Association between Parent and Child Dietary Sodium and Potassium Intakes as Assessed by 24-h Urinary Excretion

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection and Measures
2.2.1. Demographic Characteristics
2.2.2. 24-h Urine Collection
2.3. Urine Analyses
2.4. Potential under/over Collections: 24-h Urine Samples
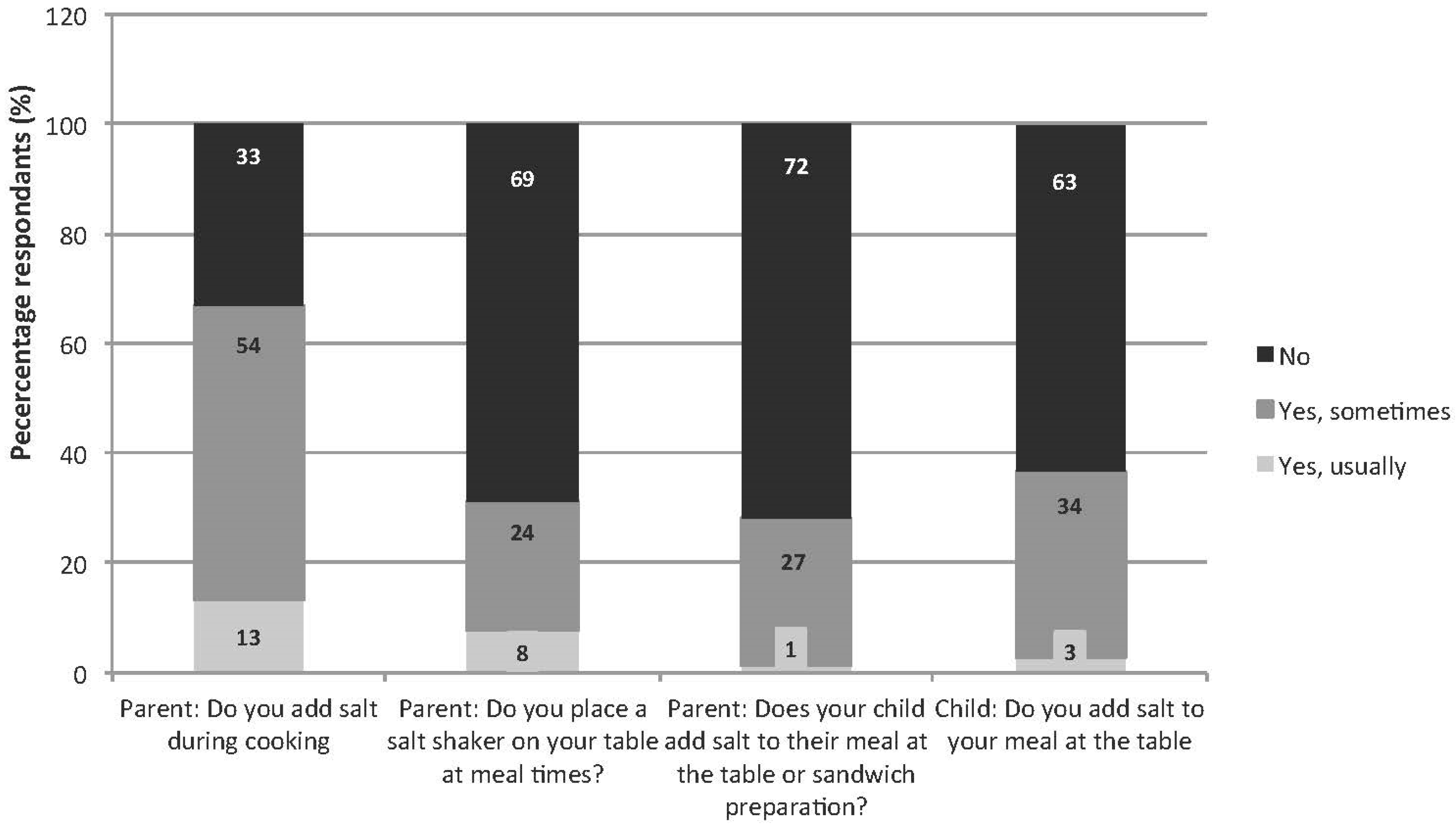
Discretionary Salt Use
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| 24hUE | 24-h urinary excretion |
| BMI | body mass index |
| CV | coefficient of variation |
| CVD | cardiovascular disease |
| IOFT | International Obesity Taskforce |
| K | potassium |
| Na | sodium |
| SD | standard deviation |
| SEM | standard error of the mean |
| SONIC | Salt and Other Nutrient Intakes in Children |
References
- Aaron, K.J.; Sanders, P.W. Role of dietary salt and potassium intake in cardiovascular health and disease: A review of the evidence. Mayo Clin. Proc. 2013, 88, 987–995. [Google Scholar] [CrossRef] [PubMed]
- Aburto, N.J.; Hanson, S.; Gutierrez, H.; Hooper, L.; Elliott, P.; Cappuccio, F.P. Effect of increased potassium intake on cardiovascular risk factors and disease: Systematic review and meta-analyses. BMJ 2013, 346, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aburto, N.J.; Ziolkovska, A.; Hooper, L.; Elliott, P.; Cappuccio, F.P.; Meerpohl, J.J. Effect of lower sodium intake on health: Systematic review and meta-analyses. BMJ 2013, 346, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, F.J.; MacGregor, G.A. Importance of salt in determining blood pressure in children: Meta-analysis of controlled trials. J. Hypertens. 2006, 48, 861–869. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation Guideline: Potassium Intake for Adults and Children. Available online: http://www.ncbi.nlm.nih.gov/books/NBK132460/ (accessed on 10 March 2014).
- Geleijnse, J.M.; Grobbee, D.E.; Hofman, A. Sodium and potassium intake and blood pressure change in childhood. BMJ 1990, 300, 899–902. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Krupp, D.; Remer, T. Salt, fruit and vegetable consumption and blood pressure development: A longitudinal investigation in healthy children. Br. J. Nutr. 2014, 111, 662–671. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Wang, Y. Tracking of blood pressure from childhood to adulthood: A systematic review and meta-regression analysis. Circulation 2008, 117, 3171–3180. [Google Scholar] [CrossRef] [PubMed]
