Magnesium in Prevention and Therapy

Abstract
:1. Introduction
2. Functions of Magnesium

| Magnesium is involved in more than 300 essential metabolic reactions (e.g., all Adenosine Triphosphate (ATP)-dependent reactions). |
| Energy production (→ ATP production) |
| Breakdown and energetic utilization of carbohydrates, proteins and fats in intermediate metabolism (e.g., glycolysis, respiratory chain phosphorylation). ATP exists primarily as a complex with magnesium (MgATP). |
| Enzyme activation (examples) |
| Mitochondrial ATP synthase, Na+/K+-ATPase, Hexokinase, Creatine kinase, Adenylate cyclase, Phosphofructokinase, tyrosine kinase activity of the insulin receptor. |
| Calcium antagonist/NMDA-receptor antagonist |
| Control of calcium influx at the cell membrane (course of contractions, regulation of vascular muscle tone): muscle contraction/relaxation, neurotransmitter release, action potential conduction in nodal tissue, neuromuscular impulse conduction (inhibition of calcium-dependent acetylcholine release at the motor end plate), maintenance and stabilization of membrane physiology, muscle contraction. |
| Cardiovascular system |
| Economization of cardiac pump function, regulation of potassium movement in myocardial cells, protection against stress, vasodilation of the coronary and peripheral arteries, reduction of platelet aggregation. |
| Membrane function |
| Transmembrane electrolyte flux, active transport of potassium and calcium across cell membranes, regulation of cell adhesion and cell migration. |
| Structural roles |
| Component of mineralized bone (structure, microarchitecture), multiple enzyme complexes, mitochondria, proteins, polyribosomes, and nucleic acids. |
| Nutrient metabolism |
| Metabolic activation and utilisation of vitamin D, B-vitamins (e.g., thiamine) and glutathione. |
3. Magnesium and Nutrition
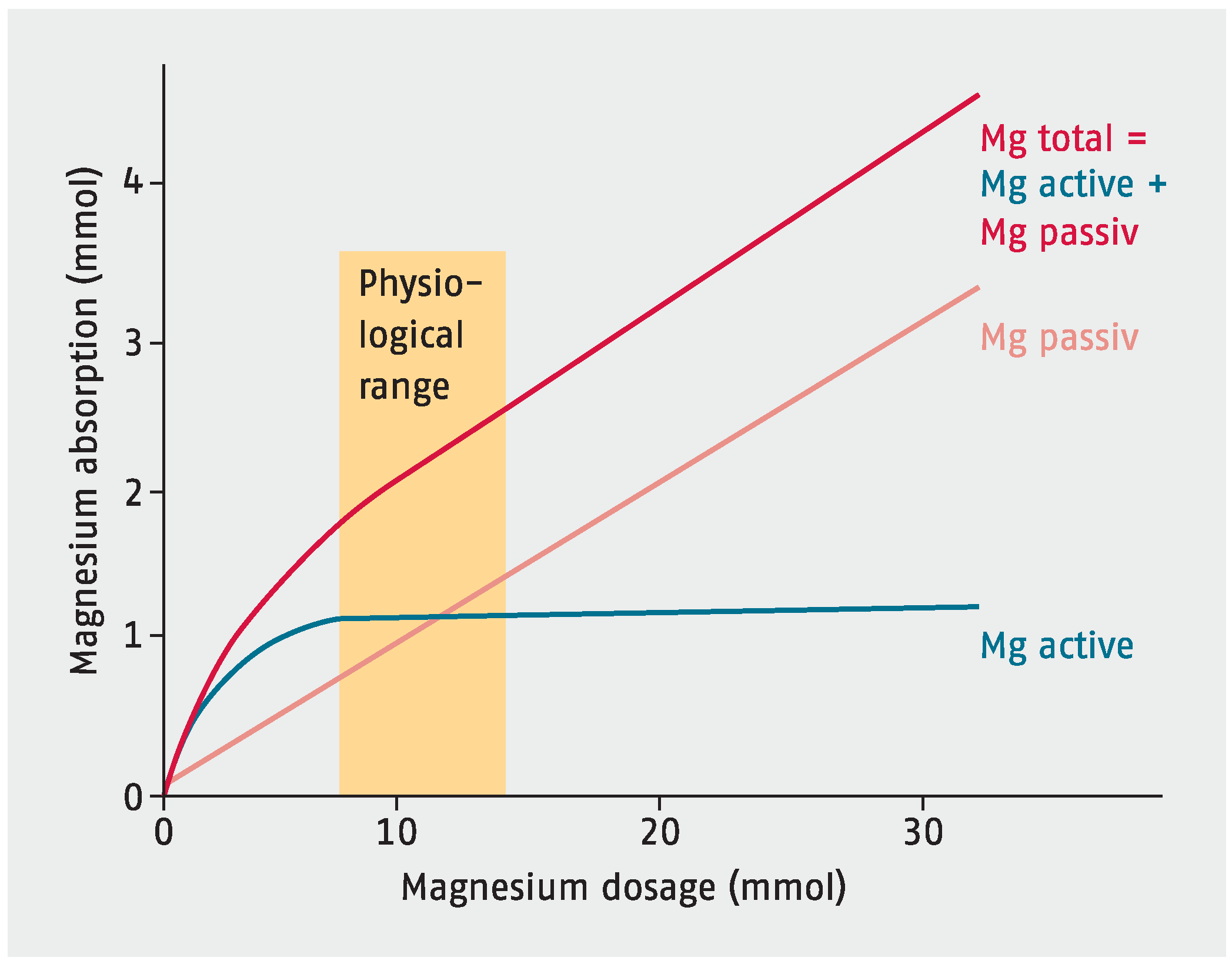
4. Magnesium Absorption and Excretion

5. Magnesium Status
6. Magnesium Deficiency
| General: Anxiety, lethargy, weakness, agitation, depression, dysmenorrhea, hyperactivity, headache, irritability, dysacusis, low stress tolerance, loss of appetite, nausea, sleep disorders, impaired athletic performance. |
| Musculature: Muscle spasm, cramps in the soles of the feet, leg cramps, facial muscles, masticatory muscles, and calves, carpopedal spasm, back aches, neck pain, urinary spasms, magnesium deficiency tetany. |
| Nerves/CNS: Nervousness, increased sensitivity of NMDA receptors to excitatory neurotransmitters, migraine, depression, nystagmus, paraesthesia, poor memory, seizures, tremor, vertigo. |
| Gastrointestinal tract: Constipation. |
| Cardiovascular system: Risk of arrhythmias, supraventricular or ventricular arrhythmias, hypertension, coronary spasm, decreased myocardial pump function, digitalis sensitivity, Torsade de pointes, death from heart disease. |
| Electrolytes: Hypokalaemia, hypocalcaemia, retention of sodium. |
| Metabolism: Dyslipoproteinemia (increased blood triglycerides and cholesterol), decreased glucose tolerance, insulin resistance, increased risk of metabolic syndrome, disturbances of bone and vitamin D metabolism, resistance to PTH, low circulating levels of PTH, resistance to vitamin D, low circulating levels of 25(OH)D, recurrence of calcium oxalate calculi. |
