Fluid Intake of Pregnant and Breastfeeding Women in Indonesia: A Cross-Sectional Survey with a Seven-Day Fluid Specific Record

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
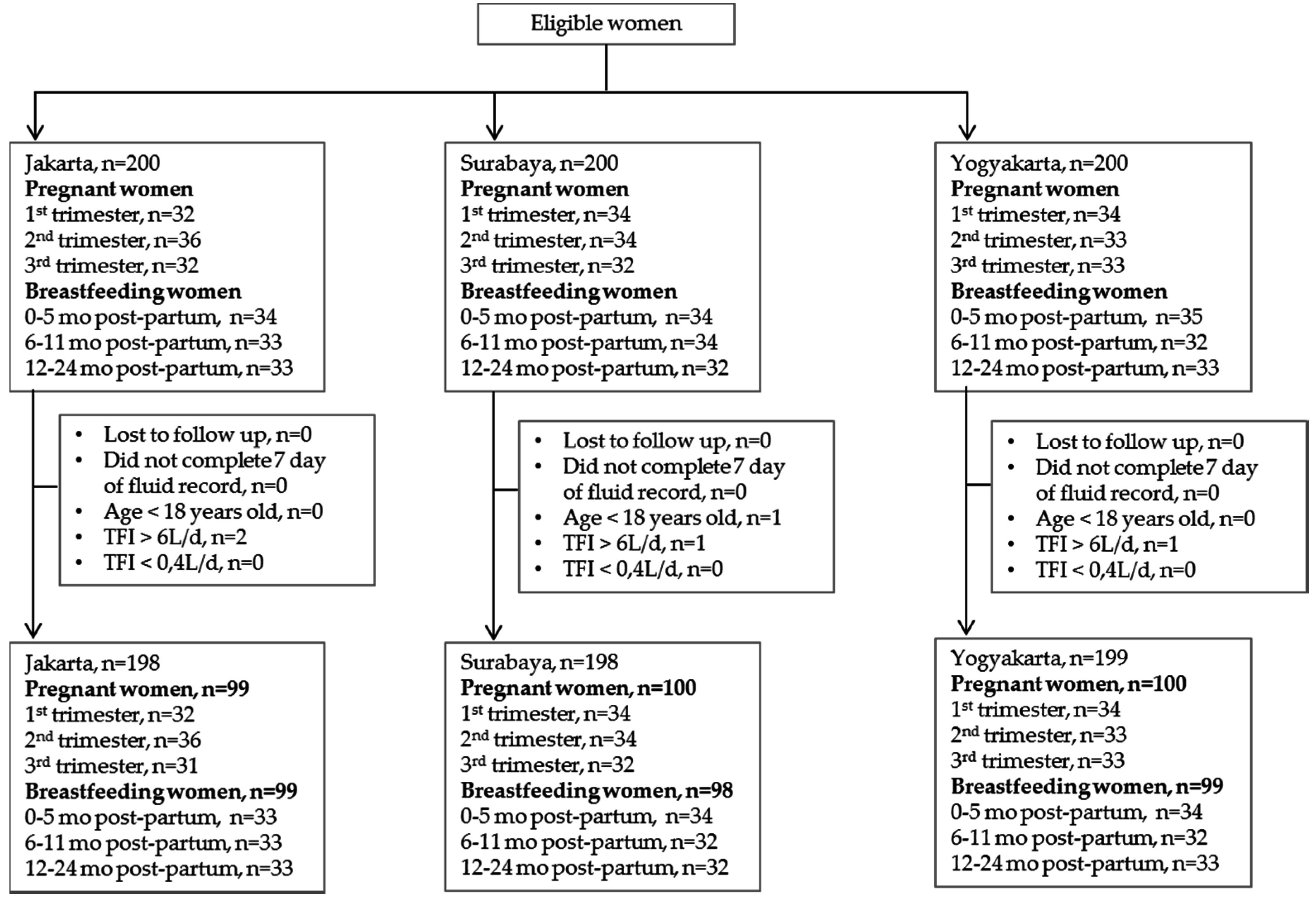
2.1. Survey Sampling and Protocol
2.2. Assessment of Fluid Intake with a Seven-Day Fluid Specific Record
2.3. Knowlegde on Fluid Intake Recommendation
- ○
- Minimally 600 cc less than recommended for non-pregnant woman
- ○
- Minimally 300 cc less than recommended for non-pregnant woman
- ○
- As recommended for non-pregnant woman
- ○
- Minimally 300 cc more than the non-pregnant recommendation
- ○
- Minimally 600 cc more than the non-pregnant recommendation
- ○
- Others: _______________________________________________
2.4. Data Management and Analysis
3. Results
3.1. Total Fluid Intake
3.2. Adherence to Indonesian Adequate Intake for Water from Fluids
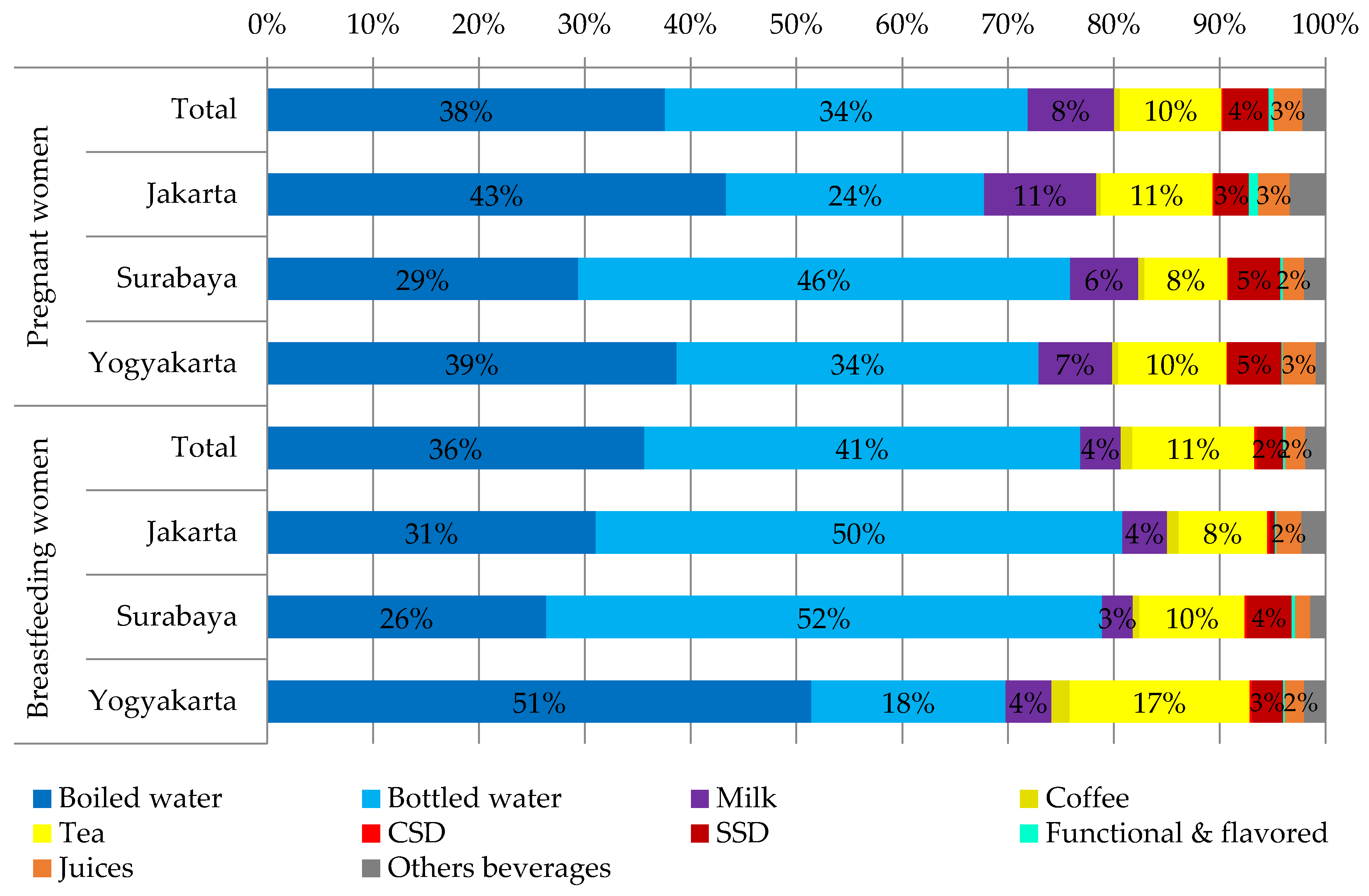
3.3. Consumption of Different Fluid Types
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Hytten, F.E.; Chamberlain, G. Clinical Pysiology in Obstetrics; Blackwell Scientific Publications: Oxford, UK, 1991. [Google Scholar]
- Larciprete, G.; Valensise, H.; Vasapollo, B.; Altomare, F.; Sorge, R.; Casalino, B.; De Lorenzo, A.; Arduini, D. Body composition during normal pregnancy: Reference ranges. Acta Diabetol. 2003, 40 (Suppl. S1), S225–S232. [Google Scholar] [CrossRef] [PubMed]
- Butte, N.F.; Ellis, K.J.; Wong, W.W.; Hopkinson, J.M.; Smith, E.O. Composition of gestational weight gain impacts maternal fat retention and infant birth weight. Am. J. Obstet. Gynecol. 2003, 189, 1423–1432. [Google Scholar] [CrossRef]
- Beall, M.H.; van den Wijngaard, J.P.; van Gemert, M.J.; Ross, M.G. Amniotic fluid water dynamics. Placenta 2007, 28, 816–823. [Google Scholar] [CrossRef] [PubMed]
- Santillan, M.K.; Santillan, D.A.; Scroggins, S.M.; Min, J.Y.; Sandgren, J.A.; Pearson, N.A.; Leslie, K.K.; Hunter, S.K.; Zamba, G.K.; Gibson-Corley, K.N.; et al. Vasopressin in preeclampsia: A novel very early human pregnancy biomarker and clinically relevant mouse model. Hypertension 2014, 64, 852–859. [Google Scholar] [CrossRef] [PubMed]
- Schnarr, J.; Smaill, F. Asymptomatic bacteriuria and symptomatic urinary tract infections in pregnancy. Eur. J. Clin. Investig. 2008, 38 (Suppl. S2), 50–57. [Google Scholar] [CrossRef] [PubMed]
- Eckford, S.D.; Keane, D.P.; Lamond, E.; Jackson, S.R.; Abrams, P. Hydration monitoring in the prevention of recurrent idiopathic urinary tract infections in pre-menopausal women. Br. J. Urol. 1995, 76, 90–93. [Google Scholar] [CrossRef] [PubMed]
