

Effects of Withania somnifera Extract in Chronically Stressed Adults: A Randomized Controlled Trial

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Participants
2.3. Study Products
2.4. Study Outcomes and Data Collection
2.5. Biochemical Parameter Analysis
2.6. Statistical Analysis
3. Results
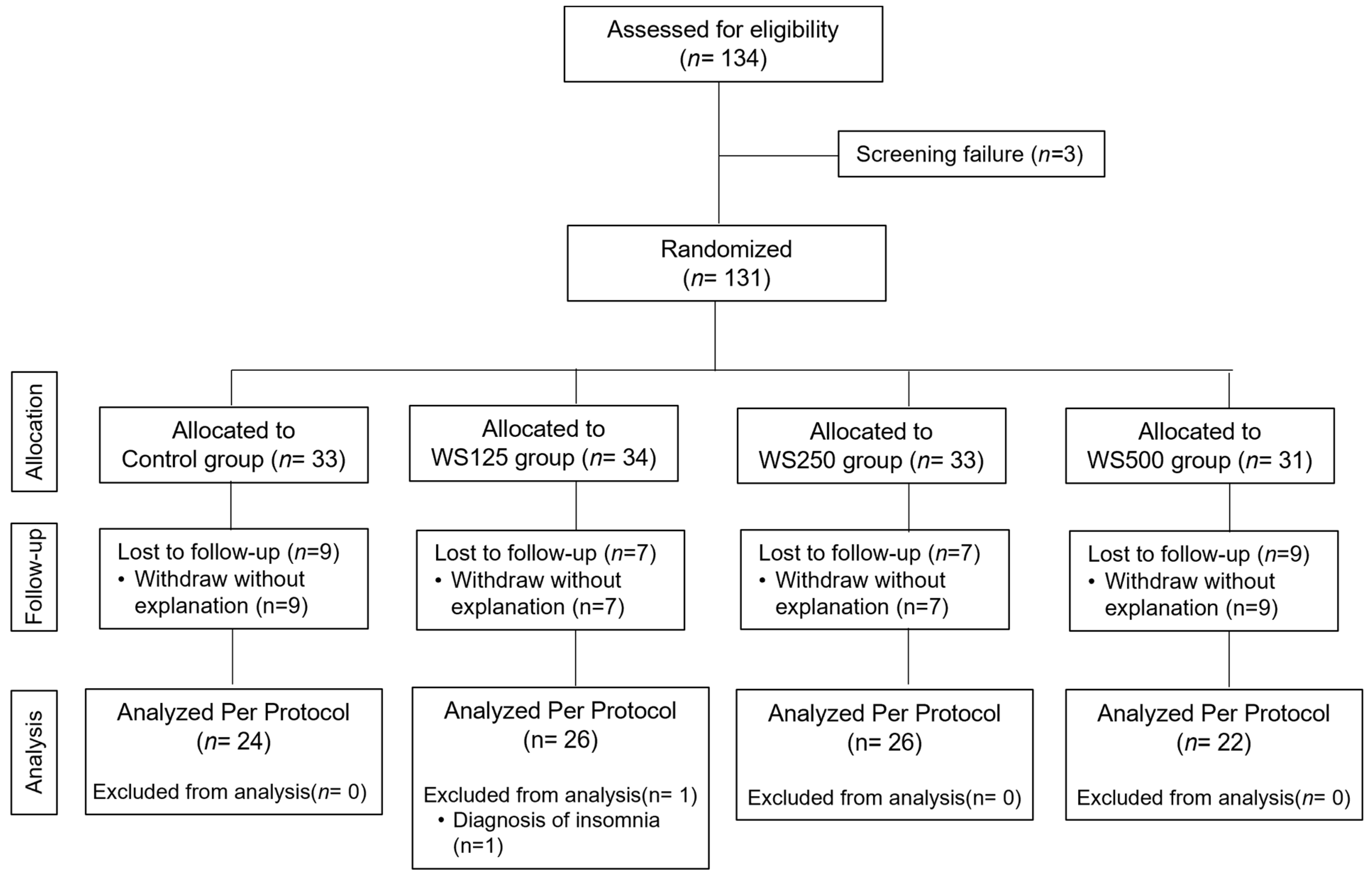
3.1. Study Data, Compliance, and Baseline Characteristics of the Subjects
3.2. Stress, Anxiety, and Depression Outcomes
3.3. Sleep, Vitality, and Quality of Life Parameters
3.4. Safety Parameters and Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO Scientific Brief: Mental Health and COVID-19: Early Evidence of the Pandemic’s Impact. WHO Reference Number: WHO/2019-nCoV/Sci_Brief/Mental_health/2022.1. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Sci_Brief-Mental_health-2022.1 (accessed on 23 April 2024).
