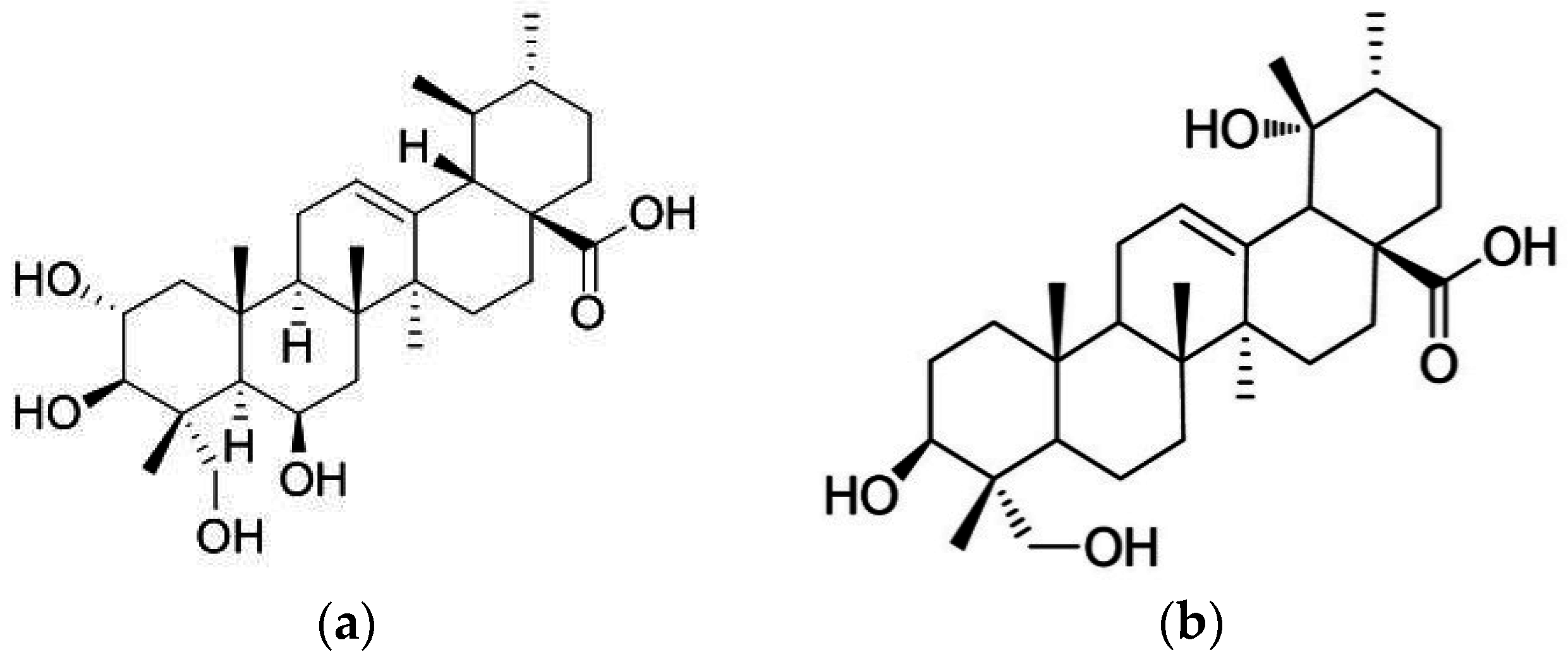
Anti-Diabetic Effects of Madecassic Acid and Rotundic Acid

Abstract
:1. Introduction

2. Materials and Methods
2.1. Materials
2.2. Animals and Diets
2.3. Experimental Design
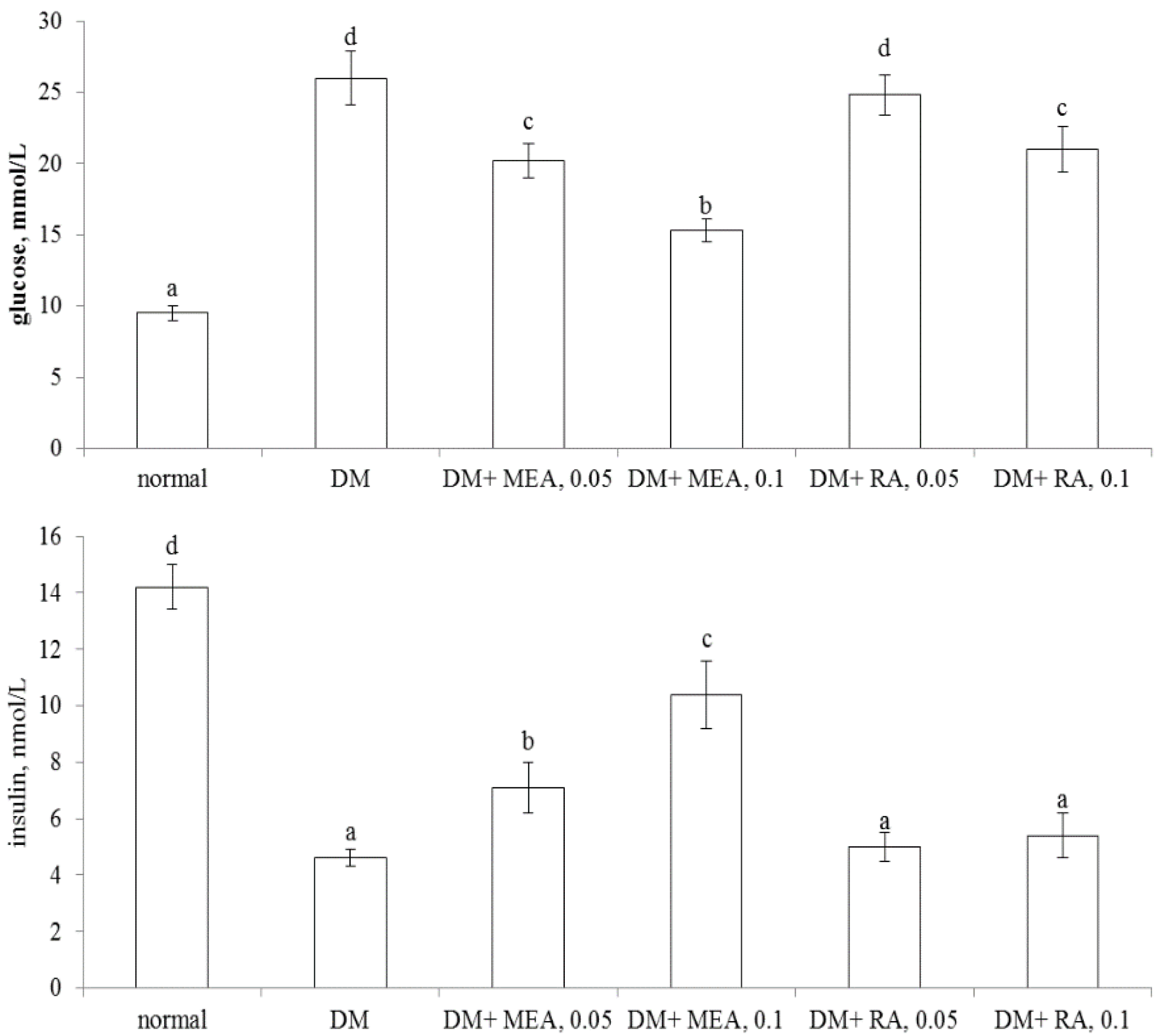
2.4. Blood Glucose and Insulin Analyses
2.5. Measurement of Coagulation and Anti-Coagulation Factors
2.6. Determination of Triglyceride (TG) and Cholesterol
2.7. Assay of Oxidative and Anti-Oxidative Status
2.8. Quantification of Inflammatory Cytokines
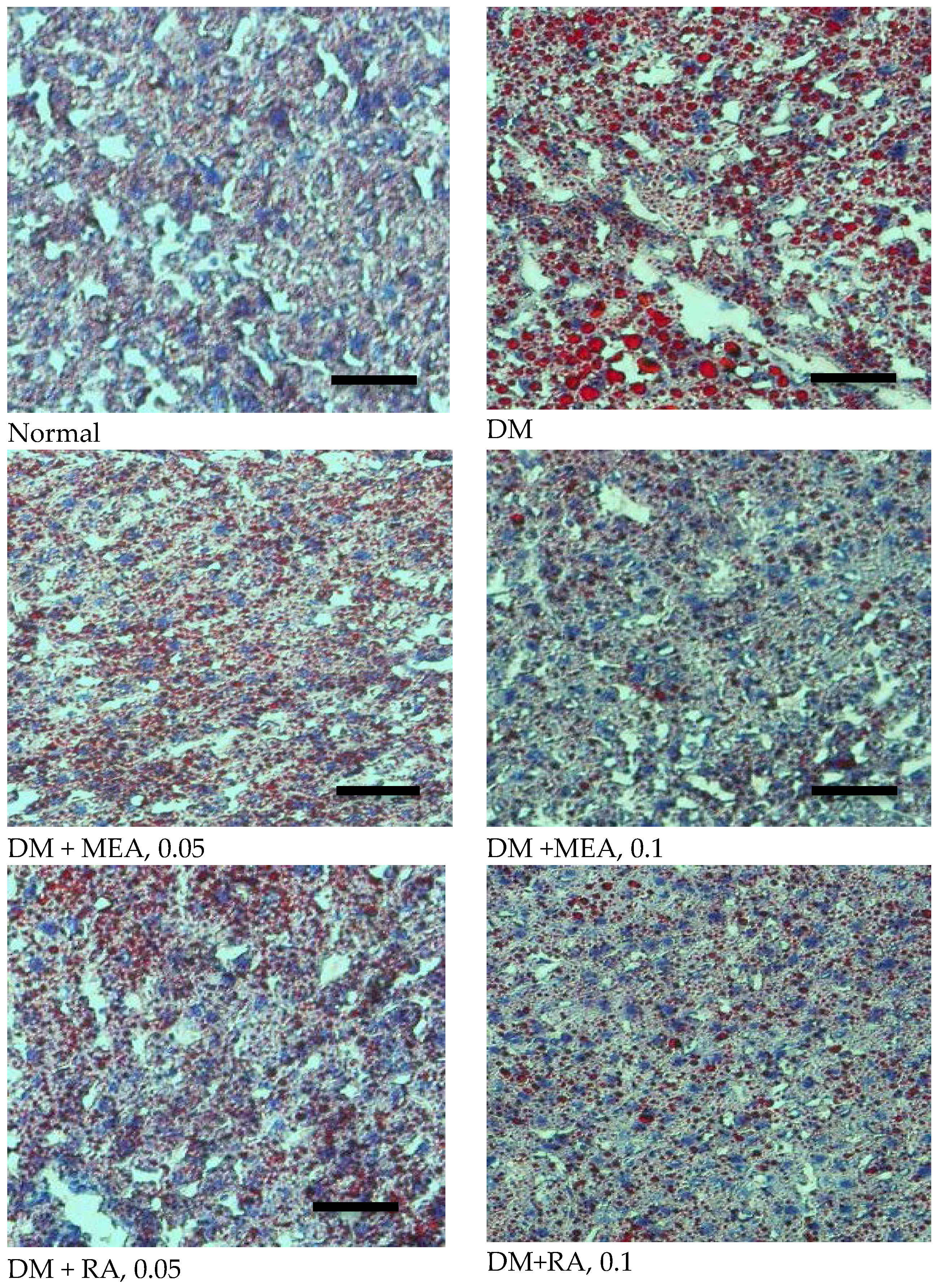
2.9. Histological Analyses
2.10. Statistical Analyses
3. Results
3.1. MEA Improved Glycemic Control and Hemostatic Imbalance

{kind=link}
{kind=link}
{kind=link}
| Normal | DM | DM + MEA, 0.05 | DM + MEA, 0.1 | DM + RA, 0.05 | DM + RA, 0.1 | |
|---|---|---|---|---|---|---|
| WI | 2.2 ± 0.6 a | 6.8 ± 1.4 d | 5.7 ± 1.0 c | 3.9 ± 0.8 b | 6.4 ± 0.7 d | 6.2 ± 0.5 d |
| FI | 2.4 ± 0.9 a | 7.0 ± 1.3 d | 5.2 ± 1.1 c | 3.6 ± 0.5 b | 6.5 ± 0.9 d | 5.5 ± 0.6 c |
| BW | 29.5 ± 1.3d | 12.2 ± 1.0 a | 15.1 ± 0.8 b | 19.4 ± 1.2 c | 13.1 ± 1.3 a | 14.7 ± 0.7 b |
| HW | 275 ± 11 a | 269 ± 9 a | 270 ± 6 a | 281 ± 10 a | 272 ± 12 a | 277 ± 8 a |
| LW | 1466 ± 18 a | 1452 ± 23 a | 1455 ± 19 a | 1460 ± 15 a | 1456 ± 18 a | 1462 ± 13 a |
| KW | 453 ± 11 a | 448 ± 14 a | 445 ±10 a | 457 ± 16 a | 442 ± 8 a | 450 ± 12 a |

| Normal | DM | DM + MEA, 0.05 | DM + MEA, 0.1 | DM + RA, 0.05 | DM + RA, 0.1 | |
|---|---|---|---|---|---|---|
| PAI-1 | 7.5 ± 0.8 a | 17.9 ± 1.1 d | 13.9 ± 1.0 c | 10.4 ± 0.9 b | 17.5 ± 1.5 d | 16.9 ± 1.3 d |
| Fibrinogen | 2.18 ± 0.08 a | 4.81 ± 0.22 d | 4.03 ± 0.12 c | 3.24 ± 0.13 b | 4.72 ± 0.09 d | 4.68 ± 0.17 d |
| AT-III | 129 ± 9 c | 70 ± 7 a | 92 ± 5 b | 117 ± 4 c | 72 ± 3 a | 75 ± 6 a |
| Protein C | 101 ± 8 c | 66 ± 5 a | 81 ± 3 b | 96 ± 6 c | 68± 4 a | 70 ± 7 a |
