Impact of the Content of Fatty Acids of Oral Fat Tolerance Tests on Postprandial Triglyceridemia: Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Types of Studies
2.2. Types of Participants
2.3. Types of Outcomes
2.4. Search Methods for Identification of Studies
2.5. Inclusion Criteria
2.6. Exclusion Criteria
2.7. Selection of the Studies
2.8. Assessment of Risk of Bias in Included Studies
2.9. Statistical Analysis
3. Results
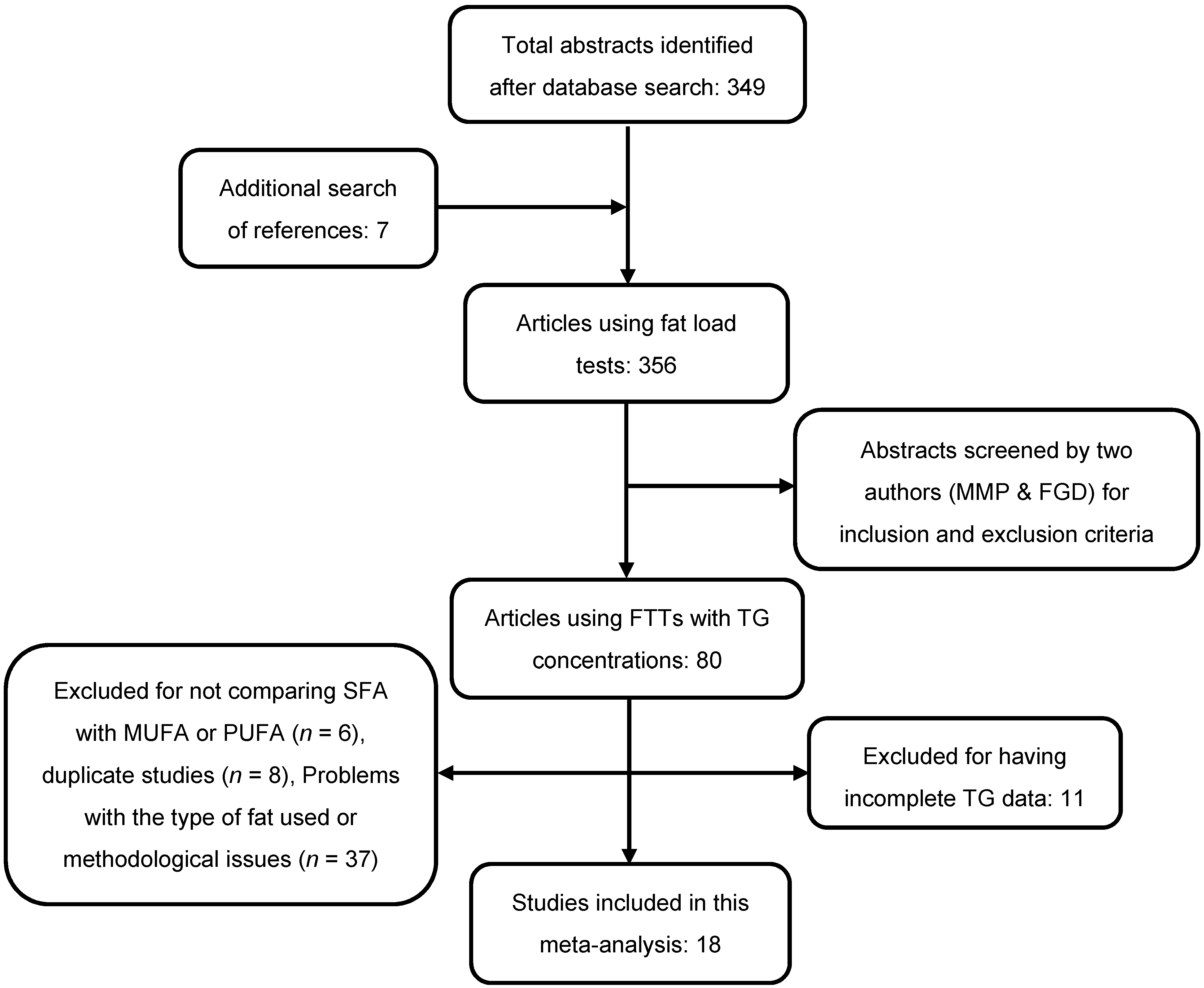
3.1. Final Selection of the Studies, and Review of Their Methodological Details
3.2. Clinical Results
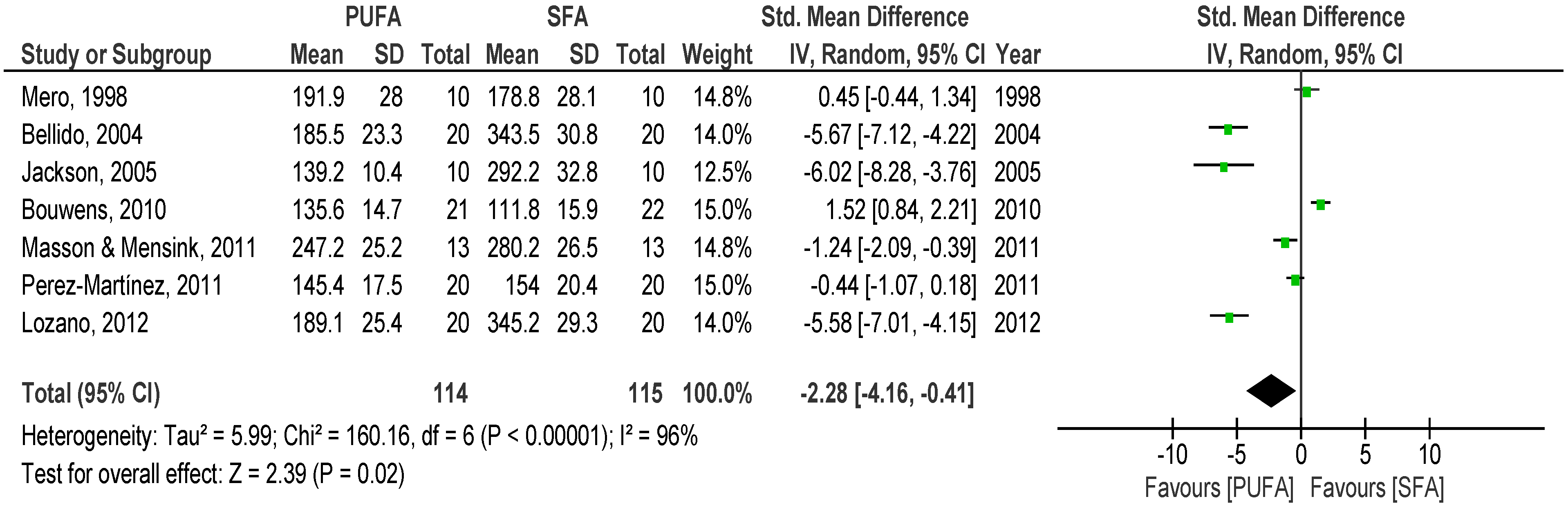
3.2.1. SFA versus PUFA
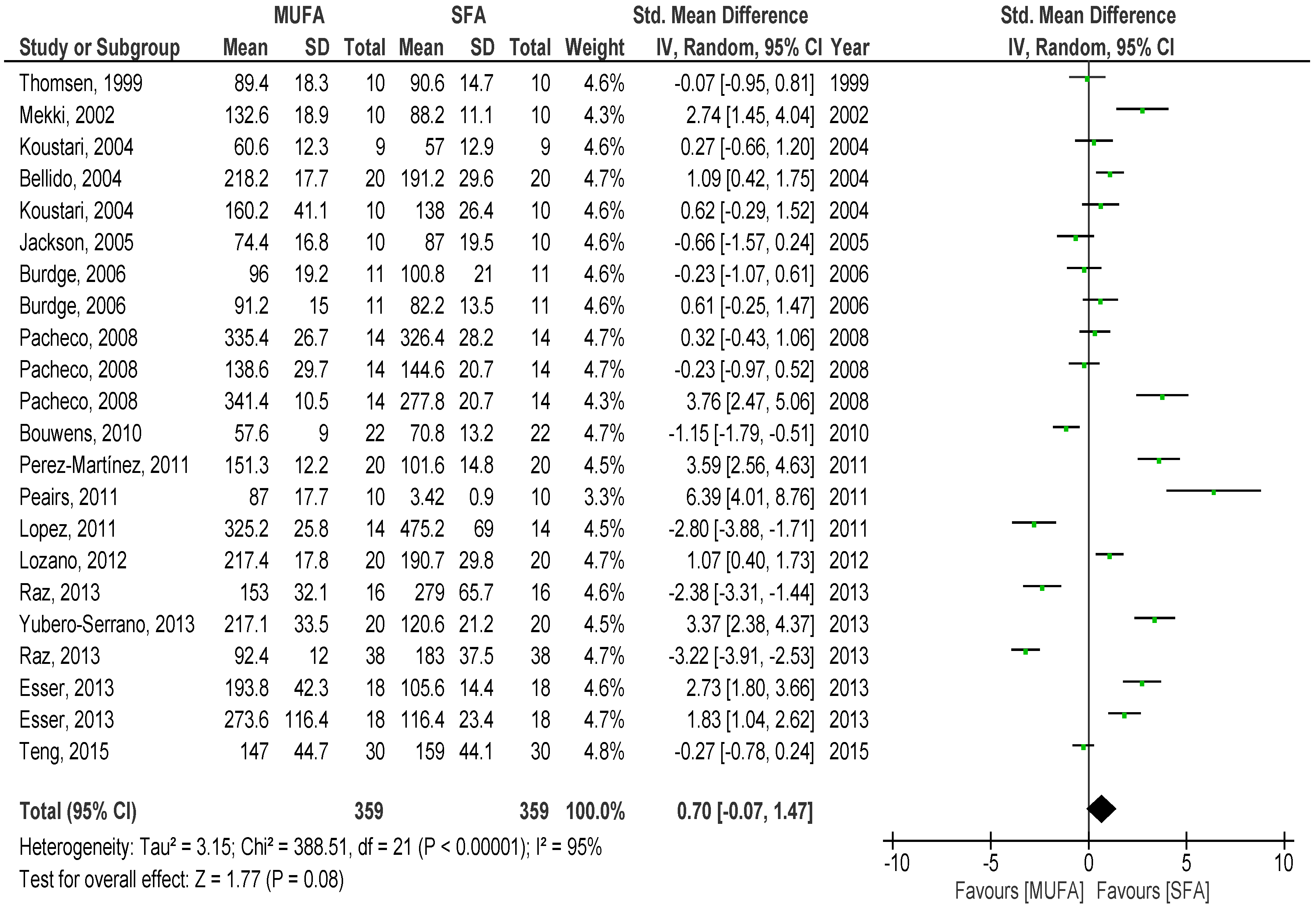
3.2.2. SFA versus MUFA
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kolovou, G.D.; Mikhailidis, D.P.; Kovar, J.; Lairon, D.; Nordestgaard, B.G.; Chye Ooi, T.; Perez-Martinez, P.; Bilianou, H.; Anagnostopoulou, K.; Panotopoulos, G. Assessment and clinical relevance of non-fasting and postprandial triglycerides: An expert panel statement. Curr. Vasc. Pharmacol. 2011, 9, 258–270. [Google Scholar] [CrossRef] [PubMed]
- DECODE Study Group; European Diabetes Epidemiology Group. Glucose tolerance and mortality: Comparison of WHO and American Diabetes Association diagnostic criteria. Lancet 1999, 354, 617–621. [Google Scholar]
- World Health Organization; International Diabetes Federation. Definition and Diagnosis of Diabetes Mellitus and Intermediate Hyperglycaemia: Report of WHO/IDF Consultation; IDF: Geneve, Switzerland, 2006. [Google Scholar]
- Nordestgaard, B.G.; Benn, M.; Schnohr, P.; Tybjærg-Hansen, A. Nonfasting triglycerides and risk of myocardial infarction, ischemic heart disease, and death in men and women. JAMA 2007, 298, 299–308. [Google Scholar] [CrossRef] [PubMed]
- Bansal, S.; Buring, J.E.; Rifai, N.; Mora, S.; Sacks, F.M.; Ridker, P.M. Fasting compared with nonfasting triglycerides and risk of cardiovascular events in women. JAMA 2007, 298, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Esposito, K.; Giugliano, D. Diet and inflammation: A link to metabolic and cardiovascular diseases. Eur. Heart J. 2006, 27, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Jackson, K.G.; Poppitt, S.D.; Minihane, A.M. Postprandial lipemia and cardiovascular disease risk: Interrelationships between dietary, physiological and genetic determinants. Atherosclerosis 2012, 220, 22–33. [Google Scholar] [CrossRef] [PubMed]
- Lairon, D.; Lopez-Miranda, J.; Williams, C. Methodology for studying postprandial lipid metabolism. Eur. J. Clin. Nutr. 2007, 61, 1145–1161. [Google Scholar] [CrossRef] [PubMed]
