Is Trabecular Bone Score Valuable in Bone Microstructure Assessment after Gastric Bypass in Women with Morbid Obesity?

Abstract
:1. Introduction
2. Material and Methods
2.1. Anthropometrical Measurements
2.2. Analytical Methods
2.3. Statistical Analysis
3. Results
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Goldner, W.S.; O’Dorisio, T.M.; Dillon, J.S.; Mason, E.E. Severe metabolic bone disease as a long-term complication of obesity surgery. Obes. Surg. 2002, 12, 685–692. [Google Scholar] [CrossRef] [PubMed]
- Coates, P.S.; Fernstrom, J.D.; Fernstrom, M.H.; Schauer, P.R.; Greenspan, S.L. Gastric bypass surgery for morbid obesity leads to an increase in bone turn-over and a decrease in bone mass. J. Clin. Endocrinol. Metab. 2004, 89, 1061–1065. [Google Scholar] [CrossRef] [PubMed]
- Vilarrasa, N.; Gomez, J.M.; Elio, I.; Gómez-Vaquero, C.; Masdevall, C.; Pujol, J.; Virgili, N.; Burgos, R.; Sánchez-Santos, R.; de Gordejuela, A.G.; et al. Evaluation of bone disease in morbidly obese women after gastric bypass and risk factors implicated in bone loss. Obes. Surg. 2009, 19, 860–866. [Google Scholar] [CrossRef] [PubMed]
- Carrasco, F.; Ruz, M.; Rojas, P.; Csendes, A.; Rebolledo, A.; Codoceo, J.; Inostroza, J.; Basfi-Fer, K.; Papapietro, K.; Rojas, J.; et al. Changes in bone mineral density, body composition and adiponectin levels inmorbidly obese patients after bariatric surgery. Obes. Surg. 2009, 19, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Stein, E.M.; Carrelli, A.; Young, P.; Bucovsky, M.; Chiyaun, Z.; Schrope, B.; Bessler, M.; Zhou, B.; Wang, J.; Guo, E.; et al. Bariatric surgery results in cortical bone loss. J. Clin. Endocrinol. Metab. 2013, 98, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Scibora, L.M.; Ikramuddin, S.; Buchwald, H.; Petit, M.A. Examining the link between bariatric surgery, bone loss, and osteoporosis: A review of bone density studies. Obes. Surg. 2012, 22, 654–667. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Carmona, Y.; Lopez-Alavez, F.J.; Gonzalez-Garay, A.G.; Solís-Galicia, C.; Meléndez, G.; Serralde-Zúñiga, A.E. Bone mineral density after bariatric surgery. A systematicreview. Int. J. Surg. 2014, 12, 976–982. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Wu, D.; Zhang, J.F.; Xu, D.; Xu, W.F.; Chen, Y.; Liu, B.Y.; Li, P.; Li, L. Changes in bone metabolism in morbidly obese patients after bariatric surgery: A meta-analysis. Obes. Surg. 2016, 26, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Goode, L.R.; Brolin, R.E.; Chowdhury, H.A.; Shapses, S.A. Bone and gastric bypass surgery: Effects of dietary calcium and vitamin D. Obes. Res. 2004, 12, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Valderas, J.P.; Velasco, S.; Solari, S.; Liberona, Y.; Viviani, P.; Maiz, A.; Escalona, A.; González, G. Increase of bone resorption and the parathyroid hormone in postmenopausal women in the long-term after roux-en-y gastric bypass. Obes. Surg. 2009, 19, 1132–1138. [Google Scholar] [CrossRef] [PubMed]
- Ko, B.J.; Myung, S.K.; Cho, K.H.; Park, Y.G.; Kim, S.G.; Kim, d.H.; Kim, S.M. Relationship between bariatric surgery and bone mineral density: A meta-analysis. Obes. Surg. 2016, 26, 1414–1421. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.M.; Haglind, E.G.; Clowes, J.A.; Achenbach, S.J.; Atkinson, E.J.; Melton, L.J., III; Kennel, K.A. Fracture risk following bariatric surgery: A population-based study. Osteoporos. Int. 2014, 25, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.W.; Chang, Y.K.; Chang, H.H.; Kuo, C.S.; Huang, C.T.; Hsu, C.C.; Huang, K.C. Fracture risk after bariatric surgery: A 12-year nationwide cohort study. Medicine (Baltimore) 2015, 94, e2087. [Google Scholar] [CrossRef] [PubMed]
- Rousseau, C.; Jean, S.; Gamache, P.; Lebel, S.; Mac-Way, F.; Biertho, L.; Michou, L.; Gagnon, C. Change in fracture risk and fracture pattern after bariatric surgery: Nested case-control study. BMJ 2016, 354, i3794. [Google Scholar] [CrossRef] [PubMed]
- Lalmohamed, A.; de Vries, F.; Bazelier, M.T.; Cooper, A.; van Staa, T.P.; Cooper, C.; Harvey, N.C. Risk of fracture after bariatric surgery in the United Kingdom: Population based, retrospective cohort study. BMJ 2012, 345, e5085. [Google Scholar] [CrossRef] [PubMed]
- Yu, E.W.; Lee, M.P.; Landon, J.E.; Lindeman, K.G.; Kim, S.C. Fracture risk after bariatric surgery: Roux-en-Y gastric bypass versus adjustable gastric banding. J. Bone Miner. Res. 2017, 32, 1229–1236. [Google Scholar] [CrossRef] [PubMed]
- Siris, E.S.; Chen, Y.T.; Abbott, T.A.; Barrett-Connor, E.; Miller, P.D.; Wehren, L.E.; Berger, M.L. Bone mineral density thresholds for pharmacological intervention to prevent fractures. Arch. Intern. Med. 2004, 164, 1108–1112. [Google Scholar] [CrossRef] [PubMed]
- Bousson, V.; Bergot, C.; Sutter, B.; Levitz, P.; Cortet, B.; Scientific Committee of the Groupe de Recherche et d’Informationsur les Ostéoporoses. Trabecular bone score (TBS): Available knowledge, clinical relevance, and future prospects. Osteoporos. Int. 2012, 23, 1489–1501. [Google Scholar] [CrossRef] [PubMed]