| Normal | DM | DM + MEA, 0.05 | DM + MEA, 0.1 | DM + RA, 0.05 | DM + RA, 0.1 | |
|---|---|---|---|---|---|---|
| Plasma | ||||||
| TG | 2.06 ± 0.14 a | 3.98 ± 0.27 d | 3.21 ± 0.13 c | 2.67 ± 0.15 b | 3.26 ± 0.1 c | 2.58 ± 0.17 b |
| TC | 1.31 ± 0.1 a | 2.69 ± 0.13 d | 2.13 ± 0.12 c | 1.76 ± 0.11 b | 2.21 ± 0.08 c | 1.82 ± 0.16 b |
| Liver | ||||||
| TG | 25.1 ± 2.3 a | 52.3 ±4.2 e | 41.4 ± 2.2 c | 34.7 ± 1.4 b | 46.5 ± 2.0 d | 40.3 ± 3.1 c |
| TC | 3.46 ±0.18a | 5.62 ± 0.31 d | 4.93 ± 0.22 c | 4.18 ± 0.16 b | 5.05 ± 0.18 c | 4.87 ± 0.19 c |

3.2. MEA and RA Lowered TG and TC Levles
3.3. MEA Attenuated Oxidative and Inflammatory Stress in the Heart and Kidneys
| Normal | DM | DM + MEA, 0.05 | DM + MEA, 0.1 | DM + RA, 0.05 | DM + RA, 0.1 | |
|---|---|---|---|---|---|---|
| Heart | ||||||
| ROS | 0.19 ± 0.06 a | 1.45 ± 0.12 d | 1.14 ±0.07 c | 0.73 ± 0.1 b | 1.37 ± 0.05 d | 1.07 ± 0.08 c |
| GSSG | 0.21 ± 0.05 a | 1.09 ± 0.13 d | 0.85 ± 0.09 c | 0.49±0.11 b | 1.02 ± 0.07 d | 0.98 ± 0.06 d |
| GSH | 19.7 ± 1.3 d | 11.6 ± 0.8 a | 13.7 ± 0.5 b | 17.0 ± 0.4 c | 12.0 ± 0.9 a | 12.3 ± 0.8 a |
| GPX | 33.8 ± 1.0 c | 18.4 ± 1.5 a | 19.0 ± 1.2 a | 24.8 ± 1.1 b | 18.1 ± 1.5 a | 19.2 ± 1.2 a |
| GR | 31.4 ± 0.9 d | 20.8 ± 1.4 a | 24.2 ± 0.8 b | 27.8 ± 1.1 c | 21.0 ± 1.3 a | 21.4 ± 0.9 a |
| Catalase | 29.1 ± 1.4 d | 14.8 ± 1.1 a | 18.7 ± 0.6 b | 23.0 ± 1.3 c | 14.5 ± 0.9 a | 15.1 ± 1.0 a |
| Kidney | ||||||
| ROS | 0.22 ± 0.08 a | 1.28 ± 0.15 d | 0.93 ±0.08 c | 0.64 ± 0.06 b | 1.23 ± 0.13 d | 0.95 ± 0.1 c |
| GSSG | 0.18 ± 0.05 a | 1.17 ± 0.11 d | 0.82 ±0.1 c | 0.58 ± 0.05 b | 1.15 ± 0.07 d | 1.04 ± 0.07 d |
| GSH | 14.2 ± 1.1 d | 5.5 ± 0.6 a | 7.6 ± 0.4 b | 10.7 ± 0.8 c | 6.0 ± 0.7 a | 6.3 ± 0.5 a |
| GPX | 21.8 ± 1.7 c | 14.0 ± 0.9 a | 14.8 ± 1.3 a | 18.0 ± 1.2 b | 14.4 ± 1.1 a | 14.7 ± 0.9 a |
| GR | 22.4 ± 1.0 d | 11.4 ± 1.1 a | 13.7 ± 0.9 b | 18.9 ± 1.4 c | 12.0 ± 0.6 a | 11.8 ± 1.3 a |
