Dietary Intake after Weight Loss and the Risk of Weight Regain: Macronutrient Composition and Inflammatory Properties of the Diet



Abstract
:1. Introduction
2. Methods
2.1. Subjects
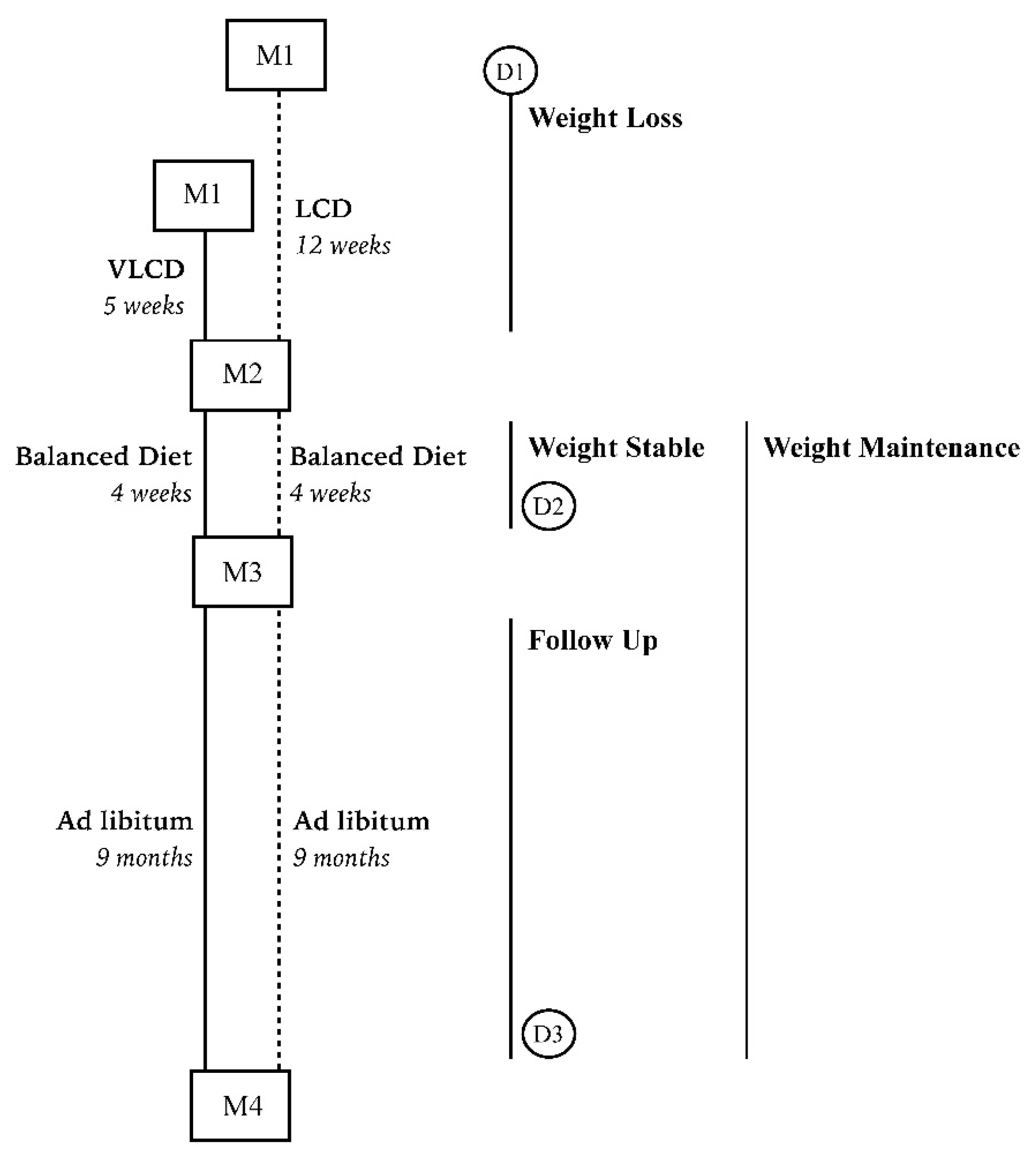
2.2. The Dietary Intervention Program
2.3. Measurements
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- GBD 2015 Obesity Collaborators; Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; et al. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Tremmel, M.; Gerdtham, U.-G.; Nilsson, P.; Saha, S. Economic Burden of Obesity: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2017, 14, 435. [Google Scholar] [CrossRef]
- Ross, R. The challenge of obesity treatment: Avoiding weight regain. CMAJ 2009, 180, 997. [Google Scholar] [CrossRef] [PubMed]
- Weiss, E.C.; Galuska, D.A.; Kettel Khan, L.; Gillespie, C.; Serdula, M.K. Weight Regain in U.S. Adults Who Experienced Substantial Weight Loss, 1999–2002. Am. J. Prev. Med. 2007, 33, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Turk, M.W.; Yang, K.; Hravnak, M.; Sereika, S.M.; Ewing, L.J.; Burke, L.E. Randomized clinical trials of weight-loss maintenance: A review. J. Cardiovasc. Nurs. 2009, 24, 58–80. [Google Scholar] [CrossRef] [PubMed]
- Kraschnewski, J.L.; Boan, J.; Esposito, J.; Sherwood, N.E.; Lehman, E.B.; Kephart, D.K.; Sciamanna, C.N. Long-term weight loss maintenance in the United States. Int. J. Obes. 2010, 34, 1644–1654. [Google Scholar] [CrossRef]
- Greenway, F.L. Physiological adaptations to weight loss and factors favouring weight regain. Int. J. Obes. 2015, 39, 1188–1196. [Google Scholar] [CrossRef]
- Mariman, E.C.M. Human biology of weight maintenance after weight loss. J. Nutrigenet. Nutrigenom. 2012, 5, 13–25. [Google Scholar] [PubMed]
- Elfhag, K.; Rössner, S. Who succeeds in maintaining weight loss? A conceptual review of factors associated with weight loss maintenance and weight regain. Obes. Rev. 2005, 6, 67–85. [Google Scholar] [CrossRef] [PubMed]
- Aller, E.E.J.G.; Larsen, T.M.; Claus, H.; Lindroos, A.K.; Kafatos, A.; Pfeiffer, A.; Martinez, J.A.; Handjieva-Darlenska, T.; Kunesova, M.; Stender, S.; et al. Weight loss maintenance in overweight subjects on ad libitum diets with high or low protein content and glycemic index: The DIOGENES trial 12-month results. Int. J. Obes. 2014, 38, 1511–1517. [Google Scholar] [CrossRef] [PubMed]
