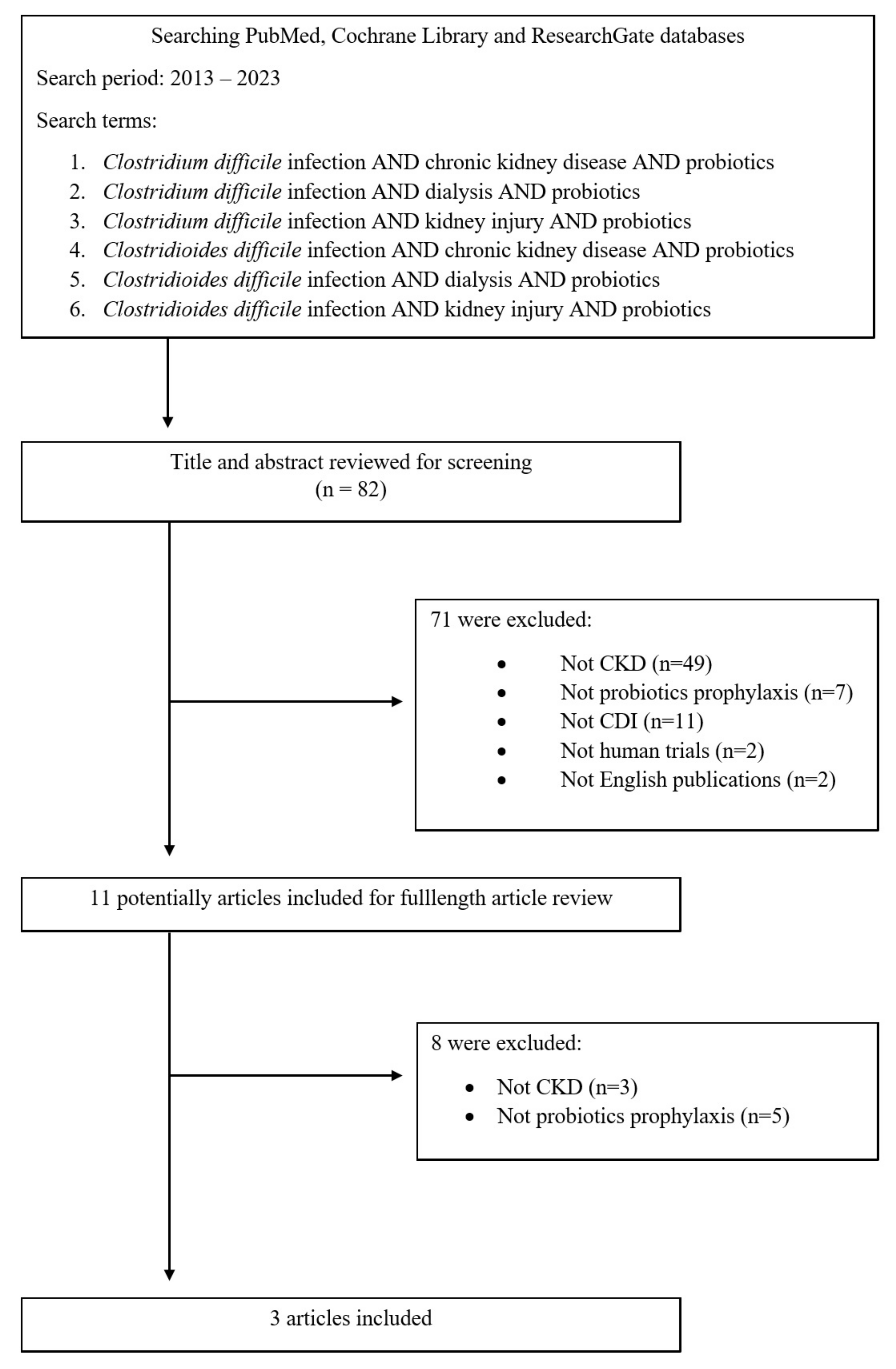
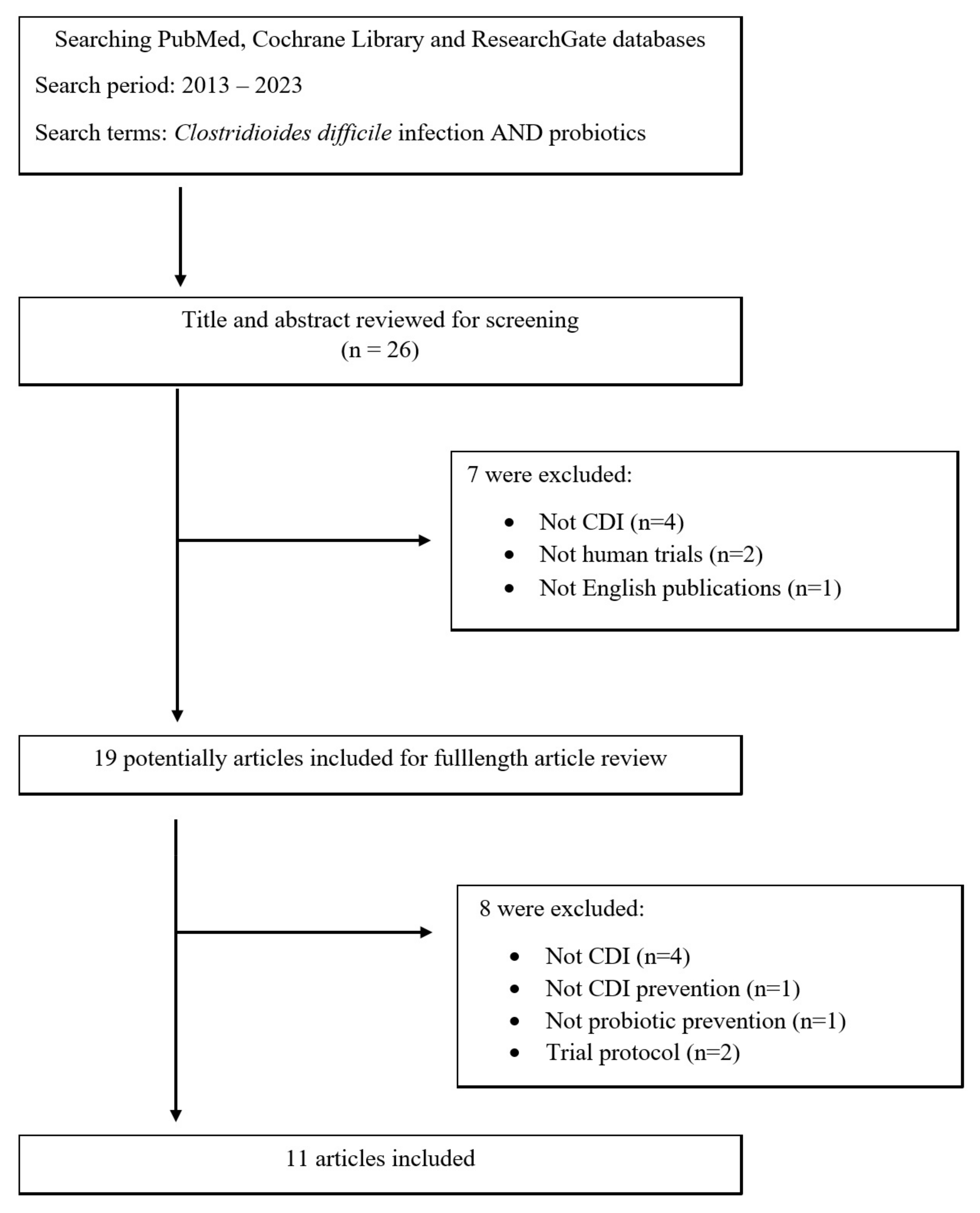
2. Methodology
3. Dysbiosis in Chronic Kidney Disease Patients
4. Clostridioides difficile
4.1. Clostridioides difficile Infection in CKD Patients
4.2. Use of Probiotics in the Prophylaxis of Clostridioides difficile Infections in Chronic Kidney Disease Patients
5. Lactobacillus plantarum 299v
6. Probiotics in the Prevention of Clostridioides difficile Infection in General Population
7. Summary
Author Contributions
Funding
Conflicts of Interest
References
- Czepiel, J.; Dróżdż, M.; Pituch, H.; Kuijper, E.J.; Perucki, W.; Mielimonka, A.; Goldman, S.; Wultańska, D.; Garlicki, A.; Biesiada, G. Clostridium difficile infection: Review. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1211–1221. [Google Scholar] [CrossRef]
- Sundström, J.; Bodegard, J.; Bollmann, A.; Vervloet, M.G.; Mark, P.B.; Karasik, A.; Taveira-Gomes, T.; Botana, M.; Birkeland, K.I.; Thuresson, M.; et al. Prevalence, outcomes, and cost of chronic kidney disease in a contemporary population of 2·4 million patients from 11 countries: The CaReMe CKD study. Lancet Reg. Health Eur. 2022, 20, 100438. [Google Scholar] [CrossRef]
- Keddis, M.T.; Khanna, S.; Noheria, A.; Baddour, L.M.; Pardi, D.S.; Qian, Q. Clostridium difficile infection in patients with chronic kidney disease. Mayo Clin. Proc. 2012, 87, 1046–1053. [Google Scholar] [CrossRef] [PubMed]
- Cooper, C.C.; Jump, R.L.; Chopra, T. Prevention of infection due to Clostridium difficile. Infect. Dis. Clin. N. Am. 2016, 30, 999–1012. [Google Scholar] [CrossRef] [PubMed]
- Plata, C.; Cruz, C.; Cervantes, L.G.; Ramírez, V. The gut microbiota and its relationship with chronic kidney disease. Int. Urol. Nephrol. 2019, 51, 2209–2226. [Google Scholar] [CrossRef] [PubMed]
- Ramezani, A.; Massy, Z.A.; Meijers, B.; Evenepoel, P.; Vanholder, R.; Raj, D.S. Role of the gut microbiome in uremia: A potential therapeutic target. Am. J. Kidney Dis. 2016, 67, 483–498. [Google Scholar] [CrossRef] [PubMed]
- Vaziri, N.D.; Goshtasbi, N.; Yuan, J.; Jellbauer, S.; Moradi, H.; Raffatellu, M.; Kalantar-Zadeh, K. Uremic plasma impairs barrier function and depletes the tight junction protein constituents of intestinal epithelium. Am. J. Nephrol. 2012, 36, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Lau, W.L.; Kalantar-Zadeh, K.; Vaziri, N.D. The gut as a source of inflammation in chronic kidney disease. Nephron 2015, 130, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Vaziri, N.; Wong, J.; Pahl, M.V.; Piceno, Y.M.; Yuan, J.; DeSantis, T.Z.; Ni, Z.; Nguyen, T.-H.; Andersen, G.L. Chronic kidney disease alters intestinal microbial flora. Kidney Int. 2013, 83, 308–315. [Google Scholar] [CrossRef]