- Mihas, C.; Kolovou, G.D.; Mikhailidis, D.P.; Kovar, J.; Lairon, D.; Nordestgaard, B.G.; Chye Ooi, T.; Perez-Martinez, P.; Bilianou, H.; Anagnostopoulou, K.; et al. Diagnostic Value of Postprandial Triglyceride Testing in Healthy Subjects: A Meta-Analysis. Curr. Vasc. Pharmacol. 2011, 9, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Peairs, A.D.; Rankin, J.W.; Lee, Y.W. Effects of acute ingestion of different fats on oxidative stress and inflammation in overweight and obese adults. Nutr. J. 2011, 10, 122. [Google Scholar] [CrossRef] [PubMed]
- Raz, O.; Steinvil, A.; Berliner, S.; Rosenzweig, T.; Justo, D.; Shapira, I. The effect of two iso-caloric meals containing equal amounts of fats with a different fat composition on the inflammatory and metabolic markers in apparently healthy volunteers. J. Inflamm. 2013, 10, 3. [Google Scholar] [CrossRef] [PubMed]
- Masson, C.J.; Mensink, R.P. Exchanging saturated fatty acids for (n-6) polyunsaturated fatty acids in a mixed meal may decrease postprandial lipemia and markers of inflammation and endothelial activity in overweight men. J. Nutr. 2011, 141, 816–821. [Google Scholar] [CrossRef] [PubMed]
- Esser, D.; van Dijk, S.; Oosterink, E.; Müller, M.; Afman, L.A. A high-fat SFA, MUFA, or n3 PUFA challenge affects the vascular response and initiates an activated state of cellular adherence in lean and obese middle-aged men. J. Nutr. 2013, 96, 489–500. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0; The Cochrane Collaboration: London, UK, 2011; Available online: http://community.cochrane.org/handbook (accessed on 16 January 2015).
- Wolever, T.M. Effect of blood sampling schedule and method of calculating the area under the curve on validity and precision of glycaemic index values. Br. J. Nutr. 2004, 91, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Review Manager (RevMan®); Version 5.3; The Nordic Cochrane Centre; The Cochrane Collaboration: Copenhagen, Denmark, 2014.
- Mero, N.; Syvanne, M.; Rosseneu, M.; Labeur, C.; Hilden, H.; Taskinen, M.R. Comparison of three fatty meals in healthy normolipidaemic men: High post-prandial retinyl ester response to soybean oil. Eur. J. Clin. Investig. 1998, 28, 407–415. [Google Scholar] [CrossRef]
- Thomsen, C.; Rasmussen, O.; Lousen, T.; Holst, J.J.; Fenselau, S.; Schrezenmeir, J.; Hermansen, K. Differential effects of saturated and monounsaturated fatty acids on postprandial lipemia and incretin responses in healthy subjects. Am. J. Clin. Nutr. 1999, 69, 1135–1143. [Google Scholar] [PubMed]
