Reported Energy Intake Accuracy Compared to Doubly Labeled Water and Usability of the Mobile Food Record among Community Dwelling Adults

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
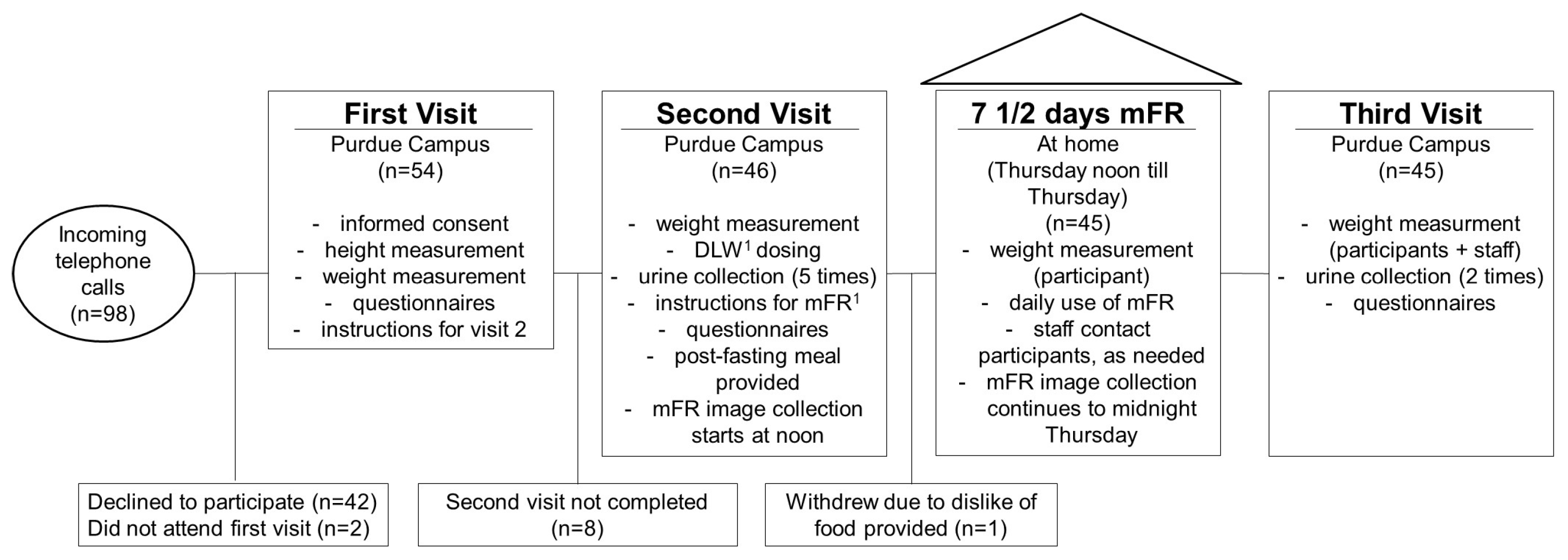
2.1. Study Participants
2.2. Study Design
2.3. Estimating Energy Content for the Food Pack-Outs
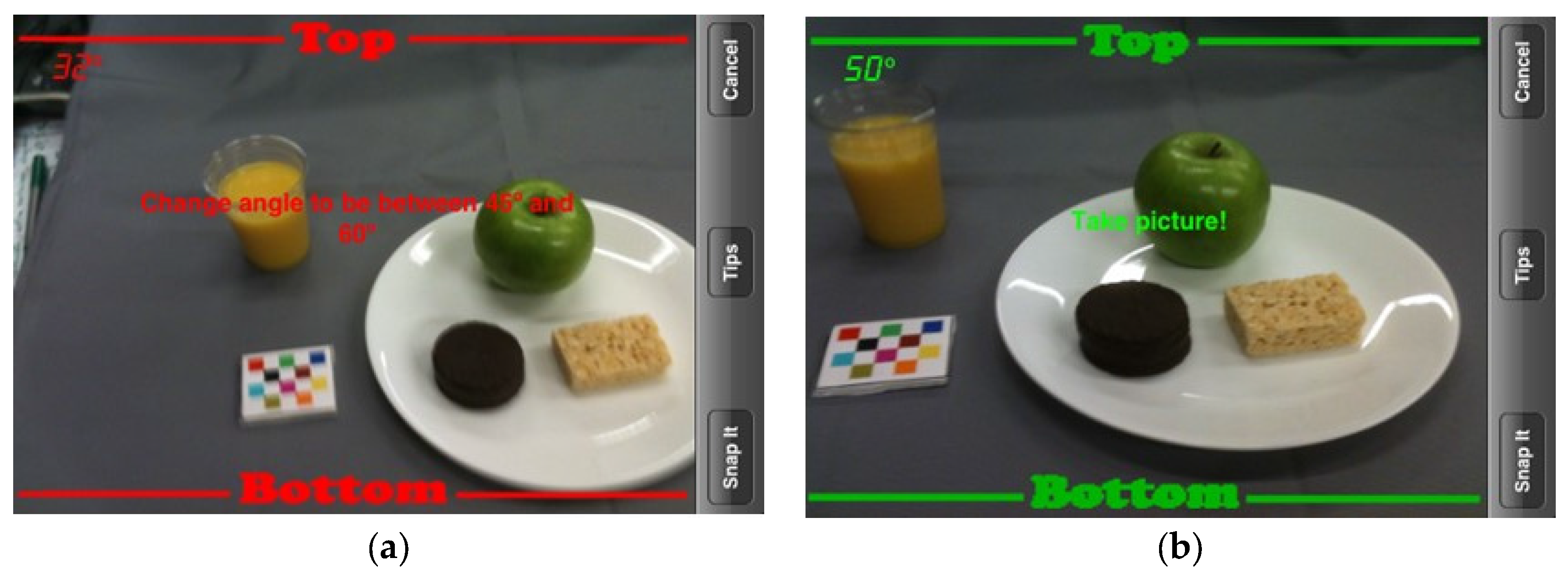
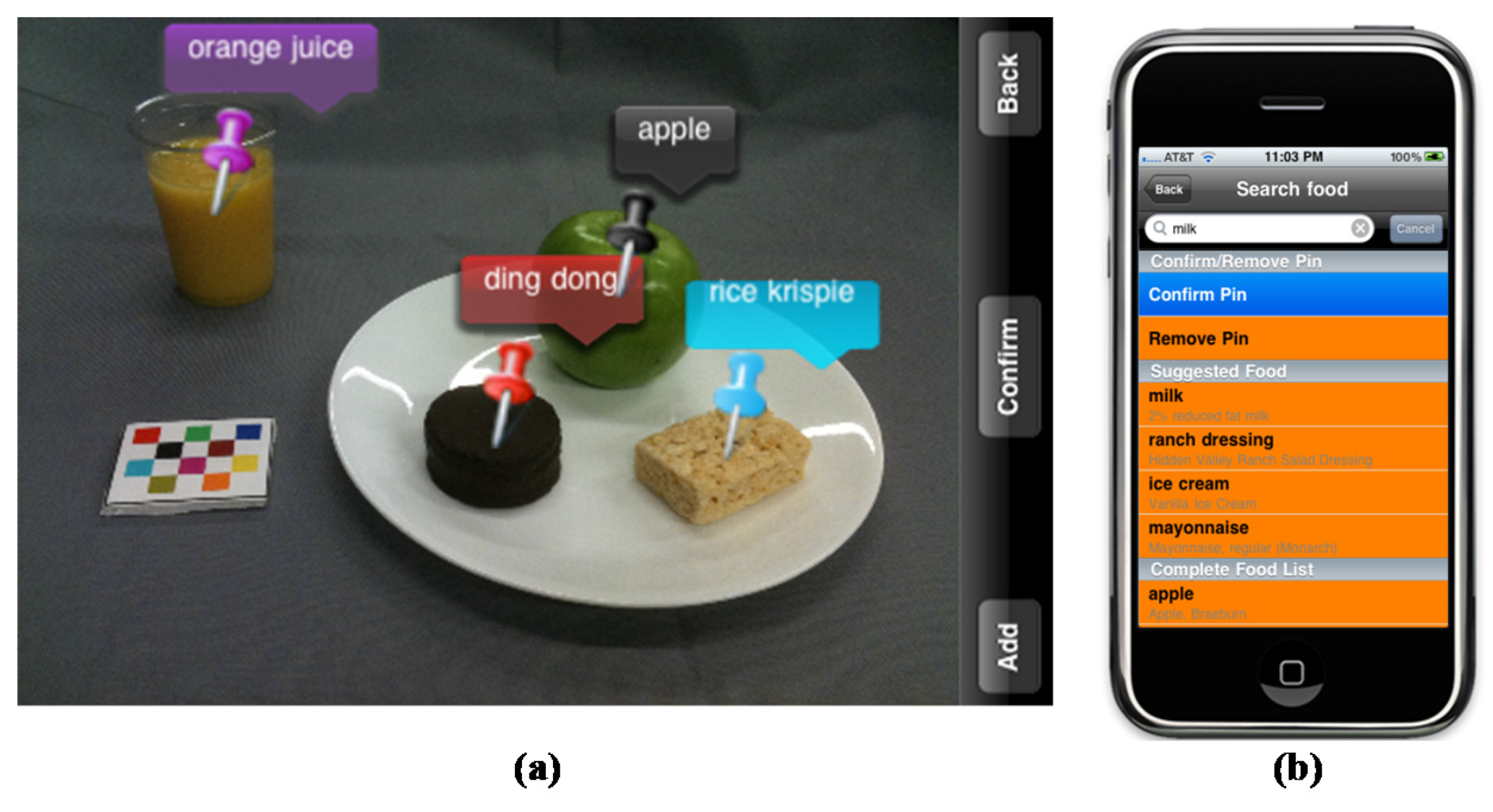
2.4. Description of the mFR
2.5. Total Energy Expenditure
2.6. Energy Intake
2.7. Identification/Quantifying of Misreporting
2.8. Statistical Methods
3. Results
3.1. Characteristics of the Study Sample
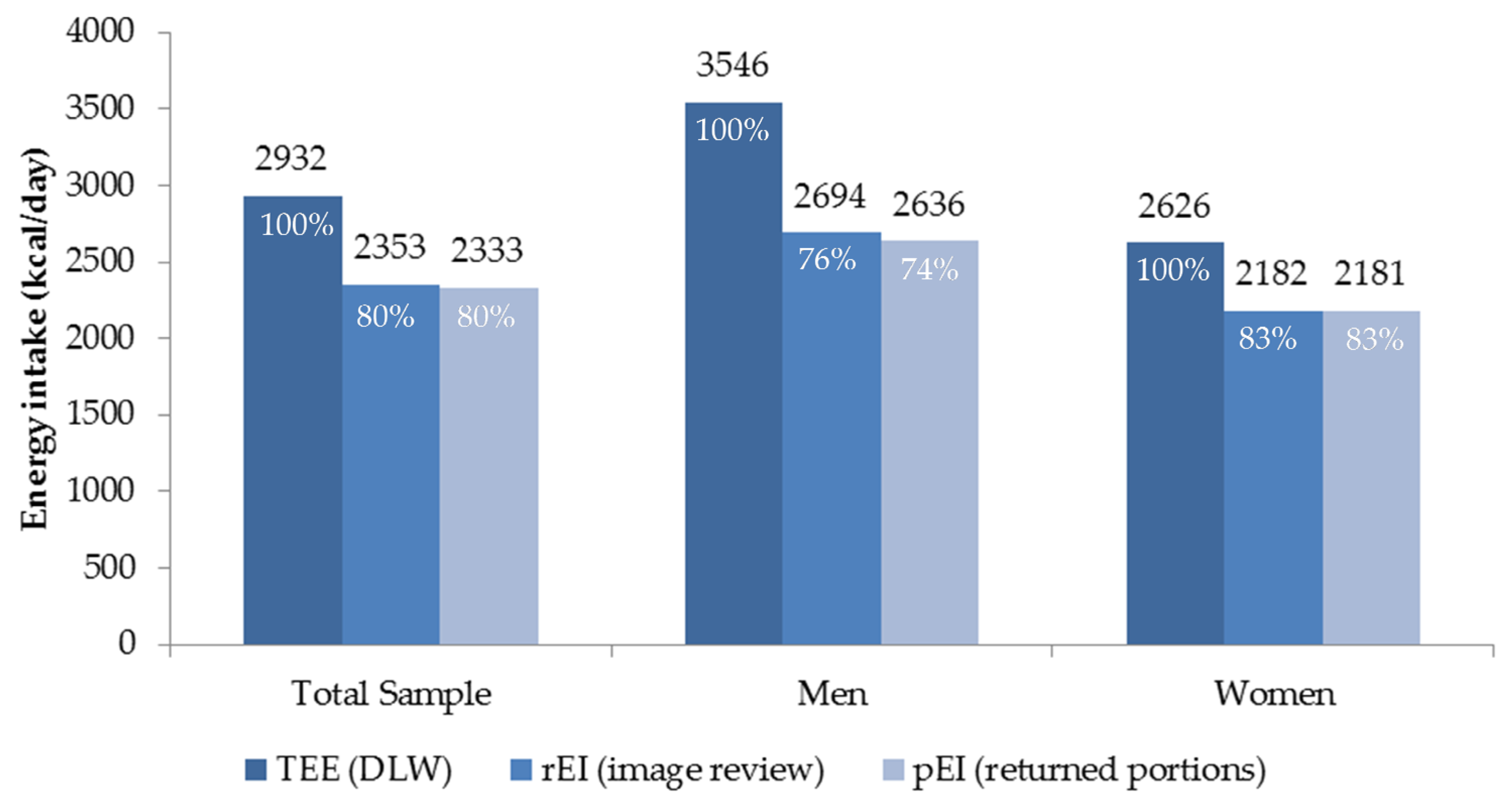
3.2. Energy Intake
3.3. Energy Misreporting
3.4. Usability
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bread, Bagel, Plain | Fruit, Orange, Clementine | Pretzels |
| Bread, English Muffin | Fruit, Orange, Navel | Pudding, Chocolate |
| Bread, Texas Toast | Fruit, Pear, Bartlett, fresh | Rice Krispie Treat |
| Bread, Whole Wheat | Fruit, Strawberries, fresh | Sandwich, Ham and Cheese |
| Cereal, Wheaties | Fruit, Watermelon | Sandwich, Turkey Wrap |
| Cheese, Cream, Plain, condiment pkt | Granola Bar | Sausage, Turkey |
| Cheese, Mozzarella Sticks | Ice Cream, Vanilla Sandwich | Snickers Bar |
| Cookies, Chocolate Chip | Jelly, Strawberry, condiment pkt | Soup, Chicken Noodle |
| Cookies, Snicker Doodle | Juice, Orange | Syrup, Maple, condiment pkt |
| Crackers, Goldfish | Lasagna, Lean Cuisine | Turkey Tettrazini, Stouffer’s |
| Crackers, Saltines | Lemonade | Veg, Broccoli w/cheese sauce |
| Ding Dong, Chocolate Cake Roll | Margarine, condiment pkt | Veg, Carrots, baby |
| Dip, Ranch Dressing, condiment pkt | Mayonnaise, condiment pkt | Veg, Celery, sticks |
| Doritos Chips | Meatloaf, Stouffer’s | Veg, Mixed/Lettuce Salad |
