Thyroid Function among Breastfed Children with Chronically Excessive Iodine Intakes

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
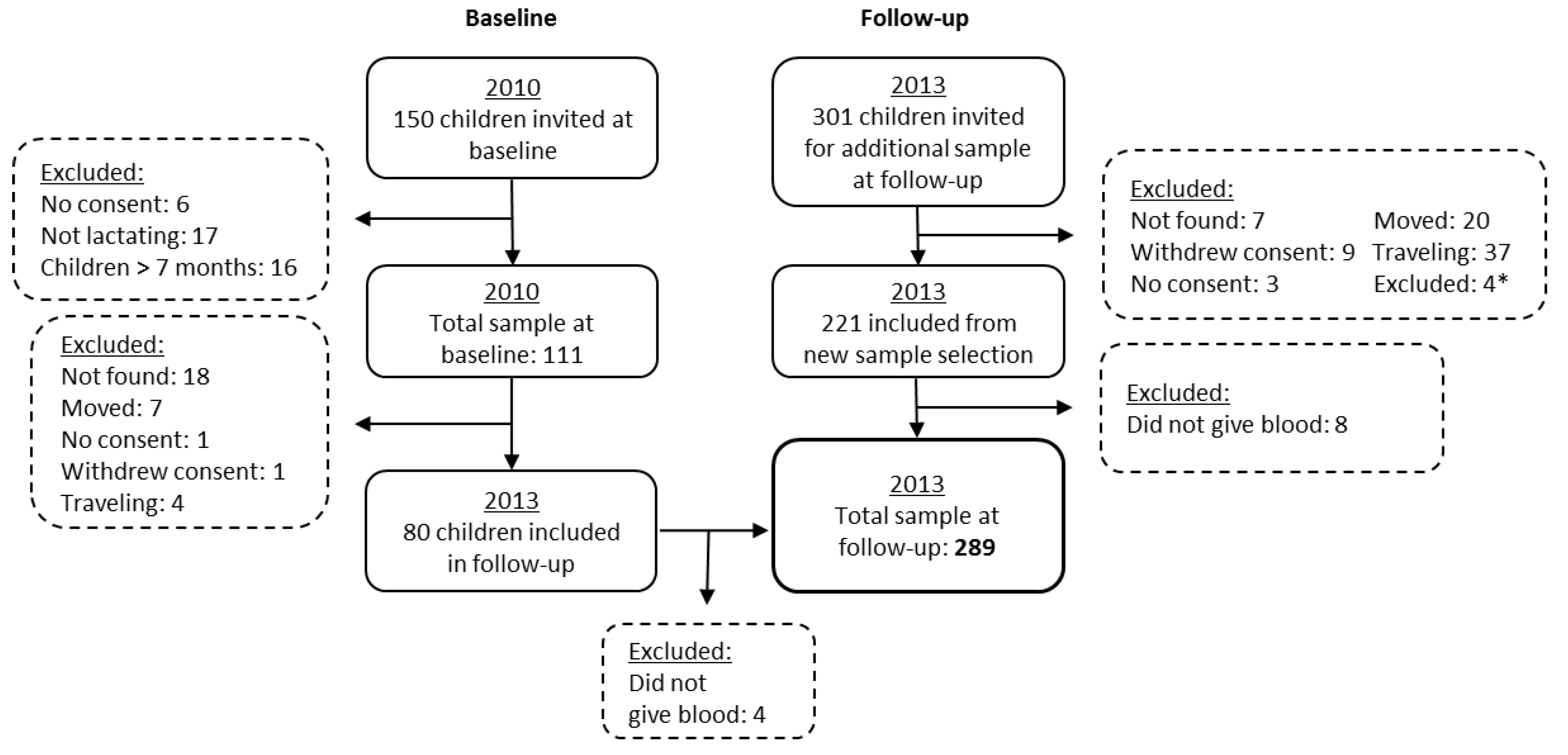
2.1. Subjects
2.2. Urine and Water Samples
2.3. Breast Milk Samples
2.4. Anthropometric Measures
2.5. Serum Samples and Thyroid Hormones
2.6. Ethical Considerations
2.7. Statistics
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. Assessment of Iodine Deficiency Disorders and Monitoring Their Elimination. A Guide for Programme Managers; World Health Organisation, International Council for Control of Iodine Deficiency Disorders, United Nations Children’s Fund: Geneva, Switserland, 2007. [Google Scholar]
- Pearce, E.N.; Andersson, M.; Zimmermann, M.B. Global iodine nutrition: Where do we stand in 2013? Thyroid 2013, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, B.M. Iodine deficiency and excess in children: Worldwide status in 2013. Endocr. Pract. 2013, 19, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Theodoropoulos, T.; Braverman, L.E.; Vagenakis, A.G. Iodide-induced hypothyroidism: A potential hazard during perinatal life. Science 1979, 502–503. [Google Scholar] [CrossRef]
- Leung, A.M.; Braverman, L.E. Consequences of excess iodine. Nat. Rev. Endocrinol. 2013, 10, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Thaker, V.; Leung, A.; Braverman, L.; Brown, R.; Levine, B. Iodine-induced hypothyroidism in full-term infants with congenital heart disease: More common than currently appreciated? J. Clin. Endocrinol. Metab. 2014, 99, 3521–3526. [Google Scholar] [CrossRef] [PubMed]
- Connelly, K.J.; Boston, B.A.; Pearce, E.N.; Sesser, D.; Snyder, D.; Braverman, L.E.; Pino, S.; LaFranchi, S.H. Congenital hypothyroidism caused by excess prenatal maternal iodine ingestion. J. Pediatr. 2012, 161, 760–762. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, B.M. The role of iodine in human growth and development. Semin. Cell Dev. Biol. 2011, 22, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.-L.; Lam, L.T.; Zeng, Q.; Han, S.-Q.; Fu, G.; Hou, C.-C. Effects of drinking water with high iodine concentration on the intelligence of children in Tianjin, China. J. Public Health 2009, 31, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Rhee, S.S.; Braverman, L.E.; Pino, S.; He, X.; Pearce, E.N. High iodine content of Korean seaweed soup: A health risk for lactating women and their infants? Thyroid 2011, 21. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.R.; Shin, C.H.; Yang, S.W.; Choi, C.W.; Kim, B.I. Subclinical hypothyroidism in korean preterm infants associated with high levels of iodine in breast milk. J. Clin. Endocrinol. Metab. 2009, 94, 4444–4447. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.; Kim, J. Iodine content of human milk and dietary iodine intake of Korean lactating mothers. Int. J. Food Sci. Nutr. 1999, 50, 165–171. [Google Scholar] [PubMed]
- Zimmermann, M.B.; Ito, Y.; Hess, S.Y.; Fuijeda, K.; Molinari, L. High thyroid volume in children with excess dietary iodine intakes. Am. J. Clin. Nutr. 2005, 81, 840–844. [Google Scholar] [PubMed]
- Lv, S.; Xie, L.; Xu, D.; Wang, Y.; Jia, L.; Du, Y. Effect of reducing iodine excess on children’s goiter prevalence in areas with high iodine in drinking water. Endocrine 2015, 52, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Nepal, A.K.; Suwal, R.; Gautam, S.; Shah, G.S.; Baral, N.; Andersson, M.; Zimmermann, M. Subclinical hypothyroidism and elevated thyroglobulin in infants with chronic excess iodine intakes. Thyroid 2015, 25, 851–859. [Google Scholar] [CrossRef] [PubMed]
- Sang, Z.; Chen, W.; Shen, J.; Tan, L.; Zhao, N.; Liu, H.; Wen, S.; Wei, W.; Zhang, G.; Zhang, W. Long-term exposure to excessive iodine from water is associated with thyroid dysfunction in children. J. Nutr. 2013, 143, 2038–2043. [Google Scholar] [CrossRef] [PubMed]
- Barikmo, I.; Henjum, S.; Dahl, L.; Oshaug, A.; Torheim, L.E. Environmental implication of iodine in water; milk and other foods used in saharawi refugees camps in tindouf; Algeria. J. Food Compos. Anal. 2011, 24, 637–641. [Google Scholar] [CrossRef]
- Henjum, S.; Barikmo, I.; Gjerlaug, A.K.; Mohamed-Lehabib, A.; Oshaug, A.; Strand, T.A.; Torheim, L.E. Endemic goitre and excessive iodine in urine and drinking water among saharawi refugee childrren. Public Health Nutr. 2010, 13, 1472–1477. [Google Scholar] [CrossRef] [PubMed]
- Henjum, S.; Barikmo, I.; Strand, T.A.; Oshaug, A.; Torheim, L.E. Iodine-induced goitre and high rates of anaemia among saharawi refugee women. Public Health Nutr. 2011, 15, 1512–1518. [Google Scholar] [CrossRef] [PubMed]