- Mekki, N.; Charbonnier, M.; Borel, P.; Leonardi, J.; Juhel, C.; Portugal, H.; Lairon, D. Butter differs from olive oil and sunflower oil in its effects on postprandial lipemia and triacylglycerol-rich lipoproteins after single mixed meals in healthy young men. J. Nutr. 2002, 132, 3642–3649. [Google Scholar] [PubMed]
- Bellido, C.; López-Miranda, J.; Blanco-Colio, J.M.; Pérez-Martínez, P.; Muriana, F.J.; Martín-Ventura, J.L.; Marín, C.; Gómez, P.; Fuentes, F.; Egido, J.; et al. Butter and walnuts, but not olive oil, elicit postprandial activation of nuclear transcription factor κB in peripheral blood mononuclear cells from healthy men. Am. J. Clin. Nutr. 2004, 80, 1487–1491. [Google Scholar] [PubMed]
- Koustari, C.; Zagana, A.; Tzoras, I.; Sidossis, L.S.; Matalas, A.L. Gender influence on plasma triacylglycerol response to meals with different monounsaturated and saturated fatty acid content. Eur. J. Clin. Nutr. 2004, 58, 495–502. [Google Scholar]
- Jackson, K.G.; Wolstencroft, E.J.; Bateman, P.A.; Yaqoob, P.; Williams, C.M. Acute effects of meal fatty acids on postprandial NEFA, glucose and apo E response: Implications for insulin sensitivity and lipoprotein regulation? Br. J. Nutr. 2005, 93, 693–700. [Google Scholar] [CrossRef] [PubMed]
- Teng, K.T.; Chang, C.Y.; Kanthimathi, M.S.; Tan, A.T.; Nesaretnam, K. Effects of amount and type of dietary fats in postprandial lipemia and thrombogenic markers in individuals with metabolic syndrome. Atherosclerosis 2015, 242, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Pacheco, Y.M.; López, S.; Bermúdez, B.; Abia, R.; Villar, J.; Muriana, F.J. A meal rich in oleic acid beneficially modulates postprandial sICAM-1 and sVCAM-1 in normotensive and hypertensive hypertriglyceridemic. J. Nutr. Biochem. 2008, 19, 200–205. [Google Scholar] [CrossRef] [PubMed]
- Lopez, S.; Bermudez, B.; Ortega, A.; Varela, L.M.; Pacheco, Y.M.; Villar, J.; Abia, R.; Muriana, F.J. Effects of meals rich in either monounsaturated or saturated fat on lipid concentrations and on insulin secretion and action in subjects with high fasting triglyceride concentrations. Am. J. Clin. Nutr. 2011, 93, 494–499. [Google Scholar] [CrossRef] [PubMed]
- Bouwens, M.; Bromhaar, M.G.; Jansen, J.; Müller, M.; Afman, L.A. Postprandial dietary lipid-specific effects on human peripheral blood mononuclear cell gene expression profiles. Am. J. Clin. Nutr. 2010, 91, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Burdge, G.C.; Powell, J.; Calder, P.C. Lack of effect of meal fatty acid composition on postprandial lipid, glucose and insulin responses in men and women aged 50–65 years consuming their habitual diets. Br. J. Nutr. 2006, 96, 489–500. [Google Scholar] [PubMed]
