Associations between Folate and Vitamin B12 Levels and Inflammatory Bowel Disease: A Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
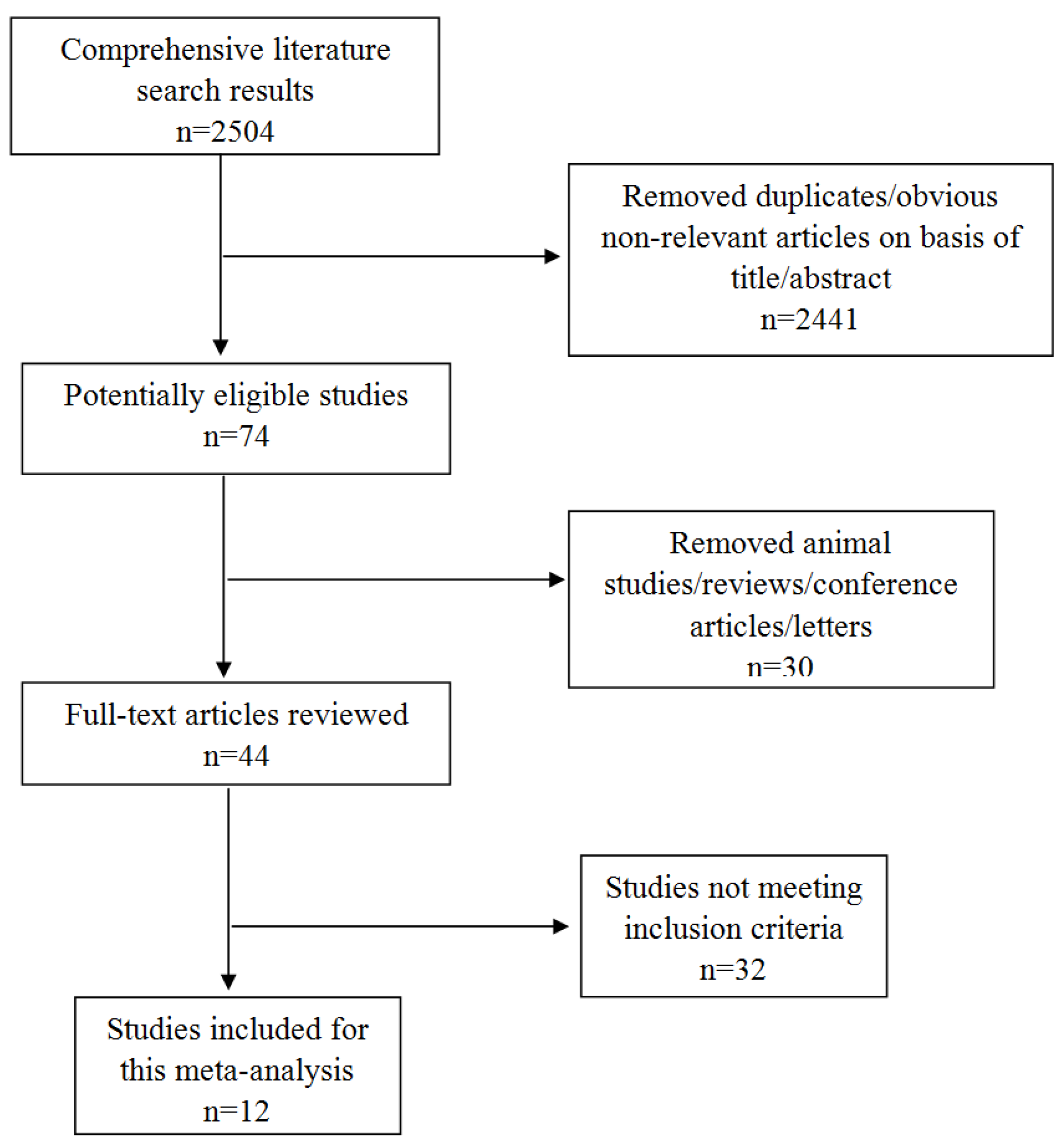
2.1. Sources and Methods of Data Retrieval
2.2. Inclusion Criteria
2.3. Data Abstraction
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Leone, V.; Chang, E.B.; Devkota, S. Diet, microbes, and host genetics: The perfect storm in inflammatory bowel diseases. J. Gastroenterol. 2013, 48, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Kaser, A.; Zeissig, S.; Blumberg, R.S. Inflammatory bowel disease. Annu. Rev. Immunol. 2010, 28, 573–621. [Google Scholar] [CrossRef] [PubMed]
- Leddin, D.; Tamim, H.; Levy, A.R. Is folate involved in the pathogenesis of inflammatory bowel disease? Med. Hypotheses 2013, 81, 940–941. [Google Scholar] [CrossRef] [PubMed]
- Shanahan, F. The microbiota in inflammatory bowel disease: Friend, bystander, and sometime-villain. Nutr. Rev. 2012, 70 (Suppl. 1), S31–S37. [Google Scholar] [CrossRef] [PubMed]
- Kellermayer, R. Epigenetics and the developmental origins of inflammatory bowel diseases. Can. J. Gastroenterol. 2012, 26, 909–915. [Google Scholar] [CrossRef] [PubMed]
- Bermejo, F.; Algaba, A.; Guerra, I.; Chaparro, M.; De-La-Poza, G.; Valer, P.; Piqueras, B.; Bermejo, A.; Garcia-Alonso, J.; Perez, M.J.; et al. Should we monitor vitamin b12 and folate levels in crohn’s disease patients? Scand. J. Gastroenterol. 2013, 48, 1272–1277. [Google Scholar] [CrossRef] [PubMed]
- Owczarek, D.; Rodacki, T.; Domagala-Rodacka, R.; Cibor, D.; Mach, T. Diet and nutritional factors in inflammatory bowel diseases. World J. Gastroenterol. 2016, 22, 895–905. [Google Scholar] [CrossRef] [PubMed]
- Lachner, C.; Steinle, N.I.; Regenold, W.T. The neuropsychiatry of vitamin B12 deficiency in elderly patients. J. Neuropsychiatry Clin. Neurosci. 2012, 24, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Cario, H.; Smith, D.E.; Blom, H.; Blau, N.; Bode, H.; Holzmann, K.; Pannicke, U.; Hopfner, K.P.; Rump, E.M.; Ayric, Z.; et al. Dihydrofolate reductase deficiency due to a homozygous DHFR mutation causes megaloblastic anemia and cerebral folate deficiency leading to severe neurologic disease. Am. J. Hum. Genet. 2011, 88, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Oussalah, A.; Gueant, J.L.; Peyrin-Biroulet, L. Meta-analysis: Hyperhomocysteinaemia in inflammatory bowel diseases. Aliment. Pharmacol. Ther. 2011, 34, 1173–1184. [Google Scholar] [CrossRef] [PubMed]