- Vaziri, N.D.; Yuan, J.; Rahimi, A.; Ni, Z.; Said, H.; Subramanian, V.S. Disintegration of colonic epithelial tight junction in uremia: A likely cause of CKD-associated inflammation. Nephrol. Dial. Transplant. 2012, 27, 2686–2693. [Google Scholar] [CrossRef]
- Lau, W.L.; Vaziri, N.D. The leaky gut and altered microbiome in chronic kidney disease. J. Ren. Nutr. 2017, 27, 458–461. [Google Scholar] [CrossRef]
- Feng, Z.; Wang, T.; Dong, S.; Jiang, H.; Zhang, J.; Raza, H.K.; Lei, G. Association between gut dysbiosis and chronic kidney disease: A narrative review of the literature. J. Int. Med. Res. 2021, 49, 3000605211053276. [Google Scholar] [CrossRef] [PubMed]
- Magliocca, G.; Mone, P.; Di Iorio, B.R.; Heidland, A.; Marzocco, S. Short-chain fatty acids in chronic kidney disease: Focus on inflammation and oxidative stress regulation. Int. J. Mol. Sci. 2022, 23, 5354. [Google Scholar] [CrossRef] [PubMed]
- Amini Khiabani, S.; Asgharzadeh, M.; Kafil, H.S. Chronic kidney disease and gut microbiota. Heliyon 2023, 9, e18991. [Google Scholar] [CrossRef]
- Tian, N.; Li, L.; Ng, J.K.; Li, P.K. The potential benefits and controversies of probiotics use in patients at different stages of chronic kidney disease. Nutrients 2022, 14, 4044. [Google Scholar] [CrossRef] [PubMed]
- Sanders, M.E. Probiotics in 2015: Their scope and use. J. Clin. Gastroenterol. 2015, 49, S2–S6. [Google Scholar] [CrossRef] [PubMed]
- Hill, C.; Guarner, F.; Reid, G.; Gibson, G.R.; Merenstein, D.J.; Pot, B.; Morelli, L.; Canani, R.B.; Flint, H.J.; Salminen, S.; et al. Expert consensus document. The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 506–514. [Google Scholar] [CrossRef] [PubMed]
- Poutanen, S.M.; Simor, A.E. Clostridium difficile-associated diarrhea in adults. Can. Med. Assoc. J. 2004, 171, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Lawler, A.J.; Lambert, P.A.; Worthington, T. A revised understanding of Clostridioides difficile spore germination. Trends Microbiol. 2020, 28, 744–752. [Google Scholar] [CrossRef]
- Buddle, J.E.; Fagan, R.P. Pathogenicity and virulence of Clostridioides difficile. Virulence 2023, 14, 2150452. [Google Scholar] [CrossRef]
- Lyon, S.A.; Hutton, M.L.; Rood, J.I.; Cheung, J.K.; Lyras, D. CdtR regulates TcdA and TcdB production in Clostridium difficile. PLoS Pathog. 2016, 12, e1005758. [Google Scholar] [CrossRef]
- Smits, W.K.; Lyras, D.; Lacy, D.B.; Wilcox, M.H.; Kuijper, E.J. Clostridium difficile infection. Nat. Rev. Dis. Primers 2016, 2, 16020. [Google Scholar] [CrossRef]