- Aakre, I.; Bjøro, T.; Norheim, I.; Strand, T.A.; Barikmo, I.; Henjum, S. Development of thyroid dysfunction among women with excessive iodine intake–a 3-year follow-up. J. Trace Elements Med. Biol. 2015, 31, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Aakre, I.; Bjøro, T.; Norheim, I.; Strand, T.A.; Barikmo, I.; Henjum, S. Excessive iodine intake and thyroid dysfunction among lactating saharawi women. J. Trace Elements Med. Biol. 2015, 31, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Sandell, E.; Kolthoff, I. Micro determination of iodine by a catalytic method. Microchim. Acta 1937, 1, 9–25. [Google Scholar] [CrossRef]
- Jooste, L.P.; Strydom, E. Methods for determination of iodine in urine and salt. Best Pract. Res. Clin. Endocrinol. 2010, 24, 77–88. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Nutrient Adequacy of Exclusive Breastfeeding for the Term Infant during the First Six Months of Life; World Health Organization: Geneva, Switserland, 2002. [Google Scholar]
- World Health Organization. Who Anthro (version 3.2.2, January 2011) and Macros. Available online: http://www.who.int/childgrowth/software/en/ (accessed on 15 September 2015).
- World Health Organization. Who Child Growth Standards. Length/Height-for Age, Weight-for -Age, Weight-for-Length, Weight-for-Height and Body Mass Index-for-Age. Methods and Development; World Health Organization: Geneva, Switserland, 2006. [Google Scholar]
- Heil, W.; Erhardt, V. Reference Ranges for Adults and Children-Pre-Analytical Considerations; Roche Diagnostics GMBH: Mannheim, Germany, 2008; pp. 129–137. [Google Scholar]
- Rohner, F.; Zimmermann, M.; Jooste, P.; Pandav, C.; Caldwell, K.; Raghavan, R.; Raiten, D.J. Biomarkers of nutrition for development—Iodine review. J. Nutr. 2014, 144, 1322S–1342S. [Google Scholar] [CrossRef] [PubMed]
- Vejbjerg, P.; Knudsen, N.; Perrild, H.; Laurberg, P.; Andersen, S.; Rasmussen, L.B.; Ovesen, L.; Jørgensen, T. Estimation of iodine intake from various urinary iodine measurements in population studies. Thyroid 2009, 19, 1281–1286. [Google Scholar] [CrossRef] [PubMed]
- Andersen, S.; Karmisholt, J.; Pedersen, K.M.; Laurberg, P. Reliability of studies of iodine intake and recommendations for number of samples in groups and in individuals. Br. J. Nutr. 2008, 99, 813–818. [Google Scholar] [CrossRef] [PubMed]
