Comparison of Mid-Upper Arm Circumference and Weight-for-Height to Diagnose Severe Acute Malnutrition: A Study in Southern Ethiopia


Abstract
:1. Introduction
2. Methods
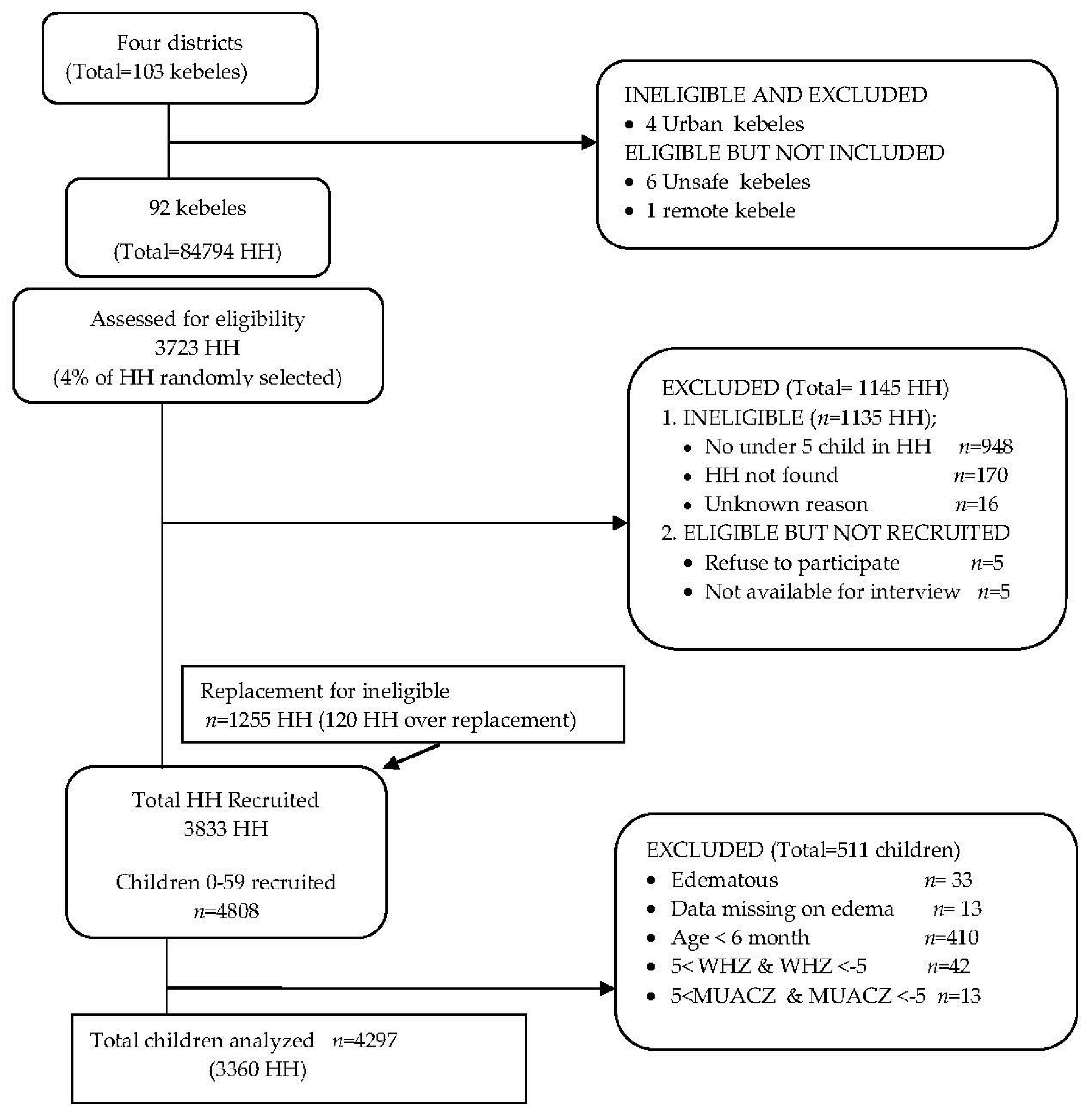
2.1. Study Setting and Design
2.2. Participants
2.3. Measures
2.3.1. Anthropometry
2.3.2. Demographics and Socio-Economic Status (SES)
2.3.3. Statistical Analyses
2.4. Ethics
3. Results
4. Key Messages
5. Discussion
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Bhutta, Z.A.; Das, J.K.; Rizvi, A.; Gaffey, M.F.; Walker, N.; Horton, S.; Webb, P.; Lartey, A.; Black, R.E. Evidence-based interventions for improvement of maternal and child nutrition: What can be done and at what cost? Lancet 2013, 382, 452–477. [Google Scholar] [CrossRef]
- World Health Organization. Management of Severe Malnutrition: A Manual for Physicians and Other Senior Health Workers; World Health Organization: Geneva, Switzerland, 1999. [Google Scholar]
- Collins, S.; Sadler, K.; Dent, N.; Khara, T.; Guerrero, S.; Myatt, M.; Saboya, M.; Walsh, A. Key issues in the success of communitybased management of severe malnutrition. Food Nutr. Bull. 2006, 27, 49–82. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization; World Food Programme; United Nations System Standing Committee on Nutrition; United Nations Children’s Fund. Community-Based Management of Severe Acute Malnutrition: A Joint Statement by the World Health Organization, the World Food Programme, the United Nations System Standing Committee on Nutrition and the United Nations Children’s Fund; World Health Organization: Geneva, Switzerland, 2007; Available online: http://www.who.int/nutrition/topics/Statement_community_based_man_sev_acute_mal_eng.pdf (accessed on 31 August 2015).
- Myatt, M.; Khara, T.; Collins, S. A review of methods to detect cases of severely malnourished children in the community for their admission into community-based therapeutic care programs. Food Nutr. Bull. 2006, 27, S7–S23. [Google Scholar] [CrossRef] [PubMed]