- Freeman, J.; Bauer, M.P.; Baines, S.D.; Corver, J.; Fawley, W.N.; Goorhuis, B.; Kuijper, E.J.; Wilcox, M.H. The changing epidemiology of Clostridium difficile infections. Clin. Microbiol. Rev. 2010, 23, 529–549. [Google Scholar] [CrossRef]
- Bartlett, J.G.; Gerding, D.N. Clinical recognition and diagnosis of Clostridium difficile infection. Clin. Infect. Dis. 2008, 46, 12–18. [Google Scholar] [CrossRef]
- Guery, B.; Galperine, T.; Barbut, F. Clostridioides difficile: Diagnosis and treatments. BMJ 2019, 366, l4609. [Google Scholar] [CrossRef]
- Nagy, E. What do we know about the diagnostics, treatment and epidemiology of Clostridioides (Clostridium) difficile infection in Europe? J. Infect. Chemother. 2018, 24, 164–170. [Google Scholar] [CrossRef]
- Doll, M.; Marra, A.R.; Apisarnthanarak, A.; Al-Maani, A.S.; Abbas, S.; Rosenthal, V.D. Prevention of Clostridioides difficile in hospitals: A position paper of the International Society for Infectious Diseases. Int. J. Infect. Dis. 2021, 102, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Leffler, D.A.; Lamont, J.T. Clostridium difficile infection. N. Engl. J. Med. 2015, 372, 1539–1548. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Yang, H. Non-antibiotic therapy for Clostridioides difficile infection: A review. Crit. Rev. Clin. Lab. Sci. 2019, 56, 493–509. [Google Scholar] [CrossRef] [PubMed]
- van Prehn, J.; Reigadas, E.; Vogelzang, E.H.; Bouza, E.; Hristea, A.; Guery, B.; Krutova, M.; Norén, T.; Allerberger, F.; Coia, J.E.; et al. European Society of Clinical Microbiology and Infectious Diseases: 2021 update on the treatment guidance document for Clostridioides difficile infection in adults. Clin. Microbiol. Infect. 2021, 27, S1–S21. [Google Scholar] [CrossRef] [PubMed]
- Tirath, A.; Tadros, S.; Coffin, S.L.; Kintziger, K.W.; Waller, J.L.; Baer, S.L.; Colombo, R.E.; Huber, L.Y.; Kheda, M.F.; Nahman, N.S., Jr. Clostridium difficile infection in dialysis patients. J. Investig. Med. 2017, 65, 353–357. [Google Scholar] [CrossRef] [PubMed]
- Phatharacharukul, P.; Thongprayoon, C.; Cheungpasitporn, W.; Edmonds, P.J.; Mahaparn, P.; Bruminhent, J. The risks of incident and recurrent Clostridium difficile associated diarrhea in chronic kidney disease and endstage kidney disease patients: A systematic review and meta-analysis. Dig. Dis. Sci. 2015, 60, 2913–2922. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Cheungpasitporn, W.; Phatharacharukul, P.; Edmonds, P.J.; Kaewpoowat, Q.; Mahaparn, P.; Bruminhent, J.; Erickson, S.B. Chronic kidney disease and end-stage renal disease are risk factors for poor outcomes of Clostridium difficile infection: A systematic review and meta-analysis. Int. J. Clin. Pract. 2015, 69, 998–1006. [Google Scholar] [CrossRef] [PubMed]
