

Vitamin D Supplementation for Patients with Dysmenorrhoea: A Meta-Analysis with Trial Sequential Analysis of Randomised Controlled Trials


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol
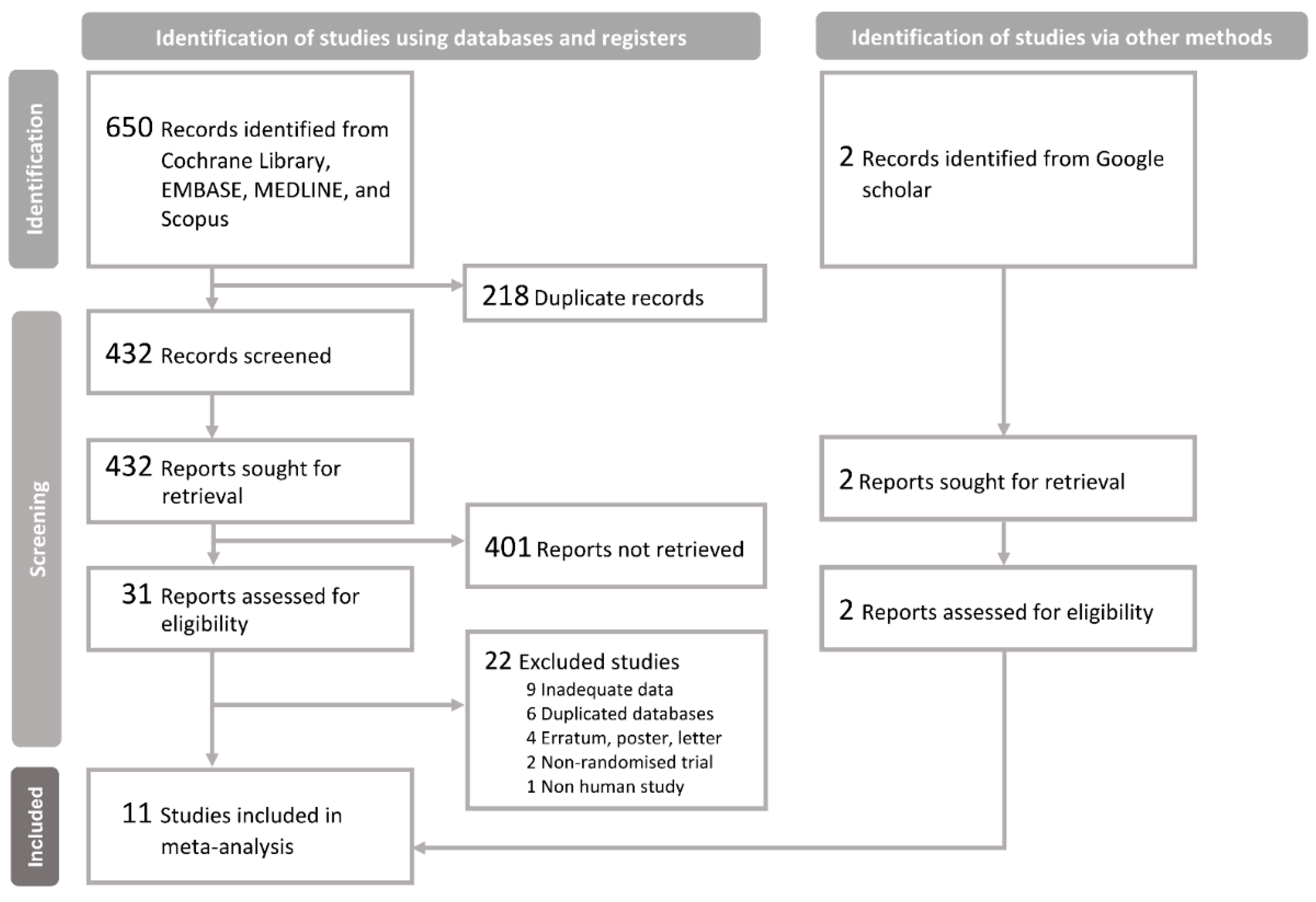
2.2. Search Strategy
2.3. Outcome Measures
2.4. Data Extraction and Assessment of Methodological Quality
2.5. Data Collection, Processing, and Analysis
2.6. Trial Sequential Analysis
2.7. Grading of the Certainty of Evidence (CoE)
3. Results
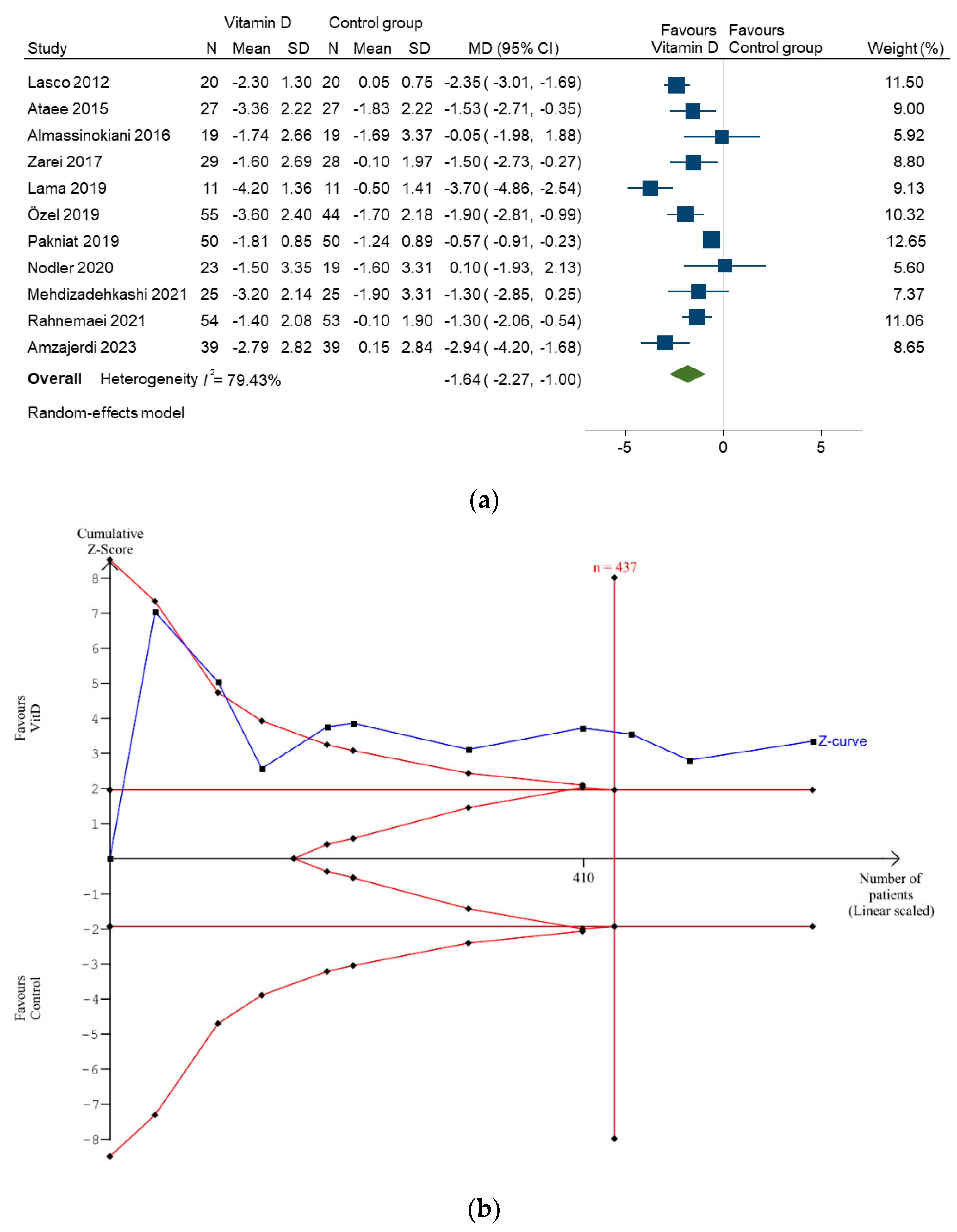
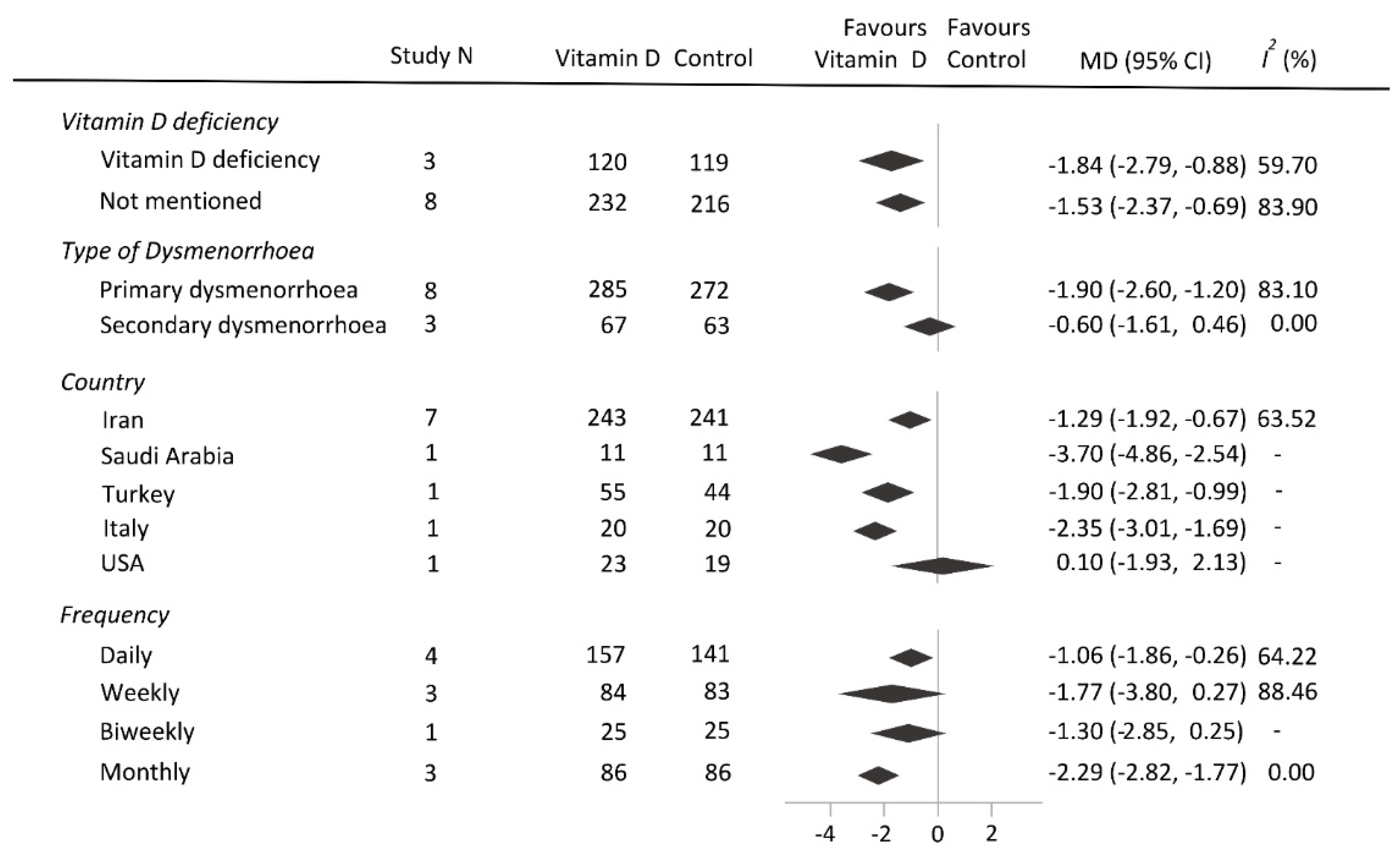
3.1. Primary and Secondary Outcomes
3.2. GRADE Assessment
4. Discussion
4.1. Main Findings
4.2. Interpretation
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Proctor, M.; Farquhar, C. Diagnosis and management of dysmenorrhoea. BMJ 2006, 332, 1134–1138. [Google Scholar] [CrossRef]
- ACOG Committee. ACOG Committee Opinion No. 760: Dysmenorrhea and endometriosis in the adolescent. Obstet. Gynecol. 2018, 132, e249–e258. [Google Scholar] [CrossRef]
- MacGregor, B.; Allaire, C.; Bedaiwy, M.A.; Yong, P.J.; Bougie, O. Disease burden of dysmenorrhea: Impact on life course potential. Int. J. Womens Health 2023, 15, 499–509. [Google Scholar] [CrossRef]
- Akiyama, S.; Tanaka, E.; Cristeau, O.; Onishi, Y.; Osuga, Y. Evaluation of the treatment patterns and economic burden of dysmenorrhea in Japanese women, using a claims database. Clinicoecon. Outcomes Res. 2017, 9, 295–306. [Google Scholar] [CrossRef]
- Chen, I.; Thavorn, K.; Shen, M.; Goddard, Y.; Yong, P.; MacRae, G.S.; Nishi, C.; Matar, A.; Allaire, C. Hospital-associated costs of chronic pelvic pain in Canada: A population-based descriptive study. J. Obstet. Gynaecol. Can. 2017, 39, 174–180. [Google Scholar] [CrossRef] [PubMed]
- French, L. Dysmenorrhea. Am. Fam. Phys. 2005, 71, 285–291. [Google Scholar]
- Harirforoosh, S.; Asghar, W.; Jamali, F. Adverse effects of nonsteroidal antiinflammatory drugs: An update of gastrointestinal, cardiovascular and renal complications. J. Pharm. Pharm. Sci. 2013, 16, 821–847. [Google Scholar] [CrossRef]
