Cardiovascular, Metabolic Effects and Dietary Composition of Ad-Libitum Paleolithic vs. Australian Guide to Healthy Eating Diets: A 4-Week Randomised Trial


Abstract
:
1. Introduction
2. Materials and Methods
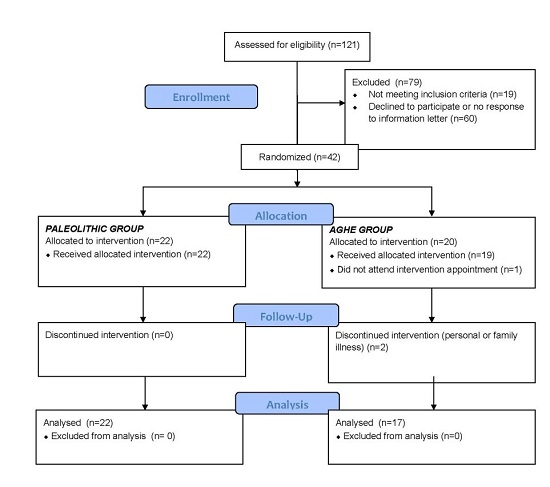
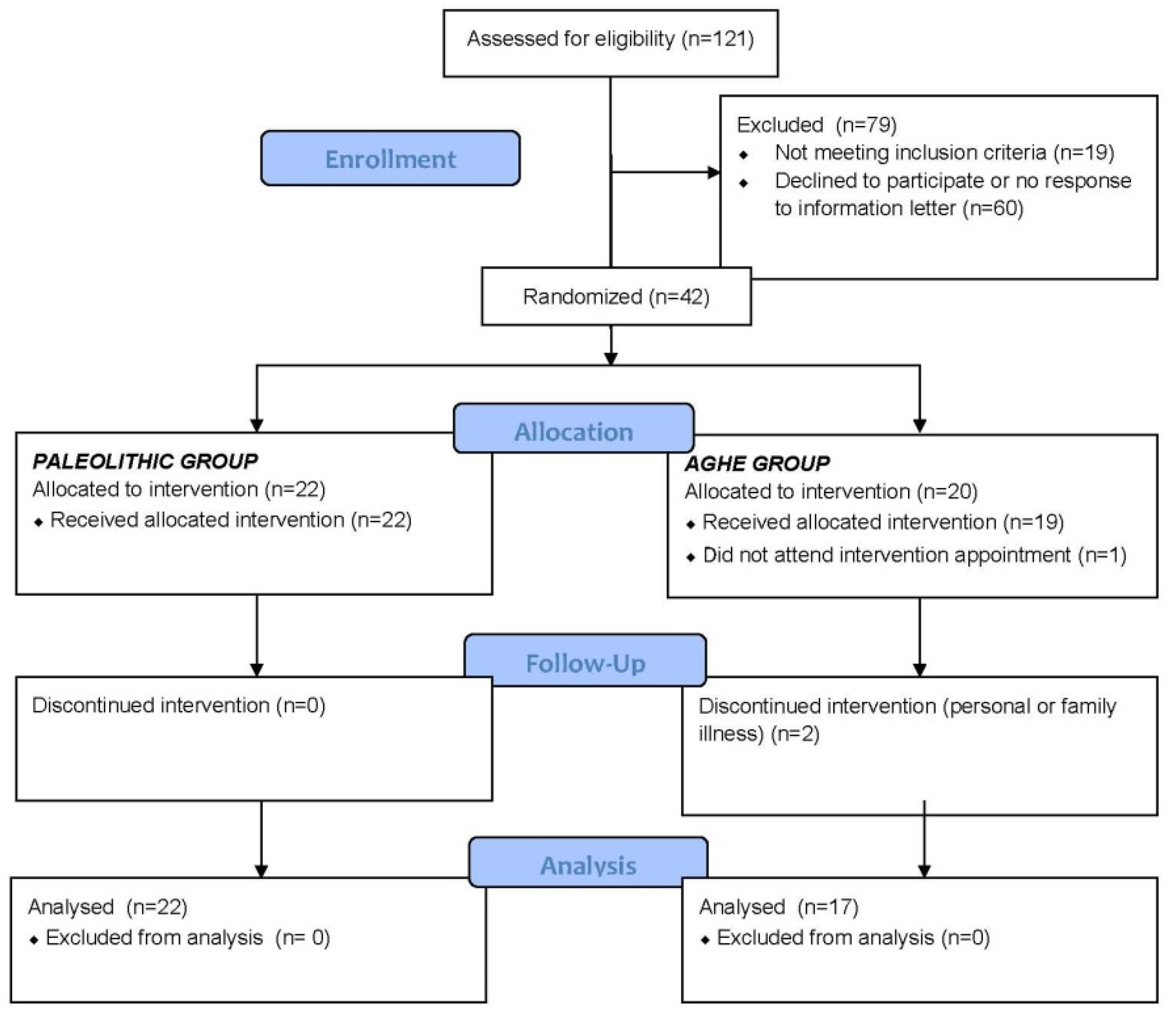
2.1. Study Population
2.2. Anthropometric and Biochemical Assessment
2.3. Dietary Intervention
2.4. Dietary Assessment
Compliance
2.5. Statistical Analysis
3. Results
3.1. Anthropometric
3.2. Biochemicalu
3.3. Dietary Intake
3.3.1. Macronutrients
3.3.2. Micronutrients
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| AGHE | Australian Guide to Healthy Eating |
| PDE | Percentage of Dietary Energy |
| WDR | Weighed Diet Record |
| ES | Effect Size |
References
- Eaton, S.B.; Konner, M. Paleolithic nutrition: A consideration of its nature and current implications. N. Engl. J. Med. 1985, 312, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Cordain, L. The Paleo Diet; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2011. [Google Scholar]
- National Health and Medical Research Council. Australian Dietary Guidelines; National Health and Medical Research Council: Canberra, Australia, 2013. [Google Scholar]
- Frassetto, L.A.; Schloetter, M.; Mietus-Synder, M.; Morris, R.C.; Sebastian, A. Metabolic and physiologic improvements from consuming a paleolithic, hunter-gatherer type diet. Eur. J. Clin. Nutr. 2009, 63, 947–955. [Google Scholar] [CrossRef] [PubMed]
- Osterdahl, M.; Kocturk, T.; Koochek, A.; Wändell, P.E. Effects of a short-term intervention with a paleolithic diet in healthy volunteers. Eur. J. Clin. Nutr. 2008, 62, 682–685. [Google Scholar] [CrossRef] [PubMed]
- Ryberg, M.; Sandberg, S.; Mellberg, C.; Stegle, O.; Lindahl, B.; Larsson, C.; Hauksson, J.; Olsson, T. A Palaeolithic-type diet causes strong tissue-specific effects on ectopic fat deposition in obese postmenopausal women. J. Intern. Med. 2013, 274, 67–76. [Google Scholar] [CrossRef] [PubMed]
- G*Power; Version 3.1.9.2; University of Kiel: Kiel, Germany, 2014.
- Marfell-Jones, M.; Olds, T.; Stewart, A.; Carter, J.L. International Standards for Anthropometric Assessment; The International Society for the Advancement of Kinanthropometry: Potchefstroom, South Africa, 2007. [Google Scholar]
- National Institute of Science and Technology. Standard Reference Material Standard 968e: Fat Soluble Vitamins and Carotenoids in Human Serum; US Department of Commerce: Washington, DC, USA, 2010. [Google Scholar]
- SPSS for Windows; Version 22.0; IBM Corporation: Chicago, IL, USA, 2013.
