Vitamin D: Moving Forward to Address Emerging Science

Abstract
:1. Introduction
2. Promoting Consideration of the Totality of the Evidence
2.1. Systematic Reviews Underpin the Totality of Evidence
2.2. Incorporating the Totality of the Evidence
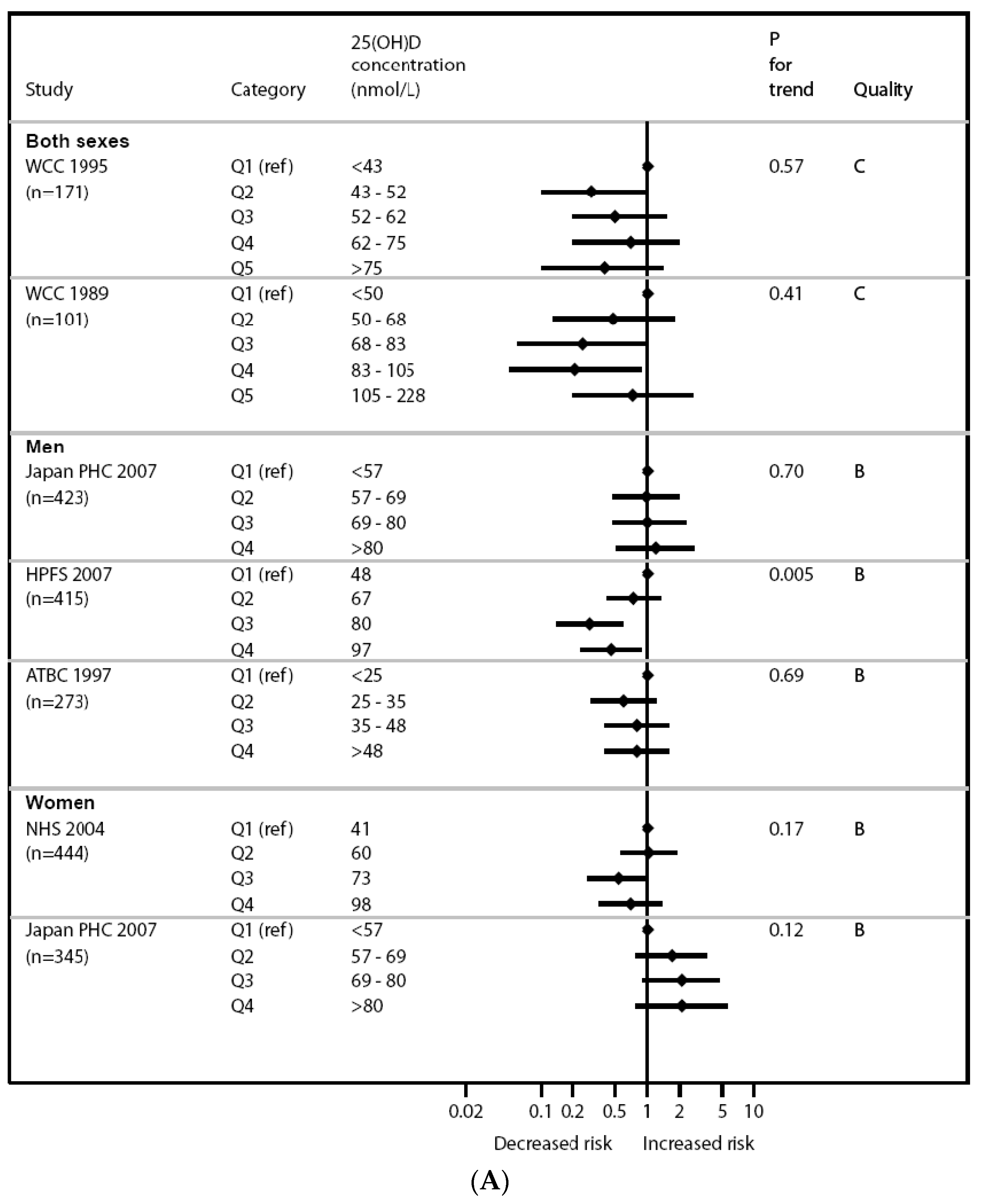
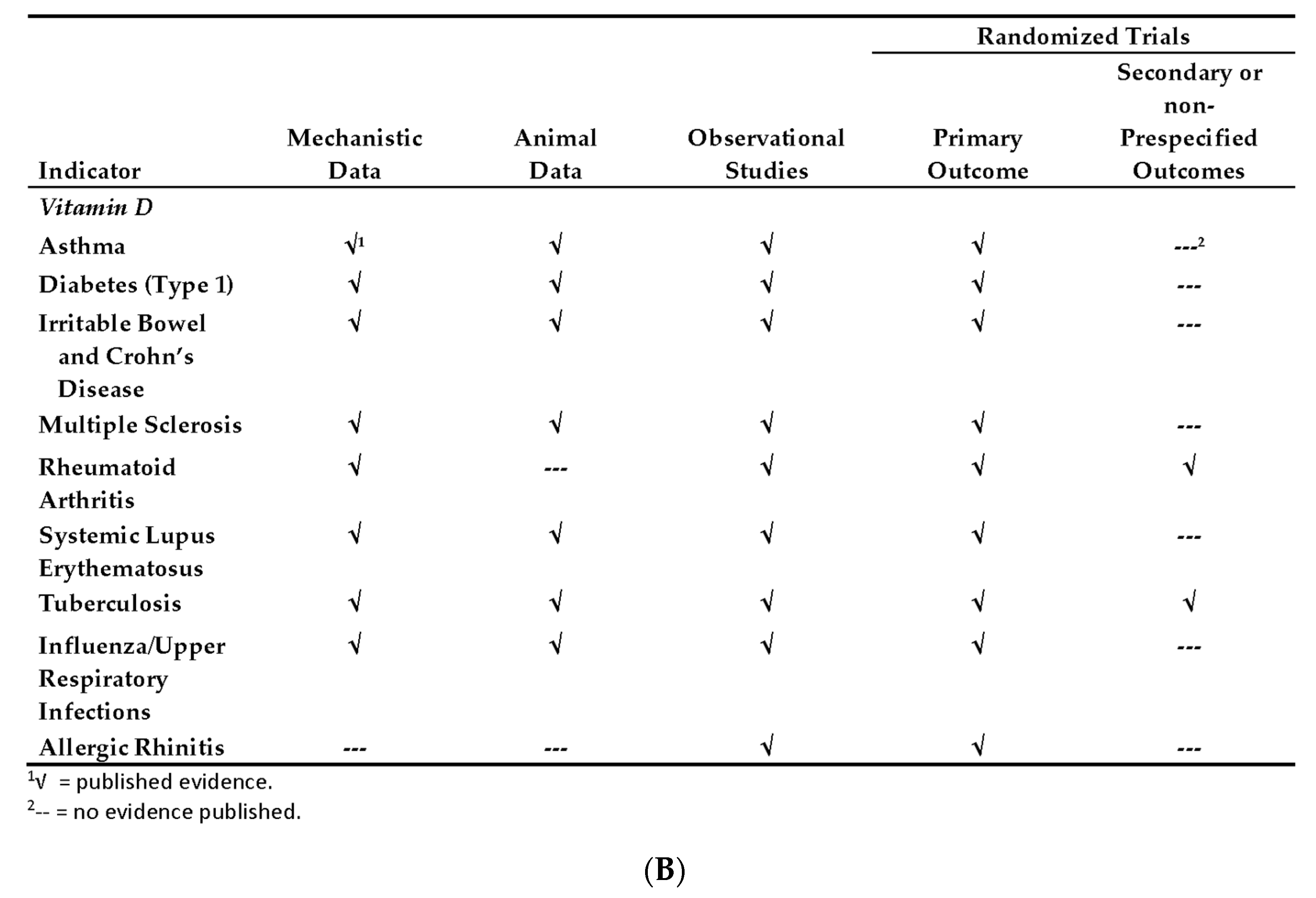