- Curtis, K.M.; Tepper, N.K.; Jatlaoui, T.C.; Berry-Bibee, E.; Horton, L.G.; Zapata, L.B.; Simmons, K.B.; Pagano, H.P.; Jamieson, D.J.; Whiteman, M.K.U.S. U.S. Medical eligibility criteria for contraceptive use, 2016. MMWR Recomm. Rep. 2016, 65, 1–103. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.J.; Li, Y.X.; Wu, C.J.; Chang, W.C.; Wei, L.H.; Sheu, B.C. Effects of dienogest on breasts of women of reproductive age and women in menopausal transition: A cohort study. Int. J. Gynaecol. Obstet. 2023, 162, 1114–1116. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Malihi, Z.; Stewart, A.W.; Lawes, C.M.; Scragg, R. Effect of vitamin D supplementation on pain: A systematic review and meta-analysis. Pain Phys. 2016, 19, 415–427. [Google Scholar]
- Zadro, J.R.; Shirley, D.; Ferreira, M.; Carvalho Silva, A.P.; Lamb, S.E.; Cooper, C.; Ferreira, P.H. Is vitamin D supplementation effective for low back pain? A systematic review and meta-analysis. Pain Physician 2018, 21, 121–145. [Google Scholar] [CrossRef] [PubMed]
- Helde-Frankling, M.; Björkhem-Bergman, L. Vitamin D in pain management. Int. J. Mol. Sci. 2017, 18, 2170. [Google Scholar] [CrossRef] [PubMed]
- Habib, A.M.; Nagi, K.; Thillaiappan, N.B.; Sukumaran, V.; Akhtar, S. Vitamin D and its potential interplay with pain signaling pathways. Front. Immunol. 2020, 11, 820. [Google Scholar] [CrossRef] [PubMed]
- Abdi, F.; Amjadi, M.A.; Zaheri, F.; Rahnemaei, F.A. Role of vitamin D and calcium in the relief of primary dysmenorrhea: A systematic review. Obstet. Gynecol. Sci. 2021, 64, 13–26. [Google Scholar] [CrossRef]
- Lasco, A.; Catalano, A.; Benvenga, S. Improvement of primary dysmenorrhea caused by a single oral dose of vitamin D: Results of a randomized, double-blind, placebo-controlled study. Arch. Intern. Med. 2012, 172, 366–367. [Google Scholar] [CrossRef] [PubMed]
- Mina Ataee, M.Z.; Mahboubi, M. Cholecalciferol for Primary Dysmenorrhea in a College- aged Population—A Clinical Trial. J. Biol. Today’s World 2015, 4, 54–57. [Google Scholar] [CrossRef]