- Mwangome, M.K.; Fegan, G.; Mbunya, R.; Prentice, A.M.; Berkley, J.A. Reliability and accuracy of anthropometry performed by community health workers among infants under 6 months in rural Kenya. Trop. Med. Int. Health 2012, 17, 622–629. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization; United Nations Children’s Fund; Standing Committee on Nutrition. SCN Nutrition Policy Paper No. 21: WHO, UNICEF, and SCN Informal Consultation on Community-Based Management of Severe Malnutrition in Children. Available online: http://www.who.int/nutrition/publications/severemalnutrition/FNB_0379-5721.pdf (accessed on 5 August 2015).
- Briend, A.; Maire, B.; Fontaine, O.; Garenne, M. Mid-upper arm circumference and weight-for-height to identify high-risk malnourished under-five children. Matern. Child Nutr. 2012, 8, 130–133. [Google Scholar] [CrossRef] [PubMed]
- Briend, A.; Garenne, M.; Maire, B.; Fontaine, O.; Dieng, K. Nutritional status, age and survival: The muscle mass hypothesis. Eur. J. Clin. Nutr. 1989, 43, 715–726. [Google Scholar] [PubMed]
- Vella, V.; Tomkins, A.; Ndiku, J.; Marshal, T.; Cortinovis, I. Anthropometry as a predictor for mortality among Ugandan children, allowing for socio-economic variables. Eur. J. Clin. Nutr. 1994, 48, 189–197. [Google Scholar] [PubMed]
- World Health Organization. Guideline: Updates on the Management of Severe Acute Malnutrition in Infants and Children; World Health Organization: Geneva, Switzerland, 2013; Available online: http://apps.who.int/iris/bitstream/10665/95584/1/9789241506328_eng.pdf (accessed on 19 November 2015).
- World Health Organization; United Nations Children’s Fund. WHO Child Growth Standards and Identification of Severe Acute Malnutrition in Infants and Children: A Joint statement by the World Health Organization and the United Nations Children’s Fund; World Health Organization Press: Geneva, Switzerland, 2009; Available online: http://apps.who.int/iris/bitstream/10665/44129/1/9789241598163_eng.pdf (accessed on 20 September 2015).