- Larsen, T.M.; Dalskov, S.-M.; van Baak, M.; Jebb, S.A.; Papadaki, A.; Pfeiffer, A.F.H.; Martinez, J.A.; Handjieva-Darlenska, T.; Kunešová, M.; Pihlsgård, M.; et al. Diets with high or low protein content and glycemic index for weight-loss maintenance. N. Engl. J. Med. 2010, 363, 2102–2113. [Google Scholar] [CrossRef] [PubMed]
- Claessens, M.; van Baak, M.A.; Monsheimer, S.; Saris, W.H.M. The effect of a low-fat, high-protein or high-carbohydrate ad libitum diet on weight loss maintenance and metabolic risk factors. Int. J. Obes. 2009, 33, 296–304. [Google Scholar] [CrossRef] [PubMed]
- Westerterp-Plantenga, M.S.; Lejeune, M.P.G.M.; Nijs, I.; van Ooijen, M.; Kovacs, E.M.R. High protein intake sustains weight maintenance after body weight loss in humans. Int. J. Obes. 2004, 28, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Hursel, R.; Westerterp-Plantenga, M.S. Green tea catechin plus caffeine supplementation to a high-protein diet has no additional effect on body weight maintenance after weight loss. Am. J. Clin. Nutr. 2009, 89, 822–830. [Google Scholar] [CrossRef] [PubMed]
- Sacks, F.M.; Bray, G.A.; Carey, V.J.; Smith, S.R.; Ryan, D.H.; Anton, S.D.; McManus, K.; Champagne, C.M.; Bishop, L.M.; Laranjo, N.; et al. Comparison of Weight-Loss Diets with Different Compositions of Fat, Protein, and Carbohydrates. N. Engl. J. Med. 2009, 360, 859–873. [Google Scholar] [CrossRef] [PubMed]
- Kjølbæk, L.; Sørensen, L.B.; Søndertoft, N.B.; Rasmussen, C.K.; Lorenzen, J.K.; Serena, A.; Astrup, A.; Larsen, L. Protein supplements after weight loss do not improve weight maintenance compared with recommended dietary protein intake despite beneficial effects on appetite sensation and energy expenditure: A randomized, controlled, double-blinded trial. Am. J. Clin. Nutr. 2017, 106, 684–697. [Google Scholar] [CrossRef] [PubMed]