- Zarei, S.; Mohammad-Alizadeh-Charandabi, S.; Mirghafourvand, M.; Javadzadeh, Y.; Effati-Daryani, F. Effects of calcium-vitamin D and calcium-alone on pain intensity and menstrual blood loss in women with primary dysmenorrhea: A randomized controlled trial. Pain Med. 2017, 18, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Alshaigi Lama, A.N.; Azzah, A.K.; Areej, A.; Alaa, E.; Salem, A. Vitamin D supplements as adjunctive therapy with analgesics for primary dysmenorrhea: A randomized clinical trial. Int. J. Reprod. Med. Gynecol. 2019, 4, 11–14. [Google Scholar]
- Özel, A.; Ateş, S.; Şevket, O.; Özdemİr, M.; İlhan, G.; Davutoğlu, E. A Randomized Controlled Study of Vitamin D in the Treatment of Primary Dysmenorrhea. Düzce Tıp Fak. Derg. 2019, 21, 32–36. [Google Scholar] [CrossRef]
- Pakniat, H.; Chegini, V.; Ranjkesh, F.; Hosseini, M.A. Comparison of the effect of vitamin E, vitamin D and ginger on the severity of primary dysmenorrhea: A single-blind clinical trial. Obstet. Gynecol. Sci. 2019, 62, 462–468. [Google Scholar] [CrossRef]
- Rahnemaei, F.A.; Gholamrezaei, A.; Afrakhteh, M.; Zayeri, F.; Vafa, M.R.; Rashidi, A.; Ozgoli, G. Vitamin D supplementation for primary dysmenorrhea: A double-blind, randomized, placebo-controlled trial. Obstet. Gynecol. Sci. 2021, 64, 353–363. [Google Scholar] [CrossRef]
- Amzajerdi, A.; Keshavarz, M.; Ghorbali, E.; Pezaro, S.; Sarvi, F. The effect of vitamin D on the severity of dysmenorrhea and menstrual blood loss: A randomized clinical trial. BMC Womens Health 2023, 23, 138. [Google Scholar] [CrossRef] [PubMed]
- Almassinokiani, F.; Khodaverdi, S.; Solaymani-Dodaran, M.; Akbari, P.; Pazouki, A. Effects of vitamin D on endometriosis-related pain: A double-blind clinical trial. Med. Sci. Monit. 2016, 22, 4960–4966. [Google Scholar] [CrossRef] [PubMed]