- Laillou, A.; Prak, S.; de Groot, R.; Whitney, S.; Conkle, J.; Horton, L.; Un, S.O.; Dijkhuizen, M.A.; Wieringa, F.T. Optimal Screening of Children with Acute Malnutrition Requires a Change in Current WHO Guidelines as MUAC and WHZ Identify Different Patient Groups. PLoS ONE 2014, 9, e101159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berkley, J.; Mwangi, I.; Griffiths, K.; Ahmed, I.; Mithwani, S.; English, M.; Newton, C.; Maitland, K. Assessment of severe malnutrition among hospitalized children in rural Kenya: Comparison of weight for height and mid upper arm circumference. JAMA 2005, 294, 591–597. [Google Scholar] [CrossRef] [PubMed]
- Walters, T.; Sibson, V.; McGrath, M. Mid Upper Arm Circumference and Weight-for-Height Z-Score as Indicators of Severe Acute Malnutrition: A Consultation of Operational Agencies and Academic Specialist to Understand the Evidence, Identify Knowledge Gaps and to Inform Operational Guidance. Emergency Nutrition Network: Oxford, 2012. Available online: http://www.cmamforum.org/Pool/Resources/MUAC-WFH-Report-ENN-2013.pdf (accessed on 23 December 2016).
- Munthali, T.; Jacobs, C.; Sitali, L.; Dambe, R.; Michelo, C. Mortality and morbidity patterns in under-five children with severe acute malnutrition (SAM) in Zambia: A five-year retrospective review of hospital-based records (2009–2013). Arch. Public Health 2015, 73, 23. [Google Scholar] [CrossRef] [PubMed]
- McDonald, C.M.; Olofin, I.; Flaxman, S.; Fawzi, W.W.; Spiegelman, D.; Caulfield, L.E.; Black, R.E.; Ezzat, M.; Danaei, G. The effect of multiple anthropometric deficits on child mortality: Meta-analysis of individual data in 10 prospective studies from developing countries. Am. J. Clin. Nutr. 2013, 97, 896–901. [Google Scholar] [CrossRef] [PubMed]
- Pelletier, D.L.; Frongillo, E.A. Changes in child survival are strongly associated with changes in malnutrition in developing countries. J. Nutr. 2003, 133, 107–119. [Google Scholar] [PubMed]
- Pelletier, D.L.; Low, J.W.; Johnson, F.C.; Msukwa, L.A.H. Child Anthropometry and Mortality In Malawi: Testing for Effect Modification by Age and Length of Follow-up and Confounding by Socioeconomic Factors. J. Nutr. 1994, 124, 2082S–2105S. [Google Scholar] [PubMed]
- United States Agency for International Development. Ethiopia Southern Nations, Nationalities and Peoples Region (SNNPR) Livelihood Zone Reports: SNNPR Follow-On to Regional Livelihoods Baseline Study; USAID: Washington, DC, USA, 2005. Available online: http://pdf.usaid.gov/pdf_docs/Pnadj866.pdf (accessed on 21 August 2015).
- The Harmonised Training Package Resource Material for Training on Nutrition in Emergencies. Available online: http://www.ennonline.net/resources/htpversion2 (accessed on 23 December 2016).
- World Health Organization. WHO Expert Committee on Physical Status. The Use and Interpretation of Anthropometry; Report of a WHO Expert Committee; World Health Organization: Geneva, Switzerland, 1995; Available online: http://apps.who.int/iris/bitstream/10665/37003/1/WHO_TRS_854.pdf (accessed on 14 November 2015).
- World Health Organization. WHO Anthro for Personal Computers, Version 3.2.2. Software for Assessing Growth and Development of the World’s Children; World Health Organization: Geneva, Switzerland, 2011; Available online: http://www.who.int/childgrowth/software/anthro_pc_manual_v322.pdf?ua=1 (accessed on 20 September 2015).
- World Health Organization; United Nations Children’s Fund. Meeting the MDG Drinking Water and Sanitation Target: The Urban and Rural Challenge of the Decade; World Health Organization: Geneva, Switzerland; United Nations Children’s Fund: New York, NY, USA, 2006; Available online: http://www.who.int/water_sanitation_health/monitoring/jmpfinal.pdf (accessed on 22 November 2015).