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Krieger, J.W.; Sitren, H.S.; Daniels, M.J.; Langkamp-Henken, B. Effects of variation in protein and carbohydrate intake on body mass and composition during energy restriction: A meta-regression. Am. J. Clin. Nutr. 2006, 83, 260. [Google Scholar] [PubMed]
- Mellberg, C.; Sandberg, S.; Ryberg, M.; Eriksson, M.; Brage, S.; Larsson, C.; Olsson, T.; Lindahl, B. Long-term effects of a Palaeolithic-type diet in obese postmenopausal women: A 2-year randomized trial. Eur. J. Clin. Nutr. 2014, 68, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Jönsson, T.; Granfeldt, Y.; Ahrén, B.; Branell, U.-C.; Pålsson, G.; Hansson, A.; Söderström, M.; Lindeberg, S.; Sektion, I. Beneficial effects of a Paleolithic diet on cardiovascular risk factors in type 2 diabetes: A randomized cross-over pilot study. Cardiovasc. Diabetol. 2009, 8, 35. [Google Scholar] [CrossRef] [PubMed]
- Pastore, R.L.; Brooks, J.T.; Carbone, J.W. Paleolithic nutrition improves plasma lipid concentrations of hypercholesterolemic adults to a greater extent than traditional heart-healthy dietary recommendations. Nutr. Res. 2015, 35, 474–479. [Google Scholar] [CrossRef] [PubMed]
- Lindeberg, S.; Jönsson, T.; Granfeldt, Y.; Borgstrand, E.; Soffman, J.; Sjöström, K.; Ahrén, B. A Palaeolithic diet improves glucose tolerance more than a Mediterranean-like diet in individuals with ischaemic heart disease. Diabetologia 2007, 50, 1795–1807. [Google Scholar] [CrossRef] [PubMed]
- O’Dea, K. Marked improvement in carbohydrate and lipid metabolism in diabetic Australian aborigines after temporary reversion to traditional lifestyle. Diabetes 1984, 33, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Hoffmann, G. Comparison of effects of long-term low-fat vs. high-fat diets on blood lipid levels in overweight or obese patients: A systematic review and meta-analysis. J. Acad. Nutr. Diet. 2013, 113, 1640–1661. [Google Scholar] [PubMed]
- Manheimer, E.W.; van Zuuren, E.J.; Fedorowicz, Z.; Pijl, H. Paleolithic nutrition for metabolic syndrome: Systematic review and meta-analysis. Am. J. Clin. Nutr. 2015, 102, 922–932. [Google Scholar] [CrossRef] [PubMed]
- Rietman, A.; Schwarz, J.; Tome, D.; Kok, F.J.; Mensink, M. High dietary protein intake, reducing or eliciting insulin resistance? Eur. J. Clin. Nutr. 2014, 68, 973–979. [Google Scholar] [CrossRef] [PubMed]