- Nodler, J.L.; DiVasta, A.D.; Vitonis, A.F.; Karevicius, S.; Malsch, M.; Sarda, V.; Fadayomi, A.; Harris, H.R.; Missmer, S.A. Supplementation with vitamin D or ω-3 fatty acids in adolescent girls and young women with endometriosis (SAGE): A double-blind, randomized, placebo-controlled trial. Am. J. Clin. Nutr. 2020, 112, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Mehdizadehkashi, A.; Rokhgireh, S.; Tahermanesh, K.; Eslahi, N.; Minaeian, S.; Samimi, M. The effect of vitamin D supplementation on clinical symptoms and metabolic profiles in patients with endometriosis. Gynecol. Endocrinol. 2021, 37, 640–645. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Chiang, Y.F.; Lin, Y.J.; Huang, K.C.; Chen, H.Y.; Hamdy, N.M.; Huang, T.C.; Chang, H.Y.; Shieh, T.M.; Huang, Y.J.; et al. Effect of vitamin D supplementation on primary dysmenorrhea: A systematic review and meta-analysis of randomized clinical trials. Nutrients 2023, 15, 2830. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Li, T.; Deeks, J.J. Choosing effect measures and computing estimates of effect. In Cochrane Handbook for Systematic Reviews of Interventions; Wiley Online Library: Hoboken, NJ, USA, 2019; pp. 143–176. [Google Scholar]
- Lesaffre, E.; Philstrom, B.; Needleman, I.; Worthington, H. The design and analysis of split-mouth studies: What statisticians and clinicians should know. Stat. Med. 2009, 28, 3470–3482. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ. 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Ferries-Rowe, E.; Corey, E.; Archer, J.S. Primary dysmenorrhea: Diagnosis and therapy. Obstet. Gynecol. 2020, 136, 1047–1058. [Google Scholar] [CrossRef] [PubMed]
- Morrow, C.; Naumburg, E.H. Dysmenorrhea. Prim. Care 2009, 36, 19–32. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M.; Endocrine Society. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef]
- Imberger, G.; Thorlund, K.; Gluud, C.; Wetterslev, J. False-positive findings in Cochrane meta-analyses with and without application of trial sequential analysis: An empirical review. BMJ Open 2016, 6, e011890. [Google Scholar] [CrossRef]
- Djulbegovic, B.; Guyatt, G.H. Progress in evidence-based medicine: A quarter century on. Lancet 2017, 390, 415–423. [Google Scholar] [CrossRef]