- Cullen, G.; O’Donoghue, D. Constipation and pregnancy. Best Pract. Res. Clin. Gastroenterol. 2007, 21, 807–818. [Google Scholar] [CrossRef] [PubMed]
- Neville, M.C.; Keller, R.; Seacat, J.; Lutes, V.; Neifert, M.; Casey, C.; Allen, J.; Archer, P. Studies in human lactation: Milk volumes in lactating women during the onset of lactation and full lactation. Am. J. Clin. Nutr. 1988, 48, 1375–1386. [Google Scholar] [PubMed]
- Bauer, J.; Gerss, J. Longitudinal analysis of macronutrients and minerals in human milk produced by mothers of preterm infants. Clin. Nutr. 2011, 30, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Nutrition during Lactation; National Academies Press: Washington, DC, USA, 1991. [Google Scholar]
- Martinez, H. Fluid consumption by Mexican women during pregnancy and first semester of lactation. Biomed. Res. Int. 2014, 2014, 603282. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine; Food and Nutrition Board. Dietary Reference Intakes for Water, Potassium, Sodium, Chloride and Sulfate; National Academies Press: Washington, DC, USA, 2004. [Google Scholar]
- EFSA Panel on Dietetic Products Nutrition and Allergies (NDA). Scientific opinion on dietary reference values for water. EFSA J. 2010, 8, 1459. [Google Scholar]
- Ministry of Health of the Republic of Indonesia. Recommended Nutritional Intake for Indonesian Population; Ministry of Health: Jakarta, Indonesia, 2013.
- Ferreira-Pego, C.; Guelinckx, I.; Moreno, L.A.; Kavouras, S.A.; Gandy, J.; Martinez, H.; Bardosono, S.; Abdollahi, M.; Nasseri, E.; Jarosz, A.; et al. Total fluid intake and its determinants: Cross-sectional surveys among adults in 13 countries worldwide. Eur. J. Nutr. 2015, 54 (Suppl. S2), 35–43. [Google Scholar] [CrossRef] [PubMed]
- Guelinckx, I.; Ferreira-Pego, C.; Moreno, L.A.; Kavouras, S.A.; Gandy, J.; Martinez, H.; Bardosono, S.; Abdollahi, M.; Nasseri, E.; Jarosz, A.; et al. Intake of water and different beverages in adults across 13 countries. Eur. J. Nutr. 2015, 54 (Suppl. S2), S45–S55. [Google Scholar] [CrossRef] [PubMed]
- Malisova, O.; Protopappas, A.; Nyktari, A.; Bountziouka, V.; Antsaklis, A.; Zampelas, A.; Kapsokefalou, M. Estimations of water balance after validating and administering the water balance questionnaire in pregnant women. Int. J. Food Sci. Nutr. 2014, 65, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Malisova, O.; Bountziouka, V.; Panagiotakos, D.; Zampelas, A.; Kapsokefalou, M. Evaluation of seasonality on total water intake, water loss and water balance in the general population in Greece. J. Hum. Nutr. Diet. 2013, 26 (Suppl. S1), 90–96. [Google Scholar] [CrossRef] [PubMed]
- Gandy, J. Water intake: Validity of population assessment and recommendations. Eur. J. Nutr. 2015, 54 (Suppl. S2), 11–16. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, A.L.; Munoz, C.X.; Ellis, L.A.; Perrier, E.T.; Guelinckx, I.; Klein, A.; Kavouras, S.A.; Armstrong, L.E. Urine color as an indicator of urine concentration in pregnant and lactating women. Eur. J. Nutr. 2015. [Google Scholar] [CrossRef] [PubMed]
- Health Research and Development; Ministry of Health Republic of Indonesia. Total Diet Study: Food Consumption Survey of Indonesian Individual; Ministry of Health: Jakarta, Indonesia, 2014.
- Zheng, J. Molecular mechanism of TRP channels. Compr. Physiol. 2013, 3, 221–242. [Google Scholar] [PubMed]
- Gomez, P.; Boesen-Mariani, S.; Lambert, J.L.; Monrozier, R. A water intervention program to improve fluid intakes among french women. Nutr. Today 2013, 48, S40–S42. [Google Scholar] [CrossRef]
- Lahlou, S.; Boesen-Mariani, S.; Franks, B.; Guelinckx, I. Increasing water intake of children and parents in the family setting: A randomized controlled intervention using installation theory. Ann. Nutr. Metab. 2015, 66, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Storckdieck Gennant Bonsmann, S.; Mak, N.T.; Louro Caldeira, S.; Wollgast, J. How to Promote Water Intake in Schools: A Toolkit; Publications Office of the European Union: Luxembourg, 2016. [Google Scholar]
- Huang, T.T.; Drewnowski, A.; Kumanyika, S.K.; Glass, T.A. A systems-oriented multilevel framework for addressing obesity in the 21st century. Prev. Chronic Dis. 2009, 6, A82. [Google Scholar] [PubMed]