| Miscellaneous: Asthma, chronic fatigue syndrome, osteoporosis, hypertension, altered glucose homeostasis. |
| Pregnancy: Pregnancy complications (e.g., miscarriage, premature labor, eclampsia). |
| Drug Group (Drug Substance) | Mechanism/Effect |
|---|---|
| Aminoglycosides (e.g., gentamicin, tobramycin, amikacin) | increased renal magnesium loss, secondary hyperaldosteronism |
| Antimicrobial medication (Pentamidine) | increased renal magnesium loss |
| Antiviral medication (foscarnet) | nephrotoxicity, increased renal magnesium loss |
| Beta adrenergic agonists (e.g., Fenoterol, salbutamol, theophylline) | increased renal magnesium excretion, metabolic abnormalities (magnesium shift into cells) |
| Bisphosphonates (pamidronate) | renal impairment, magnesium excretion |
| Chemotherapeutic agents (e.g., amsacrine, cisplatin) | nephrotoxicity, cisplatin accumulates in renal cortex, increased renal magnesium loss |
| Immunosuppressants (cyclosporine, sirolimus) | 2- to 3-fold increased urinary magnesium excretion (→ magnesium wasting) |
| Loop diuretics, esp. long-term use | increased renal magnesium loss, secondary hyperaldosteronism |
| Monoclonal antibody (e.g. cetuximab, panitumumab) | EGFR blockade in the nephron impairs the active transport of magnesium (→ magnesium wasting) |
| Polyene antifungals (amphotericin B) | nephrotoxicity |
| Proton pump inhibitors | loss of active magnesium absorption via transient receptor potential melastatin-6 and -7 (TRPM6/7) |
| Thiazide diuretics, esp. long-term use (e.g., hydrochlorothiazide) | increased renal magnesium loss, secondary hyperaldosteronism |
7. Magnesium in the Treatment and Prevention of Diseases
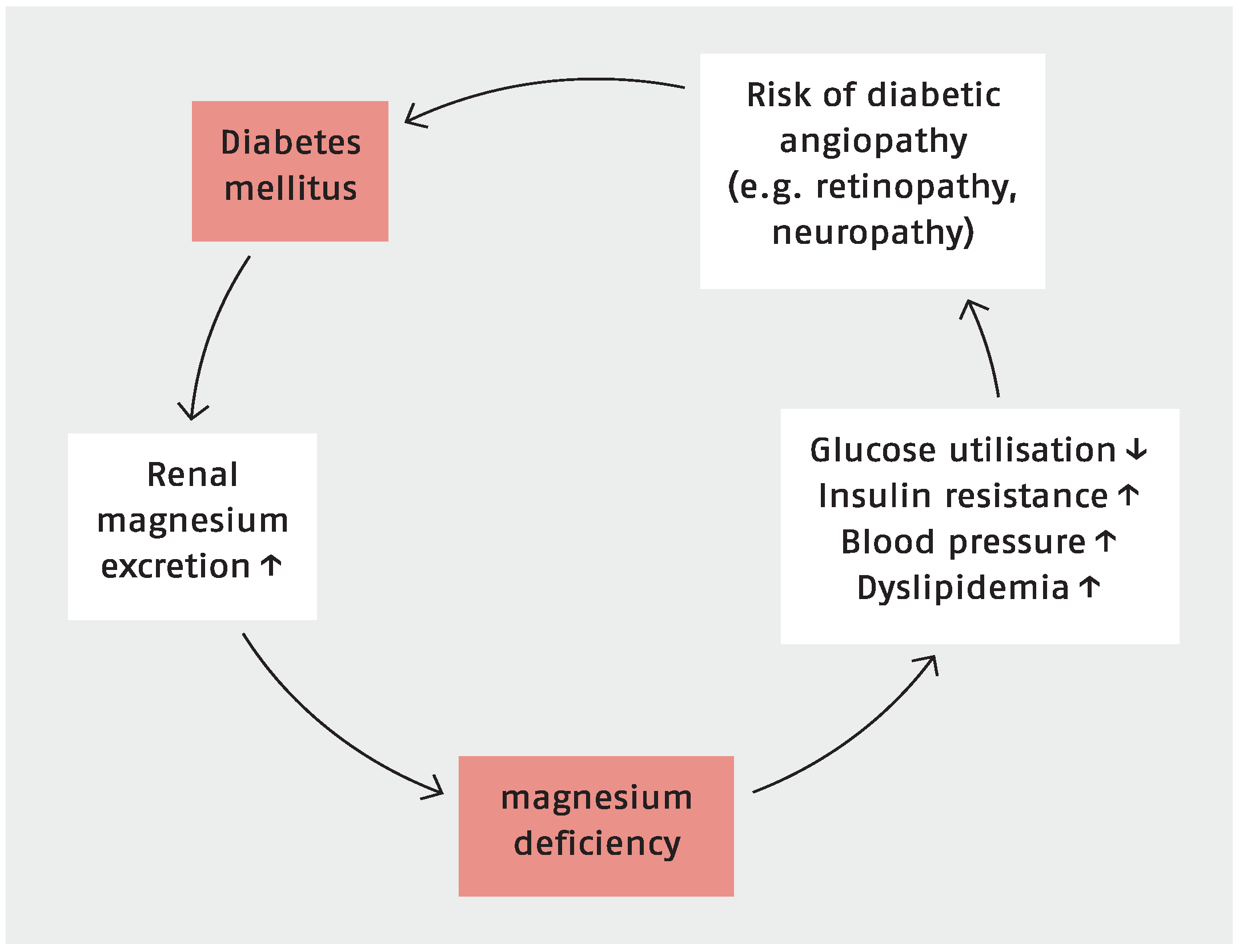
7.1. Magnesium, Type 2 Diabetes and Metabolic Syndrome

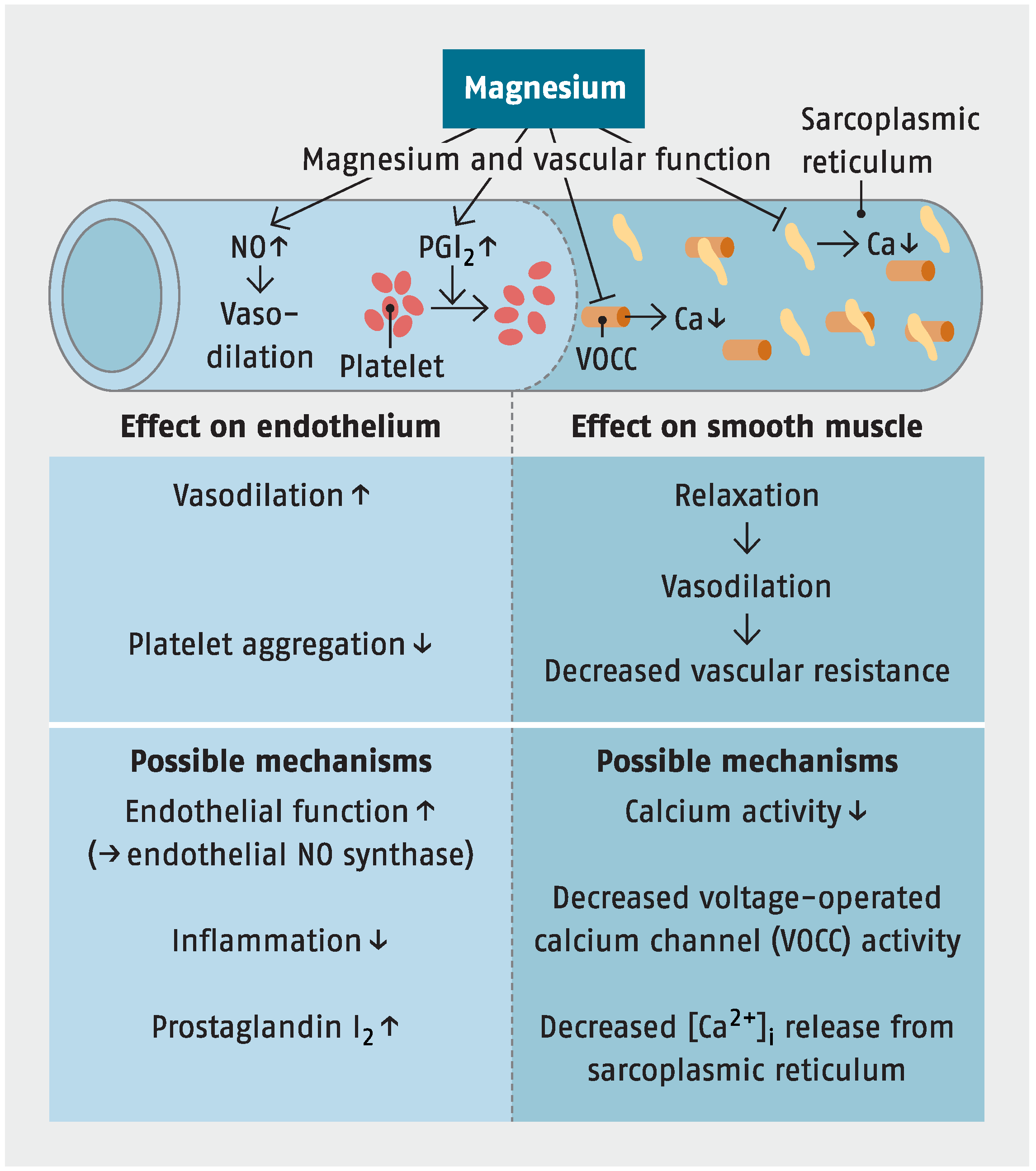
7.2. Cardiovascular Disease
7.2.1. Hypertension

{kind=link}
{kind=link}
{kind=link}
7.2.2. Coronary Heart Disease, Myocardial Infarction and Stroke
7.3. Pre-Eclampsia and Eclampsia
7.4. Migraine Headaches
7.5. ADHD
7.6. Alzheimer’s Disease
7.7. Asthma
7.8. Miscellaneous
8. Dosage and Supplements
9. Adverse Effects and Interactions
10. Conclusions
Conflicts of Interest
References
- Cotton, F.A.; Wilkinson, G. Anorganische Chemie; Chemie GmbH: Weilheim, Germany, 1967. [Google Scholar]
- Weast, R.C. Handbook of Chemistry and Physics; CRC Press: Boca Raton, FL, USA, 1987. [Google Scholar]
- Hollemann, A.F.; Wiberg, E. Lehrbuch der Anorganischen Chemie; De Gruyter: Berlin, Germany, 1964. [Google Scholar]
- Bodaker, I.; Sharon, I.; Suzuki, M.; Feingersch, R.; Shmoish, M.; Andreishcheva, E.; Sogin, M.L.; Rosenberg, M.; Maguiere, M.E.; Belkin, S.; et al. Comparative community genomics in the Dead Sea: An increasingly extreme environment. ISME J. 2010, 4, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Ridker, P.M.; Manson, J.E.; Cook, N.R.; Buring, J.E.; Liu, S. Magnesium intake, C-reactive protein, and the prevalence of metabolic syndrome in middle-aged and older U.S. Women. Diabetes Care 2005, 28, 1438–1444. [Google Scholar] [CrossRef] [PubMed]
