Antidepressant Use is Associated with Increased Energy Intake and Similar Levels of Physical Activity

Abstract
:1. Introduction
2. Experimental Section
2.1. Population
2.2. Medication and Tobacco Use
2.3. Energy Intake
2.4. Physical Activity and Sedentary Behaviors
2.5. Depression Symptoms
2.6. Covariates
2.7. Data Analysis
3. Results
3.1. Demographics

{kind=link}
{kind=link}
{kind=link}
| Antidepressant Non-Users (n = 2818) | Antidepressant Users (n = 221) | p-Value 1 | |
|---|---|---|---|
| Age (mean ± S.E.), years | 43.5 ± 0.6 | 48.9 ± 1.0 | <0.001 |
| Gender (% Women) | 46.6 | 72.6 | <0.001 |
| Race (% White non-Hispanic) | 70 | 89.1 | <0.001 |
| Completed some college (%) | 58.5 | 55.3 | 0.412 |
| Annual Family Income < $20,000 (%) | 15.1 | 16.2 | 0.589 |
| Annual Family Income $20,000 to $75,000 (%) | 54.9 | 52.1 | 0.564 |
| Annual Family Income ≥ $75,000 (%) | 30.1 | 31.7 | 0.724 |
| BMI (mean ± S.E.), kg/m2 | 28.0 ± 0.3 | 29.8 ± 0.5 | 0.004 |
| Normal-Weight (%) | 32.3 | 30.3 | 0.693 |
| Overweight (%) | 33.9 | 24.7 | 0.040 |
| Obese (%) | 31.2 | 42.2 | 0.006 |
| Mean PHQ-9 Depression Score (Scale 0–27) | 2.3 ± 0.1 | 4.7 ± 0.4 | <0.001 |
| Used Tobacco/Nicotine in the last 5 days (%) | 31.2 | 33.5 | 0.422 |
| Antipsychotic use (%) | 0.6 | 5.9 | 0.048 |
| Non-psychiatric medications (mean ± S.E.), n | 1.2 ± 0.1 | 3.2 ± 0.2 | <0.001 |
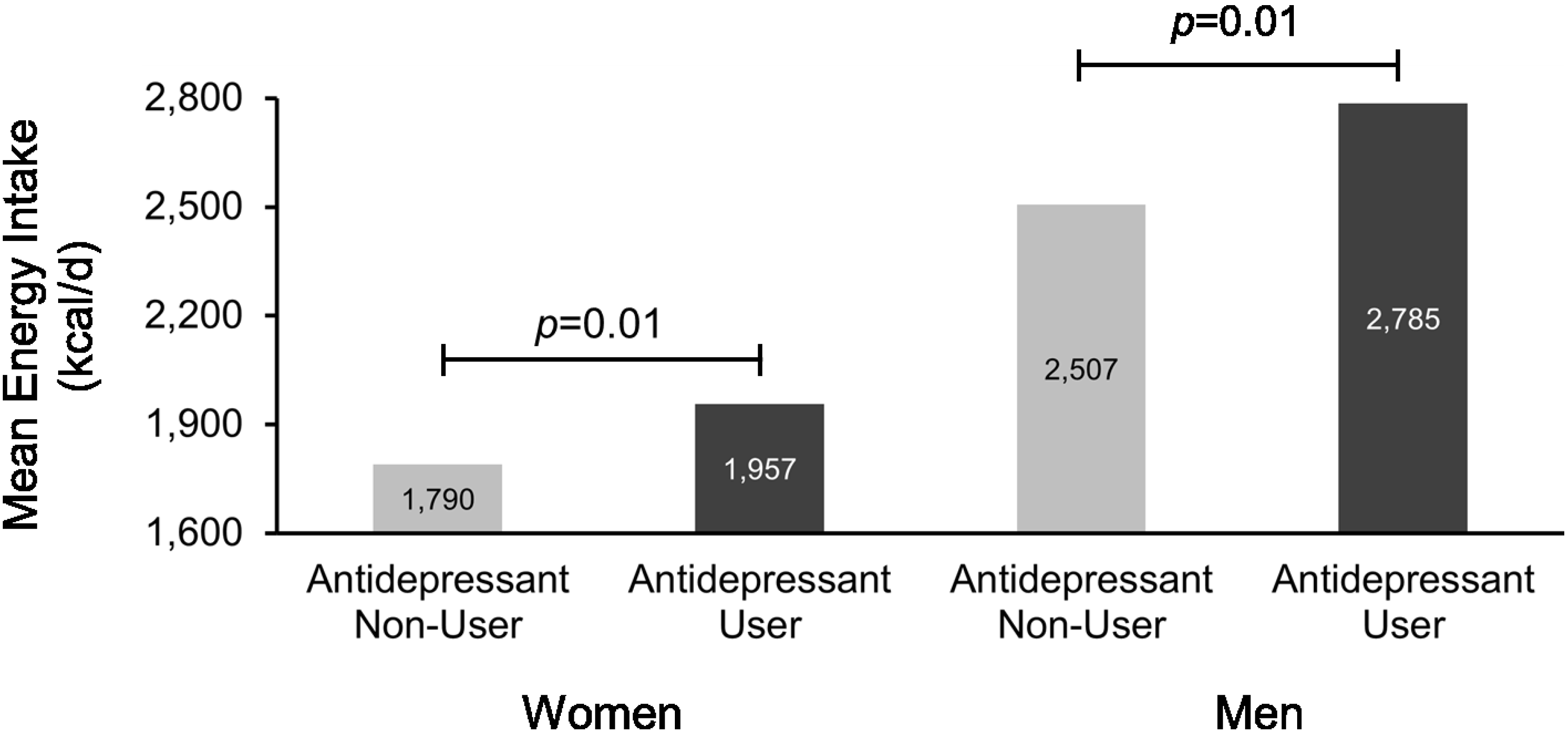
3.2. Energy Intake and Diet Composition
| Macronutrient 3 (% Energy) | Antidepressant Non-Users (n = 2818) | Antidepressant Users (n = 221) | p-Value 2 |
|---|---|---|---|
| Carbohydrate (%) | 48.1 ± 0.2 | 48.7 ± 0.6 | 0.484 |
| Sugar (%) | 21.8 ± 0.3 | 23.0 ± 0.7 | 0.118 |
| Non-sugar carbohydrates (%) | 26.2 ± 0.2 | 25.7 ± 0.5 | 0.413 |
| Protein (%) | 15.5 ± 0.1 | 14.9 ± 0.3 | 0.033 |
| Total Fat (%) | 33.2 ± 0.2 | 33.8 ± 0.5 | 0.434 |
| SFAs (%) | 11.1 ± 0.1 | 11.6 ± 0.2 | 0.191 |
| MUFAs (%) | 12.2 ± 0.1 | 12.3 ± 0.2 | 0.650 |
| PUFAs (%) | 7.1 ± 0.1 | 7.1 ± 0.2 | 0.785 |
| Alcohol (%) | 3.2 ± 0.2 | 2.6 ± 0.4 | 0.219 |

3.3. Physical Activity and Sedentary Behavior


4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Blumenthal, S.R.; Castro, V.M.; Clements, C.C.; Rosenfield, H.R.; Murphy, S.N.; Fava, M.; Weilburg, J.B.; Erb, J.L.; Churchill, S.E.; Kohane, I.S.; et al. An electronic health records study of long-term weight gain following antidepressant use. JAMA Psychiatry 2014, 71, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Kivimaki, M.; Hamer, M.; Batty, G.D.; Geddes, J.R.; Tabak, A.G.; Pentti, J.; Virtanen, M.; Vahtera, J. Antidepressant medication use, weight gain, and risk of type 2 diabetes: A population-based study. Diabetes Care 2010, 33, 2611–2616. [Google Scholar] [CrossRef] [PubMed]
