Assessment of Diet and Physical Activity in Paediatric Non-Alcoholic Fatty Liver Disease Patients: A United Kingdom Case Control Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Demographic and Anthropometric Data
2.3. Dietary Assessment
2.4. Physical Activity Assessment
2.5. Statistical Analysis
3. Results
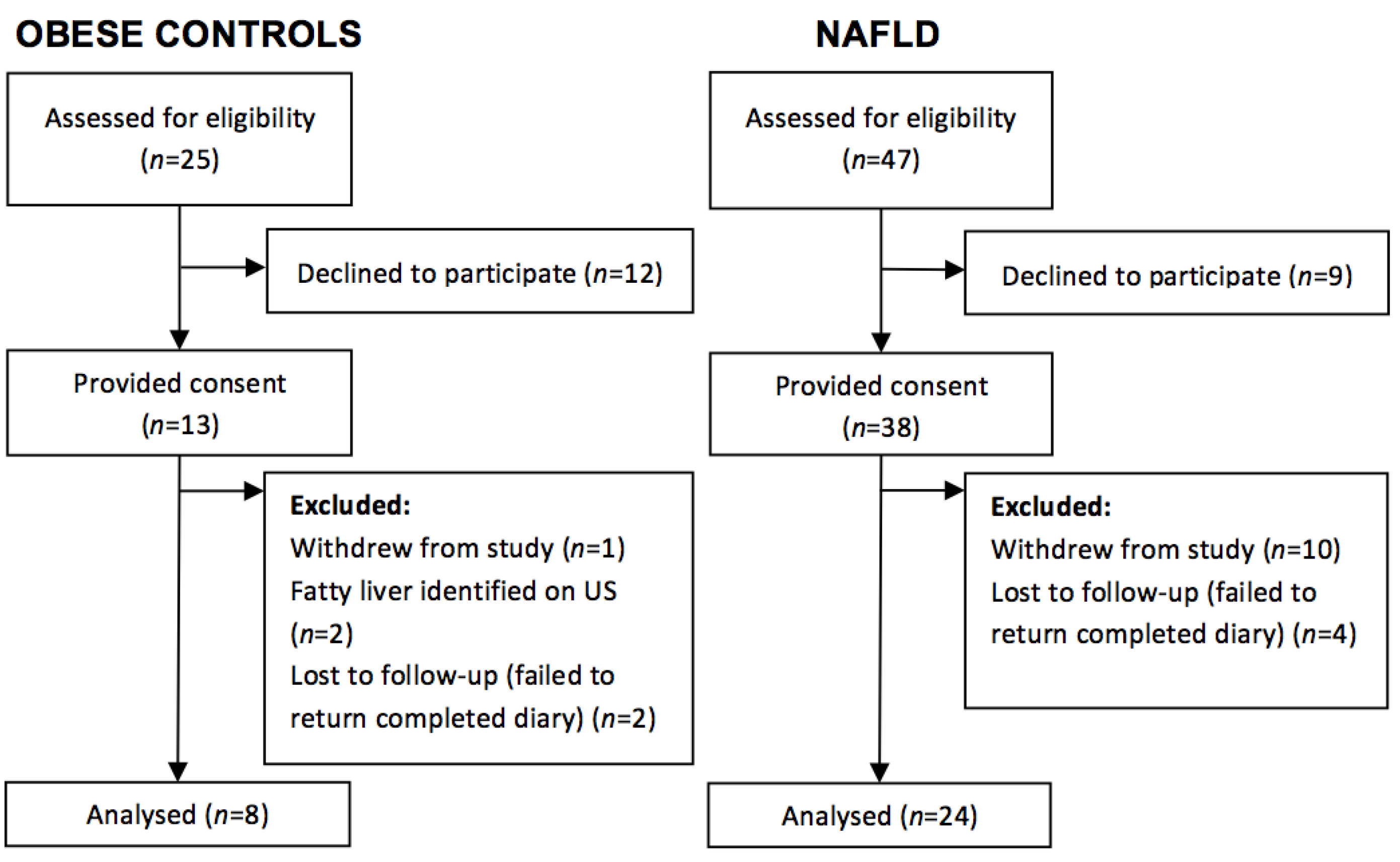
3.1. Study Population


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics 1 | Unit | NAFLD (n = 24) | Control (n = 8) | p-Value 2 |
|---|---|---|---|---|
| Gender | n (%) | Females 12 (50) | Females 5 (62.5) | 0.69 a |
| Males 12 (50) | Males 3 (37.5) | |||
| Ethnicity | n (%) | Black British 0 (0) | Black British 6 (75) | <0.001 a |
| White 19 (79) | White 2 (25) | |||
| Asian 5 (21) | Asian 0 (0) | |||
| Weight classification | n (%) | Healthy Weight Range 1 (4) | Health Weight Range 0 (0) | 0.99 a |
| Overweight 4 (17) | Overweight 1 (12.5) | |||
| Obese6 (25) | Obese 2 (25) | |||
| Extremely Obese 13 (54) | Extremely Obese 5 (62.5) | |||
| Age | years | 13.5 (12.0,15.0) | 12.0 (9.5,16.5) | 0.59 |
| Weight | kg | 83.3 (71.2,105.0) | 86.4 (77.2,136.5) | 0.27 |
| Height | cm | 163.0 (159.1,170.9) | 161.6 (148.1,173.7) | 0.61 |
| BMI | kg/m2 | 31.0 (27.1,36.5) | 38.4 (30.8,44.1) | 0.05 |
| BMI centile | - | 99.3 (98.0,99.6) | 99.6 (98.0,99.6) | 0.002 |
| BMI z-score | - | 2.1 (1.9,2.3) | 2.6 (2.4,2.7) | 0.006 |
| Waist circumference | cm | 101.0 (97.5,112.0) | 113.0 (95.0,133.0) | 0.31 |
| Triceps skinfold | mm | 30.5 (23.6,34.5) | 37.0 (32.2,43.6) | 0.08 |
| MUAC | cm | 32.0 (30.0,36.4) | 34.5 (29.1,34.5) | 0.62 |
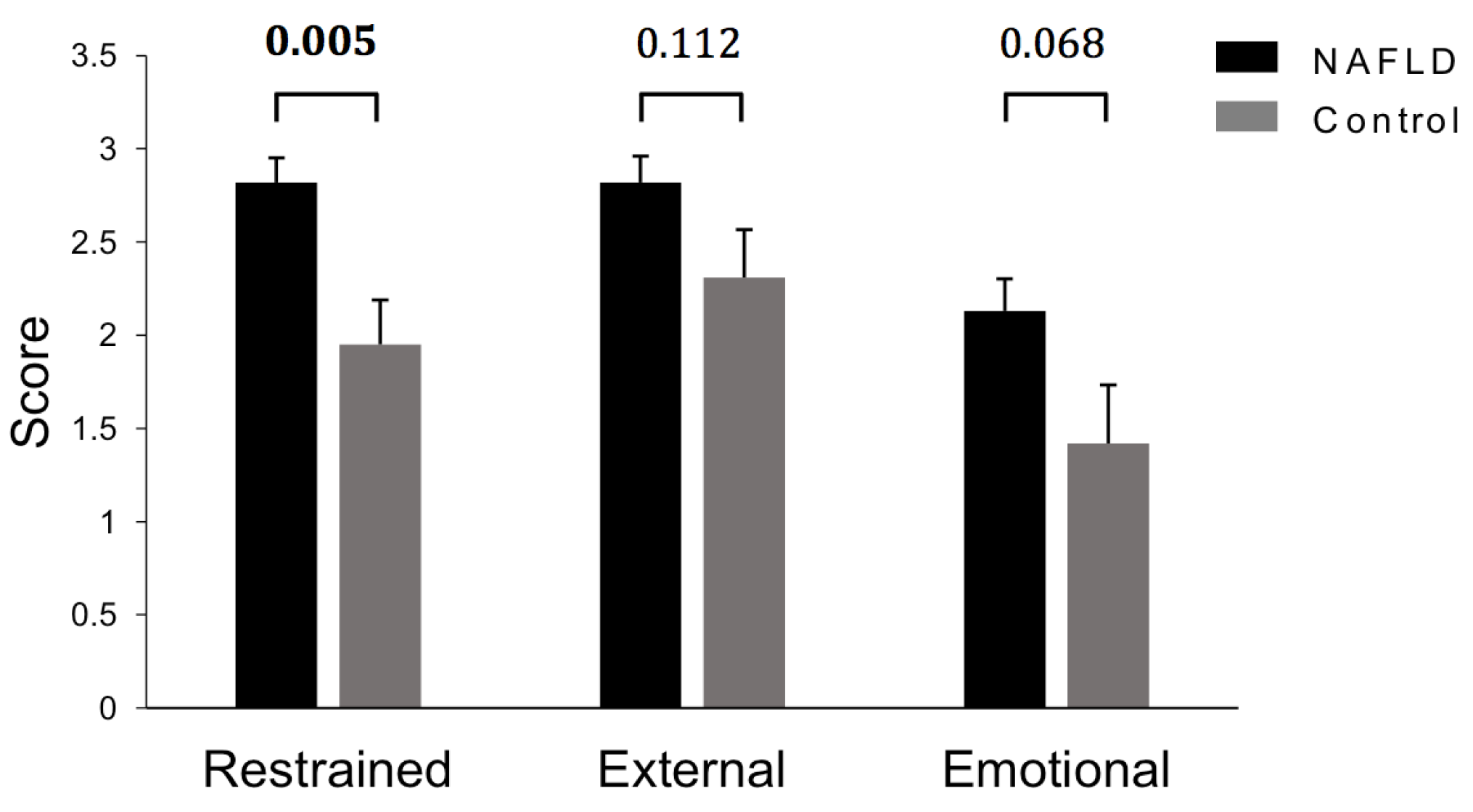
3.2. Dietary Intakes
| Nutritional Intake as per 7-Day Food Diary | Nutritional Intake as per 24-h Recall | |||||
|---|---|---|---|---|---|---|
| Nutrient 1 | NAFLD (n = 24) | Control (n = 8) | p-Value 2 | NAFLD (n = 24) | Control (n = 7) | p-Value 2 |
| Intakes of Nutrients Expressed as % DRV | ||||||
