Vitamin D Deficiency Increases the Risk of Gestational Diabetes Mellitus: A Meta-Analysis of Observational Studies

 ,
,
Abstract
:1. Introduction
2. Method
2.1. Data Sources
2.2. Study Selection
2.3. Statistical Analysis
3. Results
3.1. Selected Articles

3.2. Description of the Studies

{kind=link}
{kind=link}
{kind=link}
| Author and Year | Location | Study Type | Participants (n) | GDM (n) | GDM Criteria * | Assay Method | Mean 25(OH)D nmol/L (SD) | Prevalence | Significant | Adjustments** | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| GDM | NGT | ||||||||||
| Maghbooli (2008) [22] | Iran | Cross-sectional | 579 | 52 | C&C | RIA | 16.5(10.4) | 22.9(18.3) | 70.60% | Yes | a, b |
| Clifton-Bligh (2008) [23] | Australia | Cross-sectional | 307 | 81 | ADPS | LC–MS | 48.6(24.9) | 55.3(23.3) | 48% | Yes | a, b, c |
| Zhang (2008) [24] | US | Nested-case-control | 171 | 57 | ADA | ELISA | 60.4(21.22) | 75.13(24.21) | 19.80% | Yes | a, b, c, d |
| Farrant (2009) [16] | India | Cross-sectional | 559 | 39 | C&C | RIA | 49.3(31.2) | 46.4(30.9) | 66% | No | a, b, e, f |
| Soheilykhah (2010) [25] | Iran | Case-control | 165 | 54 | C&C | ELISA | 24.01(20.62) | 32.2(35.74) | 78.40% | Yes | NR |
| Baker (2012) [15] | US | Nested-case-control | 180 | 60 | NDDG | LC–MS | 97.0(29.0) | 86.0(22.0) | 7.20% | Yes | a, b, e, h |
| Makgoba (2011) [26] | UK | Case-control | 248 | 90 | WHO | LC–MS | 47.2(26.7) | 47.6 (26.7) | 58.80% | No | a, b, c, d, e, g |
| Parlea (2012) [27] | Canada | Nested-case-control | 337 | 118 | NDDG | CLIA | 56.3(19.4) | 62.0(21.6) | NR | Yes | h, i |
| Fernandez-Alonso (2012) [28] | Spain | Cross-sectional | 466 | 36 | ADA | ECLIA | NR | NR | 23.40% | NR | NR |
| Parildar (2013) [29] | Turkey | Case-control | 122 | 44 | IADPSG | CLIA | 48.67(23.21) | 57.16(24.96) | 43.40% | No | NR |
| Wang (2012) [30] | China | Nested-case-control | 400 | 200 | ADA | ELISA | 22.4(10.7) | 25.9(12.3) | 96.25% | Yes | a, d, j |
| Burris (2012) [31] | US | Cross-sectional | 1155 | 68 | ADA | CLIA | NR | NR | 33.10% | NR | a, b, c, e, h, k, l, m, n, o, p, t |
| Perez-Ferre (2012) [32] | Spain | Cross-sectional | 266 | 49 | ADA | CLIA | NR | NR | 59.02% | NR | a, c, d, g |