- Spinedi, E.; Giacomini, M.; Jacquier, M.C.; Gaillard, R.C. Changes in the hypothalamo corticotroph axis bilateral adrenalectomy: Evidence for a median eminence site of glucocorticoids action. Neuroendocrinology 1991, 53, 60–170. [Google Scholar] [CrossRef] [PubMed]
- Dedovic, K.; Duchesne, A.; Andrews, J.; Engert, V.; Pruessner, J.C. The brain and the stress axis: The neural correlates of cortisol regulation in response to stress. Neuroimage 2009, 47, 864–871. [Google Scholar] [CrossRef] [PubMed]
- Lupien, S.J.; McEwen, B.S.; Gunnar, M.R.; Heim, C. Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nat. Rev. Neurosci. 2009, 10, 434–445. [Google Scholar] [CrossRef] [PubMed]
- Dhabhar, F.S.; McEwen, B.S. Acute stress enhances while chronic stress suppresses cell-mediated immunity in vivo: A potential role for leukocyte trafficking. Brain Behav. Immun. 1997, 11, 286–306. [Google Scholar] [CrossRef] [PubMed]
- Rozanski, A.; Blumenthal, J.A.; Davidson, K.W.; Saab, P.G.; Kubzansky, L. The epidemiology, pathophysiology, and management of psychosocial risk factors in cardiac practice: The emerging field of behavioral cardiology. J. Am. Coll. Cardiol. 2005, 45, 637–651. [Google Scholar] [CrossRef] [PubMed]
- Shastry, J.L.N. Ayurvedokta Oushadha Niruktamala, 1st ed.; Chaukhambka Orient: Varanasi, India, 2001; p. 36. [Google Scholar]
- Kaur, R.; Sharma, R. Ayurvedic concept of liver disorders and its management. World J. Pharm. Res. 2015, 4, 346–370. [Google Scholar]
- Braun, L.; Cohen, M. Herbs and Natural Supplements, Volume 1: An Evidence-Based Guide; Elsevier Health Sciences: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Shenoy, S.; Chaskar, U.; Sandhu, J.S.; Paadhi, M.M. Effects of eight-week Supplementation of Ashwagandha on cardio-respiratory endurance in elite Indian cyclists. J. Ayurveda Integr. Med. 2012, 3, 209–214. [Google Scholar] [CrossRef]
- Abascal, K.; Yarnell, E. Increasing vitality with adaptogens: Multifaceted herbs for treating physical and mental stress. Altrn. Complement Ther. 2003, 9, 54–60. [Google Scholar] [CrossRef]
- Bagchi, D.; Nair, S.; Sen, C.K. Nutrition and Enhanced Sports Performance. Muscle Building, Endurance and Strength; Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Auddy, B.; Hazra, J.; Mitra, A.; Abedon, B.G.; Ghosal, S.; Nagar, B. A Standardized Withania somnifera Extract Significantly Reduces Stress-Related Parameters in Chronically Stressed Humans: A Double-Blind, Randomized, Placebo-Controlled Study. Jana 2008, 11, 50–56. [Google Scholar]