- Montenegro-Bethancourt, G.; Johner, S.A.; Stehle, P.; Neubert, A.; Remer, T. Iodine status assessment in children: Spot urine iodine concentration reasonably reflects true twenty-four–hour iodine excretion only when scaled to creatinine. Thyroid 2015, 25, 688–697. [Google Scholar] [CrossRef] [PubMed]
- Scientific Committee on Food. Scientific Panel on Dietetic Products, Nutrition and Allergies. In Tolerable Upper Intake Levels for Vitamins and Minerals; European Food Safety Authority: Parma, Italy, 2006. [Google Scholar]
- Institute of Medicine (US) Panel on Micronutrients. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academies Press: Washington, DC, USA, 2001. [Google Scholar]
- Bouhouch, R.R.; Bouhouch, S.; Cherkaoui, M.; Aboussad, A.; Stinca, S.; Haldimann, M.; Andersson, M.; Zimmermann, M.B. Direct iodine supplementation of infants versus supplementation of their breastfeeding mothers: A double-blind, randomized, placebo-controlled trial. Lancet Diabetes Endocrinol. 2014, 2, 197–209. [Google Scholar] [CrossRef]
- Ordookhani, A.; Pearcet, N.E.; Hedayati, M.; Mirmiran, P.; Salimi, S.; Azizi, F.; Braverman, E.L. Assessment of thyroid function and urinary and breast milk iodine concentrations in healthy newborns and their mothers in tehran. Clin. Endocrinol. 2007, 67, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Sukkhojaiwaratkul, D.; Mahachoklertwattana, P.; Poomthavorn, P.; Panburana, P.; Chailurkit, L.-O.; Khlairit, P.; Pongratanakul, S. Effects of maternal iodine supplementation during pregnancy and lactation on iodine status and neonatal thyroid-stimulating hormone. J. Perinatol. 2014, 34, 594–598. [Google Scholar] [CrossRef] [PubMed]
- Hashemipour, M.; Nasri, P.; Hovsepian, S.; Hadian, R.; Heidari, K.; Attar, H.M.; Amini, M.; Moohebat, L.; Sajadi, A.; Ajami, A. Urine and milk iodine concentrations in healthy and congenitally hypothyroid neonates and their mothers. Endokrynol. Polska 2010, 61, 371–376. [Google Scholar]