- Perez-Martinez, P.; Ordovas, J.M.; Garcia-Rios, A.; Delgado-Lista, J.; Delgado-Casado, N.; Cruz-Teno, C.; Camargo, A.; Yubero-Serrano, E.M.; Rodriguez, F.; Perez-Jimenez, F.; et al. Consumption of diets with different type of fat influences triacylglycerols-rich lipoproteins particle number and size during the postprandial state. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Lozano, A.; Perez-Martinez, P.; Delgado-Lista, J.; Marin, C.; Cortes, B.; Rodriguez-Cantalejo, F.; Gomez-Luna, M.J.; Cruz-Teno, C.; Perez-Jimenez, F.; Lopez-Miranda, J. Body mass interacts with fat quality to determine the postprandial lipoprotein response in healthy young adults. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Yubero-Serrano, E.M.; Gonzalez-Guardia, L.; Rangel-Zuñiga, O.; Delgado-Casado, N.; Delgado-Lista, J.; Perez-Martinez, P.; Garcia-Rios, A.; Caballero, J.; Marin, C.; Gutierrez-Mariscal, F.M.; et al. Postprandial antioxidant gene expression is modified by Mediterranean diet supplemented with coenzyme Q10 in elderly men and women. Age 2013, 35, 159–170. [Google Scholar] [CrossRef] [PubMed]
- Lindman, A.S.; Veierød, M.B.; Tverdal, A.; Pedersen, J.I.; Selmer, R. Nonfasting triglycerides and risk of cardiovascular death in men and women from the Norwegian Counties Study. Eur. J. Epidemiol. 2010, 25, 789–798. [Google Scholar] [CrossRef] [PubMed]
- Siri-Tarino, P.W.; Sun, Q.; Hu, F.B.; Krauss, R.M. Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease. Am. J. Clin. Nutr. 2010, 91, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Vafeiadou, K.; Weech, M.; Altowaijri, H.; Todd, S.; Yaqoob, P.; Jackson, K.G.; Lovegrove, J.A. Replacement of saturated with unsaturated fats had no impact on vascular function but beneficial effects on lipid biomarkers, E-selectin, and blood pressure: Results from the randomized, controlled Dietary Intervention and VAScular function (DIVAS) study. Am. J. Clin. Nutr. 2015, 102, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Mani, D.N.; Bawankule, D.; Saroj, B.K. Hyperlipidemic model: Studying lipid profile in small experimental animal. Int. J. Pharm. Pharm. Sci. 2012, 4, 337–340. [Google Scholar]
- Vessby, B.; Uusitupa, M.; Hermansen, K.; Riccardi, G.; Rivellese, A.A.; Tapsell, L.C.; Nälsén, C.; Berglund, L.; Louheranta, A.; Rasmussen, B.M.; et al. Substituting dietary saturated for monounsaturated fat impairs insulin sensitivity in healthy men and women: The KANWU study. Diabetologia 2001, 44, 312–939. [Google Scholar] [CrossRef] [PubMed]