- Phelan, S. Pregnancy: A “teachable moment” for weight control and obesity prevention. Am. J. Obstet. Gynecol. 2010, 202, 135.e1–135.e8. [Google Scholar] [CrossRef] [PubMed]
- Coulston, A.M.; Boushey, C.J. Nutrition in the Prevention and Treatment of Disease; Academic Press: Amsterdam, The Netherlands, 2008. [Google Scholar]
- Gandy, J.; Martinez, H.; Guelinckx, I.; Moreno, L.A.; Bardosono, S.; Salas-Salvado, J.; Kavouras, S.A. Relevance of assessment methods for fluid intake. Ann. Nutr. Metab. 2016, 68 (Suppl. S2), 1–5. [Google Scholar] [CrossRef] [PubMed]
- Bardosono, S.; Monrozier, R.; Permadhi, I.; Manikam, N.R.; Pohan, R.; Guelinckx, I. Total fluid intake assessed with a seven-day fluid record versus a 24-h dietary recall: A crossover study in Indonesian adolescents and adults. Eur. J. Nutr. 2015, 54 (Suppl. S2), 17–25. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Total | Jakarta | Surabaya | Yogyakarta |
|---|---|---|---|---|
| Age (years) | ||||
| Pregnant women | 28.5 (4.3) | 29.2 (4.4) | 28.5 (4.1) | 27.8 (4.3) |
| Breastfeeding women | 28.6 (4.0) | 28.9 (4.2) | 28.5 (3.9) | 28.5 (3.8) |
| Education Level | ||||
| None | 4 (1) | 0 (0) | 1 (1) | 3 (2) |
| Elementary school | 41 (7) | 20 (10) | 14 (7) | 7 (4) |
| Junior high school | 109 (18) | 38 (19) | 33 (17) | 38 (19) |
| Senior high school | 335 (56) | 117 (59) | 103 (52) | 115 (58) |
| Higher education | 106 (18) | 23 (12) | 47 (24) | 36 (18) |
| Working Status | ||||
| Any job | 3 (1) | 1 (1) | 2 (1) | 0 (0) |
| Housewife | 428 (72) | 159 (80) | 133 (67) | 136 (68) |
| College student | 2 (0) | 0 (0) | 0 (0) | 2 (1) |
| Labor | 4 (1) | 2 (1) | 1 (1) | 1 (1) |
| Service | 5 (1) | 2 (1) | 1 (1) | 2 (1) |
| Para/medical profession | 20 (2) | 0 (0) | 10 (5) | 0 (0) |
| Education | 5 (1) | 1 (1) | 2 (1) | 2 (1) |
| Finance/Business | 29 (5) | 6 (3) | 7 (4) | 16 (8) |
| Government employment | 10 (2) | 3 (2) | 3 (2) | 4 (2) |
| Private sector employment | 98 (16) | 24 (12) | 39 (20) | 35 (18) |
| Other | 1 (0) | 0 (0) | 0 (0) | 1 (1) |
| BMI Categories | ||||
| Pregnant women 1 | ||||
| Underweight | 13 (4) | 2 (2) | 2 (2) | 9 (9) |
| Normal weight | 134 (45) | 37 (37) | 47 (47) | 50 (50) |
| Overweight | 110 (37) | 37 (37) | 41 (41) | 32 (32) |
| Obese | 42 (14) | 23 (23) | 10 (10) | 9 (9) |
| Breastfeeding women | ||||
| Underweight | 25 (8) | 8 (8) | 6 (6) | 11 (11) |
| Normal weight | 160 (54) | 53 (54) | 53 (54) | 54 (55) |
| Overweight | 76 (26) | 29 (29) | 25 (26) | 22 (22) |
| Obese | 35 (12) | 9 (9) | 14 (14) | 12 (12) |
| Total Fluid Intake | n (%) | Mean (SD) | Percentiles | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 5 | 10 | 25 | 50 | 75 | 90 | 95 | |||