| Zuhur (2013) [33] | Turkey | Cross-sectional | 402 | 234 | IADPSG | ECLIA | 30.8(16.3) | 36.0(16.2) | 84.30% | Yes | a, b, d, g |
| Bener (2013) [34] | Qatari | Prospective cohort | 1873 | 260 | WHO | RIA | NR | NR | 48.40% | NR | NR |
| Lacroix (2014) [35] | Canada | Cross-sectional | 655 | 54 | IADPSG | LC–MS | 57.5(17.2) | 63.5(18.9) | 26.70% | Yes | a, c, d, e, g, r, s, t, u |
| McManus (2014) [36] | Canada | Case-control | 73 | 36 | CDA | RIA | 77.3(24.3) | 93.2(19.2) | 6.85% | Yes | a, b |
| Park (2014) [37] | Korea | Prospective cohort | 523 | 23 | C&C | ECLIA | 49.4(19.4) | 48(24.8) | 88.90% | No | a, b, e, h, g, v |
| Arnold (2015) [38] | US | Nested-case-control | 652 | 135 | ADA | LC–MS | 59.7(23.5) | 66.6(22) | 25.61% | Yes | a, b, c, d, e |
| Pleskacova (2015) [39] | Czech | Case-control | 76 | 47 | WHO | EIASA | 28(3.76) | 31.85(4.62) | 94.7% | No | b |
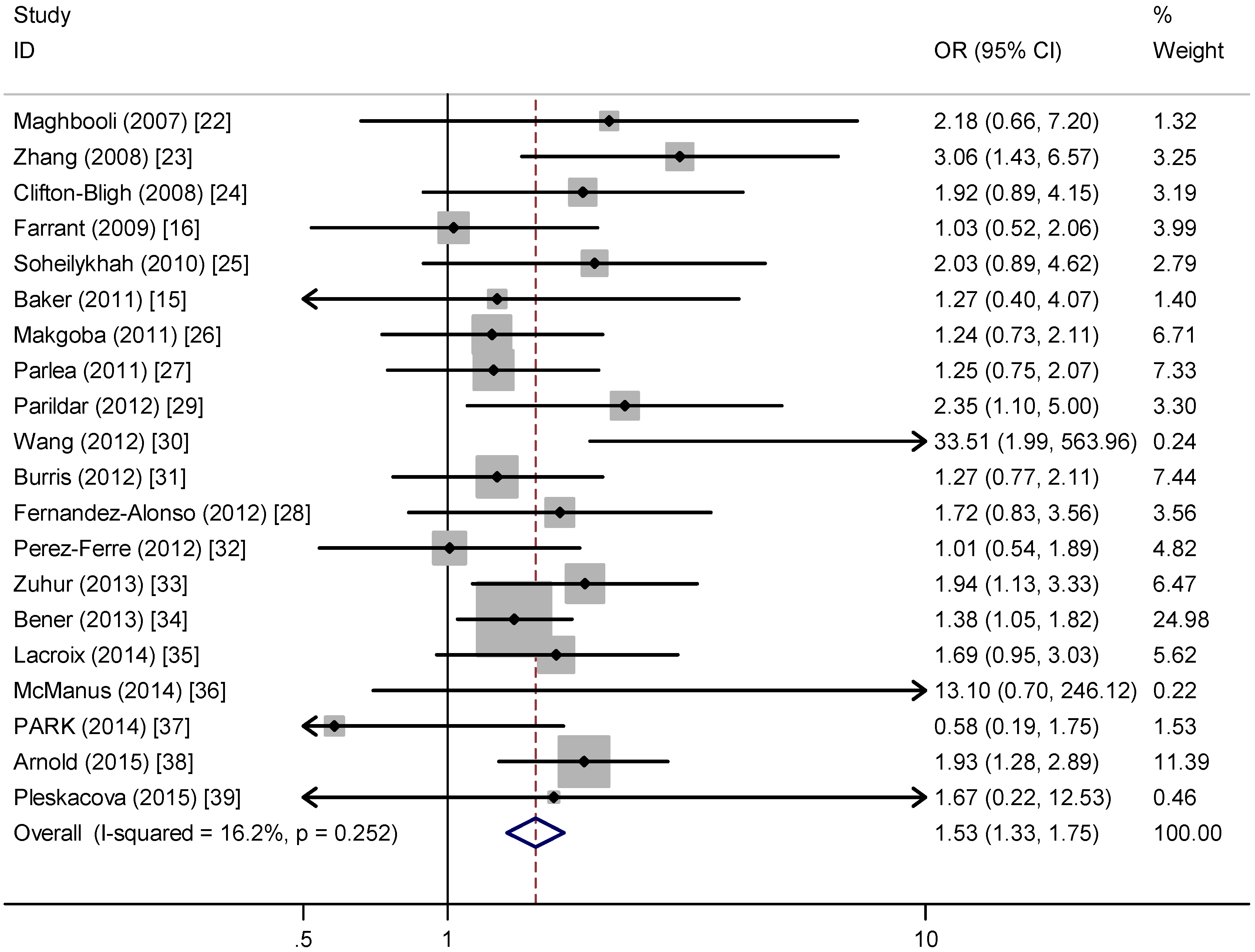
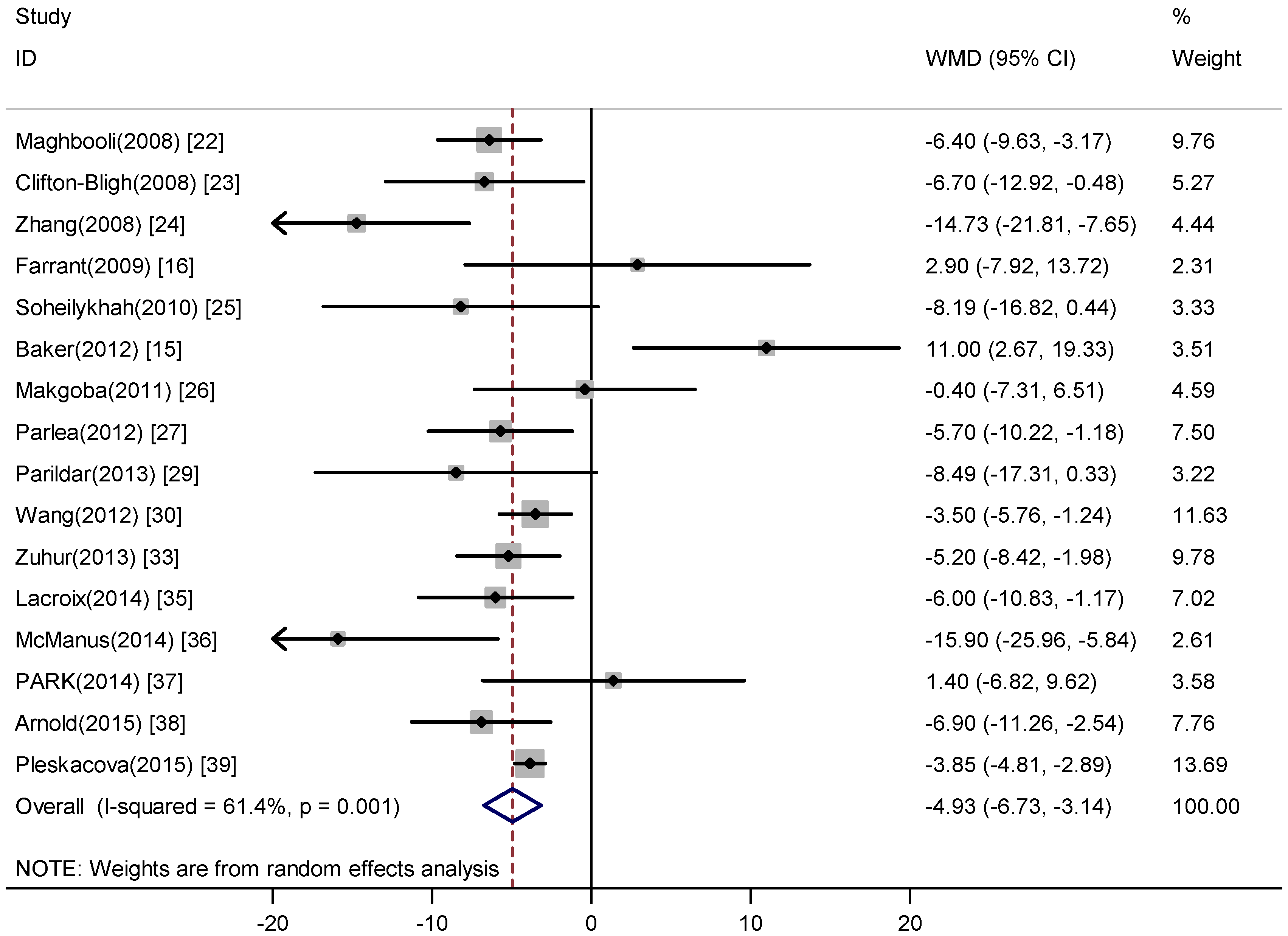
3.3. Main Analysis


3.4. Sensitivity and Subgroup Analyses
3.5. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Association, A.D. Standards of medical care in diabetes—2014. Diabetes Care 2014, 37 (Suppl. 1), S14–S80. [Google Scholar] [CrossRef] [PubMed]
- Reece, E.A.; Leguizamon, G.; Wiznitzer, A. Gestational diabetes: The need for a common ground. Lancet 2009, 373, 1789–1797. [Google Scholar] [CrossRef]
- Jarrett, R.J. Reflections on gestational diabetes mellitus. Lancet (Lond., Engl.) 1981, 2, 1220–1221. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Chen, T.C. Vitamin D deficiency: A worldwide problem with health consequences. Am. J. Clin. Nutr. 2008, 87, 1080s–1086s. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Marwaha, R.; Tandon, N.; Chopra, S.; Agarwal, N.; Garg, M.; Sharma, B.; Kanwar, R.; Bhadra, K.; Singh, S.; Mani, K. Vitamin D status in pregnant indian women across trimesters and different seasons and its correlation with neonatal serum 25-hydroxyvitamin D levels. Br. J. Nutr. 2011, 106, 1383–1389. [Google Scholar] [CrossRef] [PubMed]