- Watson, P.F.; Petrie, A. Method agreement analysis: A review of correct methodology. Theriogenology 2010, 73, 1167–1179. [Google Scholar] [CrossRef] [PubMed]
- Sim, J.; Wright, C.C. The kappa statistic in reliability studies: Use, interpretation, and sample size requirements. Phys. Ther. 2005, 85, 257–268. [Google Scholar] [PubMed]
- Viera, A.J.; Garrett, J.M. Understanding Interobserver Agreement: The Kappa Statistic. Fam. Med. 2005, 37, 360–363. [Google Scholar] [PubMed]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Hop, L.T.; Gross, R.; Sastroamidjojo, S.; Giay, T.; Schultink, W. Mid-upper-arm circumeference development and its validity in assessment of undernutrition. Asia Pac. J. Clin. Nutr. 1998, 7, 65–69. [Google Scholar]
- Manary, M.J.; Sandige, H.L. Management of acute moderate and severe childhood malnutrition. BMJ. 2008, 337, a2180. [Google Scholar] [CrossRef] [PubMed]
- Ross, D.A.; Taylor, N.; Hayes, R.; McLean, M. Measuring malnutrition in famines: Are weight-for-height and arm circumference interchangeable? Int. J. Epidemiol. 1990, 19, 636–645. [Google Scholar] [CrossRef] [PubMed]
- Gayle, H.D.; Binkin, N.J.; Staehling, N.W.; Trowbridge, F.L. Arm circumference vs weight for height in nutritional assessment: Are the findings comparable? J. Trop. Pediatr. 1998, 34, 213–217. [Google Scholar] [CrossRef]
- Myatt, M.; Duffield, A.; Seal, A.; Pasteur, F. The effect of body shape on weight-for-height and mid-upper arm circumference based case definitions of acute malnutrition in Ethiopian children. Ann. Hum. Biol. 2009, 36, 5–20. [Google Scholar] [CrossRef] [PubMed]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, J.; Andersen, A.; Fisker, A.B.; Ravn, H.; Sodemann, M.; Rodrigues, A.; Benn, C.S.; Aaby, P. Mid-upper-arm-circumference and mid-upper-arm circumference z-score: The best predictor of mortality? Eur. J. Clin. Nutr. 2012, 66, 998–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isanaka, S.; Villamor, E.; Shepherd, S.; Grais, R.F. Assessing the impact of the introduction of the World Health Organization growth standards and weight-for-height z-score criterion on the response to treatment of severe acute malnutrition in children: Secondary data analysis. Pediatrics 2009, 123, e54–e59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goossens, S.; Bekele, Y.; Yun, O.; Harczi, G.; Ouannes, M.; Shepherd, S. Mid-Upper Arm Circumference Based Nutrition Programming: Evidence for a New Approach in Regions with High Burden of Acute Malnutrition. PLoS ONE 2012, 7, e49320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kottner, J.; Audigé, L.; Brorson, S.; Donner, A.; Gajewski, B.J.; Hróbjartsson, A.; Roberts, C.; Shoukri, M.; Streiner, D.L. Guidelines for Reporting Reliability and Agreement Studies (GRRAS) were proposed. J. Clin. Epidemiol. 2011, 64, 96–106. [Google Scholar] [CrossRef] [PubMed]