- Chandrasekhar, K.; Kapoor, J.; Anishetty, S. A prospective, randomized double- blind, placebo-controlled study of safety and efficacy of a high- concentration full-spectrum extract of ashwagandha root in reducing stress and anxiety in adults. Indian J. Psychol. Med. 2012, 34, 255–262. [Google Scholar] [CrossRef]
- Ambiye, V.R.; Langade, D.; Dongre, S.; Aptikar, P.; Kulkarni, M.; Dongre, A. Clinical evaluation of the spermatogenic activity of the root extract of ashwagandha (Withania somnifera) in oligospermic males: A pilot study. Evid. -Based Complement. Altern. Med. 2013, 2013, 571420. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Yan, Y.; Wu, Y.; Yang, H.; Zhu, P.; Yan, F.; Zhao, R.; Tian, P.; Wang, T.; Fan, Q. Medicinal herbs for the treatment of anxiety: A systematic review and network meta-analysis. Pharmacol. Res. 2022, 179, 106204. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Speers, A.B.; Cabey, K.A.; Soumyanath, A.; Wright, K.M. Effects of Withania somnifera (Ashwagandha) on Stress and the Stress- Related Neuropsychiatric Disorders Anxiety, Depression, and Insomnia. Curr. Neuropharmacol. 2021, 19, 1468–1495. [Google Scholar] [CrossRef] [PubMed]
- Yılmaz Koğar, E.; Koğar, H. A systematic review and meta-analytic confirmatory factor analysis of the perceived stress scale (PSS-10 and PSS-14). Stress Health 2023, 40, e3285. [Google Scholar] [CrossRef] [PubMed]
- Pangtey, R.; Basu, S.; Meena, G.S.; Banerjee, B. Perceived Stress and its Epidemiological and Behavioral Correlates in an Urban Area of Delhi, India: A Community-Based Cross-Sectional Study. Indian J. Psychol. Med. 2020, 42, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M.A.X. The assessment of anxiety states by rating. Br. J. Med. Psychol. 1959, 32, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M.A.X. Development of a rating scale for primary depressive illness. Br. J. Soc. Clin. Psychol. 1967, 6, 278–296. [Google Scholar] [CrossRef]
- Nater, U.M.; Skoluda, N.; Strahler, J. Biomarkers of stress in behavioural medicine. Curr. Opin. Psychiatry 2013, 26, 440–445. [Google Scholar] [CrossRef]