- Stipanuk, M.H. Sulfur amino acid metabolism: Pathways for production and removal of homocysteine and cysteine. Annu. Rev. Nutr. 2004, 24, 539–577. [Google Scholar] [CrossRef] [PubMed]
- Hoffbrand, V.; Provan, D. Abc of clinical haematology. Macrocytic anaemias. Br. Med. J. 1997, 314, 430–433. [Google Scholar] [CrossRef]
- Vasilopoulos, S.; Saiean, K.; Emmons, J.; Berger, W.L.; Abu-Hajir, M.; Seetharam, B.; Binion, D.G. Terminal ileum resection is associated with higher plasma homocysteine levels in crohn’s disease. J. Clin. Gastroenterol. 2001, 33, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Chowers, Y.; Sela, B.A.; Holland, R.; Fidder, H.; Simoni, F.B.; Bar-Meir, S. Increased levels of homocysteine in patients with Crohn’s disease are related to folate levels. Am. J. Gastroenterol. 2000, 95, 3498–3502. [Google Scholar] [CrossRef] [PubMed]
- Yakut, M.; Ustun, Y.; Kabacam, G.; Soykan, I. Serum vitamin B12 and folate status in patients with inflammatory bowel diseases. Eur. J. Intern. Med. 2010, 21, 320–323. [Google Scholar] [CrossRef] [PubMed]
- Koutroubakis, I.E.; Dilaveraki, E.; Vlachonikolis, I.G.; Vardas, E.; Vrentzos, G.; Ganotakis, E.; Mouzas, I.A.; Gravanis, A.; Emmanouel, D.; Kouroumalis, E.A. Hyperhomocysteinemia in Greek patients with inflammatory bowel disease. Dig. Dis. Sci. 2000, 45, 2347–2351. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.; Altman, D. Chapter 16: Special topics in statistics. In Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Senn, S. Overstating the evidence: Double counting in meta-analysis and related problems. BMC Med. Res. Methodol. 2009, 9, 10. [Google Scholar] [CrossRef] [PubMed]
- Cochran, W.G. The combination of estimates from different experiments. Biometrics 1954, 10, 101–129. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Br. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. Br. Med. J. 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Jiang, Y.; Zhao, J.; Jiang, T.; Ge, L.; Zhou, F.; Chen, Z.; Lei, Y.; Huang, S.; Xia, B. Genetic polymorphism of methylenetetrahydrofolate reductase g1793a, hyperhomocysteinemia, and folate deficiency correlate with ulcerative colitis in central China. J. Gastroenterol. Hepatol. 2010, 25, 1157–1161. [Google Scholar] [CrossRef] [PubMed]
