Clustering of Dietary Patterns, Lifestyles, and Overweight among Spanish Children and Adolescents in the ANIBES Study

 ,
,  ,
,  , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Methods
2.1. Measurements
2.1.1. Lifestyle Factors
Diet
Physical Activity
Sedentary Behaviors
Sleep Duration
2.1.2. Body Measurements
2.1.3. Covariates
Parental Education
Socioeconomic Status (SES)
2.2. Data Cleaning
2.3. Data Analysis
2.3.1. Dietary Patterns
2.3.2. Lifestyle Patterns
3. Results
3.1. Sample Characteristics
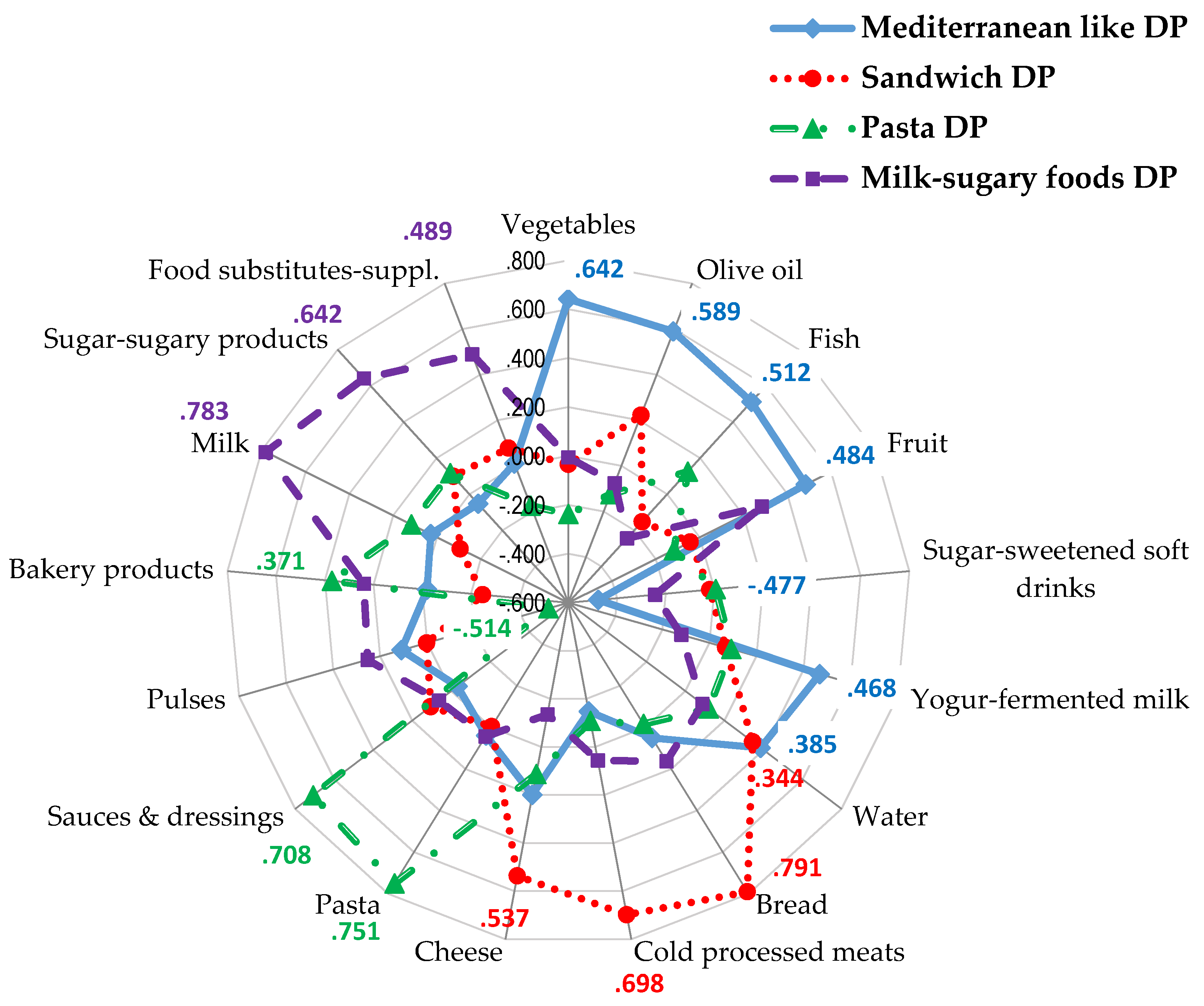
3.2. Dietary Patterns

3.3. Lifestyle Patterns

{kind=link}
| Characteristics | Unhealthier Lifestyle Pattern | Healthier Lifestyle Pattern | χ2 |
|---|---|---|---|
| N (%) | 319 (76.9%) | 96 (23.1%) | |
| Gender | N (%) | N (%) | |
| Boys | 186 (58.3%) | 72 (75.0%) | 8.74 * |
| Girls | 133 (41.7%) | 24 (25.0%) | |
| Age group | 2.74 | ||
| Children (9–12 years) | 152 (47.6%) | 55 (57.3%) | |
| Adolescents (13–17 years) | 167 (52.4%) | 41 (42.7%) | |
| Parental educational level | 1.46 | ||
| Primary or less | 107 (33.5%) | 28 (29.2%) | |
| Secondary | 157 (49.2%) | 54 (56.3%) | |
| Higher | 55 (17.2%) | 14 (14.6%) | |
| Family SES | 2.82 | ||
| Low | 71 (22.3%) | 14 (14.6%) | |
| Mid low | 79 (24.8%) | 28 (29.2%) | |
| Mid Mid high-high | 169 (53.0%) | 54 (56.3%) | |
| BMI status | 1.31 | ||
| Normal weight | 202 (63.3%) | 64 (66.7%) | |
| Overweight | 89 (27.9%) | 27 (28.1%) | |
| Obese | 28 (8.8%) | 5 (5.2%) | |
| Variables | Boys | Girls | ||||||
|---|---|---|---|---|---|---|---|---|
| Children | Adolescents | Children | Adolescents | |||||
| Unhealthier Lifestyle Pattern | Healthier Lifestyle Pattern | Unhealthier Lifestyle Pattern | Healthier Lifestyle Pattern | Unhealthier Lifestyle Pattern | Healthier Lifestyle Pattern | Unhealthier Lifestyle Pattern | Healthier Lifestyle Pattern | |