| Pregnant Women | |||||||||
| Total | 299 (100) | 2332 (746) | 1243 | 1436 | 1784 | 2229 | 2800 | 3307 | 3679 |
| Jakarta | 99 (33) | 2666 (681) | 1529 | 1784 | 2191 | 2721 | 3045 | 3643 | 3871 |
| Surabaya | 100 (33) | 2153 (732) | 1179 | 1343 | 1666 | 2000 | 2609 | 3298 | 3444 |
| Yogyakarta | 100 (33) | 2181 (717) | 1133 | 1441 | 1645 | 2039 | 2635 | 3129 | 3615 |
| Underweight | 13 (4) | 1925 (535) | 1129 | 1174 | 1607 | 1894 | 2195 | 2920 | 3119 |
| Normal Weight | 134 (45) | 2210 (706) | 1167 | 1416 | 1691 | 2129 | 2726 | 3142 | 3413 |
| Overweight | 110 (37) | 2477 (771) | 1315 | 1441 | 1876 | 2476 | 3053 | 3493 | 3857 |
| Obesity | 42 (14) | 2469 (763) | 1350 | 1606 | 1940 | 2356 | 2853 | 3567 | 4176 |
| Housewife | 186 (62) | 2397 (779) | 1183 | 1471 | 1795 | 2330 | 2900 | 3363 | 3861 |
| Other occupation | 113 (38) | 2226 (678) | 1272 | 1407 | 1726 | 2163 | 2693 | 3216 | 3473 |
| Senior high school | 163 (55) | 2305 (751) | 1226 | 1401 | 1750 | 2161 | 2833 | 3326 | 3580 |
| Other educational level | 136 (45) | 2365 (740) | 1313 | 1474 | 1837 | 2279 | 2791 | 3313 | 3850 |
| Breastfeeding Women | |||||||||
| Total | 296 (100) | 2525 (843) | 1491 | 1654 | 1971 | 2306 | 2901 | 3697 | 4357 |
| Jakarta | 99 (33) | 2722 (897) | 1463 | 1670 | 2024 | 2507 | 3240 | 3969 | 4581 |
| Surabaya | 100 (33) | 2573 (899) | 1599 | 1675 | 1952 | 2276 | 2979 | 3800 | 4404 |
| Yogyakarta | 99 (33) | 2280 (656) | 1476 | 1597 | 1907 | 2151 | 2476 | 3219 | 3519 |
| Underweight | 25 (8) | 2430 (927) | 1368 | 1460 | 1873 | 2266 | 2691 | 3559 | 5194 |
| Normal Weight | 160 (54) | 2450 (778) | 1582 | 1638 | 1910 | 2281 | 2777 | 3519 | 3942 |
| Overweight | 76 (26) | 2655 (922) | 1395 | 1647 | 2046 | 2438 | 3128 | 3840 | 4687 |
| Obesity | 35 (12) | 2653 (871) | 1718 | 1866 | 2000 | 2318 | 2957 | 4210 | 4643 |
| Housewife | 242 (82) | 2530 (873) | 1481 | 1638 | 1949 | 2285 | 2975 | 3764 | 4377 |
| Other occupation | 54 (18) | 2500 (697) | 1619 | 1724 | 2094 | 2410 | 2676 | 3324 | 3879 |
| Senior high school | 172 (58) | 2522 (804) | 1550 | 1661 | 1963 | 2306 | 2956 | 3709 | 4257 |
| Other educational Level | 124 (42) | 2529 (897) | 1433 | 1624 | 1979 | 2319 | 2825 | 3725 | 4396 |
| How Much Water Should a Pregnant Woman Drink Daily? | How Much Water Should a Breastfeeding Woman Drink Daily? | ||
|---|---|---|---|
| Total women | Incorrect answer | 514 (86) | 455 (77) |
| Correct answer | 81 (14) | 140 (23) | |
| Pregnant women | Incorrect answer | 252 (84) | 240 (80) |
| Correct answer | 47 (16) | 59 (20) | |
| Breastfeeding women | Incorrect answer | 262 (88) | 215 (73) |
| Correct answer | 34 (12) | 81 (17) |
| Pregnant Women (n = 299) | Breastfeeding Women (n = 296) | |||||||
|---|---|---|---|---|---|---|---|---|