- Perampalam, S.; Ganda, K.; CHOW, K.A.; Opie, N.; Hickman, P.E.; Shadbolt, B.; Hennessy, A.; Grunstein, H.; Nolan, C.J. Vitamin D status and its predictive factors in pregnancy in 2 Australian populations. Aust. N. Z. J. Obstet. Gynaecol. 2011, 51, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Tao, M.; Shao, H.; Gu, J.; Zhen, Z. Vitamin d status of pregnant women in Shanghai, China. J. Matern.-Fetal Neonat. Med. 2012, 25, 237–239. [Google Scholar] [CrossRef] [PubMed]
- Sääf, M.; Fernell, E.; Kristiansson, F.; Barnevik Olsson, M.; Gustafsson, S.A.; Bågenholm, G. Severe vitamin D deficiency in pregnant women of somali origin living in sweden. Acta Paediatr. 2011, 100, 612–614. [Google Scholar] [CrossRef] [PubMed]
- Shibata, M.; Suzuki, A.; Sekiya, T.; Sekiguchi, S.; Asano, S.; Udagawa, Y.; Itoh, M. High prevalence of hypovitaminosis D in pregnant Japanese women with threatened premature delivery. J. Bone Miner. Metab. 2011, 29, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Aghajafari, F.; Nagulesapillai, T.; Ronksley, P.E.; Tough, S.C.; O’Beirne, M.; Rabi, D.M. Association between maternal serum 25-hydroxyvitamin D level and pregnancy and neonatal outcomes: Systematic review and meta-analysis of observational studies. BMJ (Clin. Res. Ed.) 2013, 346, f1169. [Google Scholar] [CrossRef] [PubMed]
- Senti, J.; Thiele, D.K.; Anderson, C.M. Maternal vitamin D status as a critical determinant in gestational diabetes. J. Obst. Gyn. Neo. 2012, 41, 328–338. [Google Scholar] [CrossRef] [PubMed]
- Rudnicki, P.; Mølsted-Pedersen, L. Effect of 1, 25-dihydroxycholecalciferol on glucose metabolism in gestational diabetes mellitus. Diabetologia 1997, 40, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Baker, A.M.; Haeri, S.; Camargo, C.A., Jr.; Stuebe, A.M.; Boggess, K.A. First-trimester maternal vitamin D status and risk for gestational diabetes (GDM) a nested case-control study. Diabetes/Metab. Res. Rev. 2012, 28, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Farrant, H.J.; Krishnaveni, G.V.; Hill, J.C.; Boucher, B.J.; Fisher, D.J.; Noonan, K.; Osmond, C.; Veena, S.R.; Fall, C.H. Vitamin D insufficiency is common in indian mothers but is not associated with gestational diabetes or variation in newborn size. Eur. J. Clin. Nutr. 2009, 63, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis of observational studies in epidemiology (moose) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Duckitt, K.; Harrington, D. Risk factors for pre-eclampsia at antenatal booking: Systematic review of controlled studies. BMJ (Clin. Res. Ed.) 2005, 330, 565. [Google Scholar] [CrossRef] [PubMed]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ (Clin. Res. Ed.) 