2.3. Cancer and Vitamin D: Illustration of Why Further Research Is Worthwhile
3. Promoting Research and Collaborative Activities
3.1. ODS Research Portfolio
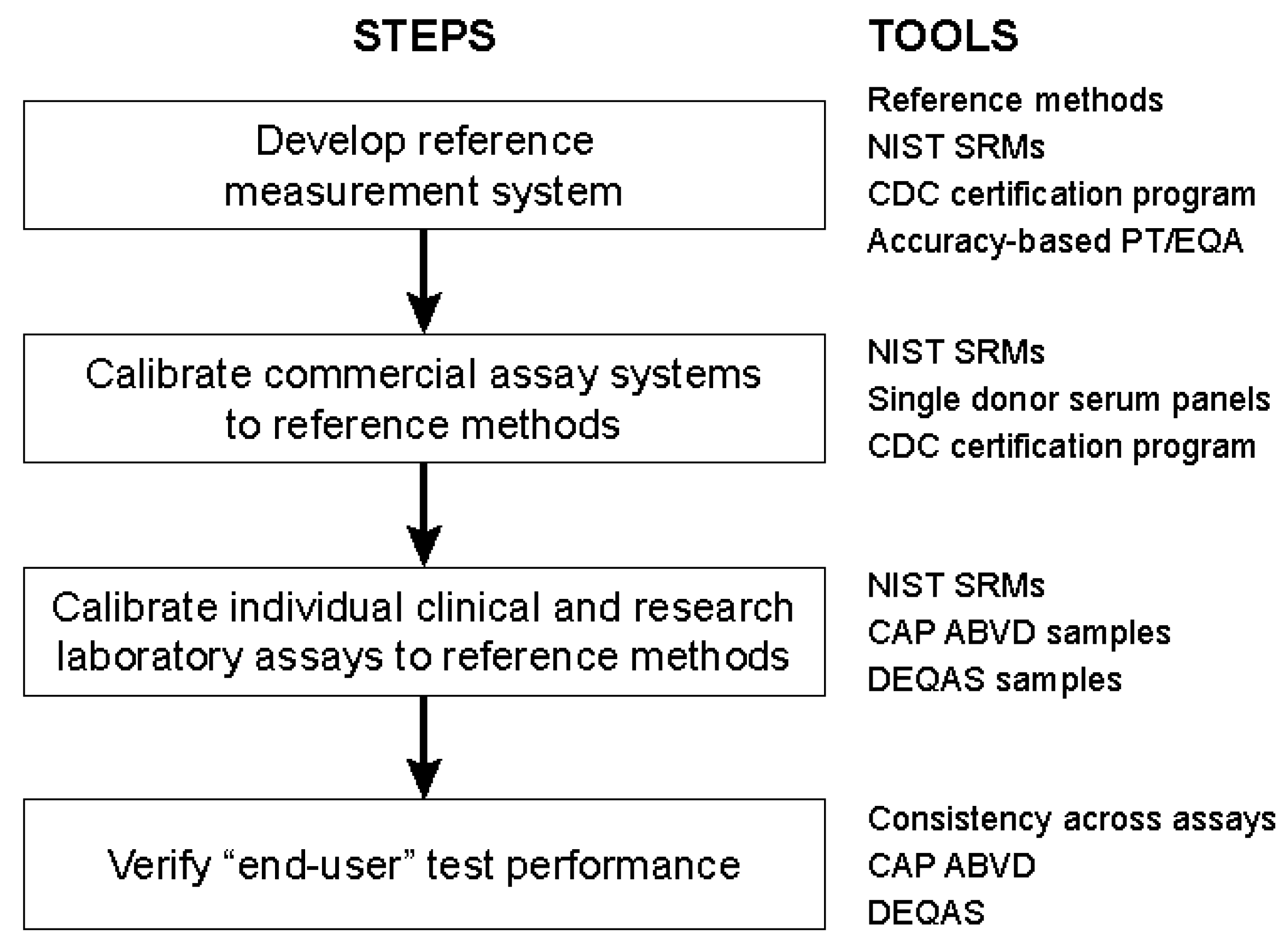
3.2. Vitamin D Assay Standardization
4. Implications
Acknowledgments
Author Contributions
Conflicts of Interest
References
- U.S. National Library of Medicine National Institutes of Health. PubMed Vitamin D Search Results. Available online: https://www.ncbi.nlm.nih.gov/pubmed/?term=vitamin+D (accessed on 8 September 2017).
- U.S. National Institutes of Health. ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ (accessed on 8 September 2017).