- Silva, B.C.; Leslie, W.D.; Resch, H.; Lamy, O.; Lesnyak, O.; Binkley, N.; McCloskey, E.V.; Kanis, J.A.; Bilezikian, J.P. Trabecular bone score: A non-invasive analytical method based upon the DXA image. J. Bone Miner. Res. 2014, 29, 518–530. [Google Scholar] [CrossRef] [PubMed]
- McCloskey, E.V.; Odén, A.; Harvey, N.C.; Leslie, W.D.; Hans, D.; Johansson, H.; Kanis, J.A. Adjusting fracture probability by trabecular bone score. Calcif. Tissue Int. 2015, 96, 500–509. [Google Scholar] [CrossRef] [PubMed]
- Capella, J.F.; Capella, R.F. Reducing early technical complications in gastric by-pass surgery. Obes. Surg. 1997, 7, 149–157. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (Report of a WHO Expert Committee). Physical status: The use and interpretation of anthropometry. World Health Organ. Tech. Rep. Ser. 1995, 854, 1–452. [Google Scholar]
- Alonso, G.C.; Curiel, M.D.; Carranza, F.H.; Cano, R.P.; Peréz, A.D. Femoral bone mineral density, neck-shaft angle and mean femoral neck width as predictors of hip fracture in men and women. Multicenter Project forResearch in Osteoporosis. Osteoporos. Int. 2000, 11, 714–720. [Google Scholar] [CrossRef] [PubMed]
- Kanis, J.A. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: Sinopsis of a WHO report. WHO Study Group. Osteoporos. Int. 1994, 4, 368–381. [Google Scholar] [CrossRef]
- Pothuaud, L.; Barthe, N.; Krieg, M.A.; Mehsen, N.; Carceller, P.; Hans, D. Evaluation of the potential use of trabecular bone score to complement bone mineral density in the diagnosis of osteoporosis: A preliminary spine BMD-matched, case control study. J. Clin. Densitom. 2009, 12, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Kanis, J.A.; McCloskey, E.; Johansson, H.; Oden, A.; Ström, O.; Borgström, F. Development and use of FRAX in osteoporosis. Osteoporos. Int. 2010, 21 (Suppl. 2), S407–S413. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]
- Vilarrasa, N.; San José, P.; García, I.; Gómez-Vaquero, C.; Miras, P.M.; de Gordejuela, A.G.; Masdevall, C.; Pujol, J.; Soler, J.; Gómez, J.M. Evaluation of bone mineral density loss in morbidly obese women after gastric bypass: 3-year follow-up. Obes. Surg. 2011, 21, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Raoof, M.; Näslund, I.; Rask, E.; Szabo, E. Effect of gastric bypass on bone mineral density, parathyroid hormone and vitamin D: 5 years follow-up. Obes. Surg. 2016, 26, 1141–1145. [Google Scholar] [CrossRef] [PubMed]