- Hill, A.M.; Jackson, K.A.H.; Roussell, M.A.; West, S.G.; Kris-Etherton, P.M. Type and amount of dietary protein in the treatment of metabolic syndrome: A randomized controlled trial. Am. J. Clin. Nutr. 2015, 102, 757–770. [Google Scholar] [CrossRef] [PubMed]
- Jönsson, T.; Granfeldt, Y.; Erlanson-Albertsson, C.; Ahrén, B.; Lindeberg, S.; Sektion, I. A paleolithic diet is more satiating per calorie than a mediterranean-like diet in individuals with ischemic heart disease. Nutr. Metab. 2010, 7, 85. [Google Scholar] [CrossRef] [PubMed]
- Rolls, B.J.; Ello-Martin, J.A.; Tohill, B.C. What can intervention studies tell us about the relationship between fruit and vegetable consumption and weight management? Nutr. Rev. 2004, 62, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Shohag, M.J.; Wei, Y.; Yu, N.; Lu, L.; Zhang, J.; He, Z.; Patring, J.; Yang, X. Folate content and composition of vegetables commonly consumed in China. J. Food Sci. 2012, 77, H239–H245. [Google Scholar] [CrossRef] [PubMed]
- Scott, K.P.; Duncan, S.H.; Flint, H.J. Dietary fibre and the gut microbiota. Nutr. Bull. 2008, 33, 201–211. [Google Scholar] [CrossRef]
- National Health and Medical Research Council and New Zealand Ministry of Health. Nutrient Reference Values for Australia and New Zealand Including Recommended Dietary Intakes; Commonwealth of Australia: Canberra, Australia, 2006; pp. 229–233. [Google Scholar]
- Food and Agriculture Organisation. Fats and Fatty Acids in Human Nutrition: Report of an Expert Consultation; Food and Agriculture Organisation: Rome, Italy, 2010. [Google Scholar]
- Fung, T.T.; van Dam, R.M.; Hankinson, S.E.; Stampfer, M.; Willett, W.C.; Hu, F.B. Low-carbohydrate diets and all-cause and cause-specific mortality two cohort studies. Ann. Intern. Med. 2010, 153, 289. [Google Scholar] [CrossRef] [PubMed]
- Lagiou, P.; Sandin, S.; Lof, M.; Trichopoulos, D.; Adami, H.O.; Weiderpass, E. Low carbohydrate-high protein diet and incidence of cardiovascular diseases in Swedish women: Prospective cohort study. BMJ 2012, 344, e4026. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Anthropometric Measure | Paleolithic (n = 22) | AGHE (n = 17) | |||||
|---|---|---|---|---|---|---|---|
| Pre (Mean ± SD) | Post (Mean ± SD) | Change within Group (95% CI) | Pre (Mean ±SD) | Post (Mean ± SD) | Change within Group (95% CI) | Change between Groups Mean Difference (95% CI) | |
| Body weight (kg) | 73.8 ± 13.3 | 70.6 ± 12.7 | −3.20 (−3.8, −2.6) ** | 73.0 ± 12.3 | 71.8 ± 12.3 | −1.21 (−2.0, −0.5) ** | −1.99 (−2.9, −1.0) ** |