- Zangene, M.; Veisi, F.; Nankali, A.; Rezaei, M.; Ataee, M. Evaluation of the effects of oral vitamin-D for pelvic pain reduction in primary dysmenorrhea. Iran. J. Obstet. Gynecol. Infertil. 2014, 16, 14–20. [Google Scholar]
- Moini, A.; Ebrahimi, T.; Shirzad, N.; Hosseini, R.; Radfar, M.; Bandarian, F.; Jafari-Adli, S.; Qorbani, M.; Hemmatabadi, M. The effect of vitamin D on primary dysmenorrhea with vitamin D deficiency: A randomized double-blind controlled clinical trial. Gynecol. Endocrinol. 2016, 32, 502–505. [Google Scholar] [CrossRef]
- Kalaitzopoulos, D.R.; Samartzis, N.; Daniilidis, A.; Leeners, B.; Makieva, S.; Nirgianakis, K.; Dedes, I.; Metzler, J.M.; Imesch, P.; Lempesis, I.G. Effects of vitamin D supplementation in endometriosis: A systematic review. Reprod. Biol. Endocrinol. 2022, 20, 176. [Google Scholar] [CrossRef]
- Wu, Z.; Malihi, Z.; Stewart, A.W.; Lawes, C.M.; Scragg, R. The association between vitamin D concentration and pain: A systematic review and meta-analysis. Public Health Nutr. 2018, 21, 2022–2037. [Google Scholar] [CrossRef] [PubMed]
- Bashmakova, N.V.; Lisovskaya, T.V.; Vlasova, V.Y. Pathogenetic role of vitamin D deficiency in the development of menstrual dysfunction in pubertal girls: A literature review. Gynecol. Endocrinol. 2017, 33 (Supp. S1), 52–55. [Google Scholar] [CrossRef] [PubMed]
- Thota, C.; Laknaur, A.; Farmer, T.; Ladson, G.; Al-Hendy, A.; Ismail, N. Vitamin D regulates contractile profile in human uterine myometrial cells via NF-κB pathway. Am. J. Obstet. Gynecol. 2014, 210, 347.e1–347.e10. [Google Scholar] [CrossRef] [PubMed]
- Matsas, A.; Sachinidis, A.; Lamprinou, M.; Stamoula, E.; Christopoulos, P. Vitamin effects in primary dysmenorrhea. Life 2023, 13, 1308. [Google Scholar] [CrossRef]
- Kahlon, B.K.; Simon-Collins, M.; Nylander, E.; Segars, J.; Singh, B. A systematic review of vitamin D and endometriosis: Role in pathophysiology, diagnosis, treatment, and prevention. FS Rev. 2023, 4, 1–14. [Google Scholar] [CrossRef]
- Vatandost, S.; Jahani, M.; Afshari, A.; Amiri, M.R.; Heidarimoghadam, R.; Mohammadi, Y. Prevalence of vitamin D deficiency in Iran: A systematic review and meta-analysis. Nutr. Health 2018, 24, 269–278. [Google Scholar] [CrossRef]