- Milanski, M.; Degasperi, G.; Coope, A.; Morari, J.; Denis, R.; Cintra, D.E.; Tsukumo, D.M.; Anhe, G.; Amaral, M.E.; Takahashi, H.K.; et al. Saturated fatty acids produce an inflammatory response predominantly through the activation of TLR4 signaling in hypothalamus: Implications for the pathogenesis of obesity. J. Neurosci. 2009, 29, 359–370. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.A.; Gu, W.; Lee, I.A.; Joh, E.H.; Kim, D.H. High fat diet-induced gut microbiota exacerbates inflammation and obesity in mice via the TLR4 signaling pathway. PLoS ONE 2012, 7, e47713. [Google Scholar] [CrossRef] [PubMed]
- Teng, K.T.; Chang, C.Y.; Chang, L.F.; Nesaretnam, K. Modulation of obesity-induced inflammation by dietary fats: Mechanisms and clinical evidence. Nutr. J. 2014, 13, 12. [Google Scholar] [CrossRef] [PubMed]
- Bos, M.B.; de Vries, J.H.; Feskens, E.J.; van Dijk, S.J.; Hoelen, D.W.; Siebelink, E.; Heijligenberg, R.; de Groot, L.C. Effect of a high monounsaturated fatty acids diet and a Mediterranean diet on serum lipids and insulin sensitivity in adults with mild abdominal obesity. Nutr. Metab. Cardiovasc. Dis. 2010, 20, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Talukdar, S.; Bae, E.J.; Imamura, T.; Morinaga, H.; Fan, W.; Li, P.; Lu, W.J.; Watkins, S.M.; Olefsky, J.M. GPR120 is an Omega-3 Fatty Acid Receptor Mediating Potent Anti-Inflammatory and Insulin Sensitizing Effects. Cell 2010, 142, 687–698. [Google Scholar]
- Lopez-Miranda, J.; Marin, C. Dietary, physiological, and genetic impacts on postprandial lipid. In Fat Detection: Taste, Texture, and Post Ingestive Effects; Montmayeur, J.P., le Coutre, J., Eds.; CRC Press: Boca Raton, FL, USA, 2009; pp. 417–460. [Google Scholar]
- Riccardi, G.; Bozzetto, L.; Annuzzi, G. Postprandial lipid metabolism. Scand. J. Food Nutr. 2006, 50, 99–106. [Google Scholar] [CrossRef]
- Wang, X.; Magkos, F.; Mittendorfer, B. Sex differences in lipid and lipoprotein profile metabolism: It´s not just about sex hormones. J. Clin. Endocrinol. Metab. 2011, 96, 885–893. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, G.; Ecker, J. The opposing effects of n−3 and n−6 fatty acids. Prog. Lipid Res. 2008, 47, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.D.; Sievenpiper, J.L.; Souza, R.J.; Cozma, A.I.; Chiavaroli, L.; Ha, V.; Mirrahimi, A.; Carleton, A.J.; Di Buono, M.; Jenkins, A.L.; et al. Effect of fructose on postprandial triglycerides: A systematic review and meta-analysis of controlled feeding trials. Atherosclerosis 2014, 232, 125–133. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study, Year, Country | Study Sample | Meal Type | Energy Content in the Test | Amount of Fatty Acids | Amount and Type of SFA | Amount and Type of MUFA | Amount and Type of PUFA | % Fat Meal Test | Times of TG Data | Type of TG Measure |