- Lambert, D.; Benhayoun, S.; Adjalla, C.; Gelot, M.A.; Renkes, P.; Felden, F.; Gerard, P.; Belleville, F.; Gaucher, P.; Gueant, J.L.; et al. Crohn’s disease and vitamin B12 metabolism. Dig. Dis. Sci. 1996, 41, 1417–1422. [Google Scholar] [CrossRef] [PubMed]
- Kuroki, F.; Iida, M.; Tominaga, M.; Matsumoto, T.; Hirakawa, K.; Sugiyama, S.; Fujishima, M. Multiple vitamin status in Crohn’s disease. Correlation with disease activity. Dig. Dis. Sci. 1993, 38, 1614–1618. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Miranda, C.; Martinez Prieto, M.; CasisHerce, B.; Sanchez Gomez, F.; Gomez Gonzalez, P.; Martinez Lopez, J.; Saenz-Lopez Perez, S.; Gomez de la Camara, A. Hyperhomocysteinemia and methylenetetrahydrofolate reductase 677c→t and 1298a→c mutations in patients with inflammatory bowel disease. Rev. Esp. Enferm. Dig. 2005, 97, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Erzin, Y.; Uzun, H.; Celik, A.F.; Aydin, S.; Dirican, A.; Uzunismail, H. Hyperhomocysteinemia in inflammatory bowel disease patients without past intestinal resections: Correlations with cobalamin, pyridoxine, folate concentrations, acute phase reactants, disease activity, and prior thromboembolic complications. J. Clin. Gastroenterol. 2008, 42, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Alkhouri, R.H.; Hashmi, H.; Baker, R.D.; Gelfond, D.; Baker, S.S. Vitamin and mineral status in patients with inflammatory bowel disease. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Akbulut, S.; Altiparmak, E.; Topal, F.; Ozaslan, E.; Kucukazman, M.; Yonem, O. Increased levels of homocysteine in patients with ulcerative colitis. World J. Gastroenterol. 2010, 16, 2411–2416. [Google Scholar] [CrossRef] [PubMed]
- Kallel, L.; Feki, M.; Sekri, W.; Segheir, L.; Fekih, M.; Boubaker, J.; Kaabachi, N.; Filali, A. Prevalence and risk factors of hyperhomocysteinemia in Tunisian patients with Crohn’s disease. J. Crohns Colitis 2011, 5, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Geerling, B.J.; Badart-Smook, A.; Stockbrugger, R.W.; Brummer, R.J. Comprehensive nutritional status in recently diagnosed patients with inflammatory bowel disease compared with population controls. Eur. J. Clin. Nutr. 2000, 54, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.L.; Mei, Q.; Xu, J.M.; Hu, N.Z.; Lu, C.X.; Fang, H.M. Significance of plasmichomocysteine, folate and vitamin B(12) in ulcerative colitis. Zhonghua Wei Chang Wai Ke Za Zhi 2011, 14, 185–187. (in Chinese). [Google Scholar] [PubMed]
- Zezos, P.; Papaioannou, G.; Nikolaidis, N.; Vasiliadis, T.; Giouleme, O.; Evgenidis, N. Hyperhomocysteinemia in ulcerative colitis is related to folate levels. World J. Gastroenterol. 2005, 11, 6038–6042. [Google Scholar] [CrossRef] [PubMed]
- Burr, N.E.; Hull, M.A.; Subramanian, V. Folic acid supplementation may reduce colorectal cancer risk in patients with inflammatory bowel disease: A systematic review and meta-analysis. J. Clin. Gastroenterol. 2017, 51, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Hwang, C.; Ross, V.; Mahadevan, U. Micronutrient deficiencies in inflammatory bowel disease: From A to zinc. Inflamm. Bowel Dis. 2012, 18, 1961–1981. [Google Scholar] [CrossRef] [PubMed]
- Bermejo, F.; Algaba, A.; Gisbert, J.P.; Nogueiras, A.R.; Poza, G.; Chaparro, M.; Valer, P.; Piqueras, B.M.; Villa, J.C.; Bermejo, A. Prospective controlled analysis of vitamin B12 and folate deficiency in Crohn’s disease. Gastroenterology 2011, 140, S-434. [Google Scholar]
- Battat, R.; Kopylov, U.; Szilagyi, A.; Saxena, A.; Rosenblatt, D.S.; Warner, M.; Bessissow, T.; Seidman, E.; Bitton, A. Vitamin B12 deficiency in inflammatory bowel disease: Prevalence, risk factors, evaluation, and management. Inflamm. Bowel Dis. 2014, 20, 1120–1128. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, S. Serum concentration of cobalamines during total parenteral nutrition in Crohn’s disease. JPEN J. Parenter. Enter. Nutr. 1986, 10, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Ward, M.; Kariyawasam, V.; Mogan, S.; Patel, K.; Pantelidou, M.; Sobczyńska-Malefora, A.; Porté, F.; Griffin, N.; Anderson, S.; Sanderson, J.; et al. Prevalence and Risk Factors for Functional Vitamin B12 Deficiency in Patients with Crohn’s Disease. Inflamm. Bowel Dis. 2015, 21, 2839–2847. [Google Scholar] [CrossRef] [PubMed]
- Jayaprakash, A.; Creed, T.; Stewart, L.; Colton, B.; Mountford, R.; Standen, G.; Probert, C. Should we monitor vitamin B12 levels in patients who have had end-ileostomy for inflammatory bowel disease? Int. J. Colorectal Dis. 2004, 19, 316–318. [Google Scholar] [CrossRef] [PubMed]
- Campbell, T.C.; Campbell, T.M. The China Study, 1st ed.; BenBella Books: Dallas, TX, USA, 2006. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Region | Score | Year | n | Assay Method | Age | Gender (Male/Female) | IBD/CD/UC (Mean ± SD) | Controls (Mean ± SD) | p | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IBD/CD/UC | C | IBD/CD/UC/C | IBD/CD/UC | C | FA (ng/mL) | B12 (pg/mL) | FA (ng/mL) | B12 (pg/mL) | FA | B12 | |||||
