The Role of Functional Foods, Nutraceuticals, and Food Supplements in Intestinal Health

{kind=link}
Abstract
:1. Introduction
2. Food and Health
3. Functional Foods
4. Probiotics, Prebiotics and Synbiotics
Mechanisms of probiotic actions
Imbalance of Intestinal Microbial Flora
5. Nutraceuticals
6. Food Supplements
7. The Intestinal Health
8. The Gastrointestinal (GI) Tract as an Ecosystem
9. Application of Intestinal Cell Models

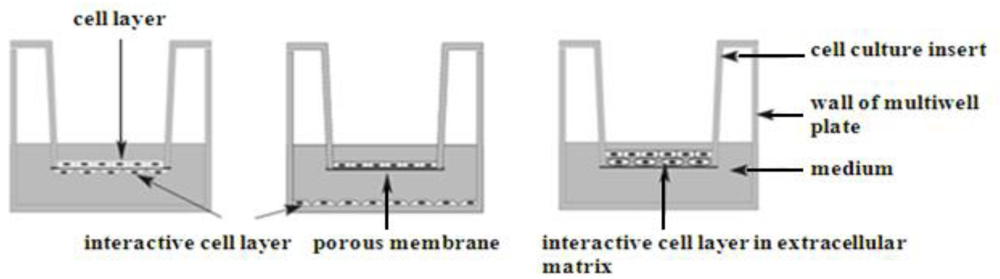
Co-culture systems and studies of interactions between probiotic bacteria and intestinal epithelium
10. Conclusion
References
- Bronzwaer, S. EFSA scientific forum “from safe food to healthy diets”. EU risk assessment -Past, present and Future. Trends Food Sci. Technol. 2008, 19, S2–S8. [Google Scholar]
- Roberts, S.B.; Rosenberg, I. Nutrition and aging: changes in the regulation of energy metabolism with aging. Physiol. Rev. 2006, 86, 651–667. [Google Scholar]
- Perez-Cueto, F.J.; Verbeke, W.; de Barcellos, M.D.; Kehagia, O.; Chryssochoidis, G.; Scholderer, J.; Grunert, K.G. Food-related lifestyles and their association to obesity in five European countries. Appetite 2009, 54, 156–562. [Google Scholar]
- The Analysis of Prehistoric Diets; Gilbert, R.L.; Mielke, J.H. (Eds.) Academic Press: Orlando, FL, USA, 1985.
- Eaton, S.B.; Eaton, S.B., III; Konner, M.J.; Shostak, M. An evolutionary perspective enhances understanding of human nutritional requirements. J. Nutr. 1996, 126, 1732–1740. [Google Scholar] [PubMed]
- Eaton, S.B.; Eaton, S.B., III; Konner, M.J. Paleolithic nutrition revisited: a twelve-year retrospective on its nature and implications. Eur. J. Clin. Nutr. 1997, 51, 207–216. [Google Scholar] [PubMed]
- Roskam, A.J.; Kunst, A.E.; Van Oyen, H.; Demarest, S.; Klumbiene, J.; Regidor, E.; Helmert, U.; Jusot, F.; Dzurova, D.; Mackenbach, J.P. Comparative appraisal of educational inequalities in overweight and obesity among adults in 19 European countries. Int. J. Epidemiol. 2009. [Epub ahead of print]. [Google Scholar]
- Crawford, M.A.; Marsh, D. Nutrition and Evolution; Keats Publishing: New Canaan, CT, USA, 1995. [Google Scholar]
- EFSA (European Food Safety Authority). Scientific Opinion of the Panel on Dietetic Products, Nutrition and Allergies on a request from the EC on Food-Based Dietary Guidelines. The EFSA J. 2008, 1–44.
- Boylan, S.; Welch, A.; Pikhart, H.; Malyutina, S.; Pajak, A.; Kubinova, R.; Bragina, O.; Simonova, G.; Stepaniak, U.; Gilis-Januszewska, A.; Milla, L.; Peasey, A.; Marmot, M.; Bobak, M. Dietary habits in three Central and Eastern European countries: the HAPIEE study. BMC Public Health. 2009, 9, 439. [Google Scholar]
- Acheson, D. Independent Inquiry into Inequalities in Health, Foodaware Proposals for an EU Nutrition Policy, Comments on the Joint WHO/FAO Expert Consultation on Diet, Nutrition and the Prevention of Chronic Diseases. 2002. Available online: http://www.who.int/dietphysicalactivity/media/en/gsfao_cmo_035.pdf (accessed on 25 February 2010).
- NHS, Exploration of Adult Food Portion Size Tools. NHS Health Scotland: Edinburgh, Scotland, 2008.
- Brunso, K.; Fjord, T.A.; Grunert, K.G. Consumers' food choice and quality perception; Aarhus School of Business: Aarhus, Denmark, 2002; MAPP Working Paper No. 77. [Google Scholar]
- Grunert, K.G.; Brunso, K.; Bredahl, L.; Bech, A.C. Food-Related Lifestyle: A Segmentation Approach to European Food Consumers. In Food, People and Society: A European Perspective of Consumers’ Food Choices; Frewer, L.J., Risvik, E., Schifferstein, H.N.J., von Alvensleben, R., Eds.; Springer Verlag: Berlin, Germany, 2001; pp. 211–230. [Google Scholar]
- Public Health Boon or 21st Century Quackery? International, Functional Foods, Center for Science in the Public. CSPI Reports. 1998. Available online: http://www.cspinet.org/reports/functional_foods/introduction.html/ (accessed on 25 February 2010).
- Caetano, M.C.; Ortiz, T.T.; da Silva, S.G.; de Souza, F.I.; Sarni, R.O. Complementary feeding: inappropriate practices in infants. J. Pediatr. (Rio J). 2010, 86. [Epub ahead of print]. [Google Scholar]
- Cencic, A.; Chingwaru, W. Antimicrobial Agents Deriving from Indigenous Plants. RPFNA 2010, 2, 83–92. [Google Scholar]
- Balsano, C.; Alisi, A. Antioxidant effects of natural bioactive compounds. Curr. Pharm. Des. 2009, 15, 3063–3073. [Google Scholar]
- Liu, R.H. Potential synergy of phytochemicals in cancer prevention: mechanism of action. J. Nutr. 2004, 134, 3479S–3485S. [Google Scholar]
- Terry, P.; Giovannucci, E.; Michels, K.B.; Bergkvist, L.; Hansen, H.; Holmberg, L.; Wolk, A. Fruit, vegetables, dietary fiber, and risk of colorectal cancer. J. Natl. Cancer. Inst. 2001, 93, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Denny, A.; Buttriss, J. Synthesis Report No 4: Plant Foods and Health: Focus on Plant Bioactives. British Nutrition Foundation, 2005. Available online: http://www.eurofir.net/temp/PLANTspFOODSspANDspHEALTHspFOCUSspONspPLANTspBIOACTIVEShs1hs.pdf (accessed on 11 October 2009).