- Roumans, N.J.T.; Vink, R.G.; Fazelzadeh, P.; Van Baak, M.A.; Mariman, E.C.M. A role for leukocyte integrins and extracellular matrix remodeling of adipose tissue in the risk of weight regain after weight loss. Am. J. Clin. Nutr. 2017, 105, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Roumans, N.J.T.; Camps, S.G.; Renes, J.; Bouwman, F.G.; Westerterp, K.R.; Mariman, E.C.M. Weight loss-induced stress in subcutaneous adipose tissue is related to weight regain. Br. J. Nutr. 2016, 115, 913–920. [Google Scholar] [CrossRef] [PubMed]
- Cavicchia, P.P.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Hebert, J.R. A New Dietary Inflammatory Index Predicts Interval Changes in Serum High-Sensitivity C-Reactive Protein. J. Nutr. 2009, 139, 2365–2372. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hébert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Tabung, F.; Hébert, J.R. A population-based dietary inflammatory index predicts levels of C-reactive protein in the Seasonal Variation of Blood Cholesterol Study (SEASONS). Public Health Nutr. 2014, 17, 1825–1833. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Hébert, J.R.; Rietzschel, E.R.; De Buyzere, M.L.; Langlois, M.; Debruyne, E.; Marcos, A.; Huybrechts, I. Associations between dietary inflammatory index and inflammatory markers in the Asklepios Study. Br. J. Nutr. 2015, 113, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Vink, R.G.; Roumans, N.J.T.; Arkenbosch, L.A.J.; Mariman, E.C.M.; Van Baak, M.A. The effect of rate of weight loss on long-term weight regain in adults with overweight and obesity. Obesity 2016, 24, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Netherlands Nutrition Center. Richtlijnen Voedselkeuze. Available online: http://www.voedingscentrum.nl/professionals/schijf-van-vijf/Richtlijnen.aspx (accessed on 19 August 2015).
- Willett, W.; Stampfer, M.J. Total energy intake: Implications for epidemiologic analyses. Am. J. Epidemiol. 1986, 124, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Tabung, F.K.; Smith-Warner, S.A.; Chavarro, J.E.; Fung, T.T.; Hu, F.B.; Willett, W.C.; Giovannucci, E.L. An Empirical Dietary Inflammatory Pattern Score Enhances Prediction of Circulating Inflammatory Biomarkers in Adults. J. Nutr. 2017, 147, 1567–1577. [Google Scholar] [CrossRef] [PubMed]
- Baecke, J.A.H.; Burema, J.; Frijters, J.E.R. A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am. J. Clin. Nutr. 1982, 36, 936–942. [Google Scholar] [CrossRef] [PubMed]