- Zimmermann, M.B.; Aeberli, I.; Andersson, M.; Assey, V.; Yorg, J.A.J.; Jooste, P.; Jukić, T.; Kartono, D.; Kusić, Z.; Pretell, E. Thyroglobulin is a sensitive measure of both deficient and excess iodine intakes in children and indicates no adverse effects on thyroid function in the uic range of 100–299 μg/L: A unicef/iccidd study group report. J. Clin. Endocrinol. Metab. 2013, 98, 1271–1280. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.; Brown, R.S.; Daumerie, C.; Hubalewska-Dydejczyk, A.; Negro, R.; Vaidya, B. 2014 European thyroid association guidelines for the management of subclinical hypothyroidism in pregnancy and in children. Eur. Thyroid J. 2014, 3, 76–94. [Google Scholar] [CrossRef] [PubMed]
- Shriraam, M.; Sridhar, M. Subclinical hypothyroidism in children. Indian Pediatr. 2014, 51, 889–895. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Flowers, J.W.; Tudiver, F.; Wilson, J.L.; Punyasavatsut, N. Subclinical thyroid disorders and cognitive performance among adolescents in the United States. BMC Pediatr. 2006, 6, 12. [Google Scholar] [CrossRef] [PubMed]
- Marwaha, R.K.; Tandon, N.; Garg, M.; Desai, A.; Kanwar, R.; Sastry, A.; Narang, A.; Arora, S.; Bhadra, K. Thyroid status two decades after salt iodization: Country-wide data in school children from india. Clin. Endocrinol. 2012, 76, 905–910. [Google Scholar] [CrossRef] [PubMed]
- Laurberg, P.; Cerqueira, C.; Ovesen, L.; Rasmussen, L.B.; Perrild, H.; Andersen, S.; Pedersen, I.B.; Carle, A. Iodine intake as a determinant of thyroid disorders in populations. Best Pract. Res. Clin. Endocrinol. 2010, 24, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Lazar, L.; Frumkin, R.B.-D.; Battat, E.; Lebenthal, Y.; Phillip, M.; Meyerovitch, J. Natural history of thyroid function tests over 5 years in a large pediatric cohort. J. Clin. Endocrinol. Metab. 2009, 94, 1678–1682. [Google Scholar] [CrossRef] [PubMed]
- Cioffi, M.; Gazzerro, P.; Vietri, M.T.; Magnetta, R.; Durantey, A.; D’Auria, A.; Puca, G.A.; Molinari, A.M. Serum concentration of free t3, free t4, and tsh in healthy children. J. Pediatr. Endocrinol. Metab. 2001, 14, 1635–1640. [Google Scholar] [CrossRef] [PubMed]
- Karavani, G.; Strich, D.; Edri, S.; Gillis, D. Increases in thyrotropin within the near-normal range are associated with increased triiodothyronine but not increased thyroxine in the pediatric age group. J. Clin. Endocrinol. Metab. 2014, 99, E1471–E1475. [Google Scholar] [CrossRef] [PubMed]