- Standing Committee on the Scientific Evaluation of Dietary Reference Intakes; Food and Nutrition Board; Institute of Medicine (IOM). Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride; National Academies Press: Washington, DC, USA, 1997. [Google Scholar]
- Gröber, U. Magnesium. In Micronutrients: Metabolic Tuning-Prevention-Therapy, 1st ed.; Gröber, U., Ed.; MedPharm Scientific Publishers: Stuttgart, Germany, 2009; pp. 159–166. [Google Scholar]
- Rude, R.K. Magnesium. In Encyclopedia of Dietary Supplements, 2nd ed.; Coates, P.M., Betz, J.M., Eds.; Informa Healthcare: New York, NY, USA, 2010; pp. 527–537. [Google Scholar]
- Rude, R.K. Magnesium. In Modern Nutrition in Health and Disease, 11th ed.; Ross, A.C., Caballero, B., Cousins, R.J., Tucker, K.L., Ziegler, T.R., Eds.; Lippincott Williams & Wilkins: Baltimore, MA, USA, 2012; pp. 159–175. [Google Scholar]
- Swaminathan, R. Magnesium metabolism and its disorders. Clin. Biochem. Rev. 2003, 24, 47–66. [Google Scholar] [PubMed]
- Castiglioni, S.; Cazzaniga, A.; Albisetti, W.; Maier, J.A. Magnesium and osteoporosis: Current state of knowledge and future research directions. Nutrients 2013, 5, 3022–3033. [Google Scholar] [CrossRef] [PubMed]
- Classen, H.G.; Nowitzki, S. The clinical importance of magnesium. 2. The indications for supplementation and therapy. Fortschr. Med. 1990, 10, 198–200. [Google Scholar]
- Kisters, K. Störungen des Magnesiumhaushaltes. Internist 1998, 39, 815–819. [Google Scholar] [CrossRef] [PubMed]
- Seelig, M.S. Magnesium requirements in human nutrition. J. Med. Soc. N. J. 1982, 79, 849–850. [Google Scholar] [PubMed]
- Jahnen-Dechent, J.; Ketteler, M. Magnesium basics. Clin. Kidney J. 2012, 5, i3–i14. [Google Scholar] [CrossRef] [PubMed]
- Ismail, Y.; Ismail, A.A. The underestimated problem of using serum magnesium measurements to exclude magnesium deficiency in adults; a health warning is needed for “normal” results. Clin. Chem. Lab. Med. 2010, 48, 323–327. [Google Scholar] [CrossRef] [PubMed]
- Von Ehrlich, E.; Barbagallo, M.; Classen, H.G.; Guerrero-Romero, F.; Morren, F.C.; Rodriguez-Moran, M.; Vierling, W.; Vormann, J; Kisters, K. The significance of magnesium in insulin resistance, metabolic syndrome, and diabetes—Recommendations of the Association of Magnesium Research e.V. Diabetol. Stoffwechs. 2014, 9, 96–100. [Google Scholar]
- Vormann, J. Update: Magnesium und Diabetes. OM—Z. Orthomol. Med. 2014, 1, 6–8. [Google Scholar]
- Švagždienė, M.; Širvinskas, E.; Baranauskienė, D.; Adukauskienė, D. Correlation of magnesium deficiency with C-reactive protein in elective cardiac surgery with cardiopulmonary bypass for ischemic heart disease. Medicina (Kaunas) 2015, 51, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Moshfegh, A.; Goldman, J.; Ahuja, J.; Rhodes, D.; LaComb, R. What We Eat in America, NHANES 2005–2006: Usual Nutrient Intakes from Food and Water Compared to 1997 Dietary Reference Intakes for Vitamin D, Calcium, Phosphorus, and Magnesium; U.S. Department of Agriculture, Agricultural Research Service: Washington, DC, USA, 2009. [Google Scholar]
- Nationale Verzehrsstudie II. Available online: http://www.was-esse-ich.de/uploads/media/NVSII_Abschlussbericht_Teil_2.pdf (accessed on 13 June 2015).
- Shah, N.C.; Shah, J.G.; Li, Z.; Jiang, X.C.; Altura, B.T.; Altura, B.M. Short-term magnesium deficiency downregulates telomerase, upregulates neutral sphingomyelinase and induces oxidative DNA damage in cardiovascular tissues: relevance to atherogenesis, cardiovascular diseases and aging. Int. J. Clin. Exp. Med. 2014, 7, 497–514. [Google Scholar] [PubMed]
- Ma, J.; Folsom, A.R.; Melnick, S.L.; Eckfeldt, J.H.; Sharrett, A.R.; Nabulsi, A.A.; Hutchinson, R.G.; Metcalf, P.A. Associations of serum and dietary magnesium with cardiovascular disease, hypertension, diabetes, insulin, and carotid arterial wall thickness: The ARIC study. Atherosclerosis Risk in Communities Study. J. Clin. Epidemiol. 1995, 48, 927–940. [Google Scholar] [CrossRef]
- Altura, B.M. Introduction: importance of Mg in physiology and medicine and the need for ion selective electrodes. Scand. J. Clin. Lab. Invest. Suppl. 1994, 217, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Marx, A.; Neutra, R.R. Magnesium in drinking water and ischemic heart disease. Epidemiol. Rev. 1997, 19, 258–272. [Google Scholar] [CrossRef] [PubMed]
- Magnesium. Available online: http://fnic.nal.usda.gov/food-composition/vitamins-and-minerals/magnesium (accessed on 8 January 2015).
- Nielsen, F.H. Magnesium, inflammation, and obesity in chronic disease. Nutr Rev. 2010, 68, 333–340. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). National Health and Nutrition Examination Survey. Available online: http://www.ars.usda.gov/SP2UserFiles/Place/80400530/pdf/0506/usual_nutrient_intake_vitD_ca_phos_mg_2005-06.pdf (accessed on 8 January 2015).
- Chiuve, S.E.; Korngold, E.C.; Januzzi, J.L., Jr.; Gantzer, M.L.; Albert, C.M. Plasma and dietary magnesium and risk of sudden cardiac death in women. Am. J. Clin. Nutr. 2011, 93, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Orsini, N.; Wolk, A. Dietary magnesium intake and risk of stroke: A meta-analysis of prospective studies. Am. J. Clin. Nutr. 2012, 95, 362–366. [Google Scholar] [CrossRef] [PubMed]
- Durlach, J. Magnesium depletion and pathogenesis of Alzheimer’s disease. Magnes. Res. 1990, 3, 217–218. [Google Scholar] [PubMed]
- Rosanoff, A.; Plesset, M.R. Oral magnesium supplements decrease high blood pressure (SBP > 155 mm Hg) in hypertensive subjects on anti-hypertensive medications: A targeted meta-analysis. Magnes. Res. 2013, 26, 93–99. [Google Scholar] [PubMed]
- Barbagallo, M.; Belvedere, M.; Dominguez, L.J. Magnesium homeostasis and aging. Magnes. Res. 2009, 22, 235–246. [Google Scholar] [PubMed]
- Palmer, B.F.; Clegg, D.J. Electrolyte and Acid-Base Disturbances in Patients with Diabetes Mellitus. N. Engl. J. Med. 2015, 373, 548–559. [Google Scholar] [PubMed]
- Graham, L.A.; Caesar, J.J.; Burgen, A.S. Gastrointestinal absorption and excretion of Mg 28 in man. Metabolism 1960, 9, 646–659. [Google Scholar] [PubMed]
- Saris, N.E.; Mervaala, E.; Karppanen, H.; Khawaja, J.A.; Lewenstam, A. Magnesium: An update on physiological, clinical and analytical aspects. Clin. Chim. Acta 2000, 294, 1–26. [Google Scholar] [CrossRef]
- Jeroen, H.; de Baaij, F.; Joost, G.; Hoenderop, J.; Rene, J.; Bindels, M. Regulation of magnesium balance: Lessons learned from human genetic disease. Clin. Kidney J. 2012, 5, i15–i24. [Google Scholar]
- Quamme, G.A. Recent developments in intestinal magnesium absorption. Curr. Opin. Gastroenterol. 2008, 24, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Amasheh, S.; Fromm, M.; Günzel, D. Claudins of intestine and nephron—A correlation of molecular tight junction structure and barrier function. Acta. Physiol. (Oxf). 2011, 201, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Touyz, R.M. Magnesium in clinical medicine. Front. Biosci. 2004, 9, 1278–1293. [Google Scholar] [CrossRef] [PubMed]
- Van der Wijst, J.; Bindels, R.J.; Hoenderop, J.G. Mg2+ homeostasis: The balancing act of TRPM6. Curr. Opin. Nephrol. Hypertens. 2014, 23, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Tokmak, F.; Kisters, K.; Hausberg, M.; Rump, L.C. Buffer function of the cell membrane for magnesium in chronic kidney disease. Trace Elem. Electrol. 2008, 25, 234–235. [Google Scholar]
- Zittermann, A. Magnesium deficit? Overlooked cause of low vitamin D status? BMC Med. 2013, 11, 229. [Google Scholar] [CrossRef] [PubMed]
- Den, X.; Song, Y.; Manson, J.E.; Signorello, L.B.; Zhang, S.M.; Shrubsole, M.J.; Ness, R.M.; Seidner, D.L.; Dai, Q. Magnesium, vitamin D status and mortality: Results from US National Health and Nutrition Examination Survey (NHANES) 2001 to 2006 and NHANES III. BMC Med. 2013, 11, 187. [Google Scholar]
- Groenestege, W.M.; Hoenderop, J.G.; van den Heuvel, L.; Knoers, N.; Bindels, R.J. The epithelial Mg2+ channel transient receptor potential melastatin 6 is regulated by dietary Mg2+ content and estrogens. J. Am. Soc. Nephrol. 2006, 17, 1035–1043. [Google Scholar] [CrossRef] [PubMed]
- Anast, C.S.; Winnacker, J.L.; Forte, L.R.; Burns, T.W. Impaired release of parathyroid hormone in magnesium deficiency. J. Clin. Endocrinol. Metab. 1976, 42, 707–717. [Google Scholar] [CrossRef] [PubMed]
- Zofková, I.; Kancheva, R.L. The relationship between magnesium and calciotrophic hormones. Magnes. Res. 1995, 8, 77–84. [Google Scholar] [PubMed]
- Tibbetts, D.M.; Aub, J.C. Magnesium metabolism in health and disease. III. In exophthalmic goiter, basophilic adenoma, Addison’s disease and steatorrhea. J. Clin. Investig. 1937, 16, 511–514. [Google Scholar]
- Gao, X.; Peng, L.; Adhikari, C.M.; Lin, J.; Zuo, Z. Spironolactone reduced arrhythmia and maintained magnesium homeostasis in patients with congestive heart failure. J. Card. Fail. 2007, 13, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Gibson, R.S. Principles of Nutritional Assessment, 2nd ed.; Oxford University Press: New York, NY, USA, 2005. [Google Scholar]
- Witkowski, M.; Hubert, J.; Mazur, A. Methods of assessment of magnesium status in humans: A systematic review. Magnes. Res. 2011, 24, 163–180. [Google Scholar] [PubMed]
- Geiger, H.; Wanner, C. Magnesium in disease. Clin. Kidney J. 2012, 5, i25–i38. [Google Scholar] [CrossRef] [PubMed]
- Elin, R.J. Assessment of magnesium status for diagnosis and therapy. Magnes. Res. 2010, 23, S194–S198. [Google Scholar] [PubMed]
- Lowenstein, F.W.; Stanton, M.F. Serum magnesium levels in the United States, 1971–1974. J. Am. Coll. Nutr. 1986, 5, 399–414. [Google Scholar] [CrossRef] [PubMed]
- Liebscher, D.H.; Liebscher, D.E. About the misdiagnosis of magnesium deficiency. J. Am. Coll. Nutr. 2004, 23, 730S–731S. [Google Scholar] [CrossRef] [PubMed]
- Everett, C.J.; King, D.E. Serum magnesium and the development of diabetes. Nutrition 2006, 22, 679. [Google Scholar] [CrossRef] [PubMed]
- Pham, P.C.; Pham, P.M.; Pham, P.A.; Pham, S.V.; Pham, H.V.; Miller, J.M.; Yanagawa, N.; Pham, P.T. Lower serum magnesium levels are associated with more rapid decline of renal function in patients with diabetes mellitus type 2. Clin. Nephrol. 2005, 63, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Pham, P.C.; Pham, P.M.; Pham, S.V.; Miller, J.M.; Pham, P.T. Hypomagnesemia in patients with type 2 diabetes. Clin. J. Am. Soc. Nephrol. 2007, 2, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Vierling, W.; Liebscher, D.H.; Micke, O.; von Ehrlich, B.; Kisters, K. Magnesium deficiency and therapy in cardiac arrhythmias: Recommendations of the German Society for Magnesium Research. Dtsch. Med. Wochenschr. 2013, 138, 1165–1171. [Google Scholar] [PubMed]
- Chernow, B.; Bamberger, S.; Stoiko, M.; Vadnais, M.; Mills, S.; Hoellerich, V.; Warshaw, A.L. Hypomagnesemia in patients in postoperative intensive care. Chest 1989, 95, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Whang, R.; Ryder, K.W. Frequency of hypomagnesemia and hypermagnesemia. Requested vs. routine. JAMA 1990, 263, 3063–3064. [Google Scholar] [CrossRef] [PubMed]
- Spätling, L.; Classen, H.G.; Külpmann, W.R.; Manz, F.; Rob, P.M.; Schimatschek, H.F.; Vierling, W.; Vormann, J.; Weigert, A.; Wink, K. Diagnosing magnesium deficiency. Current recommendations of the Society for Magnesium Research. Fortschr. Med. Orig. 2000, 118, 49–53. [Google Scholar] [PubMed]
- Gröber, U. Interactions between drugs and micronutrients. Med. Monatsschr. Pharm. 2006, 29, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Gröber, U. Antihypertensives and magnesium—Update 2007. Trace. Elem. Electrolyt. 2009, 26, 15–16. [Google Scholar] [CrossRef]
- Classen, H.G.; Gröber, U.; Kisters, K. Drug-induced magnesium deficiency. Med. Monatsschr. Pharm. 2012, 35, 274–280. [Google Scholar] [PubMed]
- Massy, Z.A.; Drüeke, T.B. Magnesium and cardiovascular complications of chronic kidney disease. Nat. Rev. Nephrol. 2015. [Google Scholar] [CrossRef] [PubMed]
- Guerrero-Romero, F.; Simental-Mendía , L.E.; Hernández-Ronquillo, G.; Rodriguez-Morán, M. Oral magnesium supplementation improves glycaemic status in subjects with prediabetes and hypomagnesaemia: A double-blind placebo-controlled randomized trial. Diabetes Metab. 2015, 41, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Kisters, K.; Gröber, U. Lowered magnesium in hypertension. Hypertension 2013, 62, e19. [Google Scholar] [CrossRef] [PubMed]
- Ishimura, E.; Okuno, S.; Yamakawa, T.; Inaba, M.; Nishizawa, Y. Serum magnesium concentration is a significant predictor of mortality in maintenance hemodialysis patients. Magnes. Res. 2007, 20, 237–244. [Google Scholar] [PubMed]
- Altura, B.M.; Altura, B.T. Magnesium and cardiovascular biology: An important link between cardiovascular risk factors and atherogenesis. Cell. Mol. Biol. Res. 1995, 41, 347–359. [Google Scholar] [PubMed]
- Djurhuus, M.S.; Skøtt, P.; Hother-Nielson, O.; Klitgaard, N.A.; Beck-Nielsen, H. Insulin increases renal magnesium excretion: A possible cause of magnesium depletion in hyperinsulinaemic states. Diabet. Med. 1995, 12, 664–669. [Google Scholar] [CrossRef] [PubMed]
- Ramadass, S.; Basu, S.; Srinivasan, A.R. Serum magnesium levels as an indicator of status of Diabetes Mellitus type 2. Diabetes Metab. Syndr. 2015, 9, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Perazella, M.A. Proton pump inhibitors and hypomagnesemia: A rare but serious complication. Kidney Int. 2013, 83, 553–556. [Google Scholar] [CrossRef] [PubMed]
- Barragán-Rodríguez, L.; Rodríguez-Morán, M.; Guerrero-Romero, F. Efficacy and safety of oral magnesium supplementation in the treatment of depression in the elderly with type 2 diabetes: A randomized, equivalent trial. Magnes. Res. 2008, 21, 218–223. [Google Scholar] [PubMed]
- Forbes, J.M.; Cooper, M.E. Mechanisms of diabetic complications. Physiol. Rev. 2013, 93, 137–188. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Wolk, A. Magnesium intake and risk of type 2 diabetes: A meta-analysis. J. Intern. Med. 2007, 262, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.J.; Xun, P.; Liu, K.; Loria, C.; Yokota, K.; Jacobs, D.R., Jr.; He, K. Magnesium intake in relation to systemic inflammation, insulin resistance, and the incidence of diabetes. Diabetes Care 2010, 33, 2604–2610. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.Y.; Xun, P.; He, K.; Qin, L.Q. Magnesium intake and risk of type 2 diabetes: Meta-analysis of prospective cohort studies. Diabetes Care 2011, 34, 2116–2122. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Persuitte, G.; Olendzki, B.C.; Wedick, N.M.; Zhang, Z.; Merriam, P.A.; Fang, H.; Carmody, J.; Olendzki, G.F.; Ma, Y. Dietary magnesium intake improves insulin resistance among non-diabetic individuals with metabolic syndrome participating in a dietary trial. Nutrients 2013, 5, 3910–3919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hruby, A.; Meigs, J.B.; O’Donnell, C.J.; Jacques, P.F.; McKeown, N.M. Higher magnesium intake reduces risk of impaired glucose and insulin metabolism and progression from prediabetes to diabetes in middle-aged americans. Diabetes Care 2014, 37, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Mooren, F.C.; Krüger, K.; Völker, K.; Golf, S.W.; Wadepuhl, M.; Kraus, A. Oral magnesium supplementation reduces insulin resistance in non-diabetic subjects—A double-blind, placebo-controlled, randomized trial. Diabetes Obes. Metab. 2011, 13, 281–284. [Google Scholar] [CrossRef] [PubMed]