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |
| Age (year) | 10.3 (1.1) | 10.3 (1.1) | 15.2 (1.5) | 14.9 (1.5) | 10.5 (1.2) | 10.4 (1.2) | 14.9 (1.5) | 15.9 (1.0) † |
| Sleep time week days (h/d) | 8.9 (0.9) | 9.1 (1.1) | 8.0 (0.8) | 8.4 (1.1) | 9.0 (0.9) | 9.1 (1.0) | 7.9 (1.0) | 8.3 (1.2) |
| Sedentary screen time (min/d) | 233 (141) | 214 (107) | 313 (147) | 294 (204) | 211 (107) | 245 (148) | 291 (185) | 259 (145) |
| Vigorous PA (min/d) | 29 (25) | 93 (50) * | 30 (31) | 72 (57) * | 18 (30) | 57 (58) * | 9 (14) | 90 (69) * |
| Moderate PA (min/d) | 27 (24) | 114 (51) * | 18 (21) | 103 (50) * | 23 (25) | 121 (48) * | 13 (14) | 98 (38) * |
| Walking (min/d) | 37 (29) | 105 (60) * | 37 (33) | 103 (57) * | 42 (30) | 90 (54) * | 43 (36) | 80 (53) * |
| Biking (min/d) | 5 (11) | 8 (14) | 2 (5) | 18 (38) * | 1 (4) | 9 (18) | 1 (4) | 1 (2) |
| Total PA (min/d) | 111 (51) | 385 (175) * | 99 (53) | 328 (127) * | 98 (51) | 385 (175) * | 77 (47) | 292 (89) * |
| Mediterranean like DP (Z-score) | −0.08 (0.86) | 0.45 (0.95) # | −0.28 (0.88) | 0.23 (1.35) # | 0.13 (1.0) | 0.35 (0.95) # | −0.16 (0.96) | 0.62 (0.47) # |
| Sandwich DP (Z-score) | 0.01 (0.94) | −0.11 (0.95) | 0.24 (1.05) | 0.12 (1.38) | −0.18 (0.95) | −0.26 (0.95) | −0.30 (0.80) | 0.01 (0.96) |
| Pasta DP (Z-score) | 0.08 (0.92) | 0.03 (1.19) | 0.09 (1.16) | 0.05 (1.05) | −0.09 (0.87) | 0.09 (1.19) | −0.20 (0.81) | −0.19 (0.64) |
| Milk-sugary foods DP (Z-score) | 0.17 (0.81) | 0.08 (0.80) | 0.19 (1.35) | −0.17 (1.09) | −0.01 (0.76) | 0.08 (0.80) | −0.24 (0.89) | −0.59 (0.55) |
| Food Groups | Boys | Girls | ||||||
|---|---|---|---|---|---|---|---|---|
