Comparison of Prognostic Impact between the Child-Pugh Score and Skeletal Muscle Mass for Patients with Liver Cirrhosis

Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Statistical Analyses
3. Results
3.1. Baseline Characteristics
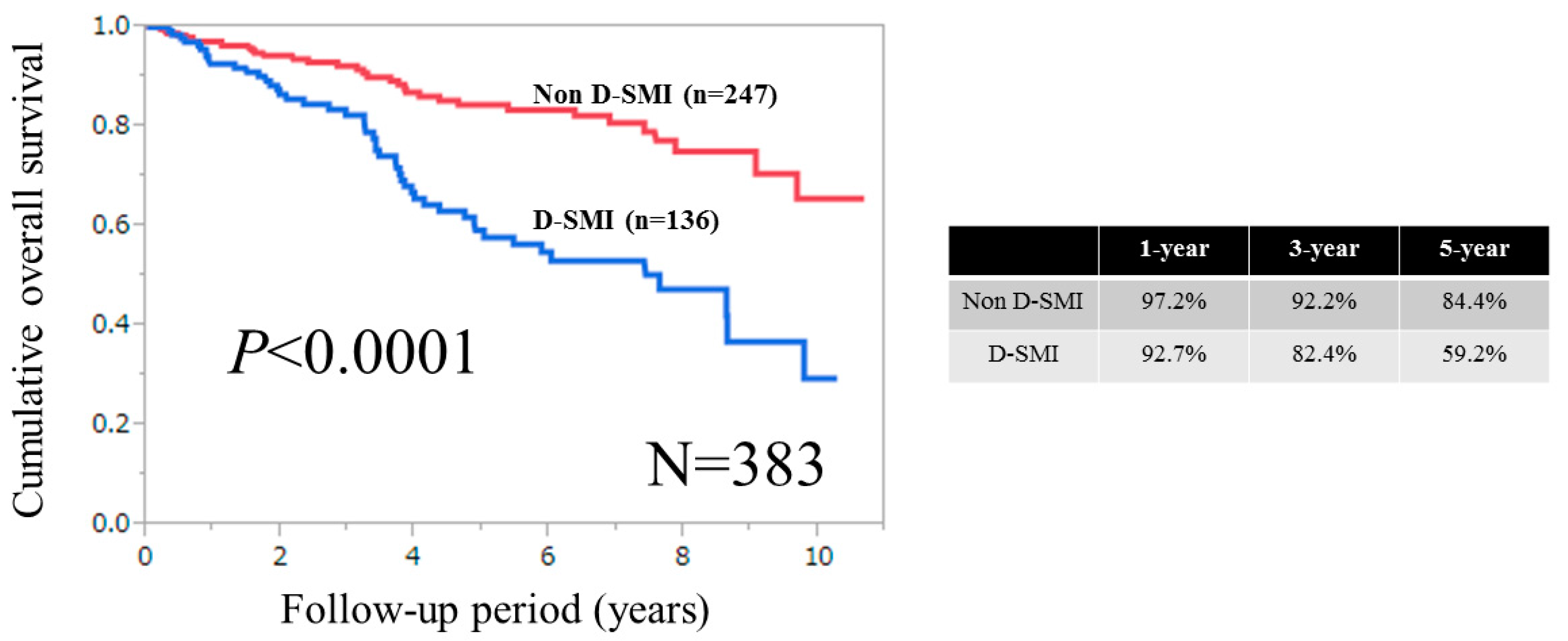
3.2. Cumulative OS Rates for the Entire Cohort, Male and Female According to SMI
3.3. Causes for Death for Males and Females
3.4. Univariate and Multivariate Analyses of Parameters Contributing to OS for Males
3.5. Univariate and Multivariate Analyses of Parameters Contributing to OS for Females
3.6. Time-Dependent ROC Analyses for OS in Males
3.7. Time-Dependent ROC Analyses for OS in Females
3.8. Time-Dependent ROC Analyses for OS in Male Patients with Child-Pugh A
3.9. Time-Dependent ROC Analyses for OS in Female Patients with Child-Pugh A
3.10. Time-Dependent ROC Analyses for OS in Male Patients with Child-Pugh B or C
3.11. Time-Dependent ROC Analyses for OS in Female Patients with Child-Pugh B or C
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
References
- Cheung, K.; Lee, S.S.; Raman, M. Prevalence and mechanisms of malnutrition in patients with advanced liver disease, and nutrition management strategies. Clin. Gastroenterol. Hepatol. 2012, 10, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Charlton, M.R. Branched-chain amino acid enriched supplements as therapy for liver disease. J. Nutr. 2006, 136 (Suppl. 1), 295S–298S. [Google Scholar] [CrossRef]
- Kawaguchi, T.; Izumi, N.; Charlton, M.R.; Sata, M. Branched-chain amino acids as pharmacological nutrients in chronic liver disease. Hepatology 2011, 54, 1063–1070. [Google Scholar] [CrossRef] [PubMed]
- Fukui, H.; Saito, H.; Ueno, Y.; Uto, H.; Obara, K.; Sakaida, I.; Shibuya, A.; Seike, M.; Nagoshi, S.; Segawa, M.; et al. Evidence-based clinical practice guidelines for liver cirrhosis 2015. J. Gastroenterol. 2016, 51, 629–650. [Google Scholar] [CrossRef] [PubMed]
- Kamath, P.S.; Wiesner, R.H.; Malinchoc, M.; Kremers, W.; Therneau, T.M.; Kosberg, C.L.; D’Amico, G.; Dickson, E.R.; Kim, W.R. A model to predict survival in patients with end-stage liver disease. Hepatology 2001, 33, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.R.; Biggins, S.W.; Kremers, W.K.; Wiesner, R.H.; Kamath, P.S.; Benson, J.T.; Edwards, E.; Therneau, T.M. Hyponatremia and mortality among patients on the liver-transplant waiting list. N. Engl. J. Med. 2008, 359, 1018–1026. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, G.; Garcia-Tsao, G.; Pagliaro, L. Natural history and prognostic indicators of survival in cirrhosis: A systematic review of 118 studies. J. Hepatol. 2006, 44, 217–231. [Google Scholar] [CrossRef] [PubMed]
- Cholongitas, E.; Papatheodoridis, G.V.; Vangeli, M.; Terreni, N.; Patch, D.; Burroughs, A.K. Systematic review: The model for end-stage liver disease—Should it replace Child-Pugh’s classification for assessing prognosis in cirrhosis? Aliment. Pharmacