Vitamin D Status Is Associated with Disease Activity among Rheumatology Outpatients



Abstract
:1. Introduction
2. Materials and Methods
3. Results

{kind=link}
| Case group (n = 60) | Control group (n = 56) | |||
|---|---|---|---|---|
| Mean | SD | Mean | SD | |
| Age * | 54.5 | 13.0 | 65.0 | 11.7 |
| BMI | 29.0 | 8.1 | 29.7 | 5.4 |
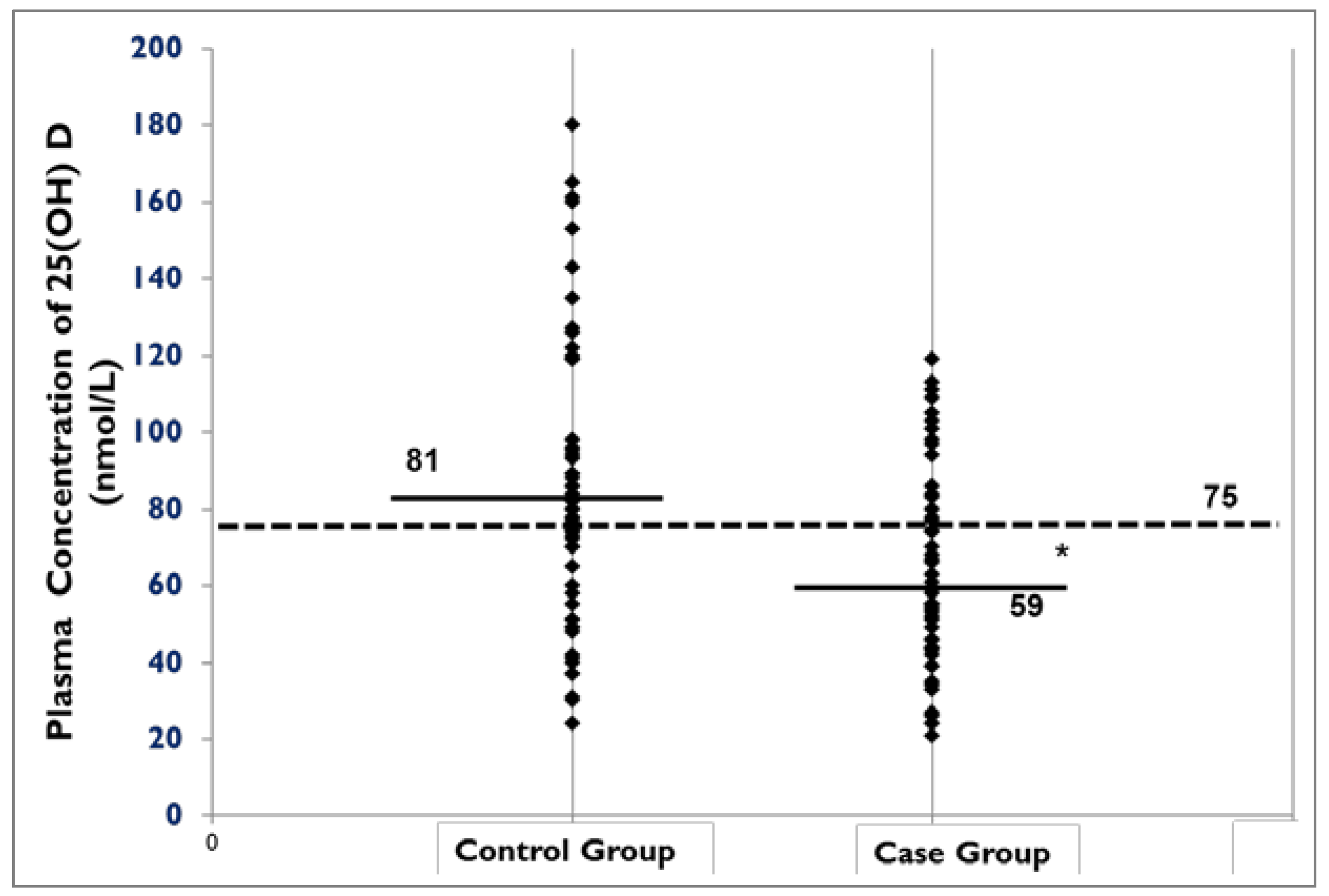
| Total 25 vitamin D value (nmol/L) * | 64.8 | 29.8 | 86.8 | 37.7 |
| Vitamin D supplement use (IU) | 1043.6 | 649.4 | 1008.0 | 664.7 |
| Serum Calcium * | 2.3 | 0.1 | 2.4 | 0.1 |
| Calcium supplement use (mg/day) * | 459.3 | 439 | 715.1 | 591 |
| Pho4 | 1.0 | 0.2 | 1.1 | 0.2 |
| ESR | 23.68 | 20.5 | 19.18 | 14.6 |
| CRP * | 12.9 | 19.3 | 6.07 | 9.6 |
| Creatinine | 72.1 | 44.4 | 78.8 | 33.9 |
| GFR | 69.9 | 28.7 | 71.6 | 20.5 |

4. Discussion
- Vitamin D receptor polymorphism and SARDs, and role of ethnicity in association between vitamin D and SARDs;
- Differences in vitamin D requirements between SARD cases and the general population as well as the requirements for individuals who are at risk of SARD and individuals with established SARD;
- Mechanisms of the impact of vitamin D in different pathways in immune system;
- The potential interaction between vitamin D and drugs in SARD cases and optimal supplementation approaches.