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Controll. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Maghbooli, Z.; Hossein-Nezhad, A.; Karimi, F.; Shafaei, A.R.; Larijani, B. Correlation between vitamin D3 deficiency and insulin resistance in pregnancy. Diabetes/Metab. Res. Rev. 2008, 24, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Clifton-Bligh, R.J.; McElduff, P.; McElduff, A. Maternal vitamin D deficiency, ethnicity and gestational diabetes. Diabet. Med. 2008, 25, 678–684. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Qiu, C.; Hu, F.B.; David, R.M.; van Dam, R.M.; Bralley, A.; Williams, M.A. Maternal plasma 25-hydroxyvitamin D concentrations and the risk for gestational diabetes mellitus. PLoS ONE 2008, 3, e3753. [Google Scholar] [CrossRef] [PubMed]
- Soheilykhah, S.; Mojibian, M.; Rashidi, M.; Rahimi-Saghand, S.; Jafari, F. Maternal vitamin D status in gestational diabetes mellitus. Nutr. Clin. Pract. 2010, 25, 524–527. [Google Scholar] [CrossRef] [PubMed]
- Makgoba, M.; Nelson, S.M.; Savvidou, M.; Messow, C.M.; Nicolaides, K.; Sattar, N. First-trimester circulating 25-hydroxyvitamin D levels and development of gestational diabetes mellitus. Diabetes Care 2011, 34, 1091–1093. [Google Scholar] [CrossRef] [PubMed]
- Parlea, L.; Bromberg, I.L.; Feig, D.S.; Vieth, R.; Merman, E.; Lipscombe, L.L. Association between serum 25-hydroxyvitamin D in early pregnancy and risk of gestational diabetes mellitus. Diabet. Med. 2012, 29, e25–e32. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Alonso, A.M.; Dionis-Sanchez, E.C.; Chedraui, P.; Gonzalez-Salmeron, M.D.; Perez-Lopez, F.R. First-trimester maternal serum 25-hydroxyvitamin D3 status and pregnancy outcome. Int. J. Gynecol. Obstet. 2012, 116, 6–9. [Google Scholar] [CrossRef] [PubMed]