- Thongprayoon, C.; Cheungpasitporn, W.; Phatharacharukul, P.; Mahaparn, P.; Bruminhent, J. High mortality risk in chronic kidney disease and end stage kidney disease patients with Clostridium difficile infection: A systematic review and meta-analysis. J. Nat. Sci. 2015, 73, 389–400. [Google Scholar]
- Kim, S.C.; Seo, M.Y.; Lee, J.Y.; Kim, K.T.; Cho, E.; Kim, M.G.; Jo, S.K.; Cho, W.Y.; Kim, H.K. Advanced chronic kidney disease: A strong risk factor for Clostridium difficile infection. Korean J. Intern. Med. 2016, 31, 125–133. [Google Scholar] [CrossRef]
- Abdelfatah, M.; Nayfe, R.; Nijim, A.; Enriquez, K.; Ali, E.; Watkins, R.R.; Kandil, H. Factors predicting recurrence of Clostridium difficile infection (CDI) in hospitalized patients: Retrospective study of more than 2000 patients. J. Investig. Med. 2015, 63, 747–751. [Google Scholar] [CrossRef]
- Ramesh, M.S.; Yee, J. Clostridioides difficile infection in chronic kidney disease/end-stage renal disease. Adv. Chronic Kidney Dis. 2019, 26, 30–34. [Google Scholar] [CrossRef]
- Lis, Ł.; Konieczny, A.; Żłobicka, K.; Witkiewicz, W.; Hruby, Z. Clostridioides difficile infection in patients with end stage renal disease. Is it preventable? Przegl Epidemiol. 2020, 74, 11–21. [Google Scholar] [CrossRef]
- Dudzicz, S.; Wiecek, A.; Adamczak, A. Clostridioides difficile infection in chronic kidney disease—An overview for clinicians. J. Clin. Med. 2021, 10, 196. [Google Scholar] [CrossRef]
- Dudzicz, S.; Adamczak, A.; Wiecek, A. Clostridium difficile infection in the nephrology ward. Kidney Blood Press. Res. 2017, 42, 844–852. [Google Scholar] [CrossRef]
- Dudzicz, S.; Kujawa-Szewieczek, A.; Kwiecień, K.; Więcek, A.; Adamczak, M. Lactobacillus plantarum 299v reduces the incidence of Clostridium difficile infection in nephrology and transplantation ward—Results of one year extended study. Nutrients 2018, 10, 1574. [Google Scholar] [CrossRef] [PubMed]
- Ladas, E.J.; Bhatia, M.; Chen, L.; Sandler, E.; Petrovic, A.; Berman, D.M.; Hamblin, F.; Gates, M.; Hawks, R.; Sung, L.; et al. The safety and feasibility of probiotics in children and adolescents undergoing hematopoietic cell transplantation. Bone Marrow Transplant. 2016, 51, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Nanwa, N.; Kendzerska, T.; Krahn, M.; Kwong, J.C.; Daneman, N.; Witteman, W.; Mittmann, N.; Cadarette, S.M.; Rosella, L.; Sander, B. The economic impact of Clostridium difficile infection: A systematic review. Am. J. Gastroenterol. 2015, 110, 511–519. [Google Scholar] [CrossRef]