| Catalase | 20.4 ± 1.2 d | 12.8 ± 0.7 a | 14.8 ± 1.1 b | 17.8 ± 1.1 c | 13.1 ± 1.0 a | 15.2 ± 0.8 b |
| Normal | DM | DM + MEA, 0.05 | DM + MEA, 0.1 | DM + RA, 0.05 | DM + RA, 0.1 | |
|---|---|---|---|---|---|---|
| Heart | ||||||
| IL-1β | 18 ± 4 a | 221 ± 24 d | 178 ± 16 c | 120 ± 14 b | 215 ± 10 d | 174 ± 9 c |
| IL-6 | 12 ± 2 a | 275 ± 28 d | 200 ± 20 c | 119 ± 14 b | 266 ± 22 d | 205 ± 18 c |
| TNF-α | 20 ± 3 a | 301 ± 16 d | 231 ± 19 c | 156 ± 12 b | 296 ± 13 d | 223 ± 10 c |
| MCP-1 | 13 ± 4 a | 173 ± 12 d | 130 ± 8 c | 87 ± 11 b | 170 ± 14 d | 141 ± 7 c |
| Kidney | ||||||
| IL-1β | 15 ± 3 a | 243 ± 19 d | 198 ± 10 c | 120 ± 12 b | 238 ± 19 d | 202 ± 15 c |
| IL-6 | 18 ± 4 a | 238 ± 22 d | 162 ± 14 c | 95 ± 7 b | 229 ± 13 d | 175 ± 8 c |
| TNF-α | 17 ± 2 a | 280 ± 25 d | 209 ± 13 c | 129 ± 9 b | 271 ± 17 d | 213 ± 11 c |
| MCP-1 | 10 ± 3 a | 217 ± 18 d | 160 ± 12 c | 103 ± 6 b | 213 ± 10 d | 167 ± 7 c |
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Hashim, P.; Sidek, H.; Helan, M.H.; Sabery, A.; Palanisamy, U.D.; Ilham, M. Triterpene composition and bioactivities of Centella asiatica. Molecules 2011, 16, 1310–1322. [Google Scholar] [CrossRef] [PubMed]
- Cao, X.F.; Wang, J.S.; Wang, P.R.; Kong, L.Y. Triterpenes from the stem bark of Mitragyna diversifolia and their cytotoxic activity. Chin. J. Nat. Med. 2014, 12, 628–631. [Google Scholar] [CrossRef]
- Kim, N.C.; Desjardins, A.E.; Wu, C.D.; Kinghorn, A.D. Activity of triterpenoid glycosides from the root bark of Mussaenda macrophylla against two oral pathogens. J. Nat. Prod. 1999, 62, 1379–1384. [Google Scholar] [CrossRef] [PubMed]