- Vicente, A.R.; Manganaris, G.A.; Sozzi, G.O.; Crisosto, C.H. Nutritional Quality of Fruits and Vegetables. In Postharvest Handling; Academic Press: Cambridge, MA, USA, 2009; pp. 57–106. ISBN 9780123741127. [Google Scholar]
- Gebauer, S.K.; Psota, T.L.; Harris, W.S.; Kris-Etherton, P.M. n-3 Fatty acid dietary recommendations and food sources to achieve essentiality and cardiovascular benefits. Am. J. Clin. Nutr. 2006, 83 (Suppl. S6), 1526S–1535S. [Google Scholar] [PubMed]
- Kong, L.C.; Wuillemin, P.-H.; Bastard, J.-P.; Sokolovska, N.; Gougis, S.; Fellahi, S.; Darakhshan, F.; Bonnefont-Rousselot, D.; Bittar, R.; Doré, J.; et al. Insulin resistance and inflammation predict kinetic body weight changes in response to dietary weight loss and maintenance in overweight and obese subjects by using a Bayesian network approach. Am. J. Clin. Nutr. 2013, 98, 1385–1394. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Canela, M.; Zazpe, I.; Shivappa, N.; Hébert, J.R.; Sánchez-Tainta, A.; Corella, D.; Salas-Salvadó, J.; Fitó, M.; Lamuela-Raventós, R.M.; Rekondo, J.; et al. Dietary inflammatory index and anthropometric measures of obesity in a population sample at high cardiovascular risk from the PREDIMED (PREvención con DIeta MEDiterránea) trial. Br. J. Nutr. 2015, 113, 984–995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramallal, R.; Toledo, E.; Martínez, J.A.; Shivappa, N.; Hébert, J.R.; Martínez-González, M.A.; Ruiz-Canela, M. Inflammatory Potential of Diet, Weight Gain, and Incidence of Overweight/Obesity: The SUN Cohort. Obesity 2017, 25, 997–1005. [Google Scholar] [CrossRef] [PubMed]
- Gleeson, M.; Bishop, N.C.; Stensel, D.J.; Lindley, M.R.; Mastana, S.S.; Nimmo, M.A. The anti-inflammatory effects of exercise: Mechanisms and implications for the prevention and treatment of disease. Nat. Rev. Immunol. 2011, 11, 607–615. [Google Scholar] [CrossRef] [PubMed]
- Morais, J.B.S.; Severo, J.S.; Santos, L.R.D.; de Sousa Melo, S.R.; de Oliveira Santos, R.; de Oliveira, A.R.S.; Cruz, K.J.C.; do Nascimento Marreiro, D. Role of Magnesium in Oxidative Stress in Individuals with Obesity. Biol. Trace Elem. Res. 2017, 176, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Solini, A.; Santini, E.; Ferrannini, E. Effect of short-term folic acid supplementation on insulin sensitivity and inflammatory markers in overweight subjects. Int. J. Obes. 2006, 30, 1197–1202. [Google Scholar] [CrossRef] [PubMed]
- Gunanti, I.R.; Marooks, G.C.; Al-Mamun, A.; Long, K.Z. Low serum vitamin B-12 and folate concentrations and low thiamin and riboflavin intakes are inversely associated with greater adiposity in Mexican American children. J. Nutr. 2014, 144, 2027–2033. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.-S.; Li, D.; Zhou, Y.-M.; Sun, W.-P.; Liu, Q.-G. B-vitamin consumption and the prevalence of diabetes and obesity among the US adults: Population based ecological study. BMC Public Health 2010, 10, 746. [Google Scholar] [CrossRef] [PubMed]
- Mazur-Bialy, A.I.; Pocheć, E. Riboflavin reduces pro-inflammatory activation of adipocyte-macrophage co-culture. Potential application of vitamin B2 enrichment for attenuation of insulin resistance and metabolic syndrome development. Molecules 2016, 21. [Google Scholar] [CrossRef] [PubMed]
- Mazur-Bialy, A.I.; Pocheć, E. Vitamin B2 deficiency enhances the pro-inflammatory activity of adipocyte, consequences for insulin resistance and metabolic syndrome development. Life Sci. 2017, 178, 9–16. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Baseline (M1) | Weight Loss Period (M2) | Weight Stable Period (M3) | Follow Up Period (M4) | |
|---|---|---|---|---|
| Age (years) | 51.3 ± 9.1 | |||
| Height (cm) | 172.3 ± 8.9 | |||
| Weight (kg) | 92.5 ± 9.9 | 83.9 ± 1.2 *** | 83.7 ± 9.5 | 88.3 ± 10.2 *** |
| BMI (kg/m2) | 31.2 ± 2.3 | 28.3 ± 0.3 *** | 28.2 ± 2.4 | 29.6 ± 2.7 *** |
| Fat mass (%) | 39.8 ± 8.6 | 34.8 ± 1.4 *** | 33.8 ± 10.3 *** | 36.3 ± 9.8 *** |
| Fat free mass (%) | 60.2 ± 8.6 | 65.3 ± 1.4 *** | 66.2 ± 10.3 *** | 63.7 ± 9.8 *** |
| Fat mass (kg) | 36.4 ± 7.8 | 28.9 ± 1.2 *** | 27.9 ± 8.8 *** | 31.7 ± 9.0 *** |
| Fat free mass (kg) | 55.7 ± 11.5 | 54.6 ± 1.5 *** | 55.2 ± 11.6 *** | 56.0 ± 11.6 * |
| Waist circumference (cm) | 102.3 ± 9.6 | 94.7 ± 1.2 *** | 94.63 ± 9.0 | 98.1 ± 9.2 *** |
| Hip circumference (cm) | 111.0 ± 6.2 | 105.5 ± 0.9 *** | 104.7 ± 6.3 * | 106.2 ± 8.3 ** |
| Baseline Diet (D1) | Weight Maintenance (D2 and D3) | ||||||