|---|---|---|---|---|---|---|---|---|---|---|
| Mero et al., 1998, Finland | 10 men; Mean age: 36.8 ± 3.1 years; Non-obese; Without health problems | Liquid meal | 665/616 kcal | 63 g | 63 g whipping cream | - | 63 g soybean oil | 85% | 0, 3, 4, 6 and 8 h | Plasma TG (mmol/L) |
| Thomsen et al., 1999, Denmark | 5 men + 5 women; Mean age: 23 ± 2 years; No information about BMI; Healthy | Meal | No info | 80 g | 100 g butter | 80 g olive oil | - | No info | 0, 1, 2, 3, 4, 5, 6, 7 and 8 h | Plasma TG (mmol/L) |
| Mekki et al., 2002, France | 10 men; Age range: 20–29 years; Mean BMI 22.1 kg/m2; Without health problems | Meal | No info | 40 g | 40 g butter | 40 g olive oil | 40 g sunflower | No info | 0, 1, 2, 3, 4, 5, 6 and 7 h | Changes from baseline in (mmol/L) |
| Bellido, 2004, Spain | 20 young male adults; No age or BMI information; Without health problems | Meal | 50%–66% of the subjects’; daily normal intake of calories | 1 g/kg of body weight (65%) | 38% SFA (butter) | 38% MUFA (olive oil) | 16% PUFA (walnut) | 65% | 0, 1, 2, 4, 6, 8.5 and 11 h | Plasma TG (mg/dL) |
| Koustari et al., 2004, Greece | 10 men + 10 women; Age range: 18–40 years; BMI <27 kg/m2; Healthy | Meal | 1100 kcal | 60 g (48%) | 32 g butter | 40 g (olive oil) | - | 48% | 0, 1, 2, 3, 4, 5 and 6 h | Plasma TG (mmol/L) |
| Jackson et al., 2005, UK | 10 men; Mean age: 48 ± 9 years; Mean BMI: 25 ± 3 kg/m2; Without health problems | Meal | 1000 kcal | 50 g | 50 g (palm + cocoa) | 50 g (olive oil) | 50 g safflower oil | No info | 0, 1, 2, 3, 4, 5, 6, 7 and 8 h | Plasma TG (mmol/L) |
| Pacheco et al., 2008, Spain | 42 men; Age range: 21-38 years; BMI <27 kg/m2; 28 hypertriglyceridemic (14 normotensives and 14 hypertensives) and 14 healthy men | Meal | 885 kcal | 40 g/m2 body surface area | 76.8 to 79.2 g of high palmitic sunflower oil | 76.8 to 79.2 g of refined olive oil | - | 72% fat | 0, 2, 4, 6 and 8 h | Changes from baseline (mmol/L) |
| Lopez et al., 2011, Spain | 14 men; Mean age: 33 ± 7 years; Mean BMI: 24.2 ± 5.1 kg/m2; With hyperlipoproteinemia | Meal | 800 kcal | 50 g/m2 body surface area | 65.3% butter | 81% refined olive oil | - | 72% | 0, 1, 2, 3, 4, 5, 6, 7 and 8 h | Plasma TG (mmol/L) |
| Masson and Mensinsk, 2011, The Netherlands | 13 men; Age range: 18–70 years; BMI: 25–30 kg/m2; Without health problems | Meal | 978/1015 kcal | 50 g | 50 g butter | - | 40 g margarine + 10 g safflower oil | 51% | 0, 2, 4 and 6 h | Changes from baseline in (mmol/L) |