| Unhealthier Lifestyle Pattern | Healthier Lifestyle Pattern | Unhealthier Lifestyle Pattern | Healthier Lifestyle Pattern | |||||
| Mean (SEM) | Median | Mean (SEM) | Median | Mean (SEM) | Median | Mean (SEM) | Median | |
| Olive oil (ml/d) | 15.4 (0.1) | 15.1 | 17.7 (0.2) * | 17.5 | 15.5 (0.2) | 15.5 | 13.5 (0.5) * | 13.7 |
| Vegetables (g/d) | 117 (1.0) | 114 | 137 (1.7) * | 137 | 128 (1.2) | 126 | 148 (3.3) * | 147 |
| Fruit (g/d) | 88.7 (2.1) | 88.3 | 122 (2.8) * | 121 | 106 (2.0) | 108 | 147 (6.1) * | 147 |
| Pulses (g/d) | 12.9 (0.1) | 12.8 | 13.3 (0.2) | 13.3 | 13.2 (0.1) | 13.3 | 13.4 (0.2) | 13.5 |
| Fish (g/d) | 37.8 (0.3) | 37.8 | 55.2 (0.5) * | 55.7 | 41.9 (0.2) | 42.0 | 80.4 (0.7) * | 80.7 |
| Bread (g/d) | 95.5 (1.8) | 90.9 | 96.7 (3.1) | 97.2 | 80.8 (1.6) | 78.8 | 79 (4.5) | 79.6 |
| Pasta (g/d) | 24.7 (0.8) | 23.9 | 23.8 (0.6) | 23.9 | 19.1 (0.2) | 19.3 | 15.5 (0.6) | 15.8 |
| Bakery products (g/d) | 48.3 (1.3) | 46.4 | 46.1 (2.3) | 46.7 | 41.1 (0.8) | 40.4 | 48.4 (2.4) | 48.8 |
| Sugar and sugary products (g/d) | 23.8 (0.3) | 23.5 | 20.8 (0.6) * | 20.7 | 24.0 (0.6) | 23.4 | 24.1 (1.8) | 24.3 |
| Milk (g/d) | 274 (2.8) | 267 | 247 (4.8) * | 248 | 208 (2.6) | 211 | 209 (7.8) | 215 |
| Cheese (g/d) | 16.0 (0.4) | 14.9 | 17.2 (0.6) | 17.1 | 15.0 (0.4) | 14.5 | 21.9 (0.9) * | 21.8 |
| Yoghurt and fermented milk (g/d) | 51.8 (1.3) | 53.2 | 73.3 (2.2) * | 74.9 | 50.2 (1.6) | 51.8 | 69.1 (4.8) * | 72.2 |
| Meats (g/d) | 105 (1.0) | 103 | 117 (1.5) * | 116 | 88.6 (1.2) | 88.7 | 79.4 (2.7) * | 79.5 |
| Cold and processed meats (g/d) | 59.4 (0.9) | 57.3 | 51.4 (1.6) | 51.6 | 48.7 (0.9) | 49.2 | 50.6 (2.9) | 51.9 |
| Water (g/d) | 582 (5.2) | 578 | 627 (9.3) * | 625 | 526 (0.8) | 527 | 629 (2.3) * | 630 |