|---|---|---|---|---|---|---|---|
| LCD | VLCD | All | LCD | VLCD | All | p * | |
| Energy (kcal/day) | 1991 ± 116 | 2120 ± 99 | 2071 ± 82 | 1677 ± 96 | 1713 ± 88 | 1684 ± 65 | <0.001 |
| Protein (%) a | 17.5 ± 0.6 | 17.7 ± 0.9 | 17.6 ± 0.6 | 19.7 ± 0.8 | 20.1 ± 0.8 | 20.1 ± 0.6 | <0.001 c |
| Carbohydrate (%) a | 43.3 ± 1.3 | 45.0 ± 1.5 | 43.9 ± 7.3 | 48.0 ± 1.3 | 45.8 ± 1.1 | 46.8 ± 6.2 | 0.012 |
| Sugars (%) a | 19.8 ± 1.3 | 20.3 ± 1.2 | 20.2 ± 6.5 | 21.6 ± 1.2 | 19.6 ± 1.1 | 20.4 ± 6.3 | 0.801 |
| Fat (%) a | 37.0 ± 1.3 | 35.1 ± 1.3 | 36.3 ± 6.8 | 30.2 ± 1.0 | 32.3 ± 1.1 | 31.7 ± 5.4 | <0.001 |
| Saturated fat (g/1000 kcal) b | 15.2 ± 0.8 | 14.6 ± 0.8 | 15.1 ± 0.6 | 11.7 ± 0.5 | 12.7 ± 0.4 | 12.2 ± 0.4 | <0.001 |
| Trans fat (g/1000 kcal) b | 1.17 ± 0.09 | 1.00 ± 0.08 | 1.08 ± 0.06 | 0.85 ± 0.13 | 0.95 ± 0.07 | 0.91 ± 0.08 | 0.041 c |
| MUFA (mg/1000 kcal) b | 13.8 ± 0.6 | 12.9 ± 0.5 | 13.5 ± 0.4 | 12.4 ± 0.7 | 12.4 ± 0.4 | 12.4 ± 0.4 | 0.104 c |
| PUFA (mg/1000 kcal) b | 7.75 ±0.51 | 7.67 ± 0.44 | 7.73 ± 0.34 | 6.85 ± 0.35 | 7.20 ± 0.36 | 7.05 ± 0.25 | 0.034 c |
| Omega 3 fatty acids (mg/1000 kcal) b | 0.89 ± 0.09 | 0.75 ± 0.08 | 0.83 ± 0.06 | 0.90 ± 0.09 | 0.84 ± 0.06 | 0.87 ± 0.06 | 0.584 c |
| Omega 6 fatty acids (mg/1000 kcal) b | 6.04 ±0.52 | 6.26 ± 0.43 | 6.15 ± 0.35 | 5.27 ± 0.28 | 5.65 ± 0.33 | 5.48 ± 0.21 | 0.038 |
| Cholesterol (mg/1000 kcal) b | 118.1 ±7.2 | 110.7 ± 8.1 | 117.2 ± 5.6 | 108.1 ± 8.4 | 106.3 ± 8.9 | 107.5 ± 6.1 | 0.202 |
| Fiber (g/1000 kcal) b | 9.77 ± 0.70 | 11.03 ± 0.64 | 10.48 ± 0.50 | 13.28 ± 0.55 | 13.88 ± 0.62 | 13.56 ± 0.42 | <0.001 |
| Alcohol (g/1000 kcal) b | 3.17 ± 1.02 | 2.82 ± 1.04 | 3.12 ± 0.77 | 2.25 ± 0.59 | 2.30 ± 0.72 | 2.19 ± 0.46 | 0.185 c |
| Magnesium (mg/1000 kcal) b | 145.8 ± 7.84 | 157.3 ± 6.1 | 152.2 ± 5.3 | 189.2 ± 6.7 | 182.3 ± 5.8 | 185.6 ± 4.6 | <0.001 |
| Iron (mg/1000 kcal) b | 6.14 ± 0.39 | 5.89 ± 0.31 | 6.04 ± 0.26 | 7.16 ± 0.33 | 6.94 ± 0.21 | 7.07 ± 0.20 | 0.001 c |
| Selenium (mg/1000 kcal) b | 27.8 ± 2.4 | 25.6 ± 2.0 | 26.8 ± 1.7 | 33.3 ± 2.4 | 28.6 ± 2.1 | 31.1 ± 1.6 | 0.037 c |
| Zinc (mg/1000 kcal) b | 5.00 ± 0.22 | 5.33 ± 0.34 | 5.19 ± 0.21 | 5.88 ± 0.23 | 5.78 ± 0.31 | 5.86 ± 0.2 | 0.022 c |