- Won, J.H.; Shin, J.S.; Park, H.J.; Jung, H.J.; Koh, D.J.; Jo, B.G.; Lee, J.Y.; Yun, K.; Lee, K.T. Anti-inflammatory effects of madecassic acid via the suppression of NF-κB pathway in LPS-induced RAW 264.7 macrophage cells. Planta Med. 2010, 76, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Tabassum, R.; Vaibhav, K.; Shrivastava, P.; Khan, A.; Ejaz Ahmed, M.; Javed, H.; Islam, F.; Ahmad, S.; Saeed Siddiqui, M.; Safhi, M.M.; et al. Centella asiatica attenuates the neurobehavioral, neurochemical and histological changes in transient focal middle cerebral artery occlusion rats. Neurol. Sci. 2013, 34, 925–933. [Google Scholar] [CrossRef] [PubMed]
- Yin, M.C.; Lin, M.C.; Mong, M.C.; Lin, C.Y. Bioavailability, distribution, and antioxidative effects of selected triterpenes in mice. J. Agric. Food Chem. 2012, 60, 7697–7701. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhang, M.; Tao, Y.; Wang, G.; Xia, B. Madecassic acid inhibits the mouse colon cancer growth by inducing apoptosis and immunomodulation. J. BUON 2014, 19, 372–376. [Google Scholar] [PubMed]
- Thang, T.D.; Kuo, P.C.; Yu, C.S.; Shen, Y.C.; le Hoa, T.M.; Van Thanh, T.; Kuo, Y.H.; Yang, M.L.; Wu, T.S. Chemical constituents of the leaves of Glochidion obliquum and their bioactivity. Arch. Pharm. Res. 2011, 34, 383–389. [Google Scholar] [CrossRef] [PubMed]
- He, Y.F.; Nan, M.L.; Sun, J.M.; Meng, Z.J.; Yue, F.G.; Zhao, Q.C.; Yang, X.H.; Wang, H. Synthesis, characterization and cytotoxicity of new rotundic acid derivatives. Molecules 2012, 17, 1278–1291. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; He, Y.F.; Nan, M.L.; Sun, W.Y.; Hu, J.; Cui, A.; Li, F.; Wang, F. Novel rotundic acid derivatives: Synthesis, structural characterization and in vitro antitumor activity. Int. J. Mol. Med. 2013, 31, 353–360. [Google Scholar] [PubMed]
- Fava, S. Glycaemic control: A balancing act or a different approach? Curr. Diabetes Rev. 2014, 10, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Brownlee, M. Biochemistry and molecular cell biology of diabetic complications. Nature 2001, 414, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Drimal, J.; Knezl, V.; Navarova, J.; Nedelcevova, J.; Paulovicova, E.; Sotnikova, V.R.; Drimal, D. Role of inflammatory cytokines and chemoattractants in rat model of streptozotocin-induced diabetic heart failure. Endocr. Regul. 2008, 42, 129–135. [Google Scholar] [PubMed]