- Von Ehrlich, B.; Wadepuhl, M. Erhöhtes Risiko einer diabetischen Retinopathie bei niedrigem Serum-Magnesium. Diabetes Stoffwechs. 2003, 12, 285–289. [Google Scholar]
- De Leeuw, I.; Engelen, W.; de Block, C.; van Gall, L. Long term magnesium supplementation influences favourably the natural evolution of neuropathy in Mg-depleted type 1 diabetic patients (T1DM). Mag. Res. 2004, 17, 109–114. [Google Scholar]
- Pham, P.C.; Pham, P.M.; Pham, P.T.; Pham, S.V.; Pham, P.A.; Pham, P.T. The link between lower serum magnesium and kidney function in patients with diabetes mellitus type 2 deserves a closer look. Clin. Nephrol. 2009, 71, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Grafton, G.; Bunce, C.M.; Sheppard, M.C.; Brown, G.; Baxter, M.A. Effect of Mg2+ on Na(+)-dependent inositol transport. Role for Mg2+ in etiology of diabetic complications. Diabetes 1992, 41, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.H.; Lu, Y.F.; Cheng, F.C.; Lee, J.N.; Tsai, L.C. Correlation of magnesium intake with metabolic parameters, depression and physical activity in elderly type 2 diabetes patients: A cross-sectional study. Nutr. J. 2012, 11, 41. [Google Scholar] [CrossRef] [PubMed]
- Guerrero-Romero, F.; Rascón-Pacheco, R.A.; Rodríguez-Morán, M.; de la Peña, J.E.; Wacher, N. Hypomagnesaemia and risk for metabolic glucose disorders: A 10-year follow-up study. Eur. J. Clin. Investig. 2008, 38, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Fox, C.; Ramsoomair, D.; Carter, C. Magnesium: Its proven and potential clinical significance. South. Med. J. 2001, 94, 1195–1201. [Google Scholar] [CrossRef] [PubMed]
- Kisters, K.; Gremmler, B.; Hausberg, M. Pulse pressure, plasma magnesium status, and antihypertensive therapy. Am. J. Hypertens. 2005, 18, 1136. [Google Scholar] [CrossRef] [PubMed]
- Kisters, K.; Tepel, M.; Spieker, C.; Zidek, W.; Barenbrock, M.; Tokmak, F.; Kosch, M.; Hausberg, M.; Rahn, K.H. Decreased membrane Mg2+ concentrations in a subgroup of hypertensives: Membrane model for the pathogenesis of primary hypertension. Am. J. Hypertens. 1998, 11, 1390–1393. [Google Scholar] [CrossRef]
- Kosch, M.; Hausberg, M.; Westermann, G.; Köneke, J.; Matzkies, F.; Rahn, K.H.; Kisters, K. Alterations in calcium and magnesium content of red cell membranes in patients with primary hypertension. Am. J. Hypertens. 2001, 14, 254–258. [Google Scholar] [CrossRef]
- Kisters, K.; Wessels, F.; Küper, H.; Tokmak, F.; Krefting, E.R.; Gremmler, B.; Kosch, M.; Barenbrock, M.; Hausberg, M. Increased calcium and decreased magnesium concentrations and an increased calcium/magnesium ratio in spontaneously hypertensive rats versus Wistar-Kyoto rats: Relation to arteriosclerosis. Am. J. Hypertens. 2004, 17, 59–62. [Google Scholar] [CrossRef]
- Kisters, K.; Wessels, F.; Tokmak, F; Krefting, E.R.; Gremmler, B.; Kosch, M.; Hausberg, M. Early-onset increased calcium and decreased magnesium concentrations and an increased calcium/magnesium ratio in SHR versus WKY. Magnes. Res. 2004, 17, 264–269. [Google Scholar] [PubMed]
- Nadler, J.L.; Buchanan, T.; Natarajan, R.; Antonipillai, I.; Bergman, R.; Rude, R. Magnesium deficiency produces insulin resistance and increased thromboxane synthesis. Hypertension 1993, 21, 1024–1029. [Google Scholar] [CrossRef] [PubMed]
- Euser, A.G.; Cipolla, M.J. Magnesium sulfate for the treatment of eclampsia: A brief review. Stroke 2009, 40, 1169–1175. [Google Scholar] [CrossRef] [PubMed]
- Jee, S.H.; Miller, E.R.; Guallar, E.; Singh, V.K.; Appel, L.J.; Klag, M.J. The effect of magnesium supplementation on blood pressure: A meta-analysis of randomized clinical trials. Am. J. Hypertens. 2002, 15, 691–696. [Google Scholar] [CrossRef]
- Dickinson, H.O.; Nicolson, D.J.; Campbell, F.; Cook, J.V.; Beyer, F.R.; Ford, G.A.; Mason, J. Magnesium supplementation for the management of essential hypertension in adults. Cochrane Database Syst. Rev. 2006. [Google Scholar] [CrossRef] [Green Version]
- Kass, L.; Weekes, J.; Carpenter, L. Effect of magnesium supplementation on blood pressure: A meta-analysis. Eur. J. Clin. Nutr. 2012, 66, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Hatzistavri, L.S.; Sarafidis, P.A.; Georgianos, P.I.; Tziolas, I.M.; Aroditis, C.P.; Zebekakis, P.E.; Pikilidou, M.I.; Lasaridis, A.N. Oral magnesium supplementation reduces ambulatory blood pressure in patients with mild hypertension. Am. J. Hypertens. 2009, 22, 1070–1075. [Google Scholar] [CrossRef] [PubMed]
- Kisters, K. Oral magnesium supplementation improves borderline hypertension. Magnes. Res. 2011, 24, 17. [Google Scholar] [PubMed]
- Kass, L.S.; Skinner, P.; Poeira, F. A pilot study on the effects of magnesium supplementation with high and low habitual dietary magnesium intake on resting and recovery from aerobic and resistance exercise and systolic blood pressure. J. Sports Sci. Med. 2013, 12, 144–150. [Google Scholar] [PubMed]
- Peacock, J.M.; Ohira, T.; Post, W.; Sotoodehnia, N.; Rosamond, W.; Folsom, A.R. Serum magnesium and risk of sudden cardiac death in the Atherosclerosis Risk in Communities (ARIC) Study. Am. Heart. J. 2010, 160, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Prevention of REnal and Vascular ENd-stage Disease (PREVEND). Available online: https://www.bioshare.eu/content/prevention-renal-and-vascular-end-stage-disease (accessed on 22 September 2015).