| Dressing, Fat Free Italian, condiment pkt | Milk | Veg, Peas |
| Dressing, Ranch, condiment pkt | Muffins, Mini | Veg, Potatoes, steamed |
| Frozen Fruit Bar | Mustard, condiment pkt | Veg, Tomatoes, Grape |
| Fruit, Apple, red | Pancakes | Yogurt, Mixed Berry |
| Fruit, Banana | Peanut Butter, condiment pkt | Yogurt, Strawberry |
| Fruit, Cocktail | Pizza, Stouffer’s French Bread | |
| Fruit, Grapes | Potato Chips |
| Beer | Margarita |
|---|---|
| Coffee | Marshmallow |
| Coffee latte (unsweetened) | Mellow Yellow/Mountain Dew/Orange Soda |
| Coke Zero/Diet Coke | Powerade |
| Coke/Pepsi | Red Wine |
| Diet Mountain Dew | Reese’s Cup |
| Dr. Pepper | Sprite/7-Up |
| Fruit punch | Tea (sweetened or flavored) |
| Gatorade | Tea (unsweetened) |
| Ginger Ale | Tortilla chips, Tostitos tortilla chips |
| Hawaiian Punch/Cran-Apple Juice/Hi-C | Water |
| Lemonade, Minute Maid Lemonade |
References
- Kirkpatrick, S.I.; Subar, A.F.; Douglass, D.; Zimmerman, T.P.; Thompson, F.E.; Kahle, L.L.; George, S.M.; Dodd, K.W.; Potischman, N. Performance of the Automated Self-Administered 24-h recall relative to a measure of true intakes and to an interviewer-administered 24-h recall. Am. J. Clin. Nutr. 2014, 100, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.K.; Correa, J.B.; Han, H.; Allen, H.R.; Rood, J.C.; Champagne, C.M.; Gunturk, B.K.; Bray, G.A. Validity of the remote food photography method (RFPM) for estimating energy and nutrient intake in near real-time. Obesity 2012, 20, 891–899. [Google Scholar] [CrossRef] [PubMed]
- Daugherty, B.L.; Schap, T.E.; Ettienne-Gittens, R.; Zhu, F.M.; Bosch, M.; Delp, E.J.; Ebert, D.S.; Kerr, D.A.; Boushey, C.J. Novel technologies for assessing dietary intake: Evaluating the usability of a mobile telephone food record among adults and adolescents. J. Med. Int. Res. 2012, 14, e58. [Google Scholar] [CrossRef] [PubMed]