| Sugared soft drinks (g/d) | 143 (3.8) | 138 | 98.1 (5.2) * | 91.4 | 95.6 (2.9) | 95.1 | 66.8 (6.8) * | 50.3 |
| Juices (g/d) | 115 (1.9) | 115 | 126 (3.5) * | 125 | 114 (1.9) | 111 | 159 (5.3) * | 160 |
| Sauces and dressings (g/d) | 15.4 (0.2) | 15.2 | 15.8 (0.4) | 15.8 | 14. (0.2) | 14.4 | 15.4 (0.7) | 15.7 |
| Variables | Children | Adolescents | ||||||
|---|---|---|---|---|---|---|---|---|
| PR | 95% C.I.PR | p | PR | 95% C.I.PR | p | |||
| Lower | Upper | Lower | Upper | |||||
| Gender | ||||||||
| Girls | 1 | 1 | ||||||
| Boys | 1.26 | 0.70 | 2.25 | NS | 1.79 | 0.85 | 3.76 | NS |
| Age | 0.92 | 0.72 | 1.18 | NS | 0.78 | 0.62 | 0.97 | 0.026 |
| Family Level of education | NS | NS | ||||||
| High | 1 | 1 | ||||||
| Secondary | 1.00 | 0.46 | 2.19 | NS | 0.67 | 0.26 | 1.17 | NS |
| Primary | 1.15 | 0.49 | 2.69 | NS | 0.52 | 0.19 | 1.43 | NS |
| SES | NS | NS | ||||||
| Mid-high-High | 1 | 1 | ||||||
| Mid | 0.88 | 0.42 | 1.87 | NS | 0.66 | 0.27 | 1.59 | NS |
| Mid-low-Low | 1.27 | 0.65 | 2.50 | NS | 1.88 | 0.87 | 4.06 | NS |
| Lifestyle pattern | ||||||||
| Healthier lifestyle patter | 1 | |||||||
| Unhealthier lifestyle pattern | 1.07 | 0.55 | 2.04 | NS | 2.00 | 0.82 | 4.86 | NS |
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Jackson-Leach, R.; Lobstein, T. Estimated burden of paediatric obesity and co-morbidities in Europe. Part 1. The increase in the prevalence of child obesity in Europe is itself increasing. Int. J. Pediatr. Obes. 2006, 1, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Organisation for Economic Co-Operation and Development. OECD Health Statistics 2014. Obesity Update. Available online: http://www.oecd.org/els/health-systems/Obesity-Update-2014.pdf (accessed on 10 June 2015).