- Asif, A.; Farooq, N. Vitamin D toxicity. In StatPearls; Pearls Publishing Copyright © 2024; StatPearls Publishing LLC: Treasure Island, FL, USA, 2024. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Study | Blinding | Country | Sample Size | Age Range (Years) | Type of Dysmenorrhea | Vit. D Deficiency | Baseline Serum 25(OH)D Level (ng/mL) † | Vit. D Frequency | Vit. D (IU) per Dose | Vit. D (IU) per Cycle | Follow-Up Duration | Outcome Measurement |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lasco et al., 2012 [15] | Double-blinded | Italy | 40 | 18–40 | Primary | NA ± | Vit. D: 30.0 ± 7.6 Control: 27.3 ± 7.5 | Once per month | 300,000 | 300,000 | 2 months | VAS |
| Ataee et al., 2015 [16] | Double-blinded | Iran | 54 | 18–30 | Primary | Included # | Vit. D: 7.3 ± 3.6 Control: 6.3 ± 2.8 | Once per month | 300,000 | 300,000 | 3 months | VAS |
| Almassinokiani et al., 2016 [23] | Double-blinded | Iran | 38 | 15–40 | Secondary | NA | NA | Once per week | 50,000 | 200,000 | 16 weeks | VAS |
| Zarei et al., 2017 [17] | Double-blinded | Iran | 57 | 18–32 | Primary | NA | NA | Once per day § | 5000 | 65,000 | 3 months | VAS |
| Lama et al., 2019 [18] | Non-blinded | Saudi Arabia | 22 | 13–40 | Primary | NA ± | Vit. D: 30.1 ± 13.4, Control: 33.9 ± 11.9 | Once per week | 50,000 | 200,000 | 8 weeks | VAS |
| Özel et al., 2019 [19] | Non-blinded | Turkey | 99 | 16–35 | Primary | NA | NA | Once per day for 5 days | 667 | 3335 | 2 months | VAS |
| Pakniat et al., 2019 [20] | Single-blinded | Iran | 100 | 18–25 | Primary | NA | NA | Twice per day for 5 days | 12,500 * | 125,000 | 2 months | VAS |
| Nodler et al., 2020 [24] | Double-blinded | USA | 42 | 12–25 | Secondary | NA | Vit. D: 33.8 ± 11.9 Control: 31.2 ± 12.0 | Once per day | 2000 | 56,000 | 6 months | VAS |
| Mehdizadehkashi et al., 2021 [25] | Double-blinded | Iran | 50 | 18–40 | Secondary | NA | Vit. D: 24.7 ± 7.6 Control: 25.4 ± 10.0 | Biweekly | 50,000 | 100,000 | 12 weeks | NA |