| Jiang et al. [22] | China | 8 | 2010 | 252 | 654 | chemiluminescence | -/-/45 ± 14/46 ± 17 | 147/105 | 279/374 | 4.97 ± 2.73 * | 437.53 ± 174.12 * | 6.74 ± 3.41 | 572.77 ± 175.33 | <0.001 | <0.001 |
| Lambert et al. [23] | France | 6 | 1996 | 21 | 20 | radioimmunoassay | - | 11/10 | 8/12 | 2.8 ± 2.8 # | 190 ± 146 # | 4.55 ± 3.26 | 207 ± 75 | NS | NS |
| Kuroki et al. [24] | Japan | 8 | 1993 | 24 | 24 | radioimmunoassay | -/26.4 ± 12.4/-/27.0 ± 4.2 | 17/7 | 14/10 | 641 ± 186 # | 682 ± 488 | <0.001 | |||
| Fernández-Miranda et al. [25] | Spain | 7 | 2005 | 52 | 186 | radioimmunoassay | 41.7 ± 11.9/-/-/41.9 ± 10.1 | 23/29 | 71/115 | 7.6 ± 4.1 | 499 ± 287 | 8.9 ± 3.7 | 603 ± 231 | <0.05 | <0.05 |
| Erzin et al. [26] | Turkey | 7 | 2008 | 105 | 85 | ELISA | 38.69 ± 12.13/-/-/37.61 ± 10.05 | - | - | 3.72 ± 1.44 | 600.14 ± 145.30 | 4.96 ± 1.19 | 700.32 ± 141.58 | <0.001 | |
| Alkhouri et al. [27] | U.S. | 8 | 2013 | 61 | 61 | - | 12.3 ± 3.9/12.1 ± 4.1/12.3 ± 3.5/12.1 ± 3.6 | 40/21 | 30/31 | 20.1 ± 6.5 | 775 ± 441 | 20.4 ± 5.5 | 727 ± 346 | ||
| 20.3 ± 7 # | 781 ± 372 # | ||||||||||||||
| 20.9 ± 5.9 * | 906 ± 669 * | ||||||||||||||
| Yakut et al. [15] | Turkey | 6 | 2010 | 138 | 53 | chemiluminescence | - | 64/74 | 19/34 | 7.7 ± 5.3 # | 281 ± 166 # | 9.9 ± 3.3 | 342 ± 179 | NS | NS |
| 8.6 ± 8.3 * | 348 ± 218 * | ||||||||||||||
| Akbulut et al. [28] | Turkey | 9 | 2010 | 55 | 45 | chemiluminescence | -/-/47.4 ± 13.80/46.4 ± 13.89 | 38/17 | 31/14 | 5.1 ± 2.19 * | 250.4 ± 82.49 * | 6.3 ± 0.87 | 327 ± 73.9 | <0.001 | <0.001 |
| Kallel et al. [29] | Tunisia | 6 | 2011 | 89 | 103 | specific immunochemical methods | 35.3 ± 12.6/-/-/36.5 ± 9.26 | 47/42 | 50/53 | 8.54 ± 3.04 | 295 ± 180 | 8.1 ± 3.11 | 378 ± 170 | NS | <0.001 |
| Geerling et al. [30] | Netherlands | 7 | 2000 | 69 | 69 | radioimmunoassay | -/30.1 ± 10.2/37.8 ± 14.7/35.4 ± 13.7 | 33/36 | 23/46 | 4.72 ± 4.02 # | 304.96 ± 82.27 # | 5.47 ± 2.47 * | 357.82 ± 121.58 * | NS | 0.05 |
| 5.03 ± 3.80 * | 364.59 ± 119.14 * | 5.78 ± 2.96 # | 365.95 ± 119.54 # | ||||||||||||
| Chen et al. [31] | China | 6 | 2011 | 112 | 110 | ELISA | -/-/39.4 ± 11.7/40.3 ± 10.8 | 58/54 | 56/54 | 3.37 ± 0.86 * | 147.25 ± 43.67 * | 4.03 ± 0.54 | 152.67 ± 45.17 | 0.005 | 0.004 |
| Koutroubakis et al. [16] | Greece | 6 | 2000 | 108 | 74 | IMx assay | - | 66/42 | - | 6.34 ± 3.05 # | 666.5 ± 366.8 # | 8.78 ± 3.07 | 377.5 ± 155.6 | <0.05 | <0.05 |