- Kremers, S.P. Theory and practice in the study of influences on energy balance-related behaviors. Patient Educ. Couns. 2010, 79, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Brug, J.; Lien, N.; Klepp, K.I.; van Lenthe, F.J. Exploring overweight, obesity and their behavioural correlates among children and adolescents: Results from the Health-promotion through Obesity Prevention across Europe project. Public Health Nutr. 2010, 13, 1676–1679. [Google Scholar] [CrossRef] [PubMed]
- Pate, R.R.; O’Neill, J.R.; Liese, A.D.; Janz, K.F.; Granberg, E.M.; Colabianchi, N.; Harsha, D.W.; Condrasky, M.M.; O’Neil, P.M.; Lau, E.Y.; et al. Factors associated with development of excessive fatness in children and adolescents: A review of prospective studies. Obes. Rev. 2013, 14, 645–658. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Beydoun, M.A.; Wang, Y. Is sleep duration associated with childhood obesity? A systematic review and meta-analysis. Obesity 2008, 16, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.D.; Emmett, P.M.; Newby, P.K.; Northstone, K. Dietary patterns and changes in body composition in children between 9 and 11 years. Food Nutr. Res. 2014, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Appannah, G.; Pot, G.K.; Huang, R.C.; Oddy, W.H.; Beilin, L.J.; Mori, T.A.; Jebb, S.A.; Ambrosini, G.L. Identification of a dietary pattern associated with greater cardiometabolic risk in adolescence. Nutr. Metab. Cardiovasc. Dis. 2015, 25, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Ambrosini, G. Childhood dietary patterns and later obesity: A review of the evidence. Proc. Nutr. Soc. 2014, 73, 137–146. [Google Scholar] [CrossRef] [PubMed]
- Gubbels, J.S.; van Assema, P.; Kremers, S.P.J. Physical Activity, Sedentary Behavior, and Dietary Patterns among Children. Curr. Nutr. Rep. 2013, 2, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Mikkilä, V.; Räsänen, L.; Raitakari, O.T.; Pietinen, P.; Viikari, J. Consistent dietary patterns identified from childhood to adulthood: The cardiovascular risk in Young Finns Study. Br. J. Nutr. 2005, 93, 923–931. [Google Scholar] [CrossRef] [PubMed]
- Shin, K.O.; Oh, S.Y.; Park, H.S. Empirically derived major dietary patterns and their associations with overweight in Korean preschool children. Br. J. Nutr. 2007, 98, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Lioret, S.; Touvier, M.; Lafay, L.; Volatier, J.L.; Maire, B. Dietary and physical activity patterns in French children are related to overweight and socioeconomic status. J. Nutr. 2008, 138, 101–107. [Google Scholar] [PubMed]
- Craig, L.C.; McNeill, G.; Macdiarmid, J.I.; Masson, L.F.; Holmes, B.A. Dietary patterns of school-age children in Scotland: Association with socio-economic indicators, physical activity and obesity. Br. J. Nutr. 2010, 103, 319–334. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, L.D.; Spector, P.; Stevens, M.J.; Schmidt, M.M.; Schreiber, G.B.; Striegel-Moore, R.H.; Wang, M.C.; Crawford, P.B. Dietary patterns in adolescence are related to adiposity in young adulthood in black and white females. J. Nutr. 2007, 137, 399–406. [Google Scholar] [PubMed]
- McNaughton, S.A.; Ball, K.; Mishra, G.D.; Crawford, D.A. Dietary patterns of adolescents and risk of obesity and hypertension. J. Nutr. 2008, 138, 364–370. [Google Scholar] [PubMed]