- Molin, G.; Jeppsson, B.; Johansson, M.L.; Ahrné, S.; Nobaek, S.; Ståhl, M.; Bengmark, S. Numerical taxonomy of Lactobacillus spp. associated with healthy and diseased mucosa of the human intestines. J. Appl. Bacteriol. 1993, 74, 314–323. [Google Scholar] [CrossRef]
- Mack, D.R.; Ahrne, S.; Hyde, L.; Wei, S.; Hollingsworth, M.A. Extracellular MUC3 mucin secretion follows adherence of Lactobacillus strains to intestinal epithelial cells in vitro. Gut 2003, 52, 827–833. [Google Scholar] [CrossRef] [PubMed]
- Nordström, E.A.; Teixeira, C.; Montelius, C.; Jeppsson, B.; Larsson, N. Lactiplantibacillus plantarum 299v (LP299V®): Three decades of research. Benef. Microbes 2021, 12, 441–465. [Google Scholar] [CrossRef] [PubMed]
- Oudhuis, G.J.; Bergmans, D.C.; Dormans, T.; Zwaveling, J.H.; Kessels, A.; Prins, M.H.; Stobberingh, E.E.; Verbon, A. Probiotics versus antibiotic decontamination of the digestive tract: Infection and mortality. Intensive Care Med. 2011, 37, 110–117. [Google Scholar] [CrossRef]
- Olek, A.; Woynarowski, M.; Ahrén, I.L.; Kierkuś, J.; Socha, P.; Larsson, N.; Önning, G. Efficacy and safety of Lactobacillus plantarum DSM 9843 (LP299V) in the prevention of antibiotic-associated gastrointestinal symptoms in children-randomized, double-blind, placebo-controlled study. J. Pediatr. 2017, 186, 82–86. [Google Scholar] [CrossRef]
- McNaught, C.E.; Woodcock, N.P.; MacFie, J.; Mitchell, C.J. A prospective randomised study of the probiotic Lactobacillus plantarum 299V on indices of gut barrier function in elective surgical patients. Gut 2002, 51, 827–831. [Google Scholar] [CrossRef]
- Lönnermark, E.; Friman, V.; Lappas, G.; Sandberg, T.; Berggren, A.; Adlerberth, I. Intake of Lactobacillus plantarum reduces certain gastrointestinal symptoms during treatment with antibiotics. J. Clin. Gastroenterol. 2010, 44, 106–112. [Google Scholar] [CrossRef]
- Ducrotté, P.; Sawant, P.; Jayanthi, V. Clinical trial: Lactobacillus plantarum 299v (DSM 9843) improves symptoms of irritable bowel syndrome. World J. Gastroenterol. 2012, 18, 4012–4018. [Google Scholar] [CrossRef] [PubMed]
- McNaught, C.E.; Woodcock, N.P.; Anderson, A.D.; MacFie, J. A prospective randomised trial of probiotics in critically ill patients. Clin. Nutr. 2005, 24, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Malik, M.; Suboc, T.M.; Tyagi, S.; Salzman, N.; Wang, J.; Ying, R.; Tanner, M.J.; Kakarla, M.; Baker, J.E.; Widlansky, M.E. Lactobacillus plantarum 299v supplementation improves vascular endothelial function and reduces inflammatory biomarkers in men with stable coronary artery disease. Circ. Res. 2018, 123, 1091–1102. [Google Scholar] [CrossRef] [PubMed]