- Frederiksen, K.D.; Hanson, S.; Hansen, S.; Brixen, K.; Gram, J.; Jorgensen, N.R.; Stoving, R.K. Bone structural changes and estimated strength after gastric bypass surgery evaluated by HR-pQCT. Calcif. Tissue Int. 2016, 98, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Muschitz, C.; Kocijan, R.; Haschka, J.; Zendeli, A.; Pirker, T.; Geiger, C.; Müller, A.; Tschinder, B.; Kocijan, A.; Marterer, C.; et al. The Impact of Vitamin D, Calcium, Protein Supplementation, and Physical Exercise on Bone Metabolism After Bariatric Surgery: The BABS Study. J. Bone Miner. Res. 2016, 31, 672–682. [Google Scholar] [CrossRef] [PubMed]
- Gjesdal, C.G.; Halse, J.L.; Eide, G.E.; Brun, J.G.; Tell, G.S. Impact of lean mass and fat mass on bone mineral density: The Hordaland Health study. Maturitas 2008, 59, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Bazzocchi, A.; Ponti, F.; Diano, D.; Amadori, M.; Albisinni, U.; Battista, G.; Guglielmi, G. Trabecular bone score in healthy ageing. Br. J. Radiol. 2015, 88, 20140865. [Google Scholar] [CrossRef] [PubMed]
- Romagnoli, E.; Lubrano, C.; Carnevale, V.; Costantini, D.; Nieddu, L.; Morano, S.; Migliaccio, S.; Gnessi, L.; Lenzi, A. Assessment of trabecular bone score (TBS) in overweight/obese men: Effect of metabolic and anthropometric factors. Endocrine 2016, 54, 342–347. [Google Scholar] [CrossRef] [PubMed]
- McCloskey, E.V.; Odén, A.; Harvey, N.C.; Leslie, W.D.; Hans, D.; Johansson, H.; Barkmann, R.; Boutroy, S.; Brown, J.; Chapurlat, R.; et al. A meta-analysis of trabecular bone score in fracture risk prediction and its relationship to FRAX. J. Bone Miner. Res. 2016, 31, 940–948. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, M.G.; Cawthon, P.M.; Lui, L.Y.; Schousboe, J.T.; Ensrud, K.E.; Taylor, B.C.; Cauley, J.A.; Hillier, T.A.; Black, D.M.; Bauer, D.C.; et al. Estimates of the proportion of older White women who would be recommended for pharmacologic treatment by the new US National Osteoporosis Foundation Guidelines. J. Bone Miner. Res. 2009, 24, 675–680. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Basal | 12 Months after Surgery | 36 Months after Surgery |
|---|---|---|---|
| Age (years) | 46.39 ± 8.28 | ||
| Weight (kg) | 109.25 ± 10.79 | 72.62 ± 9.50 * | 77.30 ± 11.3 ** |
| BMI (kg/m2) | 42.91 ± 3.62 | 28.50 ± 3.72 * | 30.40 ± 4.46 ** |
| Waist to Hip Ratio | 0.87 ± 0.08 | 0.83 ± 0.06 * | 0.85 ± 0.06 ** |
| DXA FM (kg) | 46.92 ± 6.19 | 23.26 ± 5.95 * | 28.68 ± 7.66 ** |