| Bouwens et al., 2010, The Netherlands | 21 men; Age range: 19–27 years; BMI range: 18–27 kg/m2 | Shake | 2824 kJ/675 kcal | 55 g | 70% SFA (butter) | 80% MUFA (High oleic sunflower oil) | 65% PUFA (40% DHA) | 73% | 0, 2, 4, 6 and 8 h | Changes from baseline in (mmol/L) (author provided data) |
| Burdge et al., 2010, UK | 11 women + 11 men; Age range: 50–65 years; BMI: 20–30 kg/m2; Without dyslipidemia | Shake | No info | 47–55 g | 38% SFA | 43% MUFA | 25% PUFA | No info | 0.5, 1, 1.5, 2, 2.5, 3, 4, 5 and 6 h | Changes from baseline (mmol/L) |
| Peairs et al., 2011, USA | 11 adults; Mean age: 31.3 ± 3.3 years; BMI >27 kg/m2; Without health problems | Shake | 1267 kcal | 85 g | 59% refined palm oil | 59% refined olive oil | 59% refined olive oil + 4 g omega-3 | 59% | 0, 1, 2, 4 and 6 h | Plasma TG (mmol/L) |
| Perez-Martínez et al., 2011, Spain | 20 men; Mean age: 22 years; BMI: 24.5 kg/m2; Without health problems | Meal | 60% daily intake | 1 g/kg of body weight | 35% SFA (butter) | 36% MUFA (olive oil) | 16% PUFA (walnuts) | 60% | 0, 1, 2, 3, 4, 5, 6, 8.5 and 11 h | Plasma TG (mmol/L) |
| Lozano et al., 2012, Spain | 21 men; Mean age: 23 years; BMI <30 kg/m2; Without health problems | Meal | No info | 1 g fat/kg body weight | 60% fat (35% SFA—butter) | 60% fat (38% MUFA—extra-virgin olive oil) | 60% fat (16% PUFA—walnuts) | 60% | 0, 1, 2, 3, 4, 5, 6, 7 and 8 h | Plasma TG (mmol/L) |
| Esser et al., 2013, The Netherlands | 36 men; Age range: 50–70 years; 18 lean + 18 obese; Without health problems | Shake | 990 kcal | 95 g | 54% total fat (palm oil) | 83% total fat (high oleic sunflower oil) | 40% total fat (n 3) (40 g palm oil + 55 g marinol) | 88% | 0, 2 and 4 h | Changes from baseline (mmol/L) |
| Raz et al., 2013, Israel | 16 men + 38 women; BMI <25.9 kg/m2; Healthy | Meal | 1161 kcal | 74 g | 56% (24 g SFA) | 56% (51 g MUFA) | - | 56% | 0, 2 and 4 h | Plasma TG (mg/dL) |
| Yubero-Serrano et al., 2013 | 10 men + 10 women; age ≥65 years; BMI: 20–40 kg/m2; Without health problems | Meal | No info | 0.7 g fat/kg of body weight | 22% SFA (butter) | 24% MUFA (olive oil) | - | 38% | 0, 2 and 4 h | Plasma TG (mg/dL) |
| Teng et al., 2015, Malasya | 15 men + 15 women; Mean age:33.8 ± 1.7 years; Mean BMI: 30.9 ± 0.8 kg/m2; With metabolic syndrome but without chronic diseases | Meal | 855 kcal | 50.9 g | Palm olein 22.9 g SFA | High-oleic sunflower oil 42.5 g MUFA | Sunflower oil 25.7 g PUFA | - | 0, 30 min, 1, 2, 3, 4, 5 and 6 h | Plasma TG (mmol/L) |
| Risk of Bias for Cross-over Clinical Trials | ||||
|---|---|---|---|---|