| Fat Mass (%) | 34.1 ± 8.9 | 32.6 ± 9.1 | −1.48 (−2.2, −0.8) ** | 31.5 ± 6.2 | 31.3 ± 6.3 | −0.14 (−1.1, 0.9) | −1.34 (−2.5, −0.2) * |
| Fat Mass (kg) | 26.2 ± 10.8 | 24.1 ± 10.4 | −2.14 (−2.7, −1.6) ** | 23.6 ± 7.5 | 23.1 ± 7.7 | −0.46 (−1.4, 0.4) | −1.68 (−2.7, −0.7) ** |
| Fat Free Mass (%) | 65.9 ± 8.9 | 67.0 ± 9.1 | 1.07 (0.3, 1.8) ** | 68.5 ± 6.2 | 68.6 ± 6.3 | 0.12 (−0.9, 1.1) | 0.94 (−0.2, 2.1) |
| Fat Free Mass (kg) | 48.5 ± 5.0 | 47.1 ± 4.7 | −1.38 (−2.1, −0.6) ** | 50.2 ± 7.2 | 49.4 ± 6.5 | −0.79 (−1.5, −0.1) * | −0.59 (−1.6, 0.5) |
| Percent Weight Loss (%) | - | −4.28 ± 1.7 | - | - | −1.66 ± 1.9 | - | −2.63 (−3.8, −1.5) ** |
| Waist Circumference (cm) 2 | 85.9 ± 14.9 | 82.5 ± 14.1 | −3.35 (−4.2, −2.5) ** | 83.0 ± 9.0 | 81.4 ± 8.6 | −1.55 (−2.6, −0.4) * | −1.9 (−3.2, −0.8) ** |
| Systolic BP (mmHg) | 119 ± 14.5 | 115 ± 11.5 | −3.32 (−9.1, 2.5) | 115 ± 11.1 | 114 ± 9.9 | −0.71 (−5.2, 3.8) | −2.61 (−10.1, 4.9) |
| Diastolic BP (mmHg) | 77.8 ± 9.0 | 75.9 ± 10.0 | −1.87 (−6.4, 2.7) | 71.7 ± 6.7 | 73.4 ± 7.2 | 1.65 (−1.0, 4.3) | −3.51 (−9.0, 2.0) |
| Biochemical Measure | Paleolithic (n = 22) | AGHE (n = 17) | Mean Difference between Groups (95% CI) | ||||
|---|---|---|---|---|---|---|---|
| Pre (Mean ± SD) | Post (Mean ± SD) | Change within Group (95% CI) | Pre (Mean ± SD) | Post (Mean ± SD) | Change within Group (95% CI) | ||
| Total Plasma Cholesterol (mmol/L) | 5.59 ± 1.2 | 5.05 ± 1.0 | −0.55 (−0.8, −0.3) ** | 5.28 ± 1.0 | 4.86 ± 0.8 | −0.41 (−0.7, −0.1) ** | −0.13 (−0.5, 0.2) |
| Triglycerides (TG) (mmol/L) | 0.97 ± 0.5 | 0.79 ± 0.3 | −0.18 (−0.3, 0.0) ** | 0.79 ± 0.2 | 0.73 ± 0.2 | −0.07 (−0.2, 0.0) | −0.14 (−0.4, 0.2) |
| Low density lipoprotein (LDL) Cholesterol 1 (mmol/L) | 3.50 ± 1.2 | 3.10 ± 0.9 | −0.40 (−0.6, −0.2) ** | 3.19 ± 0.9 | 2.93 ± 0.7 | −0.26 (−0.5, 0.0) * | −0.11 (−0.3, 0.1) |
| High density lipoprotein (HDL) Cholesterol (mmol/L) | 1.66 ± 0.3 | 1.58 ± 0.3 | −0.08 (−0.2, 0.0) | 1.72 ± 0.3 | 1.59 ± 0.3 | −0.12 (−0.2, −0.1) ** | 0.04 (−0.1, 0.1) |
| Chol/HDL Ratio | 3.56 ± 1.4 | 3.33 ± 1.0 | −0.23 (−0.5, 0.0) | 3.13 ± 0.7 | 3.15 ± 0.7 | 0.01 (−0.1, 0.2) | −0.24 (−0.5, 0.1) |
| Plasma C-Reactive Protein (mg/L) | 2.23 ± 2.9 | 1.64 ± 1.7 | −0.51 (−1.1, 0.1) | 1.42 ± 1.1 | 1.49 ± 1.7 | 0.06 (−0.9, 1.0) | −0.57 (−1.6, 0.5) |
| Fasting Plasma Glucose (mmol/L) | 4.77 ± 0.8 | 4.70 ± 0.6 | −0.06 (−0.3, 0.1) | 4.55 ± 0.4 | 4.49 ± 0.6 | −0.05 (−0.3, 0.2) | −0.01 (−0.3, 0.3) |