- Tirosh, A.; Afek, A.; Rudich, A.; Percik, R.; Gordon, B.; Ayalon, N.; Derazne, E.; Tzur, D.; Gershnabel, D.; Grossman, E.; et al. Progression of normotensive adolescents to hypertensive adults: A study of 26,980 teenagers. Hypertension 2010, 56, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Berenson, G.S. Childhood risk factors predict adult risk associated with subclinical cardiovascular disease. The Bogalusa Heart Study. Am. J. Cardiol. 2002, 90, 3L–7L. [Google Scholar] [CrossRef]
- Schwandt, P.; Haas, G.-M.; Liepold, E. Lifestyle and cardiovascular risk factors in 2001 child-parent pairs: The PEP Family Heart Study. Atherosclerosis 2010, 213, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, G.L.; Farrow, C.; Haycraft, E.; Meyer, C. Parental influences on children’s eating behaviour and characteristics of successful parent-focussed interventions. Appetite 2013, 60, 85–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenberg, R.S.; Ariza, A.J.; Binns, H.J. Activity and dietary habits of mothers and children: Close ties. Clin. Pediatr. 2010, 49, 1026–1032. [Google Scholar] [CrossRef] [PubMed]
- Grimes, C.A.; Baxter, J.R.; Campbell, K.J.; Riddell, L.J.; Rigo, M.; Liem, D.G.; Keast, R.S.; He, F.J.; Nowson, C.A. Cross-Sectional Study of 24-h Urinary Electrolyte Excretion and Associated Health Outcomes in a Convenience Sample of Australian Primary Schoolchildren: The Salt and Other Nutrients in Children (SONIC) Study Protocol. JMIR Res. Protoc. 2015, 4, e7. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Flegal, K.M.; Nicholls, D.; Jackson, A.A. Body mass index cut offs to define thinness in children and adolescents: International survey. BMJ 2007, 335, 194. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, M. Uber den niederschlag, welchen pikrinsaure in normalen hrn erzeugt und uber eine neue reaction des kreatinins. Biol. Chem. 1886, 10, 3901–3400. [Google Scholar]
- Cogswell, M.E.; Wang, C.-Y.; Chen, T.-C.; Pfeiffer, C.M.; Elliott, P.; Gillespie, C.D.; Carriquiry, A.L.; Sempos, C.T.; Liu, K.; Perrine, C.G.; et al. Validity of predictive equations for 24-h urinary sodium excretion in adults aged 18–39 years. Am. J. Clin. Nutr. 2013, 98, 1502–1513. [Google Scholar] [CrossRef] [PubMed]
- Department of Health and Ageing. User Guide 2007 Australian National Children’s Nutrition and Physical Activity Survey; Department of Health and Ageing: Canberra, Australia, 2010.