- Institute of Medicine (US). Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. In Dietary Reference Intakes for Calcium and Vitamin D; National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Brannon, P.M.; Taylor, C.L.; Coates, P.M. Use and applications of systematic reviews in public health nutrition. Annu. Rev. Nutr. 2014, 34, 401–419. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstein, A.H. Evaluating the evidence for DRI development: What are the issues in applying systematic evidence-based review approaches to DRI development? In The Development of DRIs, 1994–2004: Lessons Learned and New Challenges; National Academies Press: Washington, DC, USA, 2008. [Google Scholar]
- Agency for Healthcare Research and Quality (AHRQ). Nutritional Research Series. Available online: https://www.ahrq.gov/research/findings/evidence-based-reports/tr17-series.html (accessed on 15 July 2017).
- Cranney, A.; Horsley, T.; O’Donnell, S.; Weiler, H.; Puil, L.; Ooi, D.; Atkinson, S.; Ward, L.; Moher, D.; Hanley, D.; et al. Effectiveness and safety of vitamin D in relation to bone health. Evid. Rep. Technol. Assess. 2007, 158, 1–235. [Google Scholar]
- Chung, M.; Balk, E.M.; Brendel, M.; Ip, S.; Lau, J.; Lee, J.; Lichtenstein, A.; Patel, K.; Raman, G.; Tatsioni, A.; et al. Vitamin D and Calcium: Systematic Review of Health Outcomes; Evidence Report/Technology Assessment No. 183 (Prepared by Tufts Evidence-based Practice Center under Contract No. 290-2007-10055-I); Agency for Healthcare Research and Quality: Rockville, MD, USA, 2009.
- NIH Office of Dietary Supplements. Vitamin D: Moving Toward Evidence-Based Decision Making in Primary Care Conference, 2–3 December 2014. Available online: https://ods.od.nih.gov/Research/VitaminDConference2014.aspx (accessed on 8 September 2017).
- Newberry, S.J.; Chung, M.; Shekelle, P.G.; Booth, M.S.; Liu, J.L.; Maher, A.R.; Motala, A.; Cui, M.; Perry, T.; Shanman, R.; et al. Vitamin D and Calcium: A Systematic Review of Health Outcomes (Update); Evidence Report/Technology Assessment No. 217 (Prepared by the Southern California Evidence-based Practice Center under Contract No. 290-2012-00006-I); Agency for Healthcare Research and Quality: Rockville, MD, USA, 2014.
- Institute of Medicine. Dietary Reference Intakes: The Essential Guide to Nutrient Requirements; National Academies Press: Washington, DC, USA, 2006. [Google Scholar]
- Manson, J.E.; Brannon, P.M.; Rosen, C.J.; Taylor, C.L. Vitamin D deficiency—Is there really a pandemic? N. Engl. J. Med. 2016, 375, 1817–1820. [Google Scholar] [CrossRef] [PubMed]
- Rosen, C.J.; Taylor, C.L. Vitamin D supplementation and fall risk. Lancet Diabetes Endocrinol. 2014, 2, 532–534. [Google Scholar] [CrossRef]
- Bischoff-Ferrari, H.A.; Dawson-Hughes, B.; Orav, E.J.; Staehelin, H.B.; Meyer, O.W.; Theiler, R.; Dick, W.; Willett, W.C.; Egli, A. Monthly high-dose vitamin D treatment for the prevention of functional decline: A randomized clinical trial. JAMA Intern. Med. 2016, 176, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Scientific Advisory Committee on Nutrition (SACN). SACN Vitamin D and Health Report; Public Health England: London, UK, 2016.
- EFSA Panel on Dietetic Products Nutrition and Allergies (NDA). Dietary reference values for vitamin D. Eur. Food Saf. Auth. J. 2016, 14, 4547. [Google Scholar]
- Garland, C.F.; Garland, F.C. Do sunlight and vitamin D reduce the likelihood of colon cancer? Int. J. Epidemiol. 1980, 9, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Hanchette, C.L.; Schwartz, G.G. Geographic patterns of prostate cancer mortality. Evidence for a protective effect of ultraviolet radiation. Cancer 1992, 70, 2861–2869. [Google Scholar] [CrossRef]
- Bandera Merchan, B.; Morcillo, S.; Martin-Nunez, G.; Tinahones, F.J.; Macias-Gonzalez, M. The role of vitamin D and VDR in carcinogenesis: Through epidemiology and basic sciences. J. Steroid Biochem. Mol. Biol. 2017, 167, 203–218. [Google Scholar] [CrossRef] [PubMed]
- Ekmekcioglu, C.; Haluza, D.; Kundi, M. 25-Hydroxyvitamin D status and risk for colorectal cancer and type 2 diabetes mellitus: A systematic review and meta-analysis of epidemiological studies. Int. J. Environ. Res. Public Health 2017, 14, 127. [Google Scholar] [CrossRef] [PubMed]
- Dou, R.; Ng, K.; Giovannucci, E.L.; Manson, J.E.; Qian, Z.R.; Ogino, S. Vitamin D and colorectal cancer: Molecular, epidemiological and clinical evidence. Br. J. Nutr. 2016, 115, 1643–1660. [Google Scholar] [CrossRef] [PubMed]
- Bjelakovic, G.; Gluud, L.L.; Nikolova, D.; Whitfield, K.; Krstic, G.; Wetterslev, J.; Gluud, C. Vitamin D supplementation for prevention of cancer in adults. Cochrane Database Syst. Rev. 2014, 6, CD007469. [Google Scholar]
- Bassuk, S.S.; Manson, J.E.; Lee, I.M.; Cook, N.R.; Christen, W.G.; Bubes, V.Y.; Gordon, D.S.; Copeland, T.; Friedenberg, G.; D’Agostino, D.M.; et al. Baseline characteristics of participants in the VITamin D and OmegA-3 TriaL (VITAL). Contemp. Clin. Trials 2016, 47, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Neale, R.E.; Armstrong, B.K.; Baxter, C.; Duarte Romero, B.; Ebeling, P.; English, D.R.; Kimlin, M.G.; McLeod, D.S.; RL, O.C.; van der Pols, J.C.; et al. The D-Health Trial: A randomized trial of vitamin D for prevention of mortality and cancer. Contemp. Clin. Trials 2016, 48, 83–90. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials.gov. Finnish Vitamin D Trial (FIND). Available online: https://clinicaltrials.gov/ct2/show/NCT01463813 (accessed on 8 September 2017).
- ISRCTN Registry. Vitamin D and Longevity (VIDAL) Trial: Randomised Feasibility Study. Available online: http://www.isrctn.com/ISRCTN46328341 (accessed on 8 September 2017).
- NIH Office of Dietary Supplements. ODS Research Portfolio. Available online: https://ods.od.nih.gov/Funding/Grants__Contracts.aspx (accessed on 8 September 2017).
- NIH Office of Dietary Supplements. General NIH Funding Guidance. Available online: https://ods.od.nih.gov/Research/General_NIH_Funding_Guidance.aspx (accessed on 8 September 2017).
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Binkley, N.; Krueger, D.; Cowgill, C.S.; Plum, L.; Lake, E.; Hansen, K.E.; DeLuca, H.F.; Drezner, M.K. Assay variation confounds the diagnosis of hypovitaminosis D: A call for standardization. J. Clin. Endocrinol. Metab. 2004, 89, 3152–3157. [Google Scholar] [CrossRef] [PubMed]
- Le Goff, C.; Cavalier, E.; Souberbielle, J.C.; González-Antuña, A.; Delvin, E. Measurement of circulating 25-hydroxyvitamin D: A historical review. Pract. Lab. Med. 2015, 2, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Sempos, C.T.; Vesper, H.W.; Phinney, K.W.; Thienpont, L.M.; Coates, P.M. Vitamin D status as an international issue: National surveys and the problem of standardization. Scand. J. Clin. Lab. Investig. 2012, 72 (Suppl. S243), 32–40. [Google Scholar]
- Binkley, N.; Sempos, C.T. Standardizing vitamin D assays: The way forward. J. Bone Miner. Res. 2014, 29, 1709–1714. [Google Scholar] [CrossRef] [PubMed]
- Tai, S.S.; Bedner, M.; Phinney, K.W. Development of a candidate reference measurement procedure for the determination of 25-hydroxyvitamin D3 and 25-hydroxyvitamin D2 in human serum using isotope-dilution liquid chromatography-tandem mass spectrometry. Anal. Chem. 2010, 82, 1942–1948. [Google Scholar] [CrossRef] [PubMed]
- Stepman, H.C.; Vanderroost, A.; Van Uytfanghe, K.; Thienpont, L.M. Candidate reference measurement procedures for serum 25-hydroxyvitamin D3 and 25-hydroxyvitamin D2 by using isotope-dilution liquid chromatography-tandem mass spectrometry. Clin. Chem. 2011, 57, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Mineva, E.M.; Schleicher, R.L.; Chaudhary-Webb, M.; Maw, K.L.; Botelho, J.C.; Vesper, H.W.; Pfeiffer, C.M. A candidate reference measurement procedure for quantifying serum concentrations of 25-hydroxyvitamin D(3) and 25-hydroxyvitamin D(2) using isotope-dilution liquid chromatography-tandem mass spectrometry. Anal. Bioanal. Chem. 2015, 407, 5615–5624. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Standards and Technology (NIST). Standard Reference Materials. Available online: https://www.nist.gov/srm (accessed on 8 September 2017).