| Fasting Serum Insulin (mU/L) | 4.36 ± 2.5 | 4.32 ± 2.4 | −0.04 (−1.2, 1.1) | 4.65 ± 1.8 | 4.88 ± 1.9 | 0.23 (−0.8, 1.2) | −0.28 (−1.8, 1.3) |
| Serum α-carotene (μmol/L) | 0.39 ± 0.4 | 0.46 ± 0.2 | 0.08 (0.0, 0.2) | 0.52 ± 0.4 | 0.48 ± 0.2 | −0.05 (−0.2, 0.1) | 0.12 (−0.1, 0.3) |
| Serum β-carotene (μmol/L) | 1.54 ± 1.3 | 2.41 ± 1.8 | 0.95 (−0.2, 1.7) * | 1.53 ± 0.8 | 1.62 ± 1.1 | 0.09 (−0.3, 0.4) | 0.86 (0.0, 1.7) * |
| Serum Lycopene (μmol/L) | 0.61 ± 0.3 | 0.52 ± 0.2 | −0.07 (−0.2, 0.0) | 0.58 ± 0.2 | 0.50 ± 0.2 | 0.05 (−0.2, 0.3) | −0.12 (−0.4, 0.1) |
| Red Cell Folate (nmol/L) | 894 ± 214 | 981 ± 300 | 86.7 (23.9, 149.5) ** | 758 ± 287 | 751 ± 218 | −6.88 (−71.1, 57.3) | 93.54 (7.0, 180.1) * |
| Plasma Creatinine (μmol/L) | 70.86 ± 8.5 | 73.48 ± 10.8 | 2.52 (−0.4, 5.5) | 68.4 ± 8.2 | 67.77 ± 8.7 | −0.65 (−4.0, 2.8) | 3.17 (−1.1, 7.5) |
| 24 h Urine Sodium (mmol/day) | 95.34 ± 43.1 | 79.3 ± 50.7 | −16.1 (−36.7, 4.6) | 94.8 ± 45.5 | 99.5 ± 44.4 | 4.69 (−20.0, 29.4) | −25.35 (−57.2, 6.5) |
| 24 h Urine Creatinine (mmol/day) | 10.8 ± 4.8 | 11.9 ± 4.6 | 1.04 (−1.2, 3.3) | 10.2 ± 3.6 | 10.5 ± 2.8 | 0.34 (−1.0, 1.7) | 0.27 (−2.5, 3.1) |
| Macronutrient | Paleolithic (n = 22) | AGHE (n = 17) | Mean Difference between Groups (95% CI) | ||||
|---|---|---|---|---|---|---|---|
| Pre (Mean ± SD) | Post (Mean ± SD) | Change within Group (95% CI) | Pre (Mean ± SD) | Post (Mean ± SD) | Change within Group (95% CI) | ||
| Total Energy Intake (kJ) | 7798 ± 1928 | 5915 ± 1452 | −1883 (−2772, −993) ** | 8088 ± 2071 | 6657 ± 1725 | −1432 (2973, 109) | −450.94 (−2076, 1174) |
| Protein (g) | 90.2 ± 11.1 | 91.2 ± 31.5 | 1.78 (−11.2, 14.8) | 94.9 ± 24.9 | 83.5 ± 28.4 | −11.4 (−30.4, 7.5) | 13.21 (−8.3, 34.7) |
| Protein (% of Energy) | 20.6 ± 4.9 | 26.8 ± 7.2 | 6.19 (3.4, 9.0) ** | 20.1 ± 3.61 | 21.7 ± 5.6 | 1.52 (−1.3, 4.3) | 4.67 (0.8, 8.6) * |
| Carbohydrate (g) | 191 ± 68.0 | 103 ± 32.4 | −87.8 (−115.4, −60.2) ** | 188 ± 62.1 | 163 ± 46.5 | −24.9 (−58.6, 8.8) | −62.88 (−104.6, −21.2) ** |
| Carbohydrate (% of Energy) | 39.1 ± 6.2 | 27.8 ± 8.05 | −11.3 (−15.0, −7.6) ** | 37.2 ± 7.67 | 40.6 ± 9.4 | 3.34 (0.1, 6.5) * | −14.63 (−19.5, −9.7) ** |
| Total Fat (g) | 71.3 ± 22.8 | 64.7 ± 26.7 | −6.62 (−18.4, 5.2) | 78.7 ± 24.1 | 60.1 ± 24.1 | −18.5 (−38.4, 1.0) | 11.92 (−9.0, 32.9) |
| Total Fat (% of Energy) | 33.6 ± 5.3 | 39.8 ± 9.6 | 6.20 (2.0, 10.4) ** | 35.8 ± 5.5 | 32.6 ± 7.3 | −3.20 (−7.1, 0.7) | 9.39 (3.7, 15.1) ** |