- Smith, S.M.; Vale, W.W. The role of the hypothalamic-pituitary-adrenal axis in neuroendocrine responses to stress. Dialogues Clin. Neurosci. 2006, 8, 383–395. [Google Scholar] [CrossRef]
- van Stegeren, A.; Rohleder, N.; Everaerd, W.; Wolf, O.T. Salivary alpha amylase as marker for adrenergic activity during stress: Effect of betablockade. Psychoneuroendocrinology 2006, 31, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.Z.; Wang, Y.X.; Jiang, C.L. Inflammation: The Common Pathway of Stress-Related Diseases. Front. Hum. Neurosci. 2017, 11, 316. [Google Scholar] [CrossRef] [PubMed]
- Senthil, K.; Thirugnanasambantham, P.; Oh, T.J.; Kim, S.H.; Choi, H.K. Free radical scavenging activity and comparative metabolic profiling of in vitro cultured and field grown Withania somnifera roots. PLoS ONE 2015, 10, e0123360. [Google Scholar] [CrossRef] [PubMed]
- Martire, V.L.; Caruso, D.; Palagini, L.; Zoccoli, G.; Bastianini, S. Stress & sleep: A relationship lasting a lifetime. Neurosci. Biobehav. Rev. 2020, 117, 65–77. [Google Scholar]
- Gopukumar, K.; Thanawala, S.; Somepalli, V.; Rao, T.S.S.; Thamatam, V.B.; Chauhan, S. Efficacy and Safety of Ashwagandha Root Extract on Cognitive Functions in Healthy, Stressed Adults: A Randomized, Double-Blind, Placebo-Controlled Study. Evid. Based Complement. Altern. Med. 2021, 2021, 8254344. [Google Scholar] [CrossRef]
- Van Reeth, O.; Weibel, L.; Spiegel, K.; Leproult, R.; Dugovic, C.; Maccari, S. PHYSIOLOGY OF SLEEP (REVIEW)–Interactions between stress and sleep: From basic research to clinical situations. Sleep Med. Rev. 2000, 4, 201–219. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Placebo (n = 24) | WS125 mg (n = 26) | WS250 mg (n = 26) | WS500 mg (n = 22) | p between Groups | |
|---|---|---|---|---|---|
| Age (years) | 35.58 ± 9.80 | 35.62 ± 9.25 | 35.38 ± 9.13 | 34.55 ± 11.07 | 0.9807 |
| Sex | |||||
| Females (n, %) | 7(29.17%) | 11(42.31%) | 6(23.08%) | 4(18.18%) | 0.2662 |
| Males (n, %) | 17(70.83%) | 15(57.69%) | 20(76.92%) | 18(81.82%) | |
| BMI (kg/m2) | 24.26 ± 3.43 | 23.81 ± 3.91 | 23.21 ± 3.76 | 23.63 ± 3.51 | 0.7911 |
| Weight(kg) | 63.80 ± 8.41 | 60.10 ± 10.56 | 60.14 ± 12.35 | 62.66 ± 9.02 | 0.4949 |
| Height(cm) | 162.55 ± 10.86 | 158.91 ± 9.12 | 160.70 ± 10.35 | 163.09 ± 7.96 | 0.4240 |