- Institute of Medicine. Dietary Reference Intakes for Water, Potassium, Sodium, Chloride and Sulfate; The National Academies Press: Washington, DC, USA, 2004. [Google Scholar]
- Oliveria, S.A.; Ellison, R.C.; Moore, L.L.; Gillman, M.W.; Garrahie, E.J.; Singer, M.R. Parent-child relationships in nutrient intake: The Framingham Children’s Study. Am. J. Clin. Nutr. 1992, 56, 593–598. [Google Scholar] [PubMed]
- McPhie, S.; Skouteris, H.; Daniels, L.; Jansen, E. Maternal correlates of maternal child feeding practices: A systematic review. Mater. Child Nutr. 2014, 10, 18–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patterson, T.L.; Rupp, J.W.; Sallis, J.F.; Atkins, C.J.; Nader, P.R. Aggregation of dietary calories, fats, and sodium in Mexican-American and Anglo families. Am. J. Prev. Med. 1988, 4, 75–82. [Google Scholar] [PubMed]
- Australian Health Survey: Nutrition First Results-Food and Nutrients, 2011–2012. Available online: http://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/4364.0.55.0072011-12?OpenDocument (accessed on 2 August 2014).
- Forrestal, S.G. Energy intake misreporting among children and adolescents: A literature review. Mater. Child Nutr. 2011, 7, 112–127. [Google Scholar] [CrossRef] [PubMed]
- James, W.P.; Ralph, A.; Sanchez-Castillo, C.P. The dominance of salt in manufactured food in the sodium intake of affluent societies. Lancet 1987, 1, 426–429. [Google Scholar] [CrossRef]
- Savage, J.S.; Fisher, J.O.; Birch, L.L. Parental influence on eating behavior: Conception to adolescence. J. Law Med. Ethics 2007, 35, 22–34. [Google Scholar] [CrossRef] [PubMed]
- Coppins, D.F.; Margetts, B.M.; Fa, J.L.; Brown, M.; Garrett, F.; Huelin, S. Effectiveness of a multi-disciplinary family-based programme for treating childhood obesity (the Family Project). Eur. J. Clin. Nutr. 2011, 65, 903–909. [Google Scholar] [CrossRef] [PubMed]
- Knowlden, A.P.; Sharma, M. Systematic review of family and home-based interventions targeting paediatric overweight and obesity. Obes. Rev. 2012, 13, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Koivisto Hursti, U.K. Factors influencing children’s food choice. Ann. Med. 1999, 31, 26–32. [Google Scholar] [PubMed]
- Patrick, H.; Nicklas, T.A. A review of family and social determinants of children’s eating patterns and diet quality. J. Am. Coll. Nutr. 2005, 24, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Mennella, J.A. Ontogeny of taste preferences: basic biology and implications for health. Am. J. Clin. Nutr. 2014, 99, 704–711. [Google Scholar] [CrossRef] [PubMed]
- Bouhlal, S.; Chabanet, C.; Issanchou, S.; Nicklaus, S. Salt content impacts food preferences and intake among children. PLoS ONE 2013, 8, e53971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, G.H.; Lee, H.M. Frequent consumption of certain fast foods may be associated with an enhanced preference for salt taste. J. Hum. Nutr. Diet. 2009, 22, 475–480. [Google Scholar] [CrossRef] [PubMed]
- Stein, L.J.; Cowart, B.J.; Beauchamp, G.K. The development of salty taste acceptance is related to dietary experience in human infants: A prospective study. Am. J. Clin. Nutr. 2012, 95, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Lioret, S.; McNaughton, S.A.; Spence, A.C.; Crawford, D.; Campbell, K.J. Tracking of dietary intakes in early childhood: The Melbourne InFANT Program. Eur. J. Clin. Nutr. 2013, 67, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Protocol for Population Level Sodium Determination in 24-h Urine Samples. Available online: http://www.google.com.au/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=0CB8QFjAA&url=http%3A%2F%2Fnew.paho.org%2Fhq%2Fdmdocuments%2F2010%2Fpahosaltprotocol.pdf&ei=Q44vVIbrGdL58AX2wYGoCg&usg=AFQjCNGoDAziPnJs3Lbm0zeOkazWyDJbKA&sig2=x0qUmo50y-Z6LYyjrH12MA&bvm=bv.76802529,d.dGc (accessed on 26 March 2015).
- Intersalt cooperative research group. Intersalt: An international study of electrolyte excretion and blood pressure. Results for 24 h urinary sodium and potassium excretion. Intersalt Cooperative Research Group. BMJ 1988, 297, 319–328. [Google Scholar]
- Margetts, B.M.; Nelson, M. Design Concepts in Nutritional Epidemiology, 2nd ed.; Oxford University Press: Oxford, UK, 1997; p. 472. [Google Scholar]
- Grimes, C.A.; Campbell, K.J.; Riddell, L.J.; Nowson, C.A. Is socioeconomic status associated with dietary sodium intake in Australian children? A cross-sectional study. BMJ Open 2013, 3, e002106. [Google Scholar] [CrossRef] [PubMed]
- Grimes, C.A.; Riddell, L.J.; Campbell, K.J.; He, F.J.; Nowson, C.A. 24-h urinary sodium excretion is associated with obesity in a cross-sectional sample of Australian schoolchildren. Br. J. Nutr. 2016, 115, 1071–1079. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Measure | Total (n = 168) | 4–8 Years (n = 76) | 9–12 Years (n = 92) | |||
|---|---|---|---|---|---|---|
| Mean or n | SD or % | Mean or n | SD or % | Mean or n | SD or % | |
| Gender (male) 1 | 87 | 51.8% | 41 | 54.0% | 46 | 50.0% |
| Age (years) 2 | 9.1 | 2.0 | 7.3 | 1.1 | 10.6 | 1.0 |
| BMI 1,3 | ||||||
| Underweight | 18 | 10.7% | 12 | 15.8% | 6 | 6.5% |
| Healthy weight | 129 | 76.8% | 61 | 80.3% | 68 | 73.9% |
| Overweight | 17 | 10.1% | 2 | 2.6% | 15 | 16.3% |
| Obese | 4 | 2.4% | 1 | 1.3% | 3 | 3.3% |
| Day of urine collection 1 | ||||||
| School day | 54 | 32.1% | 23 | 30.3% | 31 | 33.7% |
| Non-school day | 114 | 67.9% | 53 | 69.7% | 61 | 66.3% |
| Na (mmol/24-h) 2 | 101 | 47 | 90 | 36 | 110 | 53 |
| Salt equivalent (g/24-h) 2 | 5.9 | 2.7 | 5.2 | 2.1 | 6.4 | 3.1 |
| K (mmol/24-h) 2 | 48 | 18 | 43 | 15 | 52 | 20 |
| Na:K 2,4 | 2.3 | 1.1 | 2.3 | 1.1 | 2.3 | 1.2 |