- Stramba-Badiale, M.; Fox, K.M.; Priori, S.G.; Collins, P.; Daly, C.; Graham, I.; Jonsson, B.; Schenck-Gustafsson, K.; Tendera, M. Cardiovascular diseases in women: a statement from the policy conference of the European Society of Cardiology. Eur. Heart. J. 2006, 27, 994–1005. [Google Scholar]
- Wang, C.Z.; Mehendale, S.R.; Yuan, C.S. Commonly used antioxidant botanicals: active constituents and their potential role in cardiovascular illness. Am. J. Chin. Med. 2007, 35, 543–558. [Google Scholar]
- Riccioni, G.; Mancini, B.; Di Ilio, E.; Bucciarelli, T.; D'Orazio, N. Protective effect of lycopene in cardiovascular disease. Eur. Rev. Med. Pharmacol. Sci. 2008, 12, 183–190. [Google Scholar]
- The Expert Panel. Summary of the second report of the National Cholesterol Education Program (NCEP) Expert Panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel II). JAMA 1993, 269, 3015–3023. [PubMed]
- Austin, M.A. Plasma triglyceride and coronary heart disease. Arterioscler. Thromb. 1991, 11, 2–14. [Google Scholar]
- Lampe, J.W. Health effects of vegetables and fruit: assessing mechanisms of action in human experimental studies. Am. J. Clin. Nutr. 1999, 70, 475S–490S. [Google Scholar]
- Dwyer, J. Overview: dietary approaches for reducing cardiovascular disease risks. J. Nutr. 1995, 125, 656S–665S. [Google Scholar]
- Haslam, D.W.; James, W.P. Obesity. Lancet 2005, 366, 1197–1209. [Google Scholar]
- Rayalam, S.; Della-Fera, M.A.; Baile, C.A. Phytochemicals and regulation of the adipocyte life cycle. J. Nutr. Biochem. 2008, 19, 717–726. [Google Scholar]
- Martorell, R.; Kettel Khan, L.; Hughes, M.L.; Grummer-Strawn, L.M. Overweight and obesity in preschool children from developing countries. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 959–967. [Google Scholar]
- International Obesity TaskForce (IOTF). Obesity in Europe, EU Platform Briefing Paper, prepared by Lobstein, T.; Rigby, N.; in collaboration with European Association for the Study of Obesity. 2005. Available online: http://www.iaso.org/popout.asp?linkto=http%3A//www.iotf.org/media/euobesity3.pdf (accessed on 25 February 2010).
- Pan, M.H.; Ghai, G.; Ho, C.T. Food bioactives, apoptosis, and cancer. Mol. Nutr. Food. Res. 2008, 52, 43–52. [Google Scholar]
- Food and Agriculture Organization of the United Nations (FAO). Report on Functional Foods, Food Quality and Standards Service (AGNS). 2007. Available online: http://www.fao.org/ag/agn/agns/files/Functional_Foods_Report_Nov2007.pdf (accessed on 25 February 2010).
- Laparra, J.M.; Sanz, Y. Interactions of gut microbiota with functional food components and nutraceuticals. Pharmacol. Res. 2010, 61, 219–225. [Google Scholar]
- Guarner, F.; Schaafsma, G.J. Probiotics. Int. J. Food Microbiol. 1998, 39, 237–238. [Google Scholar]
- de Vrese, M.; Schrezenmeir, J. Probiotics, prebiotics, and synbiotics. Adv. Biochem. Eng. Biotechnol. 2008, 111, 1–66. [Google Scholar]
- Bengmark, S. Ecological control of the gastrointestinal tract. The role of probiotic flora. Gut. 1998, 42, 2–7. [Google Scholar]
- Nissen, L.; Chingwaru, W.; Sgorbati, B.; Biavati, B.; Cencic, A. Gut health promoting activity of new putative probiotic/protective Lactobacillus spp. strains: a functional study in the small intestinal cell model. Int. J. Food. Microbiol. 2009, 135, 288–294. [Google Scholar]
- Maragkoudakis, P.A.; Chingwaru, W.; Gradisnik, L.; Tsakalidou, E.; Cencic, A. Lactic acid bacteria efficiently protect human and animal intestinal epithelial and immune cells from enteric virus infection. Int. J. Food. Microbiol. 2010. [Epub ahead of print].. [Google Scholar]