- Yamada, T.; Sato, A.; Nishimori, T.; Mitsuhashi, T.; Terao, A.; Sagai, H.; Komatsu, M.; Aizawa, T.; Hashizume, K. Importance of hypercoagulability over hyperglycemia for vascular complication in type 2 diabetes. Diabetes Res. Clin. Pract. 2000, 49, 23–31. [Google Scholar] [CrossRef]
- Urano, T.; Ihara, H.; Suzuki, Y.; Takada, Y.; Takada, A. Coagulation-associated enhancement of fibrinolytic activity via a neutralization of PAI-1 activity. Semin. Thromb. Hemost. 2000, 26, 39–42. [Google Scholar] [CrossRef] [PubMed]
- Asakawa, H.; Tokunaga, K.; Kawakami, F. Elevation of fibrinogen and thrombin-antithrombin III complex levels of type 2 diabetes mellitus patients with retinopathy and nephropathy. J. Diabet. Complicat. 2000, 14, 121–126. [Google Scholar] [CrossRef]
- Pastromas, S.; Terzi, A.B.; Tousoulis, D.; Koulouris, S. Postprandial lipemia: An under-recognized atherogenic factor in patients with diabetes mellitus. Int. J. Cardiol. 2008, 126, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Aso, Y.; Okumura, K.; Yoshida, N.; Tayama, K.; Kanda, T.; Kobayashi, I.; Takemura, Y.; Inukai, T. Plasma interleukin-6 is associated with coagulation in poorly controlled patients with Type 2 diabetes. Diabet. Med. 2003, 20, 930–934. [Google Scholar] [CrossRef] [PubMed]
- Martinovic, I.; Abegunewardene, N.; Seul, M.; Vosseler, M.; Horstick, G.; Buerke, M.; Darius, H.; Lindemann, S. Elevated monocyte chemoattractant protein-1 serum levels in patients at risk for coronary artery disease. Circulation J. 2005, 69, 1484–1489. [Google Scholar] [CrossRef]