| Vitamin A (μg/1000 kcal) b | 362.9 ± 34.4 | 360.6 ± 41.5 | 373.2 ± 27.7 | 375.2 ± 28.2 | 534.6 ± 77.7 | 449.5 ± 40.9 | 0.046 c |
| Vitamin D (mg/1000 kcal) b | 2.31 ± 0.42 | 1.77 ± 0.18 | 2.07 ± 0.25 | 1.99 ± 0.18 | 2.11 ± 0.25 | 2.05 ± 0.15 | 0.362 c |
| Vitamin E (mg/1000 kcal) b | 6.58 ± 0.52 | 6.89 ± 0.49 | 6.79 ± 0.37 | 6.83 ± 0.39 | 6.48 ± 0.48 | 6.65 ± 0.31 | 0.667 |
| Thiamin (mg/1000 kcal) b | 0.64 ± 0.04 | 0.73 ± 0.06 | 0.69 ± 0.04 | 0.84 ± 0.05 | 0.72 ± 0.05 | 0.79 ± 0.04 | 0.037 c |
| Riboflavin (mg/1000 kcal) b | 0.79 ± 0.07 | 0.78 ± 0.06 | 0.79 ± 0.04 | 0.99 ± 0.06 | 0.92 ± 0.07 | 0.97 ± 0.05 | 0.003 c |
| Vitamin B6 (mg/1000 kcal) b | 0.89 ± 0.05 | 1.07 ± 0.08 | 0.99 ± 0.05 | 1.30 ± 0.08 | 1.25 ± 0.08 | 1.27 ± 0.06 | <0.001 c |
| Folate (μg/1000 kcal) b | 87.1 ± 10.3 | 95.8 ± 6.3 | 93.0 ± 6.4 | 128.1 ± 9.6 | 110.1 ± 6.9 | 119.7 ± 6.3 | <0.001 c |
| Vitamin B12 (mg/1000 kcal) b | 3.46 ± 0.96 | 2.26 ± 0.29 | 2.96 ± 0.55 | 3.27 ± 0.62 | 2.87 ± 0.44 | 3.04 ± 0.39 | 0.257 c |
| Niacin (mg/1000 kcal) b | 9.28 ± 0.53 | 9.13 ± 0.61 | 9.15 ± 0.42 | 11.67 ± 0.68 | 10.81 ± 0.58 | 11.24 ± 0.46 | 0.001 c |
| Vitamin C (mg/1000 kcal) b | 46.2 ± 7.6 | 54.0 ± 5.4 | 52.0 ± 4.9 | 67.4 ± 6.6 | 57.2 ± 5.5 | 61.2 ±4.2 | 0.025 c |
| Dietary Inflammatory Index ^ | 6.11 ± 0.43 | 5.73 ± 0.39 | 5.84 ± 0.31 | 4.44 ± 0.35 | 4.49 ± 0.35 | 4.48 ± 0.25 | <0.001 c |
| Physical Activity # | 9.07 ± 0.18 | 9.07 ± 0.21 | 8.95 ± 0.14 | 9.06 ± 0.20 | 8.78 ± 0.18 | 9.03 ± 0.14 | 0.437 |
| Uncorrected Bivariate Correlation | Partial Correlation (Corrected for Physical Activity) | |||
|---|---|---|---|---|
| r | p | r | p | |
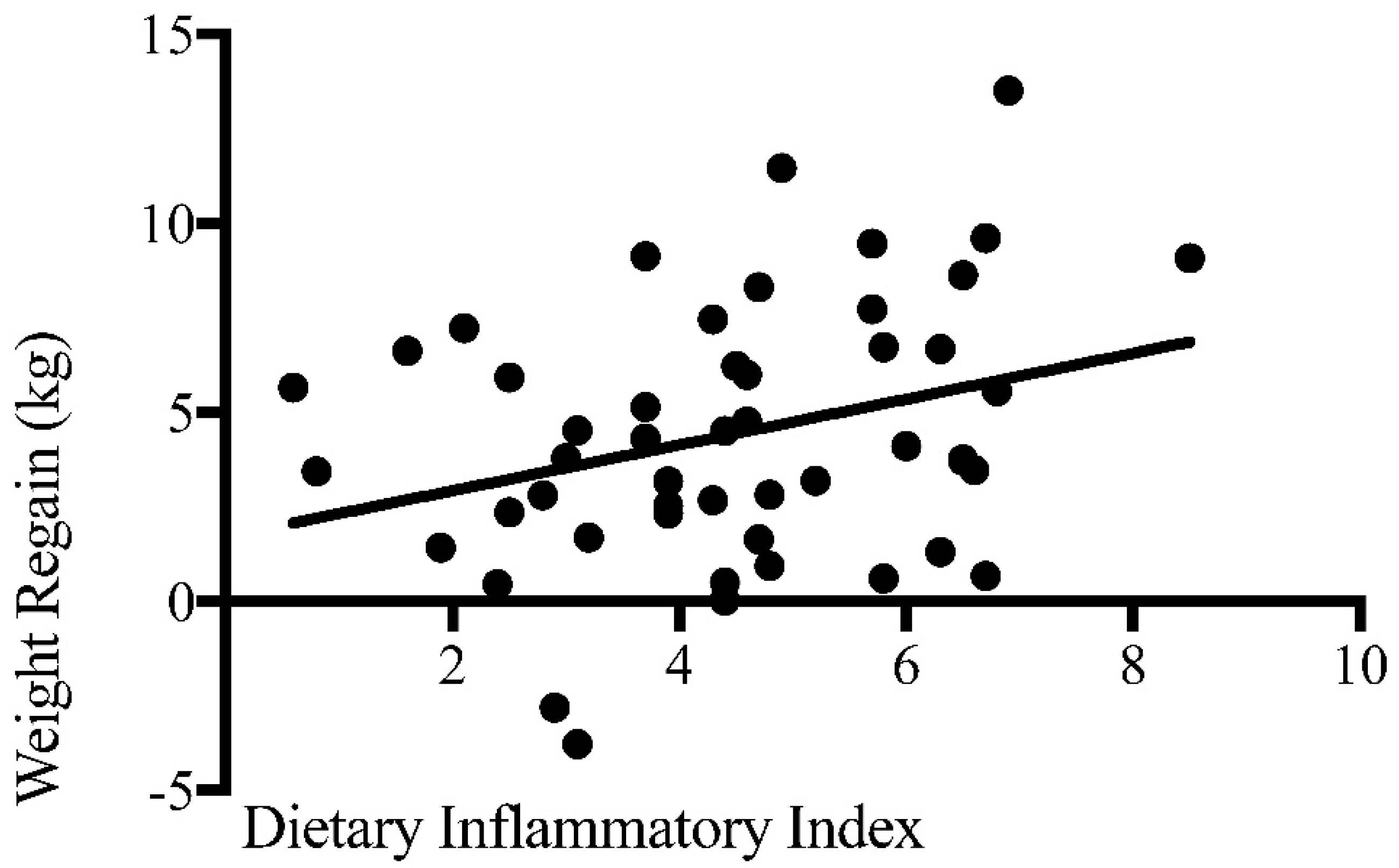
| Dietary Inflammatory Index ^ | 0.304 b | 0.032 * | 0.287 | 0.045 * |
| Energy #,^^ | 0.363 a | 0.018 * | 0.344 | 0.027 * |
| Protein ^^ | −0.204 b | 0.196 | −0.212 | 0.183 |
| Carbohydrate ^^ | 0.157 a | 0.322 | 0.169 | 0.292 |
| Sugars | 0.043 | 0.786 | 0.058 | 0.721 |
| Fat ^^ | −0.054 a | 0.735 | −0.106 | 0.510 |
| Saturated fat ^^ | −0.035 a | 0.824 | −0.068 | 0.674 |
| Trans fat ^^ | −0.060 b | 0.704 | −0.090 | 0.577 |
| MUFA ^^ | −0.018 a | 0.909 | −0.059 | 0.714 |
| PUFA ^^ | −0.043 a | 0.789 | −0.070 | 0.663 |
| Omega 3 fatty acids ^^ | −0.095 a | 0.551 | −0.123 | 0.443 |