| Energy (%) | 77.4 (67.0,101.2) | 86.0 (74.4,114.1) | 0.41 | 84.7 (56.3,101.7) | 52.1 (43.6,93.6) | 0.10 |
| Protein (%) | 153.6 (120.2,199.5) | 169.2 (146.7,233.5) | 0.26 | 148.6 (113.8,215.4) | 104.9 (59.4,129.1) | 0.02 |
| Fat (%) | 82.7 (50.1,105.6) | 91.7 (67.1,118.4) | 0.28 | 77.0 (47.3,105.0) | 60.7 (39.8,66.5) | 0.13 |
| SFA (%) | 97.4 (50.3,127.2) | 108.3 (85.7,139.4) | 0.36 | 93.6 (56.7,138.5) | 61.5 (35.7,73.2) | 0.05 |
| MUFA (%) | 79.5 (40.6,92.7) | 89.7 (58.5,107.5) | 0.30 | 61.9 (40.7,102.5) | 53.0 (44.1,60.6) | 0.34 |
| PUFA (%) | 67.0 (46.6,84.7) | 82.0 (51.4,118.5) | 0.34 | 44.0 (33.4,93.4) | 57.9 (56.0,83.3) | 0.17 |
| Carbohydrate (%) | 73.0 (56.0,95.2) | 87.3 (65.4,95.3) | 0.51 | 60.2 (44.8,85.2) | 51.0 (39.3,83.4) | 0.44 |
| Sodium (%) | 156.3 (110.9,201.4) | 167.9 (106.2,199.3) | 0.86 | 154.1 (91.2,232.0) | 109.8 (86.1,131.1) | 0.16 |
| Potassium (%) | 75.9 (50.5,90.8) | 75.8 (63.2,97.7) | 0.32 | 73.3 (51.9,97.23) | 52.5 (45.3,78.7) | 0.08 |
| Calcium (%) | 81.5 (51.1,114.6) | 79.1 (72.5,106.3) | 0.79 | 74.0 (32.9,110.8) | 57.8 (43.7,77.6) | 0.48 |
| Iron (%) | 61.4 (48.5,89.7) | 72.5 (59.8,91.4) | 0.40 | 63.0 (44.5,79.4) | 43.4 (39.3,49.1) | 0.05 |
| Copper (%) | 100.5 (78.2,148.2) | 114.1 (99.7,114.1) | 0.41 | 89.4 (62.5,153.9) | 58.8 (52.0,75.0) | 0.04 |
| Zinc (%) | 78.5 (61.0,118.3) | 84.4 (78.4,112.9) | 0.43 | 62.4 (51.4,103.7) | 34.3 (33.3,56.6) | 0.01 |
| Vitamin E (%) | 101.0 (63.7,147.5) | 120.4 (86.0,186.2) | 0.43 | 67.5 (40.6,116.1) | 109.6 (84.2,155.4) | 0.30 |
| Vitamin B12 (%) | 258.3 (167.7,330.5) | 250.0 (139.3,545.4) | 0.76 | 185.0 (115.3,489.2) | 127.5 (55.3,190.0) | 0.09 |
| Folate (%) | 88.0 (60.6,116.2) | 91.6 (81.3,100.8) | 0.60 | 67.7 (48.2,95.5) | 50.6 (46.5,77.0) | 0.32 |
| Vitamin C (%) | 187.1 (77.2,302.0) | 211.2 (151.6,312.4) | 0.43 | 181.0 (115.5,331.4) | 82.5 (55.0,260.0) | 0.19 |
| Intakes of Nutrients Expressed as Absolute Intake | ||||||
| Starch (g) | 119.4 (84.7,158.2) | 127.4 (101.7,137.6) | 0.83 | 105.4 (80.3,136.9) | 107.2 (52.3,148.2) | 0.67 |