| Smoking (yes) | 3(12.50%) | 2(7.69%) | 2(7.69%) | 2(9.09%) | 0.9286 |
| Placebo (n = 24) | WS125 mg (n = 26) | WS250 mg (n = 26) | WS500 mg (n = 22) | p between Groups | |
|---|---|---|---|---|---|
| Perceived Stress Scale (PSS) | |||||
| Baseline | 37.96 ± 4.99 | 39.15 ± 4.42 | 39.92 ± 4.85 | 39.36 ± 4.25 | 0.507 |
| 2 weeks | 36.00 ± 5.21 | 36.54 ± 4.76 | 35.54 ± 4.31 | 35.36 ± 4.96 | 0.828 |
| 4 weeks | 32.92 ± 5.04 a | 33.65 ± 3.30 a | 30.38 ± 4.23 ab | 29.91 ± 5.14 ab | 0.007 |
| 8 weeks | 31.50 ± 5.76 a | 30.04 ± 4.06 a | 26.27 ± 3.98 b | 23.73 ± 4.67 b | <0.001 |
| Hamilton’s Anxiety Scale (HAM-A) | |||||
| Baseline | 16.90 ± 1.33 | 16.67 ± 1.64 | 16.48 ± 1.69 | 16.48 ± 1.64 | 0.770 |
| 2 weeks | 15.73 ± 1.57 | 15.44 ± 2.00 | 14.21 ± 2.01 | 14.36 ± 2.82 | 0.028 |
| 4 weeks | 15.38 ± 1.97 a | 12.50 ± 2.45 b | 12.19 ± 2.50 b | 12.07 ± 2.39 b | <0.001 |
| 8 weeks | 15.15 ± 2.10 a | 11.08 ± 2.53 b | 8.98 ± 2.91 c | 9.50 ± 2.89 c | <0.001 |
| Hamilton’s Depression Scale (HAM-D) | |||||
| Baseline | 14.83 ± 2.33 | 14.54 ± 2.85 | 13.19 ± 2.25 | 14.43 ± 3.22 | 0.139 |
| 2 weeks | 13.17 ± 2.08 a | 12.23 ± 3.01 ab | 10.69 ± 2.24 b | 11.82 ± 3.08 ab | 0.013 |
| 4 weeks | 13.15 ± 2.41 a | 10.77 ± 3.24 b | 7.81 ± 1.98 c | 8.70 ± 3.92 bc | <0.001 |
| 8 weeks | 13.04 ± 2.42 a | 8.58 ± 2.52 b | 5.83 ± 2.12 c | 6.27 ± 2.27 c | <0.001 |
| Placebo (n = 24) | WS125 mg (n = 26) | WS250 mg (n = 26) | WS500 mg (n = 22) | p between Groups | |
|---|---|---|---|---|---|
| Salivary α-amylase (ng/mL) | |||||
| Baseline | 66.52 ± 7.68 | 64.05 ± 9.53 | 66.49 ± 8.58 | 68.07 ± 10.78 | 0.498 |
| 8 weeks | 71.22 ± 11.44 a | 53.79 ± 7.62 b | 47.27 ± 6.78 c | 42.14 ± 7.47 c | <0.001 |
| Plasma cortisol (μg/dL) | |||||
| Baseline | 11.16 ± 3.84 | 10.23 ± 4.20 | 11.78 ± 4.74 | 11.08 ± 4.24 | 0.632 |
| 8 weeks | 12.34 ± 4.73 a | 8.61 ± 3.32 b | 9.65 ± 3.77 ab | 7.90 ± 2.51 b | <0.001 |
| Plasma DHEA-S (μg/dL) | |||||
| Baseline | 181.78 ± 81.22 | 180.61 ± 92.76 | 211.96 ± 139.12 | 227.44 ± 123.58 | 0.389 |
| 8 weeks | 176.13 ± 85.45 | 170.72 ± 87.15 | 198.16 ± 134.65 | 199.22 ± 106.28 | 0.696 |
| DHEAS-to-Cortisol ratio | |||||
| Baseline | 19.01 ± 14.14 | 19.90 ± 12.02 | 19.06 ± 12.44 | 22.21 ± 12.72 | 0.816 |
| 8 weeks | 16.50 ± 11.13 | 21.46 ± 10.90 | 23.09 ± 17.93 | 25.38 ± 12.85 | 0.153 |
| Plasma ACTH (pg/mL) | |||||