- Bona, G.; Prodam, F.; Monzani, A. Subclinical hypothyroidism in children: Natural history and when to treat. J. Clin. Res. Pediatr. Endocrinol. 2013, 5, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Eyal, O.; Blum, S.; Mueller, R.; Smith, F.O.; Rose, S.R. Improved growth velocity during thyroid hormone therapy in children with fanconi anemia and borderline thyroid function. Pediatr. Blood Cancer 2008, 51, 652–656. [Google Scholar] [CrossRef] [PubMed]
- Cetinkaya, E.; Aslan, A.T.; Vidinlisan, S.; Ocal, G. Height improvement by l-thyroxinetreatment in subclinical hypothyroidism. Pediatr. Int. 2003, 45, 534–537. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Dependent Variables | Predictor Variables | |
|---|---|---|
| Baseline | Follow-Up | |
| UIC baseline b | HAZ, WAZ, WHZ, age, gender, BMIC | - |
| UIC follow-up b | HAZ, WAZ, WHZ, breastfeeding status, age, gender | |
| TSH follow-up a | fT3, fT4, UIC, breastfeeding status, age, gender | |
| Tg b | fT3, fT4, UIC, breastfeeding status, age, gender | |
| fT4 a | UIC, Tg, breastfeeding status, age, gender | |
| fT3 a | UIC, Tg, breastfeeding status, age, gender | |
| Characteristics | Baseline (n = 111) | Follow-up (n = 289) |
|---|---|---|
| Age, months | 3.1 (2.2–4.8) | 31.4 (25.3–35.1) |
| Male | 40 [36.0] | 138 [47.8] |
| Female | 71 [64.0] | 151 [52.2] |
| Household size, number | 5.1 ± 1.9 | 5.3 ± 1.8 |
| Breast-fed | 111 [100.0] | 40 [13.8] |
| Weight-for-age, z-score | −0.8 ± 1.3 | −1.0 ± 0.9 |
| <−2 (underweight) | 18 [16.5] | 34 [11.8] |
| Length/height-for-age, z-score | −0.6 ± 1.2 | −1.6 ± 1.1 |
| <−2 (stunted) | 15 [13.8] | 96 [33.2] |
| Weight-for-length/height, z-score | −0.3 ± 1.2 | −0.1 ± 1.0 |
| <−2 (wasted) | 9 [8.2] | 11 [3.8] |
| Iodine status | ||
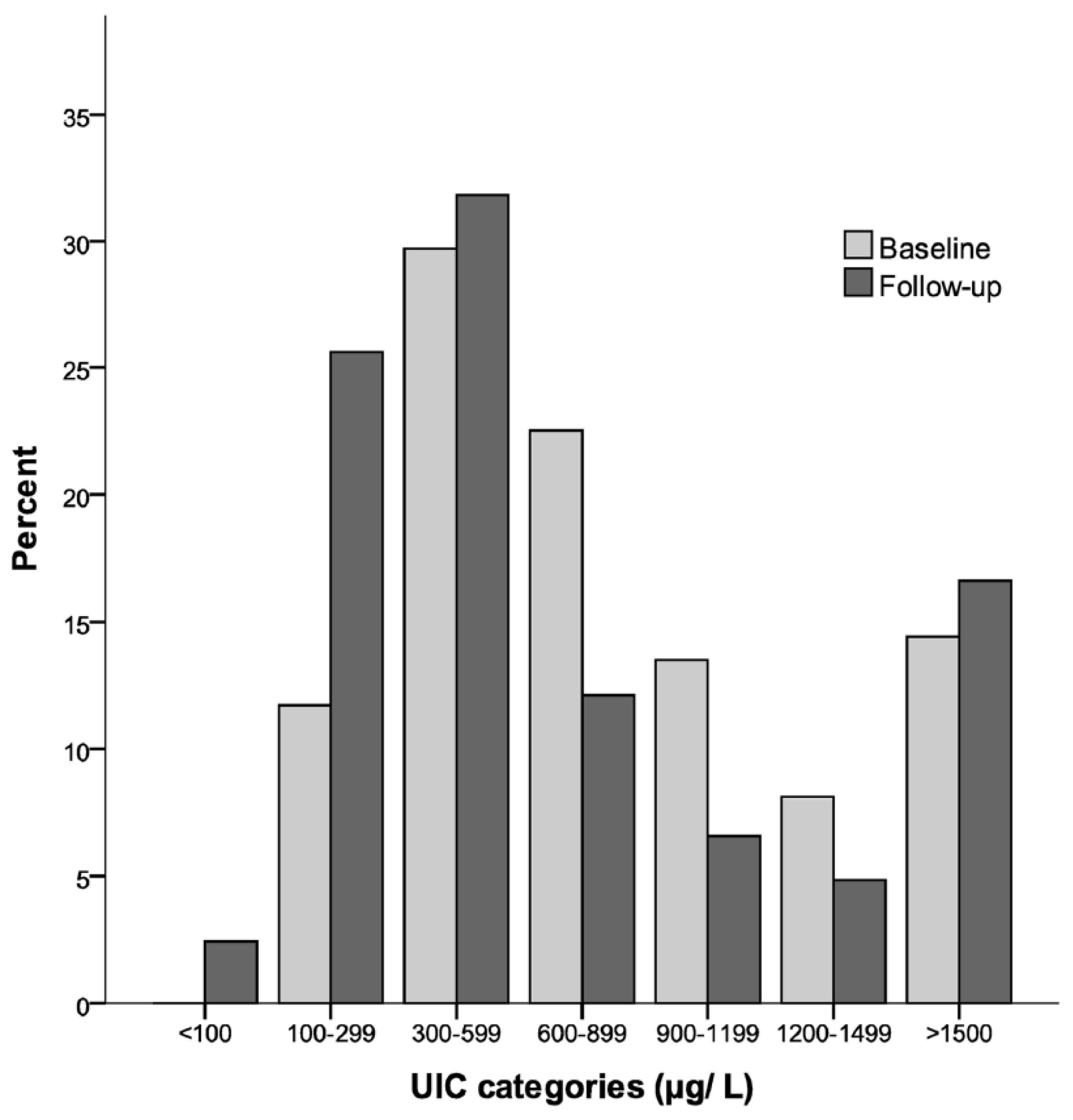
| UIC, µg/L | 722 (393−1133) | 458 (275−1026) * |
| BMIC, µg/L b | 479 (330−702) |
| Age in Months | Estimated Breast Milk Intake (g/Day) (3) | Estimated Iodine Intake from Breast Milk (µg/Day) a |
|---|---|---|
| 1 | 568 | 272 (187–399) |
| 2 | 636 | 305 (210–446) |
| 3 | 574 | 275 (189–403) |
| 4 | 643 | 308 (212–451) |
| 5 | 714 | 342 (236–501) |
| 6 | 611 | 293 (202–429) |
| Mean | 624 | 299 (206–438) |
| Thyroid Hormones and Thyroid Function Tests | Children (n = 289) | Reference Range |
|---|---|---|