| Sugar (g) | 87.5 (49.5,107.1) | 93.0 (82.2,102.9) | 0.49 | 63.5 (44.9,125.0) | 49.9 (22.8,80.1) | 0.24 |
| NMES (g) | 15.6 (5.1,25.0) | 20.8 (11.4,28.7) | 0.46 | 16.0 (2.0,36.6) | 9.8 (0.0,21.4) | 0.32 |
| Fructose (g) | 12.7 (8.9,18.4) | 16.7 (10.9,19.4) | 0.62 | 12.5 (6.3,20.2) | 9.1 (2.1,19.4) | 0.38 |
| NSP (g) | 10.7 (8.2,13.1) | 10.1 (6.3,12.3) | 0.41 | 8.7 (7.0,11.3) | 4.1 (4.0,10.9) | 0.14 |
| Carotene (g) | 1.9 (0.7,3.1) | 3.0 (0.6,5.8) | 0.32 | 1.0 (0.2,2.3) | 0.4 (0.04,1.3) | 0.22 |
| Vitamin D (µg) | 1.7 (1.3,2.2) | 3.5 (1.0,4.4) | 0.32 | 1.8 (1.2,3.6) | 1.9 (0.3,2.9) | 0.45 |
| Omega-3 Fatty Acids (g) | 0.5 (0.3,0.9) | 0.5 (0.15,1.4) | 0.91 | 0.5 (0.2,0.8) | 0.3 (0.2,0.4) | 0.59 |
| Nutrients Contributing to Energy Intake 1 | Recommended Daily Allowance (Expressed as Percentage (%) Total Energy Intake) | NAFLD (n = 24) | Control (n = 8) | p-Value 2 |
|---|---|---|---|---|
| Total Fat | <35 | 33.1 (28.2,38.6) | 34.1 (32.6,36.6) | 0.69 |
| SFA | <11 | 11.7 (9.6,13.7) | 12.4 (11.4,13.2) | 0.31 |
| MUFA | 13 | 10.4 (8.8,13.6) | 11.9 (8.7,12.7) | 0.68 |
| PUFA | 6.5 | 4.9 (4.2,6.2) | 4.9 (4.2,6.8) | 0.88 |

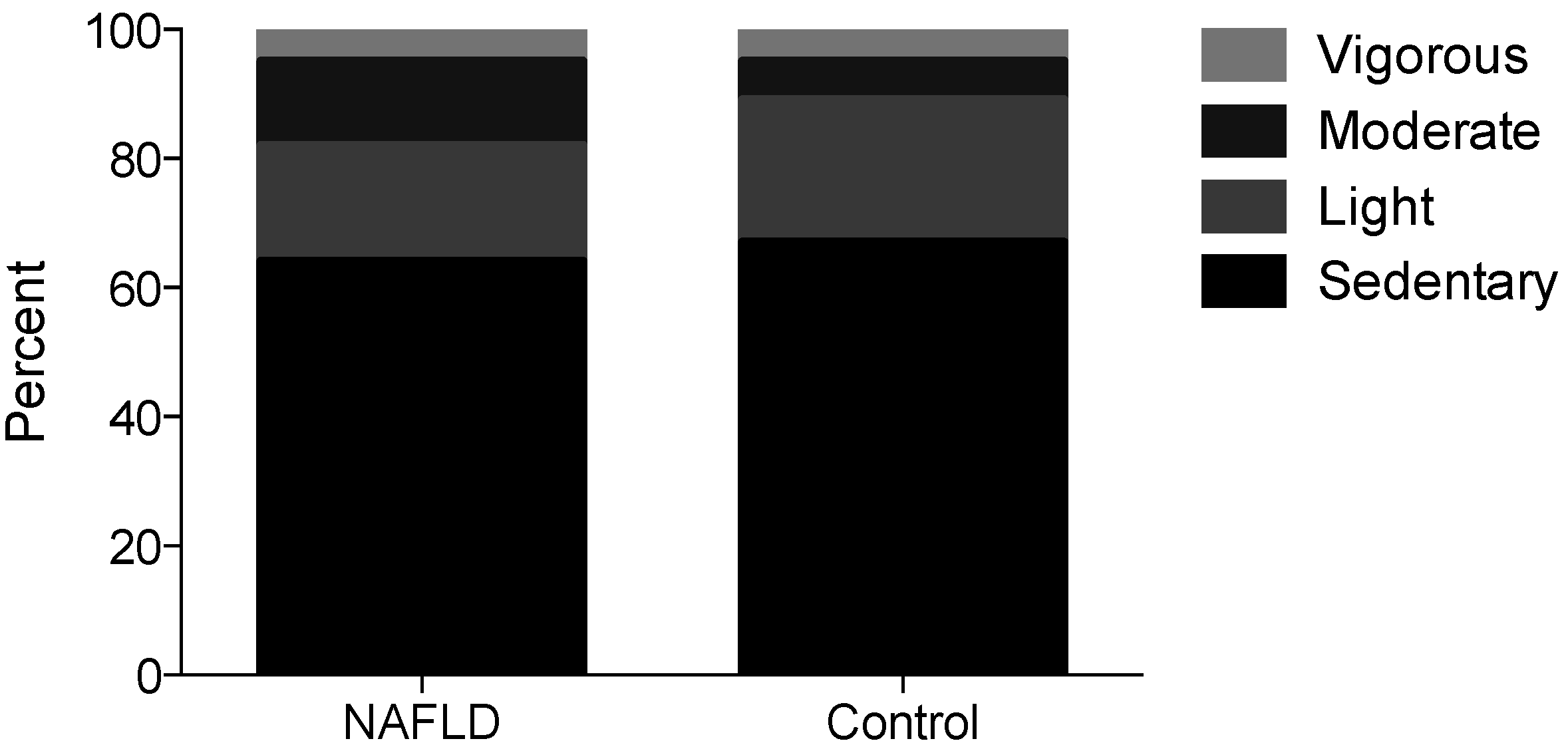
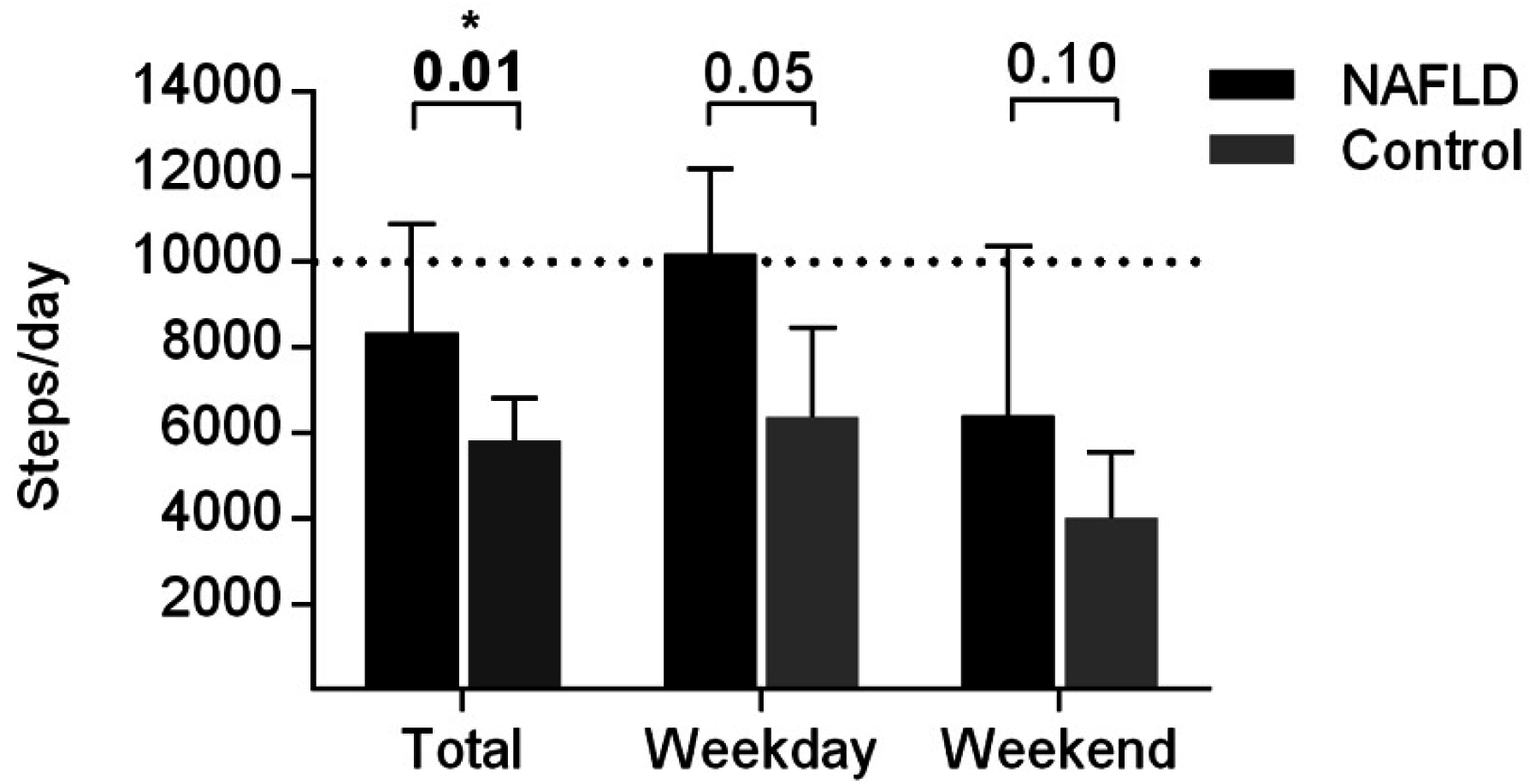
3.3. Physical Activity Levels
| Physical Activity Levels 1 (% per Day) | NAFLD (n = 22–24) | Control (n = 8) | p-Value 2 | |
|---|---|---|---|---|
| Sedentary (MET 1.0–1.5) | 7-day Average | 25 (16,32) | 20 (13,28) | 0.43 |
| Weekday Average | 22 (16,30) | 23 (16,31) | 0.95 | |
| Weekend Average | 29 (6,36) | 16 (10,22) | 0.22 | |
| Light (MET 1.6–2.9) | 7-day Average | 18 (9,23) | 13 (5,26) | 0.73 |
| Weekday Average | 25 (11,28) | 16 (6,31) | 0.41 | |
| Weekend Average | 6 (1,14) | 8 (3,13) | 0.71 | |
| Moderate (MET 3.0–5.9) | 7-day Average | 5 (3,7) | 3 (3,4) | 0.31 |
| Weekday Average | 5 (3,7) | 2 (1,4) | 0.06 | |
| Weekend Average | 4 (1,8) | 7 (5,11) | 0.13 | |