- Rask, C.; Adlerberth, I.; Berggren, A.; Ahrén, I.L.; Wold, A.E. Differential effect on cell-mediated immunity in human volunteers after intake of different lactobacilli. Clin. Exp. Immunol. 2013, 172, 321–332. [Google Scholar] [CrossRef] [PubMed]
- Bering, S.; Suchdev, S.; Sjøltov, L.; Berggren, A.; Tetens, I.; Bukhave, K. A lactic acid-fermented oat gruel increases non-haem iron absorption from a phytate-rich meal in healthy women of childbearing age. Br. J. Nutr. 2006, 96, 80–85. [Google Scholar] [CrossRef]
- Mashyn, S.; Borodanov, S.; Klymenko, O.; Lev, I.; Shipova, K. The role of Lactobacilli in the human microbiome and methods of their cultivation and preservation. Georgian Med. News 2022, 326, 23–35. [Google Scholar]
- Snydman, D.R. The safety of probiotics. Clin. Infect. Dis. 2008, 46 (Suppl. S2), S104–S111. [Google Scholar] [CrossRef]
- FAO/WHO Working Group. Guidelines for the Evaluation of Probiotics in Food; FAO/WHO Working Group: Rome, Italy, 2002; pp. 1–11. [Google Scholar]
- Allen, S.J.; Wareham, K.; Wang, D.; Bradley, C.; Hutchings, H.; Harris, W.; Dhar, A.; Brown, H.; Foden, A.; Gravenor, M.B.; et al. Lactobacilli and Bifidobacteria in the prevention of antibiotic-associated diarrhoea and Clostridium difficile diarrhoea in older inpatients (PLACIDE): A randomised, double-blind, placebo-controlled, multicentre trial. Lancet 2013, 382, 1249–1257. [Google Scholar] [CrossRef]
- Box, M.J.; Ortwine, K.N.; Goicoechea, M.; Scripps Antimicrobial Stewardship Program (SASP). No impact of probiotics to reduce Clostridium difficile infection in hospitalized patients: A real-world experience. Open Forum Infect. Dis. 2018, 5, ofy192. [Google Scholar] [CrossRef]
- Dionne, J.C.; Johnstone, J.; Heels-Ansdell, D.; Duan, E.; Lauzier, F.; Arabi, Y.M.; Adhikari, N.K.J.; Sligl, W.; Dodek, P.; Rochwerg, B.; et al. Clostridioides difficile infection in mechanically ventilated critically ill patients: A nested cohort study. J. Crit. Care 2023, 75, 154254. [Google Scholar] [CrossRef]
- Rauseo, A.M.; Hink, T.; Reske, K.A.; Seiler, S.M.; Bommarito, K.M.; Fraser, V.J.; Burnham, C.D.; Dubberke, E.R. CDC prevention epicenter program. A randomized controlled trial of Lactobacillus rhamnosus GG on antimicrobial-resistant organism colonization. Infect. Control Hosp. Epidemiol. 2022, 43, 167–173. [Google Scholar] [CrossRef]
- Rajkumar, C.; Wilks, M.; Islam, J.; Ali, K.; Raftery, J.; Davies, K.A.; Timeyin, J.; Cheek, E.; Cohen, J. Do probiotics prevent antibiotic-associated diarrhoea? Results of a multicentre randomized placebo-controlled trial. J. Hosp. Infect. 2020, 105, 280–288. [Google Scholar] [CrossRef]