| Total Sugars (g) | 92.5 ± 42.0 | 77.2 ± 26.1 | −15.2 (−32.4, 1.9) | 88.8 ± 29.2 | 75.7 ± 32.5 | −13.1 (−31.1, 4.9) | −2.18 (−26.5, 22.1) |
| Saturated Fat (g) | 26.7 ± 10.4 | 18.8 ± 7.3 | −7.86 (−12.1, 3.7) ** | 31.4 ± 12.0 | 22.1 ± 9.2 | −9.31 (−17.4, 1.2) * | 1.44 (−6.8, 9.7) |
| Saturated Fat (% of Energy) | 12.4 ± 2.5 | 11.9 ± 3.8 | −0.52 (−2.2, 1.1) | 14.1 ± 3.0 | 12.0 ± 2.8 | −2.10 (−3.9, −0.3) | 1.58 (−0.8, 4.0) |
| Monounsaturated Fat (g) | 26.3 ± 7.9 | 29.5 ± 16.8 | 3.18 (−3.7, 10.1) | 28.4 ± 9.9 | 22.3 ± 9.9 | −6.11 (−14.2, 2.0) | 9.28 (−1.0.19.6) |
| Polyunsaturated Fat (g) | 12.8 ± 6.0 | 10.8 ± 6.4 | −1.97 (−4.0, 0.1) | 12.5 ± 4.9 | 10.4 ± 5.8 | −2.13 (−5.7, 1.4) | 0.16 (−3.6, 3.9) |
| Dietary Fibre (g) | 24.6 ± 6.1 | 24.6 ± 7.2 | 0.05 (−3.7, 3.8) | 25.7 ± 6.2 | 24.9 ± 10.6 | −0.82 (−6.4, 4.8) | 0.87 (−5.4, 7.1) |
| Fibre Density (%) (Fibre (g)/Energy kJ × 100) | 0.33 ± 0.1 | 0.42 ± 0.1 | 0.10 (0.0, 0.2) ** | 0.33 ± 0.1 | 0.37 ± 0.1 | 0.04 (0.0, 0.1) | 0.06 (0.0, 0.1) |
| Alcohol (g) | 8.39 ± 8.8 | 1.78 ± 3.4 | −6.60 (−10.5, −2.7) ** | 7.11 ± 8.1 | 3.05 ± 6.7 | −4.06 (−7.1, −1.0) * | −2.54 (−7.5, 2.5) |
| Micronutrient | Paleolithic (n = 22) | AGHE (n = 17) | Mean Difference between Groups (95% CI) | ||||
|---|---|---|---|---|---|---|---|
| Pre (Mean ± SD) | Post (Mean ± SD) | Change within Group (95% CI) | Pre (Mean ± SD) | Post (Mean ± SD) | Change within Group (95% CI) | ||
| Thiamin (mg) | 1.55 ± 0.6 | 0.96 ± 0.5 | −0.59 (−0.9, −0.3) ** | 1.46 ± 0.6 | 1.49 ± 1.1 | 0.04 (−0.6, 0.6) | −0.63 (−1.2, −0.01) * |
| Riboflavin (mg) | 1.91 ± 0.6 | 1.47 ± 0.4 | −0.44 (−0.7, −0.1) ** | 2.12 ± 0.7 | 2.11 ± 1.2 | −0.01 (−0.6, 0.6) | −0.43 (−1.0, 0.8) |
| Niacin Equivalents (mg) | 42.57 ± 6.6 | 43.76 ± 19.4 | 1.19 (−6.6, 9.0) | 47.9 ± 16 | 44.4 ± 17 | −3.52 (−13.7, 6.7) | 4.71 (−7.5, 16.9) |
| Vitamin C (mg) | 107.41 ± 50 | 167.72 ± 84.2 | 60.31 (19.6, 101.0) ** | 104.1 ± 50 | 95.6 ± 51 | −8.51 (−43.0, 25.9) | 68.82 (15.2, 122.5) * |
| Vitamin E (mg) | 9.81 ± 2.5 | 14.25 ± 7.3 | 4.44 (0.9, 8.0) * | 11.04 ± 3.8 | 9.00 ± 5.0 | −2.05 (−5.2, 1.1) | 6.49 (1.8, 11.2) ** |
| Folate Equivalents (μg) | 396 ± 136 | 316.59 ± 84.9 | −78.99 (−143.7, −14.3) * | 376 ± 144 | 350 ± 132 | −25.75 (−131.0, 79.5) | −53.24 (−167.0, 60.5) |
| β-Carotene Equivalents (μg) | 4257.94 ± 2507.5 | 11,379.27 ± 7966.3 | 7121.33 (3325.3, 10917.3) ** | 4042 ± 3006 | 4386 ± 3642 | 344.40 (−1940.5, 2629.3) | 6776.93 (2143.7, 11410.2) ** |