| Vigorous (MET > 6) | 7-day Average | 2 (0,3) | 1 (0,2) | 0.28 |
| Weekday Average | 2 (0,4) | 1 (0,2) | 0.19 | |
| Weekend Average | 0 (0,3) | 0 (0,1) | 0.48 | |
| Sleep (MET 0.9) | 7-day Average | 40 (38,43) | 42 (38,46) | 0.33 |
| Weekday Average | 39 (36,42) | 41 (37,41) | 0.32 | |
| Weekend Average | 44 (42,46) | 45 (39,45) | 0.62 | |
| Unaccounted | 7-day Average | 7 (7,22) | 19 (5,32) | 0.15 |
| Weekday Average | 5 (5,10) | 22 (5,30) | 0.08 | |
| Weekend Average | 6 (0,21) | 20 (9,28) | 0.16 | |


4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Moore, J.B. Non-alcoholic fatty liver disease: The hepatic consequence of obesity and the metabolic syndrome. Proc. Nutr. Soc. 2010, 69, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Giorgio, V.; Prono, F.; Graziano, F.; Nobili, V. Pediatric non alcoholic fatty liver disease: Old and new concepts on development, progression, metabolic insight and potential treatment targets. BMC Pediatr. 2013, 13, 40. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.; Sirlin, C.B.; Schwimmer, J.B.; Lavine, J.E. Advances in pediatric nonalcoholic fatty liver disease. Hepatology 2009, 50, 1282–1293. [Google Scholar] [CrossRef] [PubMed]
- Schwimmer, J.B.; Deutsch, R.; Kahen, T.; Lavine, J.E.; Stanley, C.; Behling, C. Prevalence of fatty liver in children and adolescents. Pediatrics 2006, 118, 1388–1393. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Diehl, A.M.; Brunt, E.M.; Cusi, K.; Charlton, M.; Sanyal, A.J. The Diagnosis and Management of Non-alcoholic Fatty Liver Disease: Practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Am. J. Gastroenterol. 2012, 107, 811–826. [Google Scholar] [CrossRef] [PubMed]
- Nascimbeni, F.; Pais, R.; Bellentani, S.; Day, C.P.; Ratziu, V.; Loria, P.; Lonardo, A. From NAFLD in clinical practice to answers from guidelines. J. Hepatol. 2013, 59, 859–871. [Google Scholar] [CrossRef] [PubMed]