| Omega 6 fatty acids ^^ | −0.027 a | 0.868 | −0.065 | 0.684 |
| Cholesterol ^^ | −0.052 a | 0.743 | −0.060 | 0.711 |
| Fiber ^^ | −0.240 a | 0.094 | −0.170 | 0.242 |
| Alcohol ^^ | 0.103 b | 0.517 | 0.124 | 0.442 |
| Magnesium ^^ | −0.328 a | 0.034 * | −0.279 | 0.077 |
| Iron ^^ | −0.017 b | 0.916 | −0.092 | 0.566 |
| Selenium ^^ | −0.280 a | 0.072 | −0.277 | 0.080 |
| Zinc ^^ | −0.289 a | 0.064 | −0.253 | 0.111 |
| Vitamin A ^^ | 0.002 b | 0.990 | −0.072 | 0.655 |
| Vitamin D ^^ | −0.026 b | 0.873 | 0.025 | 0.878 |
| Vitamin E ^^ | −0.170 b | 0.283 | −0.273 | 0.084 |
| Thiamin ^^ | −0.199 b | 0.207 | −0.138 | 0.388 |
| Riboflavin ^^ | −0.387 a | 0.011 * | −0.378 | 0.015 * |
| Vitamin B6 ^^ | −0.229 a | 0.144 | −0.206 | 0.197 |
| Folate ^^ | −0.313 b | 0.044 * | −0.290 | 0.066 |
| Vitamin B12 ^^ | −0.125 b | 0.429 | −0.069 | 0.667 |
| Niacin ^^ | −0.130 a | 0.413 | −0.118 | 0.463 |
| Vitamin C ^^ | −0.230 b | 0.142 | −0.232 | 0.144 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muhammad, H.F.L.; Vink, R.G.; Roumans, N.J.T.; Arkenbosch, L.A.J.; Mariman, E.C.; Van Baak, M.A. Dietary Intake after Weight Loss and the Risk of Weight Regain: Macronutrient Composition and Inflammatory Properties of the Diet. Nutrients 2017, 9, 1205. https://doi.org/10.3390/nu9111205
Muhammad HFL, Vink RG, Roumans NJT, Arkenbosch LAJ, Mariman EC, Van Baak MA. Dietary Intake after Weight Loss and the Risk of Weight Regain: Macronutrient Composition and Inflammatory Properties of the Diet. Nutrients. 2017; 9(11):1205. https://doi.org/10.3390/nu9111205
Chicago/Turabian StyleMuhammad, Harry Freitag Luglio, Roel G. Vink, Nadia J. T. Roumans, Laura A. J. Arkenbosch, Edwin C. Mariman, and Marleen A. Van Baak. 2017. "Dietary Intake after Weight Loss and the Risk of Weight Regain: Macronutrient Composition and Inflammatory Properties of the Diet" Nutrients 9, no. 11: 1205. https://doi.org/10.3390/nu9111205
APA StyleMuhammad, H. F. L., Vink, R. G., Roumans, N. J. T., Arkenbosch, L. A. J., Mariman, E. C., & Van Baak, M. A. (2017). Dietary Intake after Weight Loss and the Risk of Weight Regain: Macronutrient Composition and Inflammatory Properties of the Diet. Nutrients, 9(11), 1205. https://doi.org/10.3390/nu9111205