- Six, B.L.; Schap, T.E.; Zhu, F.M.; Mariappan, A.; Bosch, M.; Delp, E.J.; Ebert, D.S.; Kerr, D.A.; Boushey, C.J. Evidence-based development of a mobile telephone food record. J. Am. Diet. Assoc. 2010, 110, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Boushey, C.J.; Spoden, M.; Zhu, F.M.; Delp, E.J.; Kerr, D.A. New mobile methods for dietary assessment: Review of image-assisted and image-based dietary assessment methods. Proc. Nutr. Soc. 2016, 12, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Gemming, L.; Utter, J.; Mhurchu, C.N. Image-Assisted Dietary Assessment: A Systematic Review of the Evidence. J. Acad. Nutr. Diet. 2014, 115, 64–77. [Google Scholar] [CrossRef] [PubMed]
- Rollo, M.E.; Ash, S.; Lyons-Wall, P.; Russell, A.W. Evaluation of a mobile phone image-based dietary assessment method in adults with type 2 diabetes. Nutrients 2015, 7, 4897–4910. [Google Scholar] [CrossRef] [PubMed]
- Casperson, S.L.; Sieling, J.; Moon, J.; Johnson, L.A.; Roemmich, J.N.; Whigham, L. A Mobile Phone Food Record App to Digitally Capture Dietary Intake for Adolescents in a Free-Living Environment: Usability Study. JMIR mHealth uHealth 2015, 3, e30. [Google Scholar] [CrossRef] [PubMed]
- Pettitt, C.; Liu, J.; Kwasnicki, R.M.; Yang, G.Z.; Preston, T.; Frost, G. A pilot study to determine whether using a lightweight, wearable micro-camera improves dietary assessment accuracy and offers information on macronutrients and eating rate. Br. J. Nutr. 2016, 115, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, S.I.; Potischman, N.; Dodd, K.W.; Douglass, D.; Zimmerman, T.P.; Kahle, L.L.; Thompson, F.E.; George, S.M.; Subar, A.F. The use of digital images in 24-hour recalls may lead to less misestimation of portion size compared with traditional interviewer-administered recalls. J. Nut. 2016, 146, 2567–2573. [Google Scholar] [CrossRef] [PubMed]