- Green, C.J.; Hodson, L. The influence of dietary fat on liver fat accumulation. Nutrients 2014, 6, 5018–5033. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.B.; Gunn, P.J.; Fielding, B.A. The role of dietary sugars and de novo lipogenesis in non-alcoholic fatty liver disease. Nutrients 2014, 6, 5679–5703. [Google Scholar] [CrossRef] [PubMed]
- Eliades, M.; Spyrou, E.; Agrawal, N.; Lazo, M.; Brancati, F.L.; Potter, J.J.; Koteish, A.A.; Clark, J.M.; Guallar, E.; Hernaez, R. Meta-analysis: Vitamin D and non-alcoholic fatty liver disease. Aliment. Pharmacol. Ther. 2013, 38, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Black, L.J.; Jacoby, P.; Ping-Delfos, S.W.C.; Mori, T.A.; Beilin, L.J.; Olynyk, J.K.; Ayonrinde, O.T.; Huang, R.C.; Holt, P.G.; Hart, P.H.; et al. Low serum 25-hydroxyvitamin D concentrations associate with non-alcoholic fatty liver disease in adolescents independent of adiposity. J. Gastroenterol. Hepatol. 2014, 29, 1215–1222. [Google Scholar] [CrossRef] [PubMed]
- Nobili, V.; Giorgio, V.; Liccardo, D.; Bedogni, G.; Morino, G.; Alisi, A.; Cianfarani, S. Vitamin D levels and liver histological alterations in children with nonalcoholic fatty liver disease. Eur. J. Endocrinol. 2014, 170, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Gerber, L.; Otgonsuren, M.; Mishra, A.; Escheik, C.; Birerdinc, A.; Stepanova, M.; Younossi, Z.M. Non-alcoholic fatty liver disease (NAFLD) is associated with low level of physical activity: A population-based study. Aliment. Pharmacol. Ther. 2012, 36, 772–781. [Google Scholar] [CrossRef] [PubMed]
- Hallsworth, K.; Thoma, C.; Moore, S.; Ploetz, T.; Anstee, Q.M.; Taylor, R.; Day, C.P.; Trenell, M.I. Non-alcoholic fatty liver disease is associated with higher levels of objectively measured sedentary behaviour and lower levels of physical activity than matched healthy controls. Frontline Gastroenterol. 2014, 6, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Zelber-Sagi, S.; Nitzan-Kaluski, D.; Goldsmith, R.; Webb, M.; Zvibel, I.; Goldiner, I.; Blendis, L.; Halpern, Z.; Oren, R. Role of leisure-time physical activity in nonalcoholic fatty liver disease: A population-based study. Hepatology 2008, 48, 1791–1798. [Google Scholar] [CrossRef] [PubMed]