| Creatinine (mmol/24-h) 2 | 5.4 | 2.0 | 4.3 | 1.3 | 6.3 | 2.0 |
| Total volume (mL) 2 | 858 | 414 | 730 | 329 | 961 | 449 |
| Measures | Female (n = 108) 73.0% | Male (n = 40) 27.0% | ||
|---|---|---|---|---|
| Mean or n | SD or % | Mean or n | SD or % | |
| Age (years) 1,3 | 41.8 | 5.1 | 44.4 | 4.9 |
| Day of urine collection 2 | ||||
| School day | 26 | 25.0% | 6 | 16.2% |
| Non-school day | 78 | 75.0% | 31 | 83.8% |
| Na (mmol/24-h) 1 | 120 | 45 | 152 | 49 |
| Salt equivalent (g/24-h) 1 | 7.0 | 2.6 | 8.9 | 2.9 |
| K (mmol/24-h) 1 | 68 | 19 | 91 | 40 |
| Na:K 2,4 | 1.9 | 0.8 | 1.9 | 0.8 |
| Creatinine (mmol/24-h) 1 | 10.0 | 2.2 | 16.0 | 6.2 |
| Volume (mL) 1 | 1890 | 758 | 2175 | 1033 |
| Adjusted R2 (p Value) | B | 95% CI | p Value | |
|---|---|---|---|---|
| Mothers (n = 138 mother-child pairs) | ||||
| Salt equivalent (g) | ||||
| Unadjusted model | 0.04 (0.08) | 0.18 | (−0.02, 0.39) | 0.08 |
| Model A 1 | 0.16 (0.001) | 0.20 | (0.01, 0.40) | 0.04 |
| Model B 2 | 0.19 (<0.001) | 0.18 | (−0.01, 0.38) | 0.06 |
| Model C 3,4 | 0.22(<0.001) | 0.21 | (0.02, 0.41) | 0.04 |
| Fathers (n = 51 father-child pairs) | ||||
| Salt equivalent (g) | ||||
| Unadjusted model | 0.04 (0.22) | 0.22 | (−0.14, 0.57) | 0.22 |
| Model A 1 | 0.16 (0.02) | 0.21 | (−0.13, 0.55) | 0.21 |
| Model B 2 | 0.17 (0.03) | 0.19 | (−0.14, 0.52) | 0.25 |
| Model C 3 | 0.20 (0.03) | 0.14 | (−0.23, 0.50) | 0.45 |
| Mothers (n = 138 mother-child pairs) | ||||
| Potassium (mmol) | ||||
| Unadjusted model | 0.004 (0.42) | 0.05 | (−0.01, 0.19) | 0.42 |
| Model A 1 | 0.24 (<0.001) | 0.12 | (−0.01, 0.25) | 0.08 |
| Fathers (n = 51 father-child pairs) | ||||
| Potassium (mmol) | ||||
| Unadjusted model | 0.01 (0.37) | 0.05 | (−0.1, 0.18) | 0.37 |
| Model A 1 | 0.13 (0.07) | 0.10 | (−0.06, 0.27) | 0.22 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Service, C.; Grimes, C.; Riddell, L.; He, F.; Campbell, K.; Nowson, C. Association between Parent and Child Dietary Sodium and Potassium Intakes as Assessed by 24-h Urinary Excretion. Nutrients 2016, 8, 191. https://doi.org/10.3390/nu8040191
Service C, Grimes C, Riddell L, He F, Campbell K, Nowson C. Association between Parent and Child Dietary Sodium and Potassium Intakes as Assessed by 24-h Urinary Excretion. Nutrients. 2016; 8(4):191. https://doi.org/10.3390/nu8040191
Chicago/Turabian StyleService, Carrie, Carley Grimes, Lynn Riddell, Feng He, Karen Campbell, and Caryl Nowson. 2016. "Association between Parent and Child Dietary Sodium and Potassium Intakes as Assessed by 24-h Urinary Excretion" Nutrients 8, no. 4: 191. https://doi.org/10.3390/nu8040191
APA StyleService, C., Grimes, C., Riddell, L., He, F., Campbell, K., & Nowson, C. (2016). Association between Parent and Child Dietary Sodium and Potassium Intakes as Assessed by 24-h Urinary Excretion. Nutrients, 8(4), 191. https://doi.org/10.3390/nu8040191