- Velzeboer, M.I.; Selwyn, B.J.; Sargent, F.I.; Pollitt, E.; Delgado, H. Evaluation of arm circumference as a public health index of protein energy malnutrition in early childhood. J. Trop. Pediatr. 1983, 29, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Briend, A.; Zimicki, S. Validation of arm circumference as an indicator of risk of death in one to four year old children. Nutr. Res. 1986, 6, 249–261. [Google Scholar] [CrossRef]
- Katz, J.; West, K.P.; Tarwotjo, I.; Sommer, A. The importance of age in evaluating anthropometric indices for predicting mortality. Am. J. Epidemiol. 1989, 130, 1219–1226. [Google Scholar] [CrossRef] [PubMed]
- Lapidus, N.; Minetti, A.; Djibo, A.; Guerin, P.J.; Hustache, S.; Gaboulaud, V.; Grais, R.F. Mortality risk among children admitted in a large-scale nutritional program in Niger, 2006. PLoS ONE 2009, 4, e4313. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristics | n or Mean a | (%) or SD b |
|---|---|---|
| Household | ||
| Quality of housing | ||
| Iron sheet roof (n = 3359) | 1372 | (40.8) |
| Earth floor (n = 3358) | 3296 | (98.2) |
| Wood and mud wall (n = 3359) | 3131 | (93.2) |
| Improved drinking water (n = 3358) | 2711 | (80.7) |
| Improved sanitation facility (n = 3332) | 247 | (6.5) |
| Electricity (n = 3358) | 33 | (1.0) |
| Owned land size (hectares) (n = 3360) | 0.19 a | 0.17 b |
| Maternal/caregiver | ||
| Age (year) (n = 3319) | 31 a | 8.6 b |
| 15–24 | 367 | (10.9) |
| 25–34 | 1811 | (53.9) |
| 35–44 | 818 | (24.3) |
| ≥45 | 323 | (9.6) |
| Married (n = 3334) | 2954 | (87.9) |
| Education (n = 3352) | ||
| No formal school | 2121 | (63.1) |
| Primary (Grade 1–8) | 1164 | (34.6) |
| Secondary/above | 67 | (2.0) |
| Occupation (n = 3354) | ||
| Agriculture/farmer | 1997 | (59.5) |
| Petty trade/own skilled work | 965 | (28.7) |
| No occupation | 303 | (9.0) |
| Child (n = 4297) | ||
| Age (months) | 33 a | 15.9 b |
| 6–11 | 571 | (13.3) |
| 12–23 | 812 | (18.9) |
| 24–35 | 657 | (15.3) |
| 36–47 | 1215 | (28.3) |
| 48–59 | 1042 | (24.2) |
| Male sex | 2187 | (50.9) |
| Wasting | Moderate Wasting | Severe Wasting | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| WHZ < −2 SD ∞ | MUAC < 125 mm | WHZ ≥ −3 SD and <−2 SD ∞ | MUAC ≥ 115 mm and <125 mm | WHZ < −3 SD ∞ | MUAC < 115 mm | ||||||||
| Age (Months) | % | (95% CI) | % | (95% CI) | % | (95% CI) | % | (95% CI) | % | (95% CI) | % | (95% CI) | |
| 6–23 | Combined (n = 1383) | 9.8 | (8.3, 11.5) | 20.8 | (18.7, 23.1) | 7.8 | (6.5, 9.8) | 16.9 | (15.0, 19.0) | 2.0 | (1.4, 2.9) | 3.9 | (3.0, 5.1) |
| Boys (n = 740) | 11.6 | (9.4, 14.2) | 19.1 | (16.3, 22.1) | 8.9 | (7.0, 11.3) | 15.7 | (13.2, 18.6) | 2.7 | (1.7, 4.2) | 3.4 | (2.2, 5.0) | |
| Girls (n = 643) | 7.8 | (5.9, 10.2) | 22.9 | (19.7, 26.3) | 6.5 | (4.8, 8.8) | 18.4 | (15.5, 21.6) | 1.2 | (0.6, 2.5) | 4.5 | (3.1, 6.5) | |