- Alberda, C.; Marcushamer, S.; Hewer, T.; Journault, N.; Kutsogiannis, D. Feasibility of a Lactobacillus casei drink in the intensive care unit for prevention of antibiotic associated diarrhea and Clostridium difficile. Nutrients 2018, 10, 539. [Google Scholar] [CrossRef]
- Kołodziej, M.; Szajewska, H. Lactobacillus reuteri DSM 17938 in the prevention of antibiotic-associated diarrhoea in children: A randomized clinical trial. Clin. Microbiol. Infect. 2019, 25, 699–704. [Google Scholar] [CrossRef]
- Sadahiro, S.; Suzuki, T.; Tanaka, A.; Okada, K.; Kamata, H.; Ozaki, T.; Koga, Y. Comparison between oral antibiotics and probiotics as bowel preparation for elective colon cancer surgery to prevent infection: Prospective randomized trial. Surgery 2014, 155, 493–503. [Google Scholar] [CrossRef] [PubMed]
- McFarland, L.V. Systematic review and meta-analysis of Saccharomyces boulardii in adult patients. World J. Gastroenterol. 2010, 16, 2202–2222. [Google Scholar] [CrossRef] [PubMed]
- Carstensen, J.W.; Chehri, M.; Schønning, K.; Rasmussen, S.C.; Anhøj, J.; Godtfredsen, N.S.; Andersen, C.Ø.; Petersen, A.M. Use of prophylactic Saccharomyces boulardii to prevent Clostridium difficile infection in hospitalized patients: A controlled prospective intervention study. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 1431–1439. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, J.Z.; Yap, C.; Lytvyn, L.; Lo, C.K.; Beardsley, J.; Mertz, D.; Johnston, B.C. Probiotics for the prevention of Clostridium difficile-associated diarrhea in adults and children. Cochrane Database Syst. Rev. 2017, 12, CD006095. [Google Scholar] [CrossRef]
- Shen, N.T.; Maw, A.; Tmanova, L.L.; Pino, A.; Ancy, K.; Crawford, C.V.; Simon, M.S.; Evans, A.T. Timely use of probiotics in hospitalized adults prevents Clostridium difficile infection: A systematic review with meta-regression analysis. Gastroenterology 2017, 152, 1889–1900.e9. [Google Scholar] [CrossRef]
- Johnston, B.C.; Ma, S.S.Y.; Goldenberg, J.Z.; Thorlund, K.; Vandvik, P.O.; Loeb, M.; Guyatt, G.H. Probiotics for the prevention of Clostridium difficile-associated diarrhea: A systematic review and meta-analysis. Ann. Intern. Med. 2012, 157, 878–888. [Google Scholar] [CrossRef] [PubMed]
- US Department of Health and Human Services. Guidance for industry. In Early Clinical Trials with Live Biotherapeutic Products: Chemistry, Manufacturing, and Control Information; US Department of Health and Human Services: Washington, DC, USA, 2016. [Google Scholar]