- Rijkers, G.T.; Bengmark, S.; Enck, P.; Haller, D.; Herz, U.; Kalliomaki, M.; Kudo, S.; Lenoir-Wijnkoop, I.; Mercenier, A.; Myllyluoma, E.; Rabot, S.; Rafter, J.; Szajewska, H.; Watzl, B.; Wells, J.; Wolvers, D.; Antoine, J.M. Guidance for substantiating the evidence for beneficial effects of probiotics: current status and recommendations for future research. J. Nutr. 2010, 140, 671S–676S. [Google Scholar]
- Minelli, E.B.; Benini, A. Relationship between number of bacteria and their probiotic effects. Microb. Ecol. Health Dis. 2008, 20, 1651–2235. [Google Scholar]
- Yao, T.C.; Chang, C.J.; Hsu, Y.H.; Huang, J.L. Probiotics for allergic diseases: Realities and myths. Pediatr. Allergy Immunol. 2009. [Epub ahead of print]. [Google Scholar]
- Kalliomaki, M.; Antoine, J.M.; Herz, U.; Rijkers, G.T.; Wells, J.M.; Mercenier, A. Guidance for substantiating the evidence for beneficial effects of probiotics: prevention and management of allergic diseases by probiotics. J. Nutr. 2010, 140, 713S–721S. [Google Scholar]
- Kumar, M.; Kumar, A.; Nagpal, R.; Mohania, D.; Behare, P.; Verma, V.; Kumar, P.; Poddar, D.; Aggarwal, P.K.; Henry, C.J.; Jain, S.; Yadav, H. Cancer-preventing attributes of probiotics: an update. Int. J. Food. Sci. Nutr. 2010. [Epub ahead of print]. [Google Scholar]
- Trois, L.; Cardoso, E.M.; Miura, E. Use of probiotics in HIV-infected children: a randomized double-blind controlled study. J. Trop. Pediatr. 2008, 54, 19–24. [Google Scholar]
- Kaur, I.P.; Kuhad, A.; Garg, A.; Chopra, K. Probiotics: delineation of prophylactic and therapeutic benefits. J. Med. Food. 2009, 12, 219–235. [Google Scholar]
- Douglas, L.C.; Sanders, M.E. Probiotics and prebiotics in dietetics practice. J. Am. Diet. Assoc. 2008, 108, 510–521. [Google Scholar]
- Hedin, C.; Whelan, K.; Lindsay, J.O. Evidence for the use of probiotics and prebiotics in inflammatory bowel disease: a review of clinical trials. Proc. Nutr. Soc. 2007, 66, 307–315. [Google Scholar]
- Oelschlaeger, T.A. Mechanisms of probiotic actions -A review. Int. J. Med. Microbiol. 2010, 300, 57–62. [Google Scholar]
- O'Sullivan, G.C.; Kelly, P.; O'Halloran, S.; Collins, C.; Collins, J.K.; Dunne, C.; Shanahan, F. Probiotics: An Emerging Therapy. Curr. Pharm. Design 2005, 11, 3–10. [Google Scholar]
- Dunne, C.; O'Mahony, L.; Murphy, L.; Thornton, G.; Morrissey, D.; O'Halloran, S.; Feeney, M.; Flynn, S.; Fitzgerald, G.; Daly, C.; Kiely, B.; O'Sullivan, G.C.; Shanahan, F.; Collins, J.K. In vitro selection criteria for probiotic bacteria of human origin: correlation with in vivo findings. Am. J. Clin. Nutr. 2001, 73, 386S–392S. [Google Scholar]
- Brower, V. Nutraceuticals: poised for a healthy slice of the healthcare market? Nat. Biotechnol. 1998, 16, 728–731. [Google Scholar]
- Trottier, G.; Bostrom, P.J.; Lawrentschuk, N.; Fleshner, N.E. Nutraceuticals and prostate cancer prevention: a current review. Nat. Rev. Urol. 2010, 7, 21–30. [Google Scholar]
- Zeisel, S.H. Regulation of "Nutraceuticals". Science 1999, 285, 185–186. [Google Scholar]
- Kalra, E.K. Nutraceutical -Definition and Introduction. AAPS PharmSci. 2003, 5, p. 25. Available online: http://www.aapsj.org/view.asp?art=ps050325 (accessed on 25 February 2010).
- The Regulation of Dietary Supplements. United States Pharmacopeia (USP). 2006. Available online: http://www.usp.org/pdf/EN/USPVerified/dietarySupplementRegulation.pdf (accessed on 13 January 2010).