| 7.02 ± 3.13 * | 478.8 ± 257.7 * | ||||||||||||||
| Variables | n | I2 | Adj R2 | exp(b) | Std. Err. | t | p | 95% CI |
|---|---|---|---|---|---|---|---|---|
| Testing method | 10 | 0.00% | 100.00% | 0.81 | 0.10 | −1.60 | 0.154 * | 0.61, 1.10 |
| 0.55 | 0.08 | −4.00 | 0.005 # | 0.38, 0.78 | ||||
| 0.73 | 0.08 | −2.95 | 0.021 & | 0.56, 0.94 | ||||
| Year of publication | 14 | 76.64% | −8.34% | 1.007 | 0.02 | 0.35 | 0.729 | 0.97, 1.05 |
| Sample size | 14 | 76.12% | −11.49% | 1.00 | 0.00 | −0.35 | 0.729 | 0.99, 1.00 |
| Quality of studies | 14 | 76.51% | −10.63% | 0.99 | 0.10 | −0.05 | 0.959 | 0.79, 1.25 |
| Average age of patients | 9 | 80.56% | 18.27% | 0.98 | 0.01 | −1.58 | 0.159 | 0.95, 1.01 |
| Variables | n | I2 | Adj R2 | exp(b) | Std. Err. | t | p | 95% CI |
|---|---|---|---|---|---|---|---|---|
| Testing method | 11 | 73.32% | −1.84% | 0.86 | 0.27 | −0.47 | 0.654 * | 0.43, 1.76 |
| 1.22 | 0.37 | 0.66 | 0.530 # | 0.60, 2.47 | ||||
| 0.67 | 0.16 | −1.64 | 0.139 & | 0.38, 1.18 | ||||
| Year of publication | 15 | 84.87% | 16.62% | 0.96 | 0.02 | −1.74 | 0.105 | 0.92, 1.01 |
| Sample size | 15 | 81.47% | 12.78% | 1.00 | 0.00 | −1.58 | 0.139 | 0.99, 1.00 |
| Quality of studies | 15 | 82.38% | 20.13% | 0.78 | 0.10 | −1.92 | 0.078 | 0.60, 1.03 |
| Average age of patients | 10 | 65.85% | 55.42% | 0.97 | 0.01 | −2.73 | 0.026 | 0.95, 1.00 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pan, Y.; Liu, Y.; Guo, H.; Jabir, M.S.; Liu, X.; Cui, W.; Li, D. Associations between Folate and Vitamin B12 Levels and Inflammatory Bowel Disease: A Meta-Analysis. Nutrients 2017, 9, 382. https://doi.org/10.3390/nu9040382
Pan Y, Liu Y, Guo H, Jabir MS, Liu X, Cui W, Li D. Associations between Folate and Vitamin B12 Levels and Inflammatory Bowel Disease: A Meta-Analysis. Nutrients. 2017; 9(4):382. https://doi.org/10.3390/nu9040382
Chicago/Turabian StylePan, Yun, Ya Liu, Haizhuo Guo, Majid Sakhi Jabir, Xuanchen Liu, Weiwei Cui, and Dong Li. 2017. "Associations between Folate and Vitamin B12 Levels and Inflammatory Bowel Disease: A Meta-Analysis" Nutrients 9, no. 4: 382. https://doi.org/10.3390/nu9040382
APA StylePan, Y., Liu, Y., Guo, H., Jabir, M. S., Liu, X., Cui, W., & Li, D. (2017). Associations between Folate and Vitamin B12 Levels and Inflammatory Bowel Disease: A Meta-Analysis. Nutrients, 9(4), 382. https://doi.org/10.3390/nu9040382