- Aranceta, J.; Perez-Rodrigo, C.; Ribas, L.; Serra-Majem, L. Sociodemographic and lifestyle determinants of food patterns in Spanish children and adolescents: The enKid study. Eur. J. Clin. Nutr. 2003, 57, S40–S44. [Google Scholar] [CrossRef] [PubMed]
- Leech, R.M.; McNaughton, S.A.; Timperio, A. The clustering of diet, physical activity and sedentary behavior in children and adolescents: A review. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 4. [Google Scholar] [CrossRef] [PubMed]
- Pronk, N.P.; Anderson, L.H.; Crain, A.L.; Martinson, B.C.; O’Connor, P.J.; Sherwood, N.E.; Whitebird, R.R. Meeting recommendations for multiple healthy lifestyle factors. Prevalence, clustering, and predictors among adolescent, adult, and senior health plan members. Am. J. Prev. Med. 2004, 27, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Boone-Heinonen, J.; Gordon-Larsen, P.; Adair, L.S. Obesogenic clusters: Multidimensional adolescent obesity-related behaviors in the U.S. Ann. Behav. Med. 2008, 36, 217–230. [Google Scholar] [CrossRef] [PubMed]
- Huh, J.; Riggs, N.R.; Spruijt-Metz, D.; Chou, C.P.; Huang, Z.; Pentz, M. Identifying patterns of eating and physical activity in children: A latent class analysis of obesity risk. Obesity 2011, 19, 652–658. [Google Scholar] [CrossRef] [PubMed]
- Cameron, A.J.; Crawford, D.A.; Salmon, J.; Campbell, K.; McNaughton, S.A.; Mishra, G.D.; Ball, K. Clustering of obesity-related risk behaviors in children and their mothers. Ann. Epidemiol. 2011, 21, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Gubbels, J.S.; Kremers, S.P.; Stafleu, A.; Goldbohm, R.A.; de Vries, N.K.; Thijs, C. Clustering of energy balance-related behaviors in 5-year-old children: Lifestyle patterns and their longitudinal association with weight status development in early childhood. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 77. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, J.J.; Prochaska, J.O. A Review of Multiple Health Behavior Change Interventions for Primary Prevention. Am. J. Lifestyle Med. 2011, 5. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, E.; Ávila, J.M.; Castillo, A.; Valero, T.; del Pozo, S.; Rodriguez, P.; Aranceta Bartrina, J.; Gil, A.; González-Gross, M.; Ortega, R.M.; et al. The ANIBES Study on Energy Balance in Spain: Design, protocol and methodology. Nutrients 2015, 7, 970–998. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, E.; Ávila, J.M.; Valero, T.; del Pozo, S.; Rodriguez, P.; Aranceta-Bartrina, J.; Gil, A.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; et al. Energy Intake, Profile, and Dietary Sources in the Spanish Population: Findings of the ANIBES Study. Nutrients 2015, 7, 4739–4762. [Google Scholar] [CrossRef] [PubMed]
- Moreiras, O.; Carbajal, A.; Cabrera, L.; Cuadrado, C. Tablas de Composición de Alimentos, 15th ed.; Pirámide: Madrid, Spain, 2011. [Google Scholar]
- Hagströmer, M.; Bergman, P.; de Bourdeaudhuij, I.; Ortega, F.B.; Ruiz, J.R.; Manios, Y.; Rey-López, J.P.; Phillipp, K.; von Berlepsch, J.; Sjöström, M.; et al. Concurrent validity of a modified version of the International Physical Activity Questionnaire (IPAQ-A) in European adolescents: The HELENA Study. Int. J. Obes. 2008, 32, S42–S48. [Google Scholar] [CrossRef] [PubMed]
- IPAQ. Guidelines for Data Processing and Analysis of the International Physical Activity Questionnaire (IPAQ) — Short and Long Forms, November 2005. Available online: https://sites.google.com/site/theipaq/scoring-protocol (accessed on 27 October 2015).