| 24–59 | Combined (n = 2914) | 3.3 | (2.7, 4.0) | 5.6 | (4.8, 6.5) | 2.7 | (2.2, 3.4) | 5.1 | (4.3, 6.0) | 0.5 | (0.3, 0.9) | 0.5 | (0.3, 0.8) |
| Boys (n = 1447) | 3.8 | (2.9, 5.0) | 4.7 | (3.7, 6.0) | 3.1 | (2.3, 4.2) | 4.1 | (3.2, 5.3) | 0.7 | (0.4, 1.3) | 0.6 | (0.3, 1.1) | |
| Girls (n = 1467) | 2.8 | (2.0, 3.8) | 6.4 | (5.2, 7.8) | 2.4 | (1.7, 3.3) | 6.0 | (4.9, 7.4) | 0.4 | (0.2, 0.9) | 0.4 | (0.2, 0.9) | |
| 6–59 | Combined (n = 4297) | 5.4 | (4.8, 6.1) | 10.5 | (9.6, 11.4) | 4.4 | (3.8, 5.0) | 8.9 | (8.1, 9.8) | 1.0 | (0.8, 1.4) | 1.6 | (1.2, 2.0) |
| Boys (n = 2187) | 6.4 | (5.5, 7.6) | 9.6 | (8.4, 10.9) | 5.1 | (4.2, 6.1) | 8.0 | (7.0, 9.3) | 1.4 | (0.9, 2.0) | 1.5 | (1.1, 2.1) | |
| Girls (n = 2110) | 4.3 | (3.5, 5.3) | 11.4 | (10.1, 12.9) | 3.6 | (2.9, 4.6) | 9.8 | (8.5, 11.1) | 0.7 | (0.4, 1.1) | 1.7 | (1.2, 2.3) | |
| WHZ < −3 | −3 ≤ WHZ < −2 | −2 ≤ WHZ | Total | |
|---|---|---|---|---|
| All Children | ||||
| MUAC < 115 | 16 | 28 | 24 | 68 |
| 115 ≤ MUAC < 125 | 11 | 77 | 294 | 382 |
| 125 ≤ MUAC | 17 | 83 | 3747 | 3847 |
| Total | 44 | 188 | 4065 | 4297 |
| † κ = 0.28 | ||||
| Boys | ||||
| MUAC < 115 | 12 | 15 | 6 | 33 |
| 115 ≤ MUAC < 125 | 8 | 44 | 124 | 176 |
| 125 ≤ MUAC | 10 | 52 | 1916 | 1978 |
| Total | 30 | 111 | 2046 | 2187 |
| † κ = 0.37 | ||||
| Girls | ||||
| MUAC < 115 | 4 | 13 | 18 | 35 |
| 115 ≤ MUAC < 125 | 3 | 33 | 170 | 206 |
| 125 ≤ MUAC | 7 | 31 | 1831 | 1869 |
| Total | 14 | 77 | 2019 | 2110 |
| † κ = 0.15 | ||||
| <24 months | ||||
| MUAC < 115 | 14 | 21 | 19 | 54 |
| 115 ≤ MUAC < 125 | 6 | 50 | 178 | 234 |
| 125 ≤ MUAC | 8 | 37 | 1050 | 1095 |
| Total | 28 | 108 | 1228 | 1383 |
| † κ = 0.32 | ||||
| ≥24 months | ||||
| MUAC < 115 | 2 | 7 | 5 | 14 |
| 115 ≤ MUAC < 125 | 5 | 27 | 116 | 148 |
| 125 ≤ MUAC | 9 | 46 | 2697 | 2752 |
| Total | 16 | 80 | 2818 | 2914 |
| † κ = 0.13 | ||||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tadesse, A.W.; Tadesse, E.; Berhane, Y.; Ekström, E.-C. Comparison of Mid-Upper Arm Circumference and Weight-for-Height to Diagnose Severe Acute Malnutrition: A Study in Southern Ethiopia. Nutrients 2017, 9, 267. https://doi.org/10.3390/nu9030267
Tadesse AW, Tadesse E, Berhane Y, Ekström E-C. Comparison of Mid-Upper Arm Circumference and Weight-for-Height to Diagnose Severe Acute Malnutrition: A Study in Southern Ethiopia. Nutrients. 2017; 9(3):267. https://doi.org/10.3390/nu9030267
Chicago/Turabian StyleTadesse, Amare Worku, Elazar Tadesse, Yemane Berhane, and Eva-Charlotte Ekström. 2017. "Comparison of Mid-Upper Arm Circumference and Weight-for-Height to Diagnose Severe Acute Malnutrition: A Study in Southern Ethiopia" Nutrients 9, no. 3: 267. https://doi.org/10.3390/nu9030267
APA StyleTadesse, A. W., Tadesse, E., Berhane, Y., & Ekström, E. -C. (2017). Comparison of Mid-Upper Arm Circumference and Weight-for-Height to Diagnose Severe Acute Malnutrition: A Study in Southern Ethiopia. Nutrients, 9(3), 267. https://doi.org/10.3390/nu9030267