5. Conclusions
Acknowledgments
Conflict of Interest
References
- Bernatsky, S.; Lix, L.; Hanly, G.J.; Hudson, M.; Badley, E.; Peschken, C.; Pineau, C.A.; Clarke, A.E.; Fortin, R.; Smith, M.; et al. Surveillance of systemic autoimmune rheumatic diseases using administrative data. Rheumatol. Int. 2011, 31, 549–554. [Google Scholar] [CrossRef]
- The Impact of Arthritis in Canada: Today and over the Next 30 Years. Available online: http://www.arthritisnetwork.ca/downloads/20111022_Impact_of_arthritis.pdf (accessed on 12 November 2012).
- Cutolo, M.; Straub, R.H. Insights into endocrine-immunological disturbances in autoimmunity and their impact on treatment. Arthritis Res. Ther. 2009, 11, 218. [Google Scholar] [CrossRef]
- Whiting, S.J.; Langlois, K.A.; Vatanparast, H.; Greene-Finestone, L.S. The vitamin D status of Canadians relative to the 2011 Dietary Reference Intakes: An examination in children and adults with and without supplement use. Am. J. Clin. Nutr. 2011, 94, 128–135. [Google Scholar] [CrossRef]
- Institute of Medicine, Food and Nutrition Board. Dietary Reference Intakes for Calcium and Vitamin D. Available online: http://www.iom.edu/~/media/Files/Report%20Files/2010/Dietary-Reference-Intakes-for-Calcium-and-Vitamin-D/Vitamin%20D%20and%20Calcium%202010%20Report%20Brief.pdf (accessed on 26 September 2012).
- Holick, M.F. Evidence-based D-bate on health benefits of vitamin D revisited. Dermatoendocrinology 2012, 4, 183–190. [Google Scholar] [CrossRef]
- Cutolo, M.; Pizzorni, C.; Sulli, A. Vitamin D endocrine system involvement in autoimmune rheumatic diseases. Autoimmun. Rev. 2011, 11, 84–87. [Google Scholar] [CrossRef]
- Kriegel, M.A.; Manson, J.E.; Costenbader, K.H. Does vitamin D affect risk of developing autoimmune disease? A systematic review. Semin. Arthritis Rheum. 2011, 40, 512–531. [Google Scholar] [CrossRef]
- Song, G.G.; Bae, S.C.; Lee, Y.H. Association between vitamin D intake and the risk of rheumatoid arthritis: A meta-analysis. Clin. Rheumatol. 2012, 31, 1733–1739. [Google Scholar] [CrossRef]
- Webb, A.R.; Kline, L.; Holick, M.F. Influence of season and latitude on the cutaneous synthesis of vitamin D3: Exposure to winter sunlight in Boston and Edmonton will not promote vitamin D3 synthesis in human skin. J. Clin. Endocrinol. Metab. 1988, 67, 373–378. [Google Scholar] [CrossRef]
- The DAS28 Score. National Rheumatoid Arthritis Society. Available online: http://www.nras.org.uk/about_rheumatoid_arthritis/established_disease/managing_well/the_das28_score.aspx (accessed on 11 September 2011).