- Bauman, A.; Ainsworth, B.E.; Bull, F.; Craig, C.L.; Hagströmer, M.; Sallis, J.F.; Pratt, M.; Sjöström, M. Progress and Pitfalls in the Use of the International Physical Activity Questionnaire (IPAQ) for Adult Physical Activity Surveillance. J. Phys. Act. Health 2009, 6 (Suppl. 1), S5–S8. [Google Scholar] [PubMed]
- Hense, S.; Pohlabeln, H.; de Henauw, S.; Eiben, G.; Molnar, D.; Moreno, L.A.; Barba, G.; Hadjigeorgiou, C.; Veidebaum, T.; Ahrens, W. Sleep duration and overweight in European children: Is the association modified by geographic region? Sleep 2011, 34, 885–890. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Alvira, J.M.; de Bourdeaudhuij, I.; Singh, A.S.; Vik, F.N.; Manios, Y.; Kovacs, E.; Jan, N.; Brug, J.; Moreno, L.A. Clustering of energy balance-related behaviors and parental education in European children: The ENERGY-project. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marfell-Jones, M.; Olds, T.; Stewart, A.; Carter, L. International Standards for Anthropometric Assessment; International Society for the Advancement of Kinanthropometry: Potchefstroom, South Africa, 2006; pp. 1–137. [Google Scholar]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [PubMed]
- Newby, P.K.; Tucker, K.L. Empirically derived eating patterns using factor or cluster analysis: A review. Nutr. Rev. 2004, 62, 177–203. [Google Scholar] [CrossRef] [PubMed]
- Everitt, B.S.; Landau, S.; Leese, M.; Stahl, D. Cluster Analysis, 5th ed.; John Wiley & Sons, Ltd.: West Sussex, UK, 2011. [Google Scholar]
- Shang, X.; Li, Y.; Liu, A.; Zhang, Q.; Hu, X.; Du, S.; Ma, J.; Xu, G.; Li, Y.; Guo, H.; et al. Dietary pattern and its association with the prevalence of obesity and related cardiometabolic risk factors among Chinese children. PLoS ONE 2012, 7, e43183. [Google Scholar] [CrossRef] [PubMed]
- Diethelm, K.; Günther, A.L.; Schulze, M.B.; Standl, M.; Heinrich, J.; Buyken, A.E. Prospective relevance of dietary patterns at the beginning and during the course of primary school to the development of body composition. Br. J. Nutr. 2014, 111, 1488–1498. [Google Scholar] [CrossRef] [PubMed]
- Gubbels, J.; Kremers, S.; Goldbohm, A.; Stafleu, A.; Thijs, C. Energy balance-related behavioral patterns in 5-year-old children and the longitudinal association with weight status development in early childhood. Public Health Nutr. 2012, 15, 1402–1410. [Google Scholar] [CrossRef] [PubMed]
- Ambrosini, G.L.; Emmett, P.M.; Northstone, K.; Howe, L.D.; Tilling, K.; Jebb, S.A. Identification of a dietary pattern prospectively associated with increased adiposity during childhood and adolescence. Int. J. Obes. 2012, 36, 1299–1305. [Google Scholar] [CrossRef] [PubMed]
- Van der Sluis, M.E.; Lien, N.; Twisk, J.W.; Steenhuis, I.H.; Bere, E.; Klepp, K.I.; Wind, M. Longitudinal associations of energy balance-related behaviours and cross-sectional associations of clusters and body mass index in Norwegian adolescents. Public Health Nutr. 2011, 13, 1716–1721. [Google Scholar] [CrossRef] [PubMed]
- Appannah, G.; Pot, G.K.; O’Sullivan, T.A.; Oddy, W.H.; Jebb, S.A.; Ambrosini, G.L. The reliability of an adolescent dietary pattern identified using reduced-rank regression: Comparison of a FFQ and 3 d food record. Br. J. Nutr. 2014, 112, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Yannakoulia, M.; Ntalla, I.; Papoutsakis, C.; Farmaki, A.E.; Dedoussis, G.V. Consumption of vegetables, cooked meals, and eating dinner is negatively associated with overweight status in children. J. Pediatr. 2011, 157, 815–820. [Google Scholar] [CrossRef] [PubMed]
- Sabbe, D.; de Bourdeaudhuij, I.; Legiest, E.; Maes, L. A cluster analytical approach towards physical activity and eating habits among 10-year-old children. Health Educ. Res. 2008, 23, 753–762. [Google Scholar] [CrossRef] [PubMed]