- Gemming, L.; Rush, E.; Maddison, R.; Doherty, A.; Gant, N.; Utter, J.; Ni Mhurchu, C. Wearable cameras can reduce dietary under-reporting: Doubly labelled water validation of a camera-assisted 24 h recall. Br. J. Nutr. 2015, 113, 284–291. [Google Scholar] [CrossRef] [PubMed]
- DeLany, J.P. Energy Requirement Methodology. In Nutrition in the Prevention and Treatment of Disease; Coulston, A.M., Boushey, C.J., Ferruzzi, M., Eds.; Academic Press: Cambridge, MA, USA, 2013; pp. 81–95. [Google Scholar]
- Livingstone, M.B.E.; Black, A.E. Markers of the validity of reported energy intake. J. Nutr. 2003, 133, 895S–920S. [Google Scholar] [PubMed]
- Schoeller, D.A. Recent advances from application of doubly labeled water to measurement of human energy expenditure. J. Nutr. 1999, 129, 1765–1768. [Google Scholar] [PubMed]
- Six, B.L.; Mariappan, A.; Schap, T.E.; Kerr, D.A.; Delp, E.J.; Ebert, D.S.; Boushey, C.J. Evaluation of adolescents’ ability to use a mobile telephone food record. J. Am. Diet. Assoc. 2008, 109, A78. [Google Scholar] [CrossRef]
- Aflague, T.F.; Boushey, C.J.; Guerrero, R.T.; Ahmad, Z.; Kerr, D.A.; Delp, E.J. Feasibility and Use of the Mobile Food Record for Capturing Eating Occasions among Children Ages 3–10 Years in Guam. Nutrients 2015, 7, 4403–4415. [Google Scholar] [CrossRef] [PubMed]
- Boushey, C.J.; Harray, A.J.; Kerr, D.A.; Schap, T.E.; Paterson, S.; Aflague, T.; Bosch, R.M.; Ahmad, Z.; Delp, E.J. How Willing Are Adolescents to Record Their Dietary Intake? The Mobile Food Record. JMIR mHealth uHealth 2015, 3, e47. [Google Scholar] [CrossRef] [PubMed]