| Baseline | 14.77 ± 7.68 | 17.88 ± 9.66 | 14.52 ± 8.11 | 19.17 ± 10.69 | 0.210 |
| 8 weeks | 16.52 ± 9.05 a | 7.37 ± 1.76 b | 7.77 ± 1.24 b | 8.55 ± 5.81 b | <0.001 |
| Plasma hs-CRP (mg/L) | |||||
| Baseline | 0.83 ± 0.37 | 0.82 ± 0.39 | 0.82 ± 0.27 | 0.97 ± 0.56 | 0.504 |
| 8 weeks | 1.34 ± 2.12 | 0.76 ± 0.36 | 0.67 ± 0.20 | 0.75 ± 0.36 | 0.124 |
| Plasma IL−1β (pg/mL) | |||||
| Baseline | 21.78 ± 13.09 | 25.06 ±10.21 | 26.23 ±15.58 | 25.94 ± 14.02 | 0.639 |
| 8 weeks | 19.68 ± 11.67 a | 17.00 ± 7.27 ab | 13.47 ± 6.06 b | 11.59 ± 5.34 b | 0.004 |
| Plasma IL−6 (pg/mL) | |||||
| Baseline | 276.46 ± 135.26 | 261.77 ± 136.33 | 258.52 ± 117.47 | 266.23 ± 114.06 | 0.963 |
| 8 weeks | 249.75 ± 118.29 a | 187.56 ± 88.29 ab | 177.96 ± 78.21 b | 154.36 ± 69.58 b | 0.004 |
| Plasma TNF-α (pg/mL) | |||||
| Baseline | 1070.8 ± 415.5 | 1086.9 ± 234.0 | 1199.4 ± 645.9 | 1130.0 ± 419.4 | 0.749 |
| 8 weeks | 1067.29 ± 348.6 a | 886.5 ± 259.9 ab | 792.0 ± 365.4 b | 788.2 ± 390.1 b | 0.018 |
| Placebo (n = 24) | WS125 mg (n = 26) | WS250 mg (n = 26) | WS500 mg (n = 22) | p between Groups | |
|---|---|---|---|---|---|
| Pittsburgh Sleep Quality Index (PSQI). | |||||
| Baseline | 16.17 ± 5.37 | 15.31 ± 7.04 | 14.08 ± 5.49 | 18.41 ± 7.39 | 0.128 |
| 2 weeks | 12.58 ± 4.95 | 11.81 ± 5.62 | 10.31 ± 4.54 | 12.64 ± 6.76 | 0.408 |
| 4 weeks | 11.04 ± 4.69 | 10.58 ± 5.89 | 7.31 ± 4.70 | 9.23 ± 5.49 | 0.055 |
| 8 weeks | 10.96 ± 4.41 a | 7.58 ± 2.97 b | 5.00 ± 2.65 c | 7.45 ± 3.86 bc | <0.001 |
| Visual Analogue Sleep Scale (VAS-S). | |||||
| Baseline | 4.88 ± 1.40 | 5.08 ± 1.60 | 5.56 ± 1.56 | 4.52 ± 1.64 | 0.140 |
| 2 weeks | 5.25 ± 1.29 | 5.77 ± 1.73 | 6.35 ± 1.23 | 5.84 ± 1.51 | 0.075 |
| 4 weeks | 4.67 ± 1.09 a | 6.08 ± 1.72 b | 7.13 ± 1.49 b | 6.50 ± 1.74 b | <0.001 |
| 8 weeks | 4.63 ± 1.13 a | 7.27 ± 1.40 b | 8.31 ± 1.23 c | 7.50 ± 1.60 bc | <0.001 |
| Visual Analogue Energy, Vitality and Drive Scale (VAS-E). | |||||
| Baseline | 4.27 ± 1.80 | 4.81 ± 1.96 | 4.63 ± 1.71 | 4.82 ± 1.26 | 0.661 |
| 2 weeks | 4.69 ± 1.41 a | 5.58 ± 1.65 ab | 5.83 ± 1.33 b | 5.82 ± 1.56 ab | 0.029 |
| 4 weeks | 4.67 ± 1.17 a | 5.73 ± 1.69 ab | 6.88 ± 1.68 c | 6.77 ± 1.58 bc | <0.001 |
| 8 weeks | 4.73 ± 1.19 a | 6.67 ± 1.43 b | 7.87 ± 1.62 c | 7.89 ± 1.53 c | <0.001 |
| Title | Week | Placebo (n = 24) | WS125 mg (n = 27) | WS250 mg (n = 26) | WS500 mg (n = 22) |