- Joosten, M.M.; Gansevoort, R.T.; Mukamal, K.J.; van der Harst, P.; Geleijnse, J.M.; Feskens, E.J.; Navis, G.; Bakker, S.J.; PREVEND Study Group. Urinary and plasma magnesium and risk of ischemic heart disease. Am. J. Clin. Nutr. 2013, 97, 1299–1306. [Google Scholar] [CrossRef] [PubMed]
- Del Gobbo, L.C.; Imamura, F.; Wu, J.H.; de Oliveira Otto, M.C.; Chiuve, S.E.; Mozaffarian, D. Circulating and dietary magnesium and risk of cardiovascular disease: A systematic review and meta-analysis of prospective studies. Am. J. Clin. Nutr. 2013, 98, 160–173. [Google Scholar] [CrossRef] [PubMed]
- Stepura, O.B.; Martynow, A.I. Magnesium orotate in severe congestive heart failure (MACH). Int. J. Cardiol. 2009, 134, 145–147. [Google Scholar] [CrossRef] [PubMed]
- Kisters, K.; Gremmler, B.; Gröber, U. Natriuretic peptides, hypertension, heart insufficiency and magnesium. Adv. Tech. Biol. Med. 2015. [Google Scholar] [CrossRef]
- Kisters, K.; Gremmler, B.; Gröber, U. Magnesium deficiency in hypertensive heart disease. J Hypertens 2015, 33, e273. [Google Scholar] [CrossRef]
- Adebamowo, S.N.; Spiegelman, D.; Willett, W.C.; Rexrode, K.M. Association between intakes of magnesium, potassium, and calcium and risk of stroke: 2 Cohorts of US women and updated meta-analyses. Am. J. Clin. Nutr. 2015, 101, 1269–1277. [Google Scholar] [CrossRef] [PubMed]
- Drew, B.J.; Ackerman, M.J.; Funk, M.; Gibler, W.B.; Kligfield, P.; Menon, V.; Philippides, G.J.; Roden, D.M.; Zareba, W; American Heart Association Acute Cardiac Care Committee of the Council on Clinical Cardiology; the Council on Cardiovascular Nursing; the American College of Cardiology Foundation. Prevention of torsade de pointes in hospital settings: A scientific statement from the American Heart Association and the American College of Cardiology Foundation. Circulation 2010, 121, 1047–1060. [Google Scholar] [PubMed]
- Liu, F.; Zhang, X.; Qi, H.; Wang, J.; Wang, M.; Zhang, Y.; Yan, H.; Zhuang, S. Correlation of serum magnesium with cardiovascular risk factors in maintenance hemodialysis patients—A cross-sectional study. Magnes. Res. 2013, 26, 100–108. [Google Scholar] [PubMed]
- Saver, J.L.; Starkman, S.; Eckstein, M.; Stratton, S.J.; Pratt, F.D.; Hamilton, S.; Conwit, R.; Liebeskind, D.S.; Sung, G.; Kramer, I.; et al. Prehospital use of magnesium sulfate as neuroprotection in acute stroke. N. Engl. J. Med. 2015, 372, 528–536. [Google Scholar] [CrossRef] [PubMed]
- Woods, K.L.; Fletcher, S.; Roffe, C.; Haider, Y. Intravenous magnesium sulphate in suspected acute myocardial infarction: Results of the second Leicester Intravenous Magnesium Intervention Trial (LIMIT-2). Lancet 1992, 339, 1553–1558. [Google Scholar] [CrossRef]
- Fourth International Study of Infarct Survival Collaborative Group. ISIS-4: A randomised factorial trial assessing early oral captopril, oral mononitrate, and intravenous magnesium sulphate in 58050 patients with suspected acute myocardial infarction. The Lancet 1995, 345, 669–682. [Google Scholar]
- Magnesium in Coronaries (MAGIC) Trial Investigators. Early administration of intravenous magnesium to high-risk patients with acute myocardial infarction in the Magnesium in Coronaries (MAGIC) Trial: A randomised controlled trial. Lancet 2002, 360, 1189–1196. [Google Scholar]
- Altman, D.; Carroli, G.; Duley, L.; Farrell, B.; Moodley, J.; Neilson, J.; Smith, D. Magpie Trial Collaboration Group. Do women with pre-eclampsia, and their babies, benefit from magnesium sulphate? The Magpie Trial: A randomised placebo-controlled trial. Lancet 2002, 359, 1877–1890. [Google Scholar] [PubMed]
- Belfort, M.A.; Anthony, J.; Saade, G.R.; Allen, J.C., Jr.; Nimodipine Study Group. A comparison of magnesium sulfate and nimodipine for the prevention of eclampsia. N. Engl. J. Med. 2003, 348, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Mauskop, A.; Altura, B.T.; Cracco, R.Q.; Altura, B.M. Intravenous magnesium sulfate rapidly alleviates headaches of various types. Headache 1996, 36, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Mauskop, A.; Altura, B.T.; Cracco, R.Q.; Altura, B.M. Intravenous magnesium sulfate relieves cluster headaches in patients with low serum ionized magnesium levels. Headache 1995, 35, 597–600. [Google Scholar] [CrossRef] [PubMed]
- Peikert, A; Wilimzig, C.; Köhne-Volland, R. Prophylaxis of migraine with oral magnesium: Results from a prospective, multi-center, placebo-controlled and double-blind randomized study. Cephalalgia 1996, 16, 257–263. [Google Scholar] [CrossRef] [PubMed]
- The International Headache Society Criteria. Available online: http://ihs-classification.org/de/ (accessed on 22 September 2015).