| Rahnemaei et al., 2021 [21] | Double-blinded | Iran | 107 | 18–32 | Primary | Included | Vit. D: 20.0 ± 6.0 Control: 19.5 ± 5.5 | Once per week | 50,000 | 200,000 | 8 weeks | NRS |
| Amzajerdi et al., 2023 [22] | Double-blinded | Iran | 78 | 18–25 | Primary | Included | Vit. D: 5.1 ± 3.3 Control: 6.6 ± 5.6 | Once per month | 300,000 | 300,000 | 2 months | VAS |
| No. of Trials (No. of Patients) | Risk of Bias | Inconsistency | Indirectness | Imprecision | Publication Bias | Effect (95% CI) | Overall Quality of Evidence |
|---|---|---|---|---|---|---|---|
| Pain intensity reduction | |||||||
| 11 (687) | No concerns | Downgraded I2 = 79.43% | Not downgraded | Not downgraded | Not downgraded Begg’s test = 0.28 | MD = −1.64 (−2.27 to −1.00) | ⊕⊕⊕⊖ MODERATE |
| Rescue use of analgesics | |||||||
| 2 (139) | Downgraded | Not downgraded I2 = 45.28 % | Not downgraded | Downgraded | NA | RR = 0.26 (0.05–1.33) | ⊕⊖⊖⊖ VERY LOW |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, K.-C.; Huang, K.-J.; Lin, M.-N.; Wang, C.-Y.; Tsai, T.-Y. Vitamin D Supplementation for Patients with Dysmenorrhoea: A Meta-Analysis with Trial Sequential Analysis of Randomised Controlled Trials. Nutrients 2024, 16, 1089. https://doi.org/10.3390/nu16071089
Lin K-C, Huang K-J, Lin M-N, Wang C-Y, Tsai T-Y. Vitamin D Supplementation for Patients with Dysmenorrhoea: A Meta-Analysis with Trial Sequential Analysis of Randomised Controlled Trials. Nutrients. 2024; 16(7):1089. https://doi.org/10.3390/nu16071089
Chicago/Turabian StyleLin, Kan-Chu, Kuan-Ju Huang, Ming-Nan Lin, Cheng-Yu Wang, and Tou-Yuan Tsai. 2024. "Vitamin D Supplementation for Patients with Dysmenorrhoea: A Meta-Analysis with Trial Sequential Analysis of Randomised Controlled Trials" Nutrients 16, no. 7: 1089. https://doi.org/10.3390/nu16071089
APA StyleLin, K. -C., Huang, K. -J., Lin, M. -N., Wang, C. -Y., & Tsai, T. -Y. (2024). Vitamin D Supplementation for Patients with Dysmenorrhoea: A Meta-Analysis with Trial Sequential Analysis of Randomised Controlled Trials. Nutrients, 16(7), 1089. https://doi.org/10.3390/nu16071089