- Godin, G.; Shephard, R.J. A simple method to assess exercise behavior in the community. Can. J. Appl. Sport Sci. 1985, 10, 141–146. [Google Scholar] [PubMed]
- Ekelund, U.; Sepp, H.; Brage, S.; Becker, W.; Jakes, R.; Hennings, M.; Wareham, N.J. Criterion-related validity of the last 7-day, short form of the International Physical Activity Questionnaire in Swedish adults. Public Health Nutr. 2006, 9, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Stunkard, A.J.; Messick, S. The three-factor eating questionnaire to measure dietary restraint, disinhibition and hunger. J. Psychosom. Res. 1985, 29, 71–83. [Google Scholar] [CrossRef]
- Ahmad, Z.; Bosch, M.; Khanna, N.; Kerr, D.A.; Boushey, C.J.; Zhu, F.; Delp, E.J. A Mobile Food Record For Integrated Dietary Assessment. In Proceedings of the 2nd International Workshop on Multimedia Assisted Dietary Management, Amsterdam, The Netherlands, 15–19 October 2016; pp. 53–62.
- Institute of Medicine Food and Nutrition Board. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids (Macronutrients); The National Academies Press: Washington, WA, USA, 2005. [Google Scholar]
- Zhu, F.; Bosch, M.; Khanna, N.; Boushey, C.J.; Delp, E.J. Multiple hypotheses image segmentation and classification with application to dietary assessment. IEEE J. Biomed. Health Inform. 2015, 19, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.; Bosch, M.; Woo, I.; Kim, S.; Boushey, C.J.; Ebert, D.S.; Delp, E.J. The use of mobile devices in aiding dietary assessment and evaluation. IEEE J. Sel. Top. Signal Process. 2010, 4, 756–766. [Google Scholar] [PubMed]
- Xu, C.; Zhu, F.; Khanna, N.; Boushey, C.J.; Delp, E.J. Image enhancement and quality measures for dietary assessment using mobile devices. In Proceedings of the IS&T/SPIE Conference on Computational Imagin X 8296, San Francisco, CA, USA, 22–26 January 2012.