- Parildar, H.; Dogruk Unal, A.; Aksan Desteli, G.; Cigerli, O.; Guvener Demirag, N. Frequency of vitamin D deficiency in pregnant diabetics at baskent university hospital, istanbul. Pak. J. Med. Sci. 2013, 29, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Wang, O.; Nie, M.; Hu, Y.Y.; Zhang, K.; Li, W.; Ping, F.; Liu, J.T.; Chen, L.M.; Xing, X.P. Association between vitamin D insufficiency and the risk for gestational diabetes mellitus in pregnant Chinese women. Biomed. Environ. Sci. 2012, 25, 399–406. [Google Scholar] [PubMed]
- Burris, H.H.; Rifas-Shiman, S.L.; Kleinman, K.; Litonjua, A.A.; Huh, S.Y.; Rich-Edwards, J.W.; Camargo, C.A., Jr.; Gillman, M.W. Vitamin D deficiency in pregnancy and gestational diabetes mellitus. Am. J. Obstet. Gynecol. 2012, 207, 182:e1–182:e8. [Google Scholar] [CrossRef] [PubMed]
- Perez-Ferre, N.; Torrejon, M.J.; Fuentes, M.; Fernandez, M.D.; Ramos, A.; Bordiu, E.; del Valle, L.; Rubio, M.A.; Bedia, A.R.; Montanez, C.; et al. Association of low serum 25-hydroxyvitamin D levels in pregnancy with glucose homeostasis and obstetric and newborn outcomes. Endocr. Pract. 2012, 18, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Zuhur, S.S.; Erol, R.S.; Kuzu, I.; Altuntas, Y. The relationship between low maternal serum 25-hydroxyvitamin D levels and gestational diabetes mellitus according to the severity of 25-hydroxyvitamin D deficiency. Clinics (Sao Paulo, Braz.) 2013, 68, 658–664. [Google Scholar] [CrossRef]
- Bener, A.; Al-Hamaq, A.O.; Saleh, N.M. Association between vitamin D insufficiency and adverse pregnancy outcome: Global comparisons. Int. J. Women’s Health 2013, 5, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Lacroix, M.; Battista, M.C.; Doyon, M.; Houde, G.; Menard, J.; Ardilouze, J.L.; Hivert, M.F.; Perron, P. Lower vitamin D levels at first trimester are associated with higher risk of developing gestational diabetes mellitus. Acta Diabetol. 2014, 51, 609–616. [Google Scholar] [CrossRef] [PubMed]
- McManus, R.; Summers, K.; de Vrijer, B.; Cohen, N.; Thompson, A.; Giroux, I. Maternal, umbilical arterial and umbilical venous 25-hydroxyvitamin D and adipocytokine concentrations in pregnancies with and without gestational diabetes. Clin. Endocrinol. 