- Sempos, C.T.; Durazo-Arvizu, R.A.; Binkley, N.; Jones, J.; Merkel, J.M.; Carter, G.D. Developing vitamin D dietary guidelines and the lack of 25-hydroxyvitamin D assay standardization: The ever-present past. J. Steroid Biochem. Mol. Biol. 2016, 164, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Binkley, N.; Dawson-Hughes, B.; Durazo-Arvizu, R.; Thamm, M.; Tian, L.; Merkel, J.M.; Jones, J.C.; Carter, G.D.; Sempos, C.T. Vitamin D measurement standardization: The way out of the chaos. J. Steroid Biochem. Mol. Biol. 2016, 173, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Cashman, K.D.; Kiely, M.; Kinsella, M.; Durazo-Arvizu, R.A.; Tian, L.; Zhang, Y.; Lucey, A.; Flynn, A.; Gibney, M.J.; Vesper, H.W.; et al. Evaluation of Vitamin D Standardization Program protocols for standardizing serum 25-hydroxyvitamin D data: A case study of the program’s potential for national nutrition and health surveys. Am. J. Clin. Nutr. 2013, 97, 1235–1242. [Google Scholar] [CrossRef] [PubMed]
- Sarafin, K.; Durazo-Arvizu, R.; Tian, L.; Phinney, K.W.; Tai, S.; Camara, J.E.; Merkel, J.; Green, E.; Sempos, C.T.; Brooks, S.P. Standardizing 25-hydroxyvitamin D values from the Canadian Health Measures Survey. Am. J. Clin. Nutr. 2015, 102, 1044–1050. [Google Scholar] [CrossRef] [PubMed]
- Cashman, K.D.; Dowling, K.G.; Skrabakova, Z.; Kiely, M.; Lamberg-Allardt, C.; Durazo-Arvizu, R.A.; Sempos, C.T.; Koskinen, S.; Lundqvist, A.; Sundvall, J.; et al. Standardizing serum 25-hydroxyvitamin D data from four Nordic population samples using the Vitamin D Standardization Program protocols: Shedding new light on vitamin D status in Nordic individuals. Scand. J. Clin. Lab. Investig. 2015, 75, 549–561. [Google Scholar] [CrossRef] [PubMed]
- Schleicher, R.L.; Sternberg, M.R.; Lacher, D.A.; Sempos, C.T.; Looker, A.C.; Durazo-Arvizu, R.A.; Yetley, E.A.; Chaudhary-Webb, M.; Maw, K.L.; Pfeiffer, C.M.; et al. A method-bridging study for serum 25-hydroxyvitamin D to standardize historical radioimmunoassay data to liquid chromatography-tandem mass spectrometry. Natl. Health Stat. Rep. 2016, 93, 1–16. [Google Scholar]
- Jakab, E.; Kalina, E.; Petho, Z.; Pap, Z.; Balogh, A.; Grant, W.B.; Bhattoa, H.P. Standardizing 25-hydroxyvitamin D data from the HunMen cohort. Osteoporos. Int. 2017, 28, 1653–1657. [Google Scholar] [CrossRef] [PubMed]
- Sempos, C.T.; Durazo-Arvizu, R.A.; Carter, G.D. Cost effective measures to standardize serum 25(OH)D values from completed studies. Osteoporos. Int. 2017, 28, 1503–1505. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
|
|
|
|
| Outcome | Evidence |
|---|---|
| Dose-response for fractures | No data |
| Incidence total fractures: Vitamin D ± calcium vs. placebo | 14 RCTs: OR = 0.90 (0.80–1.20) |
| Incidence total fractures: Vitamin D + calcium vs. placebo | 8 non-RCTs: OR = 0.87 (0.76–1.00) |
| Incidence hip fractures: Vitamin D + calcium vs. placebo | 8 non-RCTs: OR = 0.87 (0.76–1.00) |
| IOM | SACN | EFSA | |
|---|---|---|---|
| Serum-linked reference value 4 | EAR: 16 ng/mL RDA: 20 ng/mL | EAR (cannot establish) RNI ≥10 ng/mL | AR (cannot establish) PRI (cannot establish) AI: 20 ng/mL |