| Study | Was use of a crossover design appropriate? | Is it clear that the order of receiving treatments was randomized? | Can it be assumed that the trial was not biased from carry-over effects? | Are unbiased data available? |
| Mero et al., 1998, Finland | Yes | Yes | Yes | No |
| Thomsen et al., 1999, Denmark | Yes | Yes | Yes | Yes |
| Mekki et al., 2002, France | Yes | Yes | Yes | Yes |
| Bellido et al., 2004, Spain | Yes | Yes | Yes | Yes |
| Koustari et al., 2004, Greece | Yes | Yes | Yes | Yes |
| Jackson et al., 2005, UK | Yes | No | Yes | Yes |
| Pacheco et al., 2008, Spain | Yes | Yes | Yes | Yes |
| Lopez et al., 2011, Spain | Yes | Yes | Yes | Yes |
| Masson and Mensinsk, 2011, The Netherlands | Yes | Yes | No | Yes |
| Bouwens et al., 2010, The Netherlands | Yes | Yes | Yes | Yes |
| Burdge et al., 2010, UK | Yes | Yes | Yes | Yes |
| Peairs et al., 2011, USA | Yes | Yes | Yes | No |
| Perez-Martínez et al., 2011, Spain | Yes | Yes | Yes | Yes |
| Tholstrup et al., 2011, Denmark | Yes | Yes | Yes | Yes |
| Lozano et al., 2012, Spain | Yes | Yes | Yes | Yes |
| Esser et al., 2013, The Netherlands | Yes | Yes | Yes | Yes |
| Raz et al., 2013, Israel | Yes | Yes | Yes | No |
| Yubero-Serrano et al., 2013, Spain | Yes | Yes | Yes | Yes |
| Teng et al., 2015, Malaysia | Yes | Yes | Yes | Yes |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monfort-Pires, M.; Delgado-Lista, J.; Gomez-Delgado, F.; Lopez-Miranda, J.; Perez-Martinez, P.; Ferreira, S.R.G. Impact of the Content of Fatty Acids of Oral Fat Tolerance Tests on Postprandial Triglyceridemia: Systematic Review and Meta-Analysis. Nutrients 2016, 8, 580. https://doi.org/10.3390/nu8090580
Monfort-Pires M, Delgado-Lista J, Gomez-Delgado F, Lopez-Miranda J, Perez-Martinez P, Ferreira SRG. Impact of the Content of Fatty Acids of Oral Fat Tolerance Tests on Postprandial Triglyceridemia: Systematic Review and Meta-Analysis. Nutrients. 2016; 8(9):580. https://doi.org/10.3390/nu8090580
Chicago/Turabian StyleMonfort-Pires, Milena, Javier Delgado-Lista, Francisco Gomez-Delgado, José Lopez-Miranda, Pablo Perez-Martinez, and Sandra Roberta Gouvea Ferreira. 2016. "Impact of the Content of Fatty Acids of Oral Fat Tolerance Tests on Postprandial Triglyceridemia: Systematic Review and Meta-Analysis" Nutrients 8, no. 9: 580. https://doi.org/10.3390/nu8090580
APA StyleMonfort-Pires, M., Delgado-Lista, J., Gomez-Delgado, F., Lopez-Miranda, J., Perez-Martinez, P., & Ferreira, S. R. G. (2016). Impact of the Content of Fatty Acids of Oral Fat Tolerance Tests on Postprandial Triglyceridemia: Systematic Review and Meta-Analysis. Nutrients, 8(9), 580. https://doi.org/10.3390/nu8090580