- Mager, D.R.; Patterson, C.; So, S.; Rogenstein, C.D.; Wykes, L.J.; Roberts, E.A. Dietary and physical activity patterns in children with fatty liver. Eur. J. Clin. Nutr. 2010, 64, 628–635. [Google Scholar] [CrossRef] [PubMed]
- Hattar, L.N. Physical activity and nutrition attitudes in obese Hispanic children with non-alcoholic steatohepatitis. World J. Gastroenterol. 2011, 17, 4396. [Google Scholar] [CrossRef] [PubMed]
- Health and Social Care Information Center. Ethnic Category Code. Available online: http://www.datadictionary.nhs.uk/data_dictionary/attributes/e/end/ethnic_category_code_de.asp?shownav = 1 (accessed on 8 October 2015).
- Royal College of Paediatrics and Child Health. School Age Charts and Resources. Available online: http://www.rcpch.ac.uk/child-health/research-projects/uk-who-growth-charts/uk-growth-chart-resources-2–18-years/school-age (accessed on 8 October 2015).
- The Children’s Hospital of Philadelphia. Paediatric Z-Score Calculator. Available online: http://stokes.chop.edu/web/zscore/ (accessed on 8 October 2015).
- Public Health England. Measuring and Interpreting BMI in Children. Available online: http://www.noo.org.uk/NOO_about_obesity/measurement/children (accessed on 8 October 2015).
- World Health Organisation. Waist Circumference and Waist–Hip Ratio. Report of a WHO Expert Consultation. Geneva, 8–11 December 2008. Available online: http://www.who.int/nutrition/publications/obesity/WHO_report_waistcircumference_and_waisthip_ratio/en/ (accessed on 8 October 2008).
- Center for Disease Control and Prevention. National Health and Nutrition Examination Survey (NHAMES) Anthropometry Procedures Manual. Available online: http://www.cdc.gov/nchs/data/nhanes/nhanes_07_08/manual_an.pdf (accessed on 8 October 2015).