| Intake reference value 4 | EAR: 400 IU (10 µg) RDA: 600 IU (15 µg) | RNI: 400 IU (10 µg) | AI: 600 IU (15 µg) |
| Selected Outcome | Skeletal health | Musculoskeletal health | Musculoskeletal health |
| Components of Selected Outcome | Integrated BMC/BMD, rickets, osteomalacia, calcium absorption, fractures | Rickets, osteomalacia, bone health indicators, fractures, falls, muscle health | Consideration of increased risk of adverse musculoskeletal outcomes |
| Other Health Outcomes Reviewed But Not Selected | Cancer, diabetes, CVD, falls, immune function, infectious disease, neuropsychological outcomes, pregnancy outcomes | Pregnancy/lactation outcomes, cancer, CVD, hypertension, all-cause mortality, immune modulation, neuropsychological outcomes, oral health, macular degeneration | Pregnancy outcomes, cancer, CVD, immune function, neuropsychological function |
| Rationale for Non-Selection | Contradictory, inconclusive, lack of causality | Weak, inconclusive | Inconclusive, weak or lacking causality |
| Research Topic Area | Research Needs |
|---|---|
| Health outcomes and related conditions |
|
| Adverse effects, toxicity, and safety |
|
| Basic physiology and molecular pathways |
|
| Synthesizing evidence and research methodology |
|
| Dose-response relationship |
|
| Sun exposure |
|
| Intake assessment |
|
| Trial | Location | Sample Size | Treatment Duration (Year) | Vitamin D Intervention | Primary Endpoints | Trial Registry No. |
|---|---|---|---|---|---|---|
| VITamin D and OmegA-3 TriaL (VITAL) [23] | The United States | 25,874 | 5 | 2000 IU/day | Cancer, Cardiovascular | NCT 01169259 |
| D-Health [24] | Australia | 21,315 | 5 | 60,000 IU/month | Total mortality, Cancer | ACTRN 1263000743763 |
| Finnish Vitamin D Trial (FIND) [25] | Finland | 18,000 1 | 5 | 1600 or 3200 IU/day | Cancer, Cardiovascular | NCT 01463813 |
| Vitamin D and Longevity [26] (VIDAL) | United Kingdom | 20,000 2 | 5 | 100,000 IU/month | Total mortality, Cancer | ISRCTN 46328341 |
| ● Vitamin D metabolites in human serum/plasma |
| ○ SRM 972a Vitamin D Metabolites in Frozen Human Serum |
| ○ SRM 1950 Metabolites in Human Plasma |
| ○ SRM 968e Fat Soluble Vitamins, Carotenoids, and Cholesterol in Human Serum |
| ○ SRM 2973 Vitamin D Metabolites in Frozen Human Serum |
| ● 25-hydroxyvitamin D calibrating solutions in ethanol |
| ○ SRM 2972a |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taylor, C.L.; Sempos, C.T.; Davis, C.D.; Brannon, P.M. Vitamin D: Moving Forward to Address Emerging Science. Nutrients 2017, 9, 1308. https://doi.org/10.3390/nu9121308
Taylor CL, Sempos CT, Davis CD, Brannon PM. Vitamin D: Moving Forward to Address Emerging Science. Nutrients. 2017; 9(12):1308. https://doi.org/10.3390/nu9121308
Chicago/Turabian StyleTaylor, Christine L., Christopher T. Sempos, Cindy D. Davis, and Patsy M. Brannon. 2017. "Vitamin D: Moving Forward to Address Emerging Science" Nutrients 9, no. 12: 1308. https://doi.org/10.3390/nu9121308
APA StyleTaylor, C. L., Sempos, C. T., Davis, C. D., & Brannon, P. M. (2017). Vitamin D: Moving Forward to Address Emerging Science. Nutrients, 9(12), 1308. https://doi.org/10.3390/nu9121308