- Rigler, S.K.; Webb, M.J.; Redford, L.; Brown, E.F.; Zhou, J.; Wallace, D. Weight outcomes among antidepressant users in nursing facilities. J. Am. Geriatr. Soc. 2001, 49, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, T.L.; Nihalani, N.; Jindal, S.; Virk, S.; Jones, N. Psychiatric medication-induced obesity: A review. Obes. Rev. 2004, 5, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Serretti, A.; Mandelli, L. Antidepressants and body weight: A comprehensive review and meta-analysis. J. Clin. Psychiatry 2010, 71, 1259–1272. [Google Scholar] [CrossRef] [PubMed]
- Su, J.A.; Tsang, H.Y. Comparison of weight changes in patients treated with different antidepressants: Clinical experiences in Taiwanese patients. Chang Gung Med. J. 2006, 29, 154–161. [Google Scholar] [PubMed]
- Virk, S.; Schwartz, T.L.; Jindal, S.; Nihalani, N.; Jones, N. Psychiatric medication induced obesity: An aetiologic review. Obes. Rev. 2004, 5, 167–170. [Google Scholar] [CrossRef] [PubMed]
- Dent, R.; Blackmore, A.; Peterson, J.; Habib, R.; Kay, G.P.; Gervais, A.; Taylor, V.; Wells, G. Changes in body weight and psychotropic drugs: A systematic synthesis of the literature. PLoS ONE 2012, 7, e36889. [Google Scholar] [CrossRef] [PubMed]
- Lopresti, A.L.; Drummond, P.D. Obesity and psychiatric disorders: Commonalities in dysregulated biological pathways and their implications for treatment. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2013, 45, 92–99. [Google Scholar] [CrossRef] [PubMed]
- Patten, S.B.; Williams, J.V.; Lavorato, D.H.; Khaled, S.; Bulloch, A.G. Weight gain in relation to major depression and antidepressant medication use. J. Affect. Disorders 2011, 134, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Raeder, M.B.; Bjelland, I.; Emil Vollset, S.; Steen, V.M. Obesity, dyslipidemia, and diabetes with selective serotonin reuptake inhibitors: The Hordaland Health Study. J. Clin. Psychiatry 2006, 67, 1974–1982. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.S.; Gau, S.S.; Lai, M.S. Long-term antidepressant use and the risk of type 2 diabetes mellitus: A population-based, nested case-control study in Taiwan. J. Clin. Psychiatry 2014, 75, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Grontved, A.; Hu, F.B. Television viewing and risk of type 2 diabetes, cardiovascular disease, and all-cause mortality: A meta-analysis. J. Am. Med. Assoc. 2011, 305, 2448–2455. [Google Scholar] [CrossRef] [PubMed]
- Thorp, A.A.; Owen, N.; Neuhaus, M.; Dunstan, D.W. Sedentary behaviors and subsequent health outcomes in adults a systematic review of longitudinal studies, 1996–2011. Am. J. Prev. Med. 2011, 41, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Davison, K.M. The relationships among psychiatric medications, eating behaviors, and weight. Eat. Behav. 2013, 14, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, U.; Kraus, T.; Himmerich, H.; Schuld, A.; Pollmacher, T. Epidemiology, implications and mechanisms underlying drug-induced weight gain in psychiatric patients. J. Psychiatr. Res. 2003, 37, 193–220. [Google Scholar] [CrossRef]
- National Health and Nutrition Examination Survey. Available online: http://www.cdc.gov/nchs/nhanes.htm (accessed on 15 October 2015).