- Folch, J.; Lees, M.; Sloane, G.E. A simple method for the isolation and purification of total lipids from animal tissues. J. Biol. Chem. 1957, 226, 497–509. [Google Scholar] [PubMed]
- Cesarone, M.R.; Incandela, L.; de Sanctis, M.T.; Belcaro, G.; Bavera, P.; Bucci, M.; Ippolito, E. Evaluation of treatment of diabetic microangiopathy with total triterpenic fraction of Centella asiatica: A clinical prospective randomized trial with a microcirculatory model. Angiology 2001, 52, S49–S54. [Google Scholar] [PubMed]
- Ceriello, A.; Giacomello, R.; Stel, G.; Motz, E.; Taboga, C.; Tonutti, L.; Pirisi, M.; Falleti, E.; Bartoli, E. Hyperglycemia-induced thrombin formation in diabetes. The possible role of oxidative stress. Diabetes 1995, 44, 924–928. [Google Scholar] [CrossRef] [PubMed]
- Polat, S.B.; Ugurlu, N.; Yulek, F.; Simavli, H.; Ersoy, R.; Cakir, B.; Erel, O. Evaluation of serum fibrinogen, plasminogen, α2-anti-plasmin, and plasminogen activator inhibitor levels (PAI) and their correlation with presence of retinopathy in patients with type 1 DM. J. Diabetes Res. 2014. [Google Scholar] [CrossRef] [PubMed]
- Griffin, J.H.; Zlokovic, B.V.; Mosnier, L.O. Activated protein C: Biased for translation. Blood 2015, 125, 2898–2907. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, S.; Chait, A. Hypertriglyceridemia secondary to obesity and diabetes. Biochim. Biophys. Acta 2012, 1821, 819–825. [Google Scholar] [CrossRef] [PubMed]
- Lambert, J.E.; Ryan, E.A.; Thomson, A.B.; Clandinin, M.T. De novoDe novo lipogenesis and cholesterol synthesis in humans with long-standing type 1 diabetes are comparable to non-diabetic individuals. PLoS ONE 2013. [Google Scholar] [CrossRef] [PubMed]