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M.; Endocrine Society. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef]
- Cutolo, M.; Otsa, K.; Laas, K.; Yprus, M.; Lehtme, R.; Secchi, M.E.; Sulli, A.; Paolino, S.; Seriolo, B. Circannual vitamin D serum levels and disease activity in rheumatoid arthritis: Northern vs. Southern Europe. Clin. Exp. Rheumatol. 2006, 24, 702–704. [Google Scholar]
- Merlino, L.A.; Curtis, J.; Mikuls, T.R.; Cerhan, J.R.; Criswell, L.A.; Saag, K.G. Iowa Women’s Health Study. Vitamin D intake is inversely associated with rheumatoid arthritis: Results from the Iowa Women’s Health Study. Arthritis Rheum. 2004, 50, 72–77. [Google Scholar] [CrossRef]
- Garcia-Lozano, J.R.; Gonzalez-Escribano, M.; Valenzuela, A.; Garcia, A.; Núñez-Roldán, A. Association of vitamin D receptor genotypes with early onset rheumatoid arthritis. Eur. J. Immunogenet. 2001, 28, 89–93. [Google Scholar] [CrossRef]
- Kröger, H.; Penttilä, I.M.; Alhava, E.M. Low serum vitamin D metabolites in women with rheumatoid arthritis. Scand. J. Rheumatol. 1993, 22, 172–177. [Google Scholar] [CrossRef]
- Oelzner, P.; Müller, A.; Deschner, F.; Hüller, M.; Abendroth, K.; Hein, G.; Stein, G. Relationship between disease activity and serum levels of vitamin D metabolites and PTH in rheumatoid arthritis. Calcif. Tissue Int. 1998, 62, 193–198. [Google Scholar] [CrossRef]
- Osteoporosis Canada. Available online: http://www.osteoporosis.ca/index.php/ci_id/5536/la_id/1.htm (accessed on 15 September 2012).
- Sainaghi, P.P.; Bellan, M.; Carda, S.; Cerutti, C.; Sola, D.; Nerviani, A.; Molinari, R.; Cisari, C.; Avanzi, G.C. Hypovitaminosis D and response to cholecalciferol supplementation in patients with autoimmune and non-autoimmune rheumatic diseases. Rheumatol. Int. 2012, 32, 3365–3372. [Google Scholar] [CrossRef]
- Vatanparast, H.; Calvo, M.S.; Green, T.J.; Whiting, S.J. Despite mandatory fortification of staple foods, vitamin D intakes of Canadian children and adults are inadequate. J. Steroid Biochem. Mol. Biol. 2010, 121, 301–303. [Google Scholar] [CrossRef]
- Sainaghi, P.P.; Bellan, M.; Nerviani, A.; Sola, D.; Molinari, R.; Cerutti, C.; Pirisi, M. Superiority of a high loading dose of cholecalciferol to correct hypovitaminosis D in patients with inflammatory/autoimmune rheumatic diseases. J. Rheumatol. 2013, 40, 166–172. [Google Scholar] [CrossRef]
- Sanders, K.M.; Stuart, A.L.; Williamson, E.J.; Simpson, J.A.; Kotowicz, M.A.; Young, D.; Nicholson, G.C. Annual high-dose oral vitamin D and falls and fractures in older women: A randomized controlled trial. JAMA 2010, 303, 1815–1822. [Google Scholar] [CrossRef]
- Lee, Y.H.; Bae, S.C.; Choi, S.J.; Ji, J.D.; Song, G.G. Associations between vitamin D receptor polymorphisms and susceptibility to rheumatoid arthritis and systemic lupus erythematosus: A meta-analysis. Mol. Biol. Rep. 2011, 38, 3643–3651. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Sabbagh, Z.; Markland, J.; Vatanparast, H. Vitamin D Status Is Associated with Disease Activity among Rheumatology Outpatients. Nutrients 2013, 5, 2268-2275. https://doi.org/10.3390/nu5072268
Sabbagh Z, Markland J, Vatanparast H. Vitamin D Status Is Associated with Disease Activity among Rheumatology Outpatients. Nutrients. 2013; 5(7):2268-2275. https://doi.org/10.3390/nu5072268
Chicago/Turabian StyleSabbagh, Zohreh, Janet Markland, and Hassanali Vatanparast. 2013. "Vitamin D Status Is Associated with Disease Activity among Rheumatology Outpatients" Nutrients 5, no. 7: 2268-2275. https://doi.org/10.3390/nu5072268
APA StyleSabbagh, Z., Markland, J., & Vatanparast, H. (2013). Vitamin D Status Is Associated with Disease Activity among Rheumatology Outpatients. Nutrients, 5(7), 2268-2275. https://doi.org/10.3390/nu5072268