2014, 80, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Yoon, H.K.; Ryu, H.M.; Han, Y.J.; Lee, S.W.; Park, B.K.; Park, S.Y.; Yim, C.H.; Kim, S.H. Maternal vitamin D deficiency in early pregnancy is not associated with gestational diabetes mellitus development or pregnancy outcomes in Korean pregnant women in a prospective study. J. Nutr. Sci. Vitaminol. 2014, 60, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Arnold, D.L.; Enquobahrie, D.A.; Qiu, C.; Huang, J.; Grote, N.; VanderStoep, A.; Williams, M.A. Early pregnancy maternal vitamin D concentrations and risk of gestational diabetes mellitus. Paediatr. Perinat. Ep. 2015, 29, 200–210. [Google Scholar] [CrossRef] [PubMed]
- Pleskacova, A.; Bartakova, V.; Pacal, L.; Kuricova, K.; Belobradkova, J.; Tomandl, J.; Kankova, K. Vitamin D status in women with gestational diabetes mellitus during pregnancy and postpartum. BioMed. Res. Int. 2015, 2015, 260624. [Google Scholar] [CrossRef] [PubMed]
- Poel, Y.H.; Hummel, P.; Lips, P.; Stam, F.; van der Ploeg, T.; Simsek, S. Vitamin d and gestational diabetes: A systematic review and meta-analysis. Eur. J. Intern. Med. 2012, 23, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Chiu, K.C.; Chu, A.; Go, V.L.; Saad, M.F. Hypovitaminosis D is associated with insulin resistance and beta cell dysfunction. Am. J. Clin. Nutr. 2004, 79, 820–825. [Google Scholar] [PubMed]
- Norman, A.W.; Frankel, J.B.; Heldt, A.M.; Grodsky, G.M. Vitamin D deficiency inhibits pancreatic secretion of insulin. Science 1980, 209, 823–825. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, A.; Williams, J.S. Vitamin D and insulin sensitivity: Can gene association and pharmacogenetic studies of the vitamin d receptor provide clarity? Metab. Clin. Exp. 2012, 61, 759–761. [Google Scholar] [CrossRef] [PubMed]
- Draznin, B.; Sussman, K.E.; Eckel, R.H.; Kao, M.; Yost, T.; Sherman, N.A. Possible role of cytosolic free calcium concentrations in mediating insulin resistance of obesity and hyperinsulinemia. J. Clin. Investig. 1988, 82, 1848–1852. [Google Scholar] [CrossRef] [PubMed]
- Asemi, Z.; Hashemi, T.; Karamali, M.; Samimi, M.; Esmaillzadeh, A. Effects of vitamin D supplementation on glucose metabolism, lipid concentrations, inflammation, and oxidative stress in gestational diabetes: A double-blind randomized controlled clinical trial. Am. J. Clin. Nutr. 2013, 98, 1425–1432. [Google Scholar] [CrossRef] [PubMed]