- Limaye, P.V.; Raghuram, N.; Sivakami, S. Oxidative stress and gene expression of antioxidant enzymes in the renal cortex of streptozotocininduced diabetic rats. Mol. Cell. Biochem. 2003, 243, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Cai, L.; Wang, Y.; Zhou, G.; Chen, T.; Song, Y.; Li, X.; Kang, Y.J. Attenuation by metallothionein of early cardiac cell death via suppression of mitochondrial oxidative stress results in a prevention of diabetic cardiomyopathy. J. Am. Coll. Cardiol. 2006, 48, 1688–1697. [Google Scholar] [CrossRef] [PubMed]
- Hatanaka, E.; Monteagudo, P.T.; Marrocos, M.S.; Campa, A. Neutrophils and monocytes as potentially important sources of proinflammatory cytokines in diabetes. Clin. Exp. Immunol. 2006, 146, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Rosner, M.H.; Ronco, C.; Okusa, M.D. The role of inflammation in the cardio-renal syndrome: A focus on cytokines and inflammatory mediators. Semin. Nephrol. 2012, 32, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Niu, J.; Gilliland, M.G.; Jin, Z.; Kolattukudy, P.E.; Hoffman, W.H. MCP-1and IL-1β expression in the myocardia of two young patients with Type 1 diabetes mellitus and fatal diabetic ketoacidosis. Exp. Mol. Pathol. 2014, 96, 71–79. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, Y.-M.; Hung, Y.-c.; Hu, L.; Lee, Y.-j.; Yin, M.-c. Anti-Diabetic Effects of Madecassic Acid and Rotundic Acid. Nutrients 2015, 7, 10065-10075. https://doi.org/10.3390/nu7125512
Hsu Y-M, Hung Y-c, Hu L, Lee Y-j, Yin M-c. Anti-Diabetic Effects of Madecassic Acid and Rotundic Acid. Nutrients. 2015; 7(12):10065-10075. https://doi.org/10.3390/nu7125512
Chicago/Turabian StyleHsu, Yuan-Man, Yi-chih Hung, Lihong Hu, Yi-ju Lee, and Mei-chin Yin. 2015. "Anti-Diabetic Effects of Madecassic Acid and Rotundic Acid" Nutrients 7, no. 12: 10065-10075. https://doi.org/10.3390/nu7125512
APA StyleHsu, Y. -M., Hung, Y. -c., Hu, L., Lee, Y. -j., & Yin, M. -c. (2015). Anti-Diabetic Effects of Madecassic Acid and Rotundic Acid. Nutrients, 7(12), 10065-10075. https://doi.org/10.3390/nu7125512