| DXA LM (kg) | 54.97 ± 4.83 | 47.22 ± 4.53 * | 46.50 ± 5.42 |
| DXA BF (%) | 44.90 ± 3.14 | 31.61 ± 4.84 * | 36.72 ± 5.10 ** |
| Calcium (mmol/L) | 2.31 {0.13} | 2.40 {0.16} | 2.31 {0.20} ** |
| Phosphorus (mmol/L) | 1.10 ± 0.16 | 1.30 ± 0.14 * | 1.14 ± 0.23 ** |
| PTH (pmol/L) | 4.10 {2.45} | 5.6 {3.05} * | 6.9 {5.85} ** |
| 25(OH)D3 (nmol/L) | 57.4 {47.2} | 61.4 {41.5} * | 34.1 {21.0} ** |
| Variables | Basal | 12 Months after Surgery | 36 Months after Surgery |
|---|---|---|---|
| Femoral neck | |||
| BMD (g/cm2) | 1.10 ± 0.12 | 0.98 ± 0.12 * | 0.94 ± 0.11 ** |
| T-Score | 1.01 ± 1.06 | 0.06 ± 1.05 * | 0.06 ± 0.92 |
| Z-Score | 1.49 ± 0.78 | 0.58 ± 1.02 * | 0.56 ± 0.86 |
| Lumbar Spine | |||
| BMD (g/cm2) | 1.09 ± 1.33 | 1.06 ± 0.14 * | 1.04 ± 0.14 ** |
| T-Score | 0.65 ± 1.30 | 0.21 ± 1.28 * | −0.38 ± 1.30 ** |
| Z-Score | 1.05 ± 1.13 | 0.74 ± 1.10 * | 0.40 ± 1.23 ** |
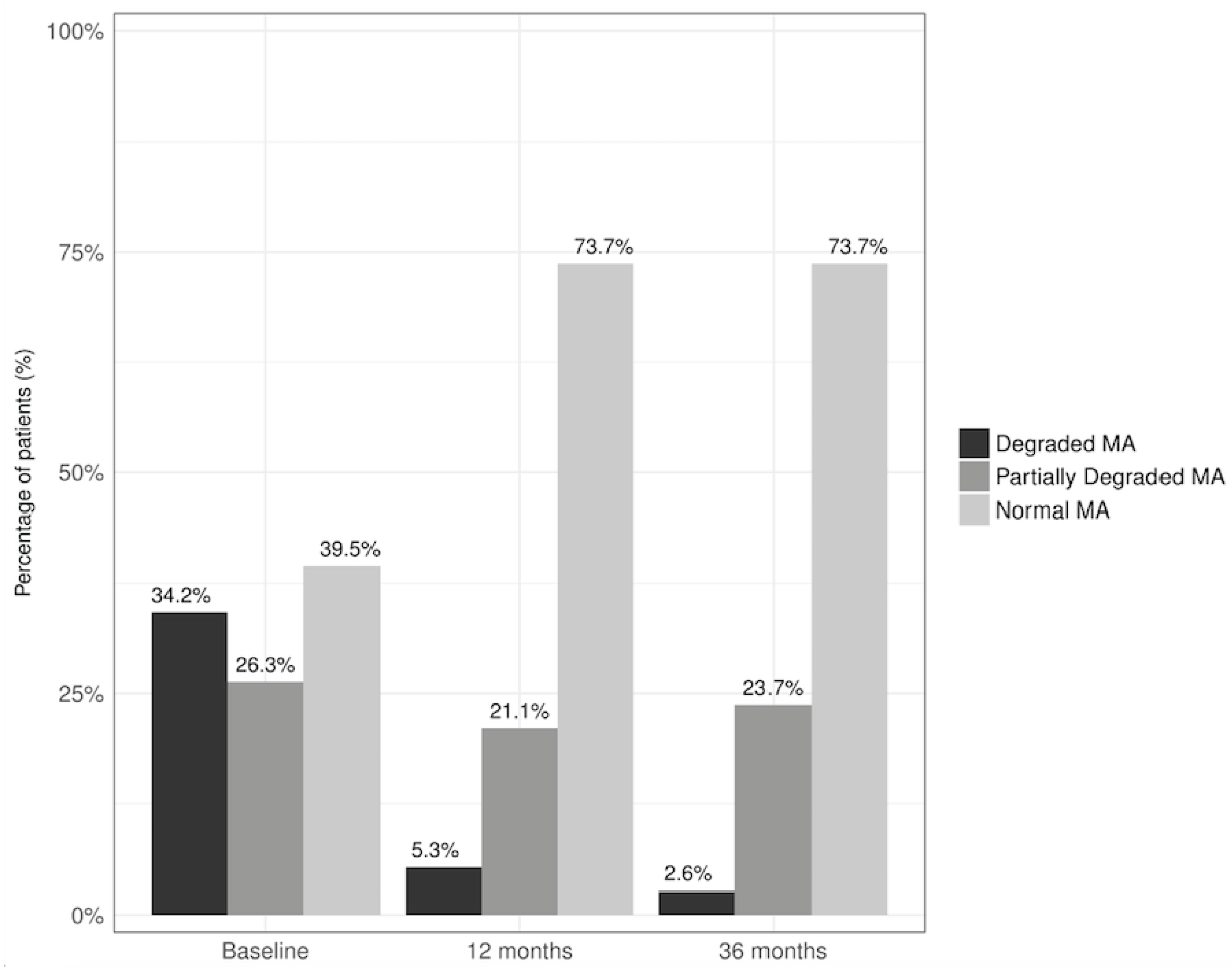
| AllTBSvalues | 1.271 ± 0.183 | 1.431 ± 0.104 * | 1.396 ± 0.109 |
| Strict TBS values | - | 1.431 ± 0.106 * | 1.414 ± 0.086 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marengo, A.P.; Guerrero Pérez, F.; San Martín, L.; Monseny, R.; Casajoana, A.; Valera, R.; Virgili, N.; Simó Servat, A.; Prats, A.; Gómez-Vaquero, C.; et al. Is Trabecular Bone Score Valuable in Bone Microstructure Assessment after Gastric Bypass in Women with Morbid Obesity? Nutrients 2017, 9, 1314. https://doi.org/10.3390/nu9121314
Marengo AP, Guerrero Pérez F, San Martín L, Monseny R, Casajoana A, Valera R, Virgili N, Simó Servat A, Prats A, Gómez-Vaquero C, et al. Is Trabecular Bone Score Valuable in Bone Microstructure Assessment after Gastric Bypass in Women with Morbid Obesity? Nutrients. 2017; 9(12):1314. https://doi.org/10.3390/nu9121314
Chicago/Turabian StyleMarengo, Agustina Pia, Fernando Guerrero Pérez, Luis San Martín, Rosa Monseny, Anna Casajoana, Rocio Valera, Nuria Virgili, Andreu Simó Servat, Albert Prats, Carmen Gómez-Vaquero, and et al. 2017. "Is Trabecular Bone Score Valuable in Bone Microstructure Assessment after Gastric Bypass in Women with Morbid Obesity?" Nutrients 9, no. 12: 1314. https://doi.org/10.3390/nu9121314
APA StyleMarengo, A. P., Guerrero Pérez, F., San Martín, L., Monseny, R., Casajoana, A., Valera, R., Virgili, N., Simó Servat, A., Prats, A., Gómez-Vaquero, C., & Vilarrasa, N. (2017). Is Trabecular Bone Score Valuable in Bone Microstructure Assessment after Gastric Bypass in Women with Morbid Obesity? Nutrients, 9(12), 1314. https://doi.org/10.3390/nu9121314