- Khanna, S.; Assi, M.; Lee, C.; Yoho, D.; Louie, T.; Knapple, W.; Aguilar, H.; Garcia-Diaz, J.; Wang, G.P.; Berry, S.M.; et al. Efficacy and safety of RBX2660 in PUNCH CD3, a phase III, randomized, double-blind, placebo-controlled trial with a bayesian primary analysis for the prevention of recurrent Clostridioides difficile infection. Drugs 2022, 82, 1527–1538. [Google Scholar] [CrossRef] [PubMed]
- Louie, T.; Golan, Y.; Khanna, S.; Bobilev, D.; Erpelding, N.; Fratazzi, C.; Carini, M.; Menon, R.; Ruisi, M.; Norman, J.M.; et al. VE303, a defined bacterial consortium, for prevention of recurrent Clostridioides difficile infection: A randomized clinical trial. JAMA 2023, 329, 1356–1366. [Google Scholar] [CrossRef] [PubMed]
- McDonald, L.C.; Gerding, D.N.; Johnson, S.; Bakken, J.S.; Carroll, K.C.; Coffin, S.E.; Dubberke, E.R.; Garey, K.W.; Gould, C.V.; Kelly, C.; et al. Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin. Infect. Dis. 2018, 66, e1–e48. [Google Scholar] [CrossRef] [PubMed]
- Kelly, C.R.; Fischer, M.; Allegretti, J.R.; LaPlante, K.; Stewart, D.B.; Limketkai, B.N.; Stollman, N.H. ACG clinical guidelines: Prevention, diagnosis, and treatment of Clostridioides difficile infections. Am. J. Gastroenterol. 2021, 116, 1124–1147. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| (n) | (% All Hospitalized Patients) | vs. Incidence during Prophylaxis of LP299v | |
|---|---|---|---|
| Before introduction of LP299v | 18 | 1.03% | p = 0.0003 |
| During prophylaxis of LP299v | 2 | 0.11% | - |
| After cessation of LP299v | 14 | 0.77% | p = 0.0028 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dudzicz-Gojowy, S.; Więcek, A.; Adamczak, M. The Role of Probiotics in the Prevention of Clostridioides difficile Infection in Patients with Chronic Kidney Disease. Nutrients 2024, 16, 671. https://doi.org/10.3390/nu16050671
Dudzicz-Gojowy S, Więcek A, Adamczak M. The Role of Probiotics in the Prevention of Clostridioides difficile Infection in Patients with Chronic Kidney Disease. Nutrients. 2024; 16(5):671. https://doi.org/10.3390/nu16050671
Chicago/Turabian StyleDudzicz-Gojowy, Sylwia, Andrzej Więcek, and Marcin Adamczak. 2024. "The Role of Probiotics in the Prevention of Clostridioides difficile Infection in Patients with Chronic Kidney Disease" Nutrients 16, no. 5: 671. https://doi.org/10.3390/nu16050671
APA StyleDudzicz-Gojowy, S., Więcek, A., & Adamczak, M. (2024). The Role of Probiotics in the Prevention of Clostridioides difficile Infection in Patients with Chronic Kidney Disease. Nutrients, 16(5), 671. https://doi.org/10.3390/nu16050671