- Hebert, J.R.; Ebbeling, C.B.; Matthews, C.E.; Hurley, T.G.; Ma, Y.; Druker, S.; Clemow, L. Systematic errors in middle-aged women’s estimates of energy intake: Comparing three self-report measures to total energy expenditure from doubly labeled water. Ann. Epidemiol. 2002, 12, 577–586. [Google Scholar] [CrossRef]
- Champagne, C.M.; Bray, G.A.; Kurtz, A.A.; Monteiro, J.B.; Tucker, E.; Volaufova, J.; Delany, J.P. Energy intake and energy expenditure: A controlled study comparing dietitians and non-dietitians. J. Am. Diet. Assoc. 2002, 102, 1428–1432. [Google Scholar] [CrossRef]
- Barnard, J.A.; Tapsell, L.C.; Davies, P.S.W.; Storlien, L.H. Relationship of high energy expenditure and variation in dietary intake with reporting accuracy of 7 days food records and diet histories in a group of healthy adult volunteers. Eur. J. Clin. Nutr. 2002, 56, 358–367. [Google Scholar] [CrossRef] [PubMed]
- DeLany, J.P.; Kelly, D.E.; Hames, K.C.; Jakicic, J.M.; Goodpaster, B.H. High energy expenditure masks low physical activity in obesity. Int. J. Obes. 2013, 37, 1006–1011. [Google Scholar] [CrossRef] [PubMed]
- Racette, S.B.; Schoeller, D.A.; Luke, A.H.; Shay, K.; Hnilicka, J.; Kushner, R.F. Relative dilution spaces of 2H- and 18O-labeled water in humans. Am. J. Physiol. 1994, 267, E585–E590. [Google Scholar] [PubMed]
- Black, A.E.; Cole, T.J. Biased over- or under-reporting is characteristic of individuals whether over time or by different assessment methods. J. Am. Diet. Assoc. 2001, 101, 70–80. [Google Scholar] [CrossRef]
- Subar, A.F.; Kipnis, V.; Troiano, R.; Midthune, D.; Schoeller, D.A.; Bingham, S.; Sharbaugh, C.O.; Trabulsi, J.; Runswick, S.; Ballard-Barbash, R.; et al. Using intake biomarkers to evaluate the extent of dietary misreporting in a large sample of adults: The OPEN Study. Am. J. Epidemiol. 2003, 158, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- National Heart Lung and Blood Institute. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. Available online: www.nhlbi.nih.gov/files/docs/guidelines/ob_gdlns.pdf (accessed on 19 March 2017).
- Amireault, S.; Godin, G. The Godin-Shephard Leisure-Time Physical Activity Questionnaire: Validity evidence supporting its use for classifying healhty adults into active and insufficiently active categories. Percept. Mot. Skills 2015, 120, 1–19. [Google Scholar] [CrossRef] [PubMed]
- McClung, H.L.; Sigrist, L.D.; Smith, T.J.; Karl, J.P.; Rood, J.C.; Young, A.J.; Bathalon, G.P. Monitoring energy intake: A hand-held personal digital assistant provides accuracy comparable to written records. J. Am. Diet. Assoc. 2009, 109, 1241–1245. [Google Scholar] [CrossRef] [PubMed]
- Blanton, C.A.; Moshfegh, A.J.; Baer, D.J.; Kretsch, M.J. The USDA automated multiple-pass method accurately estimates group total energy and nutrient intake. J. Nutr. 2006, 136, 2594–2599. [Google Scholar] [PubMed]
- Trabulsi, J.; Schoeller, D.A. Evaluation of dietary assessment instruments against doubly labeled water, a biomarker of habitual energy intake. Am. J. Physiol. Endocrinol. Metab. 2001, 281, E891–E899. [Google Scholar] [PubMed]
- Prentice, A.M.; Black, A.E.; Coward, W.A.; Davies, H.L.; Goldberg, G.R.; Nurgatroyd, P.R.; Ashford, J.; Sawyer, M.; Whitehead, R.G. High levels of energy expenditure in obese women. Br. Med. J. 1986, 292, 983–987. [Google Scholar] [CrossRef]
- Goris, A.H.; Westerterp-Plantenga, M.S.; Westerterp, K.R. Undereating and underrecording of habitual food intake in obese men: Selective underreporting of fat intake. Am. J. Clin. Nutr. 2000, 71, 130–134. [Google Scholar] [PubMed]
- Livingstone, M.B.; Prentice, A.M.; Strain, J.J.; Coward, W.A.; Ceesay, S.M.; Strain, J.J.; McKenna, P.G.; Nevin, G.B.; Barker, M.E.; Hickey, R.J. Accuracy of weighed dietary records in studies of diet and health. BMJ 1990, 300, 708–712. [Google Scholar] [CrossRef] [PubMed]
- Seale, J.L.; Rumpler, W.V. Comparison of energy expenditure measurements by diet records, energy intake balance, doubly labeled water and room calorimetry. Eur. J. Clin. Nutr. 1997, 51, 856–863. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.J.; Su, W.; Jones, P.J.; Lockwood, G.A.; Tritchler, D.L.; Boyd, N.F. Comparison of energy intakes determined by food records and doubly labeled water in women participating in a dietary-intervention trial. Am. J. Clin. Nutr. 1996, 63, 483–490. [Google Scholar] [PubMed]