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [PubMed]
- Great Britain Department of Health. Dietary Reference Values for Food Energy and Nutrients for the United Kingdom. Report of the Panel on Dietary Reference Values of the Committee on Medical Aspects of Food Policy; Great Britain Department of Health: London, UK, 1991.
- Goldberg, G.R.; Black, A.E.; Jebb, S.A.; Cole, T.J.; Murgatroyd, P.R.; Coward, W.A.; Prentice, A.M. Critical evaluation of energy intake data using fundamental principles of energy physiology: 1. Derivation of cut-off limits to identify under-recording. Eur. J. Clin. Nutr. 1991, 45, 569–581. [Google Scholar] [PubMed]
- Schofield, W.N. Predicting basal metabolic rate, new standards and review of previous work. Eur. J. Clin. Nutr. 1985, 39, 5–41. [Google Scholar]
- Van Strien, T.; Frijters, J.E.R.; Bergers, G.P.A.; Defares, P.B. The Dutch eating behavior questionnaire (DEBQ) for assessment of restrained, emotional, and external eating behavior. Int. J. Eat. Disorder 1986, 5, 295–315. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 Compendium of Physical Activities. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [PubMed]
- Corder, K.; van Sluijs, E.M.F.; Wright, A.; Whincup, P.; Wareham, N.J.; Ekelund, U. Is it possible to assess free-living physical activity and energy expenditure in young people by self-report? Am. J. Clin. Nutr. 2009, 89, 862–870. [Google Scholar] [CrossRef] [PubMed]
- Telford, A.; Salmon, J.; Jolley, D.; Crawford, D. Reliability and Validity of Physical Activity Questionnaires for Children: The Children’s Leisure Activities Study Survey (CLASS). Pediatr. Exerc. Sci. 2004, 16, 64–78. [Google Scholar]
- Department of Health, Physical Activity, Health Improvement and Protection. Start Active, Stay Active: A Report on Physical Activity from the Four Home Countries’ Chief Medical Officers. Available online: http://www.nhs.uk/Livewell/fitness/Documents/children-and-young-people-5–18-years.pdf (accessed on 8 October 2015).
- Adams, M.A.; Caparosa, S.; Thompson, S.; Norman, G.J. Translating Physical Activity Recommendations for Overweight Adolescents to Steps Per Day. Am. J. Prev. Med. 2009, 37, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Denzer, C.; Thiere, D.; Muche, R.; Koenig, W.; Mayer, H.; Kratzer, W.; Wabitsch, M. Gender-Specific Prevalences of Fatty Liver in Obese Children and Adolescents: Roles of Body Fat Distribution, Sex Steroids, and Insulin Resistance. J. Clin. Endocrinol. Metab. 2009, 94, 3872–3881. [Google Scholar] [CrossRef] [PubMed]
- Van der Poorten, D.; Milner, K.L.; Hui, J.; Hodge, A.; Trenell, M.I.; Kench, J.G.; London, R.; Peduto, T.; Chisholm, D.J.; George, J. Visceral fat: A key mediator of steatohepatitis in metabolic liver disease. Hepatology 2008, 48, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Browning, J.D.; Szczepaniak, L.S.; Dobbins, R.; Nuremberg, P.; Horton, J.D.; Cohen, J.C.; Grundy, S.M.; Hobbs, H.H. Prevalence of hepatic steatosis in an urban population in the United States: Impact of ethnicity. Hepatology 2004, 40, 1387–1395. [Google Scholar] [CrossRef] [PubMed]
- Romeo, S.; Kozlitina, J.; Xing, C.; Pertsemlidis, A.; Cox, D.; Pennacchio, L.A.; Boerwinkle, E.; Cohen, J.C.; Hobbs, H.H. Genetic variation in PNPLA3 confers susceptibility to nonalcoholic fatty liver disease. Nat. Genet. 2008, 40, 1461–1465. [Google Scholar] [CrossRef] [PubMed]
- Abdelmalek, M.F.; Suzuki, A.; Guy, C.; Unalp-Arida, A.; Colvin, R.; Johnson, R.J.; Diehl, A.M. Increased fructose consumption is associated with fibrosis severity in patients with nonalcoholic fatty liver disease. Hepatology 2010, 51, 1961–1971. [Google Scholar] [CrossRef] [PubMed]
- Thuy, S.; Ladurner, R.; Volynets, V.; Wagner, S.; Strahl, S.; Konigsrainer, A.; Maier, K.P.; Bischoff, S.C.; Bergheim, I. Nonalcoholic fatty liver disease in humans is associated with increased plasma endotoxin and plasminogen activator inhibitor 1 concentrations and with fructose intake. J. Nutr. 2008, 138, 1452–1455. [Google Scholar] [PubMed]
- Ouyang, X.; Cirillo, P.; Sautin, Y.; McCall, S.; Bruchette, J.L.; Diehl, A.M.; Johnson, R.J.; Abdelmalek, M.F. Fructose consumption as a risk factor for non-alcoholic fatty liver disease. J. Hepatol. 2008, 48, 993–999. [Google Scholar] [CrossRef] [PubMed]
- Chiu, S.; Sievenpiper, J.L.; de Souza, R.J.; Cozma, A.I.; Mirrahimi, A.; Carleton, A.J.; Ha, V.; di Buono, M.; Jenkins, A.L.; Leiter, L.A.; et al. Effect of fructose on markers of non-alcoholic fatty liver disease (NAFLD): A systematic review and meta-analysis of controlled feeding trials. Eur. J. Clin. Nutr. 2014, 68, 416–423. [Google Scholar] [CrossRef] [PubMed]