| Total Vit A Equivalents (μg) | 1014.78 ± 448.3 | 2031.93 ± 1359.0 | 1017.15 (376.6, 1657.7) ** | 968 ± 525 | 984 ± 679 | 15.79 (−402.9, 434.5) | 1001.36 (207.7, 1795.0) * |
| Iodine (μg) | 120.04 ± 38.9 | 63.91 ± 22.7 | −56.12 (−77.7, −34.5) ** | 123 ± 44 | 145 ± 40 | −8.26 (−32.2, 15.7) | −47.86 (−79.2, −16.5) ** |
| Sodium (mg) | 2173.63 ± 568.3 | 915.07 ± 488.8 | −1258.55 (−1553.5, −963.6) ** | 2082 ± 804 | 1878 ± 659 | −203.47 (−712.4, 305.4) | −1055.09 (−1592.6, −517.6) ** |
| Magnesium (mg) | 359.14 ± 85.1 | 327.88 ± 96.7 | −31.27 (−82.3, 19.8) | 399 ± 98 | 366 ± 106 | −32.59 (−100.7, 35.5) | 1.32 (−79.1, 81.8) |
| Potassium (mg) | 3124.18 ± 691.9 | 3371.21 ± 891.2 | 247.03 (−187.7, 681.8) | 3389 ± 717 | 2947 ± 863 | −442.66 (−1034.2, 148.9) | 689.69 (−2.1, 1381.5) |
| Calcium (mg) | 771.21 ± 204.3 | 355.42 ± 91.2 | −415.78 (−517.4, −314.2) ** | 883 ± 300 | 759 ± 247 | −123.41 (−311.0, 64.1) | −292.38 (−485.8, −99.0) ** |
| Iron (mg) | 12.69 ± 2.6 | 11.08 ± 2.7 | −1.61 (−3.0, −0.2) * | 11.8 ± 2.9 | 10.56 ± 3.2 | −1.27 (−3.4, 0.8) | −0.34 (−2.7, 2.0) |
| Zinc (mg) | 11.45 ± 2.4 | 11.86 ± 3.4 | 0.42 (−0.9, 1.8) | 12.5 ± 4.4 | 10.3 ± 3.1 | −2.21 (−5.0, 0.6) | 2.63 (−0.1, 5.4) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Genoni, A.; Lyons-Wall, P.; Lo, J.; Devine, A. Cardiovascular, Metabolic Effects and Dietary Composition of Ad-Libitum Paleolithic vs. Australian Guide to Healthy Eating Diets: A 4-Week Randomised Trial. Nutrients 2016, 8, 314. https://doi.org/10.3390/nu8050314
Genoni A, Lyons-Wall P, Lo J, Devine A. Cardiovascular, Metabolic Effects and Dietary Composition of Ad-Libitum Paleolithic vs. Australian Guide to Healthy Eating Diets: A 4-Week Randomised Trial. Nutrients. 2016; 8(5):314. https://doi.org/10.3390/nu8050314
Chicago/Turabian StyleGenoni, Angela, Philippa Lyons-Wall, Johnny Lo, and Amanda Devine. 2016. "Cardiovascular, Metabolic Effects and Dietary Composition of Ad-Libitum Paleolithic vs. Australian Guide to Healthy Eating Diets: A 4-Week Randomised Trial" Nutrients 8, no. 5: 314. https://doi.org/10.3390/nu8050314
APA StyleGenoni, A., Lyons-Wall, P., Lo, J., & Devine, A. (2016). Cardiovascular, Metabolic Effects and Dietary Composition of Ad-Libitum Paleolithic vs. Australian Guide to Healthy Eating Diets: A 4-Week Randomised Trial. Nutrients, 8(5), 314. https://doi.org/10.3390/nu8050314