|---|---|---|---|---|---|
| Glucose (mg/dL) | 0 | 87.04 ± 6.69 | 88.46 ± 6.27 | 92.69 ± 13.64 | 95.66 ± 30.71 |
| 8 | 87.68 ± 6.35 | 88.12 ± 7.21 | 90.65 ± 10.23 | 95.73 ± 23.79 | |
| Total Cholesterol (mg/dL) | 0 | 179.92 ± 47.85 | 175.19 ± 30.74 | 176.96 ± 37.87 | 180.91 ± 36.02 |
| 8 | 174.88 ± 42.53 | 168.11 ± 39.51 | 170.96 ± 35.12 | 178.95 ± 34.66 | |
| HDL Cholesterol (mg/dL) | 0 | 41.83 ± 8.98 | 44.07 ± 8.49 | 47.19 ± 11.77 | 43.00 ± 11.69 |
| 8 | 43.75 ± 11.47 | 43.07 ± 10.02 | 44.12 ± 8.00 | 41.09 ± 6.10 | |
| LDL Cholesterol (mg/dL) | 0 | 114.67 ± 39.61 | 108.85 ± 24.98 | 105.96 ± 28.35 | 113.64 ± 29.49 |
| 8 | 106.50 ± 29.58 | 103.59 ± 32.24 | 103.69 ± 28.48 | 112.91 ± 30.43 | |
| VLDL Cholesterol (mg/dL) | 0 | 23.42 ± 8.68 | 22.26 ± 8.10 | 23.81 ± 9.65 | 24.27 ± 8.01 |
| 8 | 24.63 ± 9.50 | 21.44 ± 7.42 | 23.15 ± 9.43 | 24.95 ± 8.28 | |
| Triglycerides (mg/dL) | 0 | 131.21 ± 79.21 | 123.44 ± 67.65 | 128.46 ± 72.53 | 129.41 ± 52.89 |
| 8 | 122.96 ± 48.71 | 118.85 ± 81.48 | 134.38 ± 85.83 | 139.18 ± 68.72 | |
| Cholesterol/HD | 0 | 4.35 ± 0.97 | 4.05 ± 0.70 | 3.90 ± 1.06 | 4.36 ± 0.90 |
| 8 | 4.10 ± 0.85 | 3.97 ± 0.86 | 3.91 ± 0.83 | 4.40 ± 0.82 | |
| LDL/HDL | 0 | 2.78 ± 0.88 | 2.53 ± 0.64 | 2.36 ± 0.83 | 2.77 ± 0.80 |
| 8 | 2.50 ± 0.68 | 2.45 ± 0.74 | 2.40 ± 0.68 | 2.78 ± 0.73 | |
| T3 (ng/mL) | 0 | 1.12 ± 0.22 | 1.17 ± 0.21 | 1.18 ± 0.17 | 1.19 ± 0.19 |
| 8 | 1.17 ± 0.19 | 1.21 ± 0.22 | 1.15 ± 0.21 | 1.24 ± 0.22 | |
| T4 (μg/dL) | 0 | 7.67 ± 1.92 | 8.00 ± 1.87 | 8.18 ± 1.31 | 8.36 ± 1.41 |
| 8 | 7.74 ± 1.49 | 8.61 ± 1.44 | 8.21 ± 1.54 | 8.37 ± 1.47 | |
| TSH (μIU/mL) | 0 | 2.85 ± 1.34 | 3.21 ± 2.38 | 3.34 ± 2.96 | 2.76 ± 2.27 |
| 8 | 2.89 ± 1.95 | 3.20 ± 3.66 | 3.04 ± 2.19 | 3.07 ± 2.86 | |
| Total Protein (g/dL) | 0 | 7.48 ± 0.43 | 7.30 ± 0.36 | 7.40 ± 0.43 | 7.52 ± 0.36 |
| 8 | 7.50 ± 0.45 | 7.27 ± 0.41 | 7.42 ± 0.40 | 7.55 ± 0.42 | |
| Albumin (g/dL) | 0 | 4.28 ± 0.28 | 4.32 ± 0.36 | 4.44 ± 0.29 | 4.36 ± 0.27 |
| 8 | 4.25 ± 0.31 | 4.29 ± 0.27 | 4.38 ± 0.27 | 4.43 ± 0.25 | |
| Globulin (g/dL) | 0 | 3.20 ± 0.33 | 2.98 ± 0.33 | 2.96 ± 0.36 | 3.15 ± 0.40 |
| 8 | 3.23 ± 0.34 | 2.99 ± 0.29 | 3.03 ± 0.29 | 3.12 ± 0.46 | |
| Albumin/Globulin | 0 | 1.35 ± 0.16 | 1.48 ± 0.26 | 1.52 ± 0.22 | 1.41 ± 0.23 |
| 8 | 1.34 ± 0.15 | 1.45 ± 0.16 | 1.46 ± 0.16 * | 1.46 ± 0.28 | |