| Total | Jakarta | Surabaya | Yogyakarta | Total | Jakarta | Surabaya | Yogyakarta | |
| Water | 1676 (737) | 1806 (681) | 1633 (755) | 1590 (761) | 1939 (885) | 2199 (922) | 2029 (904) | 1591 (707) |
| Boiled water | 877 (880) | 1156 (912) | 633 (780) | 844 (872) | 900 (1028) | 845 (1173) | 679 (961) | 1173 (875) |
| Bottled water | 799 (895) | 650 (808) | 1001 (1000) | 746 (837) | 1040 (1109) | 1354 (1130) | 1351 (1174) | 418 (686) |
| Milk | 191 (181) | 282 (213) | 139 (142) | 152 (143) | 97 (142) | 116 (146) | 75 (124) | 99 (151) |
| Hot bev. | 237 (199) | 293 (195) | 181 (186) | 236 (202) | 319 (275) | 257 (204) | 271 (243) | 427 (329) |
| Coffee | 12 (46) | 12 (44) | 12 (47) | 13 (47) | 28 (69) | 30 (68) | 16 (52) | 39 (83) |
| Tea | 224 (188) | 281 (186) | 169 (171) | 223 (191) | 290 (256) | 227 (190) | 256 (237) | 388 (302) |
| Soft drinks | 115 (141) | 115 (139) | 113 (147) | 116 (138) | 74 (116) | 24 (61) | 123 (150) | 76 (96) |
| CSD | 3 (13) | 6 (19) | 2 (9) | 2 (9) | 6 (22) | 7 (29) | 6 (18) | 5 (17) |
| SSD | 101 (126) | 86 (96) | 105 (143) | 112 (133) | 62 (104) | 13 (38) | 108 (135) | 66 (94) |
| Functional & flavored drinks | 11 (38) | 23 (60) | 6 (19) | 2 (15) | 6 (24) | 4 (21) | 9 (32) | 5 (17) |
| Juices | 63 (85) | 80 (94) | 43 (74) | 68 (82) | 47 (93) | 64 (107) | 37 (83) | 41 (87) |
| Other bev. | 51 (90) | 90 (123) | 43 (74) | 20 (38) | 48 (83) | 62 (90) | 37 (78) | 46 (78) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bardosono, S.; Prasmusinto, D.; Hadiati, D.R.; Purwaka, B.T.; Morin, C.; Pohan, R.; Sunardi, D.; Chandra, D.N.; Guelinckx, I. Fluid Intake of Pregnant and Breastfeeding Women in Indonesia: A Cross-Sectional Survey with a Seven-Day Fluid Specific Record. Nutrients 2016, 8, 651. https://doi.org/10.3390/nu8110651
Bardosono S, Prasmusinto D, Hadiati DR, Purwaka BT, Morin C, Pohan R, Sunardi D, Chandra DN, Guelinckx I. Fluid Intake of Pregnant and Breastfeeding Women in Indonesia: A Cross-Sectional Survey with a Seven-Day Fluid Specific Record. Nutrients. 2016; 8(11):651. https://doi.org/10.3390/nu8110651
Chicago/Turabian StyleBardosono, Saptawati, Damar Prasmusinto, Diah R. Hadiati, Bangun T. Purwaka, Clementine Morin, Rizki Pohan, Diana Sunardi, Dian N. Chandra, and Isabelle Guelinckx. 2016. "Fluid Intake of Pregnant and Breastfeeding Women in Indonesia: A Cross-Sectional Survey with a Seven-Day Fluid Specific Record" Nutrients 8, no. 11: 651. https://doi.org/10.3390/nu8110651
APA StyleBardosono, S., Prasmusinto, D., Hadiati, D. R., Purwaka, B. T., Morin, C., Pohan, R., Sunardi, D., Chandra, D. N., & Guelinckx, I. (2016). Fluid Intake of Pregnant and Breastfeeding Women in Indonesia: A Cross-Sectional Survey with a Seven-Day Fluid Specific Record. Nutrients, 8(11), 651. https://doi.org/10.3390/nu8110651