- Ryan, M.C.; Itsiopoulos, C.; Thodis, T.; Ward, G.; Trost, N.; Hofferberth, S.; O’Dea, K.; Desmond, P.V.; Johnson, N.A.; Wilson, A.M. The Mediterranean diet improves hepatic steatosis and insulin sensitivity in individuals with non-alcoholic fatty liver disease. J. Hepatol. 2013, 59, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Capanni, M.; Calella, F.; Biagini, M.R.; Genise, S.; Raimondi, L.; Bedogni, G.; Svegliati-Baroni, G.; Sofi, F.; Milani, S.; Abbate, R.; et al. Prolonged n-3 polyunsaturated fatty acid supplementation ameliorates hepatic steatosis in patients with non-alcoholic fatty liver disease: A pilot study. Aliment. Pharmacol. Ther. 2006, 23, 1143–1151. [Google Scholar] [CrossRef] [PubMed]
- Spadaro, L.; Magliocco, O.; Spampinato, D.; Piro, S.; Oliveri, C.; Alagona, C.; Papa, G.; Rabuazzo, A.M.; Purrello, F. Effects of n-3 polyunsaturated fatty acids in subjects with nonalcoholic fatty liver disease. Dig. Liver. Dis. 2008, 40, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Scientific Advisory Committee on Nutrition. Draft Vitamin D and Health Report. Scientific Consultation: 22 July to 23 September 2015. Available online: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/447402/Draft_SACN_Vitamin_D_and_Health_Report.pdf (accessed on 8 October 2015).
- Mendez, M.A.; Popkin, B.M.; Buckland, G.; Schroder, H.; Amiano, P.; Barricarte, A.; Huerta, J.M.; Quiros, J.R.; Sanchez, M.J.; Gonzalez, C.A. Alternative Methods of Accounting for Underreporting and Overreporting When Measuring Dietary Intake-Obesity Relations. Am. J. Epidemiol. 2011, 173, 448–458. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.O.; Johnson, R.K.; Lindquist, C.; Birch, L.L.; Goran, M.I. Influence of Body Composition on the Accuracy of Reported Energy Intake in Children. Obes. Res. 2000, 8, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Lu, A.S.; Baranowski, J.; Islam, N.; Baranowski, T. How to engage children in self-administered dietary assessment programmes. J. Hum. Nutr. Diet. 2012, 27, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Birch, L.L.; Fisher, J.O. Development of eating behaviors among children and adolescents. Pediatrics 1998, 101, 539–549. [Google Scholar] [PubMed]
- Whitsett, M.; VanWagner, L.B. Physical activity as a treatment of non-alcoholic fatty liver disease: A systematic review. World J. Hepatol. 2015, 7, 2041–2052. [Google Scholar] [CrossRef] [PubMed]
- Murtagh, J.; Dixey, R.; Rudolf, M. A qualitative investigation into the levers and barriers to weight loss in children: Opinions of obese children. Arch. Dis. Child. 2006, 91, 920–923. [Google Scholar] [CrossRef] [PubMed]
- Round Ethnic Group Population Projections. Available online: http://data.london.gov.uk/dataset/2013-round-ethnic-group-population-projections/resource/3ce5e98c-54ea-4ac5-8824-0871314fa363 (accessed on 8 October 2015).
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gibson, P.S.; Lang, S.; Gilbert, M.; Kamat, D.; Bansal, S.; Ford-Adams, M.E.; Desai, A.P.; Dhawan, A.; Fitzpatrick, E.; Moore, J.B.; et al. Assessment of Diet and Physical Activity in Paediatric Non-Alcoholic Fatty Liver Disease Patients: A United Kingdom Case Control Study. Nutrients 2015, 7, 9721-9733. https://doi.org/10.3390/nu7125494
Gibson PS, Lang S, Gilbert M, Kamat D, Bansal S, Ford-Adams ME, Desai AP, Dhawan A, Fitzpatrick E, Moore JB, et al. Assessment of Diet and Physical Activity in Paediatric Non-Alcoholic Fatty Liver Disease Patients: A United Kingdom Case Control Study. Nutrients. 2015; 7(12):9721-9733. https://doi.org/10.3390/nu7125494
Chicago/Turabian StyleGibson, Philippa S., Sarah Lang, Marianne Gilbert, Deepa Kamat, Sanjay Bansal, Martha E. Ford-Adams, Ashish P. Desai, Anil Dhawan, Emer Fitzpatrick, J. Bernadette Moore, and et al. 2015. "Assessment of Diet and Physical Activity in Paediatric Non-Alcoholic Fatty Liver Disease Patients: A United Kingdom Case Control Study" Nutrients 7, no. 12: 9721-9733. https://doi.org/10.3390/nu7125494
APA StyleGibson, P. S., Lang, S., Gilbert, M., Kamat, D., Bansal, S., Ford-Adams, M. E., Desai, A. P., Dhawan, A., Fitzpatrick, E., Moore, J. B., & Hart, K. H. (2015). Assessment of Diet and Physical Activity in Paediatric Non-Alcoholic Fatty Liver Disease Patients: A United Kingdom Case Control Study. Nutrients, 7(12), 9721-9733. https://doi.org/10.3390/nu7125494