| SGOT (U/L) | 0 | 29.91 ± 12.65 | 25.50 ± 5.82 | 30.31 ± 10.44 | 37.74 ± 28.81 |
| 8 | 29.37 ± 10.12 | 27.57 ± 14.13 | 30.60 ± 17.19 | 30.87 ± 15.83 | |
| SGPT (U/L) | 0 | 34.51 ± 23.93 | 25.20 ± 9.85 | 33.10 ± 21.95 | 42.31 ± 33.19 |
| 8 | 33.33 ± 19.16 | 28.63 ± 16.53 | 38.60 ± 45.18 | 32.63 ± 17.18 | |
| ALP (u/L) | 0 | 85.99 ± 17.64 | 73.60 ± 15.43 | 74.07 ± 17.47 | 83.85 ± 18.22 |
| 8 | 90.22 ± 43.46 | 72.11 ± 16.08 | 73.70 ± 15.28 | 84.98 ± 23.55 | |
| Total_Bilirubin(mg/dL) | 0 | 0.77 ± 0.34 | 0.87 ± 0.49 | 0.84 ± 0.39 | 0.80 ± 0.29 |
| 8 | 0.79 ± 0.35 | 0.82 ± 0.36 | 0.78 ± 0.25 | 0.74 ± 0.23 | |
| Conjugated Bilirubin (mg/dL) | 0 | 0.21 ± 0.04 | 0.22 ± 0.05 | 0.21 ± 0.03 | 0.20 ± 0.04 |
| 8 | 0.22 ± 0.04 | 0.22 ± 0.05 | 0.21 ± 0.03 | 0.20 ± 0.02 | |
| Unconjugated Bilirubin (mg/dL) | 0 | 0.56 ± 0.30 | 0.65 ± 0.45 | 0.63 ± 0.36 | 0.60 ± 0.26 |
| 8 | 0.58 ± 0.32 | 0.60 ± 0.31 | 0.57 ± 0.24 | 0.53 ± 0.22 | |
| Urea (mg/dL) | 0 | 20.52 ± 4.15 | 21.34 ± 4.50 | 20.71 ± 4.09 | 20.46 ± 3.32 |
| 8 | 20.54 ± 3.03 | 21.07 ± 4.78 | 21.85 ± 4.83 | 20.29 ± 3.58 | |
| Creatinine (mg/dL) | 0 | 0.92 ± 0.18 | 0.90 ± 0.16 | 0.90 ± 0.14 | 0.93 ± 0.13 |
| 8 | 0.89 ± 0.14 | 0.91 ± 0.14 | 0.91 ± 0.16 | 0.93 ± 0.10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pandit, S.; Srivastav, A.K.; Sur, T.K.; Chaudhuri, S.; Wang, Y.; Biswas, T.K. Effects of Withania somnifera Extract in Chronically Stressed Adults: A Randomized Controlled Trial. Nutrients 2024, 16, 1293. https://doi.org/10.3390/nu16091293
Pandit S, Srivastav AK, Sur TK, Chaudhuri S, Wang Y, Biswas TK. Effects of Withania somnifera Extract in Chronically Stressed Adults: A Randomized Controlled Trial. Nutrients. 2024; 16(9):1293. https://doi.org/10.3390/nu16091293
Chicago/Turabian StylePandit, Srikanta, Amit K. Srivastav, Tapas K. Sur, Supriyo Chaudhuri, Yan Wang, and Tuhin K. Biswas. 2024. "Effects of Withania somnifera Extract in Chronically Stressed Adults: A Randomized Controlled Trial" Nutrients 16, no. 9: 1293. https://doi.org/10.3390/nu16091293
APA StylePandit, S., Srivastav, A. K., Sur, T. K., Chaudhuri, S., Wang, Y., & Biswas, T. K. (2024). Effects of Withania somnifera Extract in Chronically Stressed Adults: A Randomized Controlled Trial. Nutrients, 16(9), 1293. https://doi.org/10.3390/nu16091293