- Ottevaere, C.; Huybrechts, I.; Benser, J.; de Bourdeaudhuij, I.; Cuenca-Garcia, M.; Dallongeville, J.; Zaccaria, M.; Gottrand, F.; Kersting, M.; Rey-López, J.P.; et al. Clustering patterns of physical activity, sedentary and dietary behavior among European adolescents: The HELENA study. BMC Public Health 2011, 11, 328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Te Velde, S.J.; de Bourdeaudhuij, I.; Thorsdottir, I.; Rasmussen, M.; Hagstromer, M.; Klepp, K.I.; Brug, J. Patterns in sedentary and exercise behaviors and associations with overweight in 9–14-year-old boys and girls—A cross-sectional study. BMC Public Health 2007, 7, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seghers, J.; Rutten, C. Clustering of multiple lifestyle behaviours and its relationship with weight status and cardiorespiratory fitness in a sample of Flemish 11- to 12-year-olds. Public Health Nutr. 2010, 13, 1838–1846. [Google Scholar] [CrossRef] [PubMed]
- Marshall, S.J.; Biddle, S.J.H.; Sallis, J.F.; McKenzie, T.L.; Conway, T.L. Clustering of sedentary behaviors and physical activity among youth: A cross-national study. Pediatr. Exerc. Sci. 2002, 14, 401–417. [Google Scholar]
- Aranceta-Bartrina, J.; Pérez-Rodrigo, C.; Santolaya-Jiménez, J.; Juan Gondra Rezola y Grupo Colaborativo Para el Estudio Perseo en Bilbao. El Proyecto PERSEO en Bilbao: Evaluación preliminar. Rev. Esp. Nutr. Comunitaria 2013, 19, 88–97. [Google Scholar]
- Kautiainen, S.; Koivusilta, L.; Lintonen, T.; Virtanen, S.M.; Rimpela, A. Use of information and communication technology and prevalence of overweight and obesity among adolescents. Int. J. Obes. 2005, 29, 925–933. [Google Scholar] [CrossRef] [PubMed]
- Jago, R.; Anderson, C.B.; Baranowski, T.; Watson, K. Adolescent patterns of physical activity: Differences by gender, day, and time of day. Am. J. Prev. Med. 2005, 28, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Spengler, S.; Mess, F.; Schmocker, E.; Woll, A. Longitudinal associations of health-related behavior patterns in adolescence with change of weight status and self-rated health over a period of 6 years: Results of the MoMo longitudinal study. BMC Pediatr. 2014, 14, 242. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; Emmett, P.; Newby, P.K.; Northstone, K. Dietary patterns obtained through principal components analysis: The effect of input variable quantification. Br. J. Nutr. 2013, 109, 1881–1891. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Rodrigo, C.; Gil, Á.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; Aranceta-Bartrina, J. Clustering of Dietary Patterns, Lifestyles, and Overweight among Spanish Children and Adolescents in the ANIBES Study. Nutrients 2016, 8, 11. https://doi.org/10.3390/nu8010011
Pérez-Rodrigo C, Gil Á, González-Gross M, Ortega RM, Serra-Majem L, Varela-Moreiras G, Aranceta-Bartrina J. Clustering of Dietary Patterns, Lifestyles, and Overweight among Spanish Children and Adolescents in the ANIBES Study. Nutrients. 2016; 8(1):11. https://doi.org/10.3390/nu8010011
Chicago/Turabian StylePérez-Rodrigo, Carmen, Ángel Gil, Marcela González-Gross, Rosa M. Ortega, Lluis Serra-Majem, Gregorio Varela-Moreiras, and Javier Aranceta-Bartrina. 2016. "Clustering of Dietary Patterns, Lifestyles, and Overweight among Spanish Children and Adolescents in the ANIBES Study" Nutrients 8, no. 1: 11. https://doi.org/10.3390/nu8010011
APA StylePérez-Rodrigo, C., Gil, Á., González-Gross, M., Ortega, R. M., Serra-Majem, L., Varela-Moreiras, G., & Aranceta-Bartrina, J. (2016). Clustering of Dietary Patterns, Lifestyles, and Overweight among Spanish Children and Adolescents in the ANIBES Study. Nutrients, 8(1), 11. https://doi.org/10.3390/nu8010011