- Gaul, C.; Diener, H.C.; Danesch, U.; Migravent® Study Group. Improvement of migraine symptoms with a proprietary supplement containing riboflavin, magnesium and Q10: A randomized, placebo-controlled, double-blind, multicenter trial. J. Headache Pain 2015, 16, 516. [Google Scholar] [CrossRef] [PubMed]
- Bigal, M.E.; Bordini, C.A.; Tepper, S.J.; Speciali, J.G. Intravenous magnesium sulphate in the acute treatment of migraine without aura and migraine with aura. A randomized, double-blind, placebo-controlled study. Cephalalgia 2002, 22, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Shahrami, A.; Assarzadegan, F.; Hatamabadi, H.R.; Asgarzadeh, M.; Sarehbandi, B.; Asgarzadeh, S. Comparison of therapeutic effects of magnesium sulfate vs. dexamethasone/metoclopramide on alleviating acute migraine headache. J. Emerg. Med. 2015, 48, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Nogovitsina, O.R.; Levitina, E.V. Diagnostic value of examination of the magnesium homeostasis in children with attention deficit syndrome with hyperactivity. Klin. Lab. Diagn. 2005, 5, 17–19. [Google Scholar] [PubMed]
- Starobrat-Hermelin, B.; Kozielec, T. The effects of magnesium physiological supplementation on hyperactivity in children with attention deficit hyperactivity disorder (ADHD). Positive response to magnesium oral loading test. Magnes. Res. 1997, 10, 149–156. [Google Scholar] [PubMed]
- Mousain-Bosc, M.; Roche, M.; Rapin, J.; Bali, J.P. Magnesium VitB6 intake reduces central nervous system hyperexcitability in children. J. Am. Coll Nutr. 2004, 23, 545S–548S. [Google Scholar] [CrossRef] [PubMed]
- Mousain-Bosc, M.; Roche, M.; Polge, A.; Pradal-Prat, D.; Rapin, J.; Bali, J.P. Improvement of neurobehavioral disorders in children supplemented with magnesium-vitamin B6. I. Attention deficit hyperactivity disorders. Magnes. Res. 2006, 19, 46–52. [Google Scholar] [PubMed]
- Mousain-Bosc, M.; Roche, M.; Polge, A.; Pradal-Prat, D.; Rapin, J.; Bali, J.P. Improvement of neurobehavioral disorders in children supplemented with magnesium-vitamin B6. II. Pervasive developmental disorder-autism. Magnes. Res. 2006, 19, 53–62. [Google Scholar] [PubMed]
- Nogovitsina, O.R.; Levitina, E.V. Effect of MAGNE-B6 on the clinical and biochemical manifestations of the syndrome of attention deficit and hyperactivity in children. Eksp. Klin. Farmakol. 2006, 69, 74–77. [Google Scholar] [PubMed]
- Bardgett, M.E.; Schultheis, P.J.; McGill, D.L.; Richmond, R.E.; Wagge, J.R. Magnesium deficiency impairs fear conditioning in mice. Brain Res. 2005, 1038, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Barbagallo, M.; Belvedere, M.; Di Bella, G.; Dominguez, L.J. Altered ionized magnesium levels in mild-to-moderate Alzheimer’s disease. Magnes. Res. 2011, 24, S115–S121. [Google Scholar] [PubMed]
- Cherbuin, N.; Kumar, R.; Sachdev, P.S.; Anstey, K.J. Dietary Mineral Intake and Risk of Mild Cognitive Impairment: The PATH through Life Project. Front. Aging Neurosci. 2014. [Google Scholar] [CrossRef] [PubMed]
- Andrási, E.; Igaz, S.; Molnár, Z.; Makó, S. Disturbances of magnesium concentrations in various brain areas in Alzheimer’s disease. Magnes. Res. 2000, 13, 189–196. [Google Scholar] [PubMed]
- Li, W.; Yu, J.; Liu, Y.; Huang, X.; Abumaria, N.; Zhu, Y.; Huang, X.; Xiong, W.; Ren, C.; Liu, X.G.; et al. Elevation of brain magnesium prevents and reverses cognitive deficits and synaptic loss in Alzheimer’s disease mouse model. J. Neurosci. 2013, 33, 8423–8441. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.P.; Li, L.; Bao, J.; Wang, Z.H.; Zeng, J.; Liu, E.J.; Li, X.G.; Huang, R.X.; Gao, D.; Li, M.Z.; et al. Magnesium protects cognitive functions and synaptic plasticity in streptozotocin-induced sporadic Alzheimer’s model. PLoS ONE 2014, 9, e108645. [Google Scholar] [CrossRef] [PubMed]
- Skobeloff, E.M.; Spivey, W.H.; McNamara, R.M.; Greenspon, L. Intravenous magnesium sulfate for the treatment of acute asthma in the emergency department. JAMA 1989, 262, 1210–1213. [Google Scholar] [CrossRef] [PubMed]
- Kokotajlo, S.; Degnan, L.; Meyers, R.; Siu, A.; Robinson, C. Use of intravenous magnesium sulfate for the treatment of an acute asthma exacerbation in pediatric patients. J. Pediatr. Pharmacol. Ther. 2014, 19, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Cheuk, D.K.; Chau, T.C.; Lee, S.L. A meta-analysis on intravenous magnesium sulphate for treating acute asthma. Arch. Dis. Child. 2005, 90, 74–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blitz, M.; Blitz, S.; Bease, R.; Diner, B.M.; Hughes, R.; Knopp, J.A.; Rowe, B.H. Inhaled magnesium sulfate in the treatment of acute asthma. Cochrane Database Syst. Rev. 2005, 3, CD003898. [Google Scholar] [PubMed]
- Tarleton, E.K.; Littenberg, B. Magnesium intake and depression in adults. J. Am. Board Fam. Med. 2015, 28, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Benassi, L.; Barletta, F.P.; Baroncini, L.; Bertani, D.; Filippini, F.; Beski, L.; Nani, A.; Tesauri, P.; Tridenti, G. Effectiveness of magnesium pidolate in the prophylactic treatment of primary dysmenorrhea. Clin. Exp. Obstet. Gynecol. 1992, 19, 176–179. [Google Scholar] [PubMed]
- Alraek, T.; Lee, M.S.; Choi, T.Y.; Cao, H.; Liu, J. Complementary and alternative medicine for patients with chronic fatigue syndrome: A systematic review. BMC Complement. Altern. Med. 2011. [Google Scholar] [CrossRef] [PubMed]
- Bagis, S.; Karabiber, M.; As, I.; Tamer, L.; Erdogan, C.; Atalay, A. Is magnesium citrate treatment effective on pain, clinical parameters and functional status in patients with fibromyalgia? Rheumatol. Int. 2013, 33, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.H.; Miller, J.M.; Tucker, K.L.; Hu, H.; Park, S.K. Antioxidant vitamins and magnesium and the risk of hearing loss in the US general population. Am. J. Clin. Nutr. 2014, 99, 148–155. [Google Scholar] [CrossRef] [PubMed]
- Riley, J.M.; Kim, H.; Averch, T.D.; Kim, H.J. Effect of magnesium on calcium and oxalate ion binding. J. Endourol. 2013, 27, 1487–1492. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi, E.; Khayati Motlagh, S.; Nemati, S.; Tavakoli, Z. Effects of magnesium and vitamin B6 on the severity of premenstrual syndrome symptoms. J. Caring Sci. 2012, 1, 183–189. [Google Scholar] [PubMed]
- Cevette, M.J.; Barrs, D.M.; Patel, A.; Conroy, K.P.; Sydlowski, S.; Noble, B.N.; Nelson, G.A.; Stepanek, J. Phase 2 study examining magnesium-dependent tinnitus. Int. Tinnitus J. 2011, 16, 168–173. [Google Scholar] [PubMed]
- Kisters, K. What is the correct magnesium supplement? Magnes. Res. 2013, 26, 41–42. [Google Scholar] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gröber, U.; Schmidt, J.; Kisters, K. Magnesium in Prevention and Therapy. Nutrients 2015, 7, 8199-8226. https://doi.org/10.3390/nu7095388
Gröber U, Schmidt J, Kisters K. Magnesium in Prevention and Therapy. Nutrients. 2015; 7(9):8199-8226. https://doi.org/10.3390/nu7095388
Chicago/Turabian StyleGröber, Uwe, Joachim Schmidt, and Klaus Kisters. 2015. "Magnesium in Prevention and Therapy" Nutrients 7, no. 9: 8199-8226. https://doi.org/10.3390/nu7095388
APA StyleGröber, U., Schmidt, J., & Kisters, K. (2015). Magnesium in Prevention and Therapy. Nutrients, 7(9), 8199-8226. https://doi.org/10.3390/nu7095388