| TSH, mIU/L | 3.1 (0.2–15.3) | 0.70–6.0 |
| fT4, pmol/L | 16.3 (11.2–21.8) | 12.3–22.8 |
| fT3, pmol/L | 6.9 (3.9–17.2) | 3.7–8.5 |
| Tg, µg/L | 38.4 (10.7–158.0) | <67 |
| Subclinical hypothyroidism b | 27 [9.3] | |
| Subclinical hyperthyroidism | 1 [0.4] | |
| Overt hyperthyroidism | 1 [0.4] | |
| fT4 low <12 pmol/L, normal TSH c | 3 [1.0] | |
| fT3 elevated >8.5 pmol/L, normal TSH d | 8 [2.8] | |
| Tg elevated >67 µg/L, normal thyroid tests | 28 [9.7] | |
| Total thyroid disturbance and/or elevated Tg | 68 [23.5] |
| Dependent Variables a | Predictor Variables | Unadjusted/Adjusted Coefficient (95% CI) d | p | Stand Beta | R2 |
|---|---|---|---|---|---|
| TSH | Tg mg/L | 6.2 (3.9−8.5) | <0.001 | 0.297 | |
| fT3 pmol/L | 0.09 (0.02−0.15) | 0.011 | 0.143 | 0.113 | |
| fT4 b | Tg c | 0.3 (0.01, 0.5) | 0.043 | 0.120 | 0.014 |
| fT3 | UIC follow-up mg/L | −0.04 (−0.06, −0.02) | <0.001 | −0.260 | 0.067 |
| Nutrition Status | Subclinical Hypothyroidism | p | |
|---|---|---|---|
| Yes (n = 27) | No (n = 260) b | ||
| Length/height-for-age, z-score | −2.2 ± 1.0 | −1.6 ± 1.1 | 0.004 |
| Weight-for-age, z-score | −1.4 ± 0.8 | −0.9 ± 1.0 | 0.012 |
| Weight-for-length/height, z-score | −0.3 ± 0.8 | −0.1 ± 1.0 | 0.349 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aakre, I.; Strand, T.A.; Bjøro, T.; Norheim, I.; Barikmo, I.; Ares, S.; Alcorta, M.D.; Henjum, S. Thyroid Function among Breastfed Children with Chronically Excessive Iodine Intakes. Nutrients 2016, 8, 398. https://doi.org/10.3390/nu8070398
Aakre I, Strand TA, Bjøro T, Norheim I, Barikmo I, Ares S, Alcorta MD, Henjum S. Thyroid Function among Breastfed Children with Chronically Excessive Iodine Intakes. Nutrients. 2016; 8(7):398. https://doi.org/10.3390/nu8070398
Chicago/Turabian StyleAakre, Inger, Tor A. Strand, Trine Bjøro, Ingrid Norheim, Ingrid Barikmo, Susana Ares, Marta Duque Alcorta, and Sigrun Henjum. 2016. "Thyroid Function among Breastfed Children with Chronically Excessive Iodine Intakes" Nutrients 8, no. 7: 398. https://doi.org/10.3390/nu8070398
APA StyleAakre, I., Strand, T. A., Bjøro, T., Norheim, I., Barikmo, I., Ares, S., Alcorta, M. D., & Henjum, S. (2016). Thyroid Function among Breastfed Children with Chronically Excessive Iodine Intakes. Nutrients, 8(7), 398. https://doi.org/10.3390/nu8070398