- Moshfegh, A.J.; Rhodes, D.G.; Baer, D.J.; Murayi, T.; Clemens, J.C.; Rumpler, W.V.; Paul, D.R.; Sebastian, R.S.; Kuczynski, K.J.; Ingwersen, L.A.; et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr. 2008, 88, 324–332. [Google Scholar] [PubMed]
- Haines, P.S.; Hama, M.Y.; Guilkey, D.K.; Popkin, B.M. Weekend eating in the United States is linked with greater energy, fat, and alcohol intake. Obes. Res. 2003, 11, 845–849. [Google Scholar] [CrossRef] [PubMed]
- De Jonge, L.; DeLany, J.P.; Nguyen, T.; Howard, J.; Hadley, E.C.; Redman, L.M.; Ravussin, E. Validation study of energy expenditure and intake during calorie restriction using doubly labeled water and changes in body composition. Am. J. Clin. Nutr. 2007, 85, 73–79. [Google Scholar] [PubMed]
- Subar, A.F.; Freedman, L.S.; Tooze, J.A.; Kirkpatrick, S.I.; Boushey, C.; Neuhouser, M.L.; Thompson, F.E.; Potischman, N.; Guenther, P.M.; Tarasuk, V.; et al. Addressing current criticism regarding the value of self-report dietary data. J. Nutr. 2015, 145, 2639–2645. [Google Scholar] [CrossRef] [PubMed]
- Rebro, S.M.; Patterson, R.E.; Kristal, A.R.; Cheney, C.L. The effect of keeping food records on eating patterns. J. Am. Diet. Assoc. 1998, 98, 1163–1165. [Google Scholar] [CrossRef]
- Vuckovic, N.; Ritenbaugh, C.; Taren, D.L.; Tobar, M. A qualitative study of participants’ experiences with dietary assessment. J. Am. Diet. Assoc. 2000, 100, 1023–1028. [Google Scholar] [CrossRef]
- Kikunaga, S.; Tin, T.; Ishibashi, G.; Wang, D.H.; Kira, S. The application of a handheld personal digital assistant with camera and mobile phone card (Wellnavi) to the general population in a dietary survey. J. Nutr. Sci. Vitaminol. 2007, 53, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.H.; Kogashiwa, M.; Ohta, S.; Kira, S. Validity and reliability of a dietary assessment method: The application of a digital camera with a mobile phone card attachment. J. Nutr. Sci. Vitaminol. 2002, 48, 498–504. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.H.; Kogashiwa, M.; Kira, S. Development of a new instrument for evaluating individuals’ dietary intakes. J. Am. Diet. Assoc. 2006, 106, 1588–1593. [Google Scholar] [CrossRef] [PubMed]
- Hebert, J.R. Social desirability trait: Biaser or driver of self-reported dietary intake. Am. J. Clin. Nutr. 2016, 116, 1895–1898. [Google Scholar] [CrossRef] [PubMed]





| Characteristics | Men | Women |
|---|---|---|
| n = 15 | n = 30 | |
| BMI 1 categories (NIH 1) | n | |
| Underweight | 0 | 2 |
| Normal weight | 7 | 12 |
| Overweight | 4 | 10 |
| Obese | 4 | 6 |
| Hispanic or Latino | 2 | 2 |
| Black | 0 | 2 |
| White | 13 | 20 |
| Asian | 2 | 7 |
| Another Race | 0 | 1 |
| Active 2 | 10 | 18 |
| Insufficiently active | 5 | 12 |
| Mean ± SD 1 | ||
| Age (years) | 32 ± 9 | 33 ± 13 |
| BMI (kg/m2) | 27 ± 5 | 26 ± 7 |
| Height (cm) | 180 ± 7 | 166 ± 6 |
| Weight (kg) | 87 ± 20 | 73 ± 19 |
| Weight Change (%) | 0.3 ± 0.6 | 0.2 ± 1 |
| Completed days of record | 7 | 6.7 |
| Reported energy intake (rEI) (kcal/day) | 2694 ± 794 | 2182 ± 577 |
| Presumed energy intake (pEI) (kcal/day) | 2636 ± 692 | 2181 ± 517 |
| TEE 1 (kcal/day) | 3546 ± 681 | 2626 ± 492 |
| Characteristics | Underreporter | Accurate Reporter | Overreporter |
|---|---|---|---|
| Variable (n) | n (%) | n (%) | n (%) |
| Total (45) | 24 (53) | 20 (44) | 1 (2) |
| Male (15) | 11 (73) | 4 (37) | |
| Female (30) | 13 (43) | 16 (53) | 1 (3) |
| Body mass index category | |||
| Underweight (2) | 2 (100) | ||
| Normal weight (19) | 11 (58) | 8 (42) | |
| Overweight (14) | 7 (50) | 7 (50) | |
| Obese (10) | 6 (60) | 3 (30) | 1 (10) |
| Age (years) | |||
| 20–29.9 (28) | 15 (54) | 12 (43) | 1 (3) |
| 30–39.9 (6) | 4 (67) | 2 (33) | |
| ≥40 (11) | 5 (46) | 6 (55) | |
| Mean ± SD | Mean ± SD | ||
| rEI 1 (kcal/day) | 2138 ± 471 | 2,515 ± 756 | 4230 |
| TEE 1 (kcal/day) | 3138 ± 596 | 2,673 ± 774 | 3180 |
| rEI:TEE | 0.68 ± 0.10 | 0.94 ± 0.10 | 1.33 |
| Questions Asked before and after Using the Technology Assisted Dietary Assessment (TADA) mFR (Before Phrase/After Phrase) | Before 7.5 Study Days 1 n (%) of 45 | After 7.5 Study Days 1 n (%) of 45 |