- Hasler, C.M. Functional Foods: Their role in disease prevention and health promotion, Institute of Food Technologists’ Expert Panel on Food Safety and Nutrition. Foodtechnology. 1998, 52, 63–70. [Google Scholar]
- Gaffe, R. The Current and Future Regulation of Dietary Supplements. 2010. Available online: http://www.richardjaffeesq.com/jaffe/dietarysupplements.asp (accessed on 25 February 2010).
- Biddle, J.; Dasgupta-O’Brien, S.; Walch, A. Gut Health, Asheville Integrative Medicine (undated). Available online: http://www.docbiddle.com/moreinfo/guthealth.pdf (accessed on 25 February 2010).
- Mangum, J.B.; Everitt, J.I.; Bonner, J.C.; Moore, L.R.; Brody, A.R. Co-culture of primary pulmonary cells to model alveolar injury and translocation of proteins. In Vitro Cell. Dev. Biol. 1990, 26, 1135–1143. [Google Scholar]
- Arnold, J.T.; Kaufman, D.G.; Seppala, M.; Lessey, B.A. Endometrial stromal cells regulate epithelial cell growth in vitro: a new co-culture model. Hum. Reprod. 2001, 16, 836–845. [Google Scholar]
- Willemsen, L.E.; Schreurs, C.C.; Kroes, H.; Spillenaar Bilgen, E.J.; Van Deventer, S.J.; Van Tol, E.A. A co-culture model mimicking the intestinal mucosa reveals a regulatory role for myofibroblasts in immune-mediated barrier disruption. Dig. Dis. Sci. 2002, 47, 2316–2324. [Google Scholar]
- Depasquale, I.; Wheatley, D.N. Action of Lovastatin (Mevinolin) on an in vitro model of angiogenesis and its co-culture with malignant melanoma cell lines. Cancer Cell Int. 2006, 6, 1475–2867. [Google Scholar]
- Hendriks, J.; Riesle, J.; van Blitterswijk, C.A. Co-culture in cartilage tissue engineering. J. Tissue Eng. Regen. Med. 2007, 1, 170–178. [Google Scholar]
- Bhatia, S.N.; Balis, U.J.; Yarmush, M.L.; Toner, M. Effect of cell-cell interactions in preservation of cellular phenotype: cocultivation of hepatocytes and nonparenchymal cells. The FASEB J. 1999, 13, 1883–1900. [Google Scholar]
- Brillet, B.; Petiot, S.; Iochmann, S.; Gaud, G.; Planque, C.; Blechet, C.; Heuze-Vourc’h, N.; Gruel, Y.; Courty, Y.; Reverdiau, P. 025 Tumor-stromal cell interactions modulate metalloproteinase and kalli Krein expression in direct and indirect co-culture cell models. Revue des Maladies Respiratoires 2008, 25, 1167, (translated). [Google Scholar]
- Gradisnik, L.; Filipic, B.; de Vaureix, C.; Lefevre, F.; La Bonnardiere, C.; Cencic, A. Establishment of a functional cell culture model of the pig small intestine, LINZ, ALTEX 23. ALTEX Altern. Tierexp. 2006, 23, 94. [Google Scholar]
© 2010 by the authors; licensee MDPI, Basel, Switzerland This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Cencic, A.; Chingwaru, W. The Role of Functional Foods, Nutraceuticals, and Food Supplements in Intestinal Health. Nutrients 2010, 2, 611-625. https://doi.org/10.3390/nu2060611
Cencic A, Chingwaru W. The Role of Functional Foods, Nutraceuticals, and Food Supplements in Intestinal Health. Nutrients. 2010; 2(6):611-625. https://doi.org/10.3390/nu2060611
Chicago/Turabian StyleCencic, Avrelija, and Walter Chingwaru. 2010. "The Role of Functional Foods, Nutraceuticals, and Food Supplements in Intestinal Health" Nutrients 2, no. 6: 611-625. https://doi.org/10.3390/nu2060611
APA StyleCencic, A., & Chingwaru, W. (2010). The Role of Functional Foods, Nutraceuticals, and Food Supplements in Intestinal Health. Nutrients, 2(6), 611-625. https://doi.org/10.3390/nu2060611