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [PubMed]
- Willett, W.C. Nutritional Epidemiology; Oxford University Press: New York, NY, USA, 1998. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9, validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.; Rief, W.; Klaiberg, A.; Braehler, E. Validity of the brief patient health questionnaire mood scale (PHQ-9) in the general population. Gen. Hosp. Psychiatry 2006, 28, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Austin, G.L.; Ogden, L.G.; Hill, J.O. Trends in carbohydrate, fat, and protein intakes and association with energy intake in normal-weight, overweight, and obese individuals: 1971–2006. Am. J. Clin. Nutr. 2011, 93, 836–843. [Google Scholar] [CrossRef] [PubMed]
- Lok, A.; Visscher, T.L.; Koeter, M.W.; Assies, J.; Bockting, C.L.; Verschuren, W.M.; Gill, A.; Schene, A.H. The ‘Weight’ of recurrent depression: A comparison between individuals with recurrent depression and the general population and the influence of antidepressants. Psychother. Psychosom. 2010, 79, 386–388. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, M.A.; Singh-Manoux, A.; Brunner, E.J.; Kaffashian, S.; Shipley, M.J.; Kivimäki, M.; Nabi, H. Bidirectional association between physical activity and symptoms of anxiety and depression: The Whitehall II study. Eur. J. Epidemiol. 2012, 27, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Pereira, S.M.P.; Geoffroy, M.C.; Power, C. Depressive symptoms and physical activity during 3 decades in adult life: Bidirectional associations in a prospective cohort study. JAMA Psychiatry 2014, 71, 1373–1380. [Google Scholar] [CrossRef] [PubMed]
- Uebelacker, L.A.; Eaton, C.B.; Weisberg, R.; Sands, M.; Williams, C.; Calhoun, D.; Manson, J.E.; Denburg, N.L.; Taylor, T. Social support and physical activity as moderators of life stress in predicting baseline depression and change in depression over time in the Women’s Health Initiative. Soc. Psychiatry Psychiatr. Epidemiol. 2013, 48, 1971–1982. [Google Scholar] [CrossRef] [PubMed]
- Roshanaei-Moghaddam, B.; Katon, W.J.; Russo, J. The longitudinal effects of depression on physical activity. Gener. Hosp. Psychiatry 2009, 31, 306–315. [Google Scholar] [CrossRef] [PubMed]
- Maurer, J.; Taren, D.L.; Teixeira, P.J.; Thomson, C.A.; Lohman, T.G.; Going, S.B.; Houtkooper, L.B. The psychosocial and behavioral characteristics related to energy misreporting. Nutr. Rev. 2006, 64, 53–66. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jensen-Otsu, E.; Austin, G.L. Antidepressant Use is Associated with Increased Energy Intake and Similar Levels of Physical Activity. Nutrients 2015, 7, 9662-9671. https://doi.org/10.3390/nu7115489
Jensen-Otsu E, Austin GL. Antidepressant Use is Associated with Increased Energy Intake and Similar Levels of Physical Activity. Nutrients. 2015; 7(11):9662-9671. https://doi.org/10.3390/nu7115489
Chicago/Turabian StyleJensen-Otsu, Elsbeth, and Gregory L. Austin. 2015. "Antidepressant Use is Associated with Increased Energy Intake and Similar Levels of Physical Activity" Nutrients 7, no. 11: 9662-9671. https://doi.org/10.3390/nu7115489
APA StyleJensen-Otsu, E., & Austin, G. L. (2015). Antidepressant Use is Associated with Increased Energy Intake and Similar Levels of Physical Activity. Nutrients, 7(11), 9662-9671. https://doi.org/10.3390/nu7115489