|---|---|---|
| Remembering to take an image BEFORE MEALS would be easy/was easy. | 32 (71) | 45 (100) 2 |
| Remembering to take an image AFTER MEALS would be easy/was easy. | 32 (71) | 34 (76) |
| Remembering to take an image BEFORE SNACKS would be easy/was easy. | 17 (38) | 36 (80) 2 |
| Remembering to take an image AFTER SNACKS would be easy/was easy. | 21 (47) | 29 (64) |
| I think it would be /I thought it was easy to carry a CREDIT CARD sized fiducial marker. | 41 (91) | 42 (93) |
| I think it would be/I thought it was easy to use a CREDIT CARD sized fiducial marker | 39 (87) | 43 (96) |
| Statements and a Question Regarding Use of the Technology Assisted Dietary Assessment (TADA) mFR Application | Responses, n (%) | ||
|---|---|---|---|
| Strongly Agree or Agree | Neither Agree or Disagree | Disagree or Strongly Disagree | |
| I found it easy to include the fiducial marker in the picture of my meals. | 38 (84) | 4 (9) | 3 (7) |
| I found it easy to include the fiducial marker in the picture of my snacks. | 40 (89) | 3 (7) | 2 (4) |
| The screens were easy to read. | 45 (100) | 0 | 0 |
| The TADA application on the iPhone was easy to use. | 37 (82) | 5 (11) | 3 (7) |
| The directions about when to take an image of my meals and snacks were easy to follow. | 43 (96) | 2 (4) | 0 |
| The TADA iPhone interfered with my daily activities. | 15 (33) | 19 (42) | 11 (24) |
| The TADA iPhone interfered with my social interactions. | 15 (33) | 13 (29) | 17 (38) |
| I would like to participate in another study using the TADA iPhone application. | 33 (73) | 8 (18) | 4 (9) |
| The directions about how to use the TADA iPhone application were easy to follow. | 44 (98) | 1 (2) | 0 |
| Overall, the TADA iPhone application was a nuisance to use. | 5 (11) | 20 (44) | 20 (45) |
| Overall, the TADA iPhone application was enjoyable to use. | 22 (49) | 21 (47) | 2 (4) |
| The extra cords helped keep the TADA iPhone charged at all times. | 35 (78) | 8 (18) | 2 (4) |
| It was easy to use the TADA iPhone application when I was away from home. | 26 (58) | 7 (16) | 12 (27) |
| It was easy to carry two phones. | 25 (56) | 6 (13) | 14 (31) |
| More instructions about how to use the TADA iPhone application would have been helpful. | 8 (18) | 14 (31) | 23 (51) |
| Understanding the purpose of the TADA iPhone application motivated me to use it. | 28 (62) | 15 (33) | 2 (4) |
| I feel confident that the information collected by the TADA iPhone application will only be seen by researchers and not used against me. | 43 (96) | 1 (2) | 1 (2) |
| Never or almost never | Sometimes | Fairly or very often | |
| I had problems using the TADA iPhone application. | 23 (51) | 16 (36) | 6 (13) |
| Extremely or mostly comfortable | Somewhat comfortable | Not too comfortable or not comfortable at all | |
| Did you feel comfortable using the TADA iPhone application? | 38 (84) | 6 (13) | 1 (2) |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boushey, C.J.; Spoden, M.; Delp, E.J.; Zhu, F.; Bosch, M.; Ahmad, Z.; Shvetsov, Y.B.; DeLany, J.P.; Kerr, D.A. Reported Energy Intake Accuracy Compared to Doubly Labeled Water and Usability of the Mobile Food Record among Community Dwelling Adults. Nutrients 2017, 9, 312. https://doi.org/10.3390/nu9030312
Boushey CJ, Spoden M, Delp EJ, Zhu F, Bosch M, Ahmad Z, Shvetsov YB, DeLany JP, Kerr DA. Reported Energy Intake Accuracy Compared to Doubly Labeled Water and Usability of the Mobile Food Record among Community Dwelling Adults. Nutrients. 2017; 9(3):312. https://doi.org/10.3390/nu9030312
Chicago/Turabian StyleBoushey, Carol J., Melissa Spoden, Edward J. Delp, Fengqing Zhu, Marc Bosch, Ziad Ahmad, Yurii B. Shvetsov, James P. DeLany, and Deborah A. Kerr. 2017. "Reported Energy Intake Accuracy Compared to Doubly Labeled Water and Usability of the Mobile Food Record among Community Dwelling Adults" Nutrients 9, no. 3: 312. https://doi.org/10.3390/nu9030312
APA StyleBoushey, C. J., Spoden, M., Delp, E. J., Zhu, F., Bosch, M., Ahmad, Z., Shvetsov, Y. B., DeLany, J. P., & Kerr, D. A. (2017). Reported Energy Intake Accuracy Compared to Doubly Labeled Water and Usability of the Mobile Food Record among Community Dwelling Adults. Nutrients, 9(3), 312. https://doi.org/10.3390/nu9030312