- Soheilykhah, S.; Mojibian, M.; Moghadam, M.J.; Shojaoddiny-Ardekani, A. The effect of different doses of vitamin D supplementation on insulin resistance during pregnancy. Gynecol. Endocrinol. 2013, 29, 396–399. [Google Scholar] [CrossRef] [PubMed]
- Asemi, Z.; Samimi, M.; Tabassi, Z.; Shakeri, H.; Esmaillzadeh, A. Vitamin D supplementation affects serum high-sensitivity C-reactive protein, insulin resistance, and biomarkers of oxidative stress in pregnant women. J. Nutr. 2013, 143, 1432–1438. [Google Scholar] [CrossRef] [PubMed]
- Wacker, M.; Holick, M.F. Sunlight and vitamin D: A global perspective for health. Derm.-Endocrinol. 2013, 5, 51–108. [Google Scholar] [CrossRef] [PubMed]
- Basraon, S.K.; Mele, L.; Myatt, L.; Roberts, J.M.; Hauth, J.C.; Leveno, K.J.; Varner, M.W.; Wapner, R.J.; Thorp, J.M., Jr.; Peaceman, A.M.; et al. Relationship of early pregnancy waist-to-hip ratio versus body mass index with gestational diabetes mellitus and insulin resistance. Available online: http://europepmc.org/abstract/med/26352680 (accessed on 9 September 2015).
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, M.-X.; Pan, G.-T.; Guo, J.-F.; Li, B.-Y.; Qin, L.-Q.; Zhang, Z.-L. Vitamin D Deficiency Increases the Risk of Gestational Diabetes Mellitus: A Meta-Analysis of Observational Studies. Nutrients 2015, 7, 8366-8375. https://doi.org/10.3390/nu7105398
Zhang M-X, Pan G-T, Guo J-F, Li B-Y, Qin L-Q, Zhang Z-L. Vitamin D Deficiency Increases the Risk of Gestational Diabetes Mellitus: A Meta-Analysis of Observational Studies. Nutrients. 2015; 7(10):8366-8375. https://doi.org/10.3390/nu7105398
Chicago/Turabian StyleZhang, Meng-Xi, Guo-Tao Pan, Jian-Fen Guo, Bing-Yan Li, Li-Qiang Qin, and Zeng-Li Zhang. 2015. "Vitamin D Deficiency Increases the Risk of Gestational Diabetes Mellitus: A Meta-Analysis of Observational Studies" Nutrients 7, no. 10: 8366-8375. https://doi.org/10.3390/nu7105398
APA StyleZhang, M. -X., Pan, G. -T., Guo, J. -F., Li, B. -Y., Qin, L. -Q., & Zhang, Z. -L. (2015). Vitamin D Deficiency Increases the Risk of Gestational Diabetes Mellitus: A Meta-Analysis of Observational Studies. Nutrients, 7(10), 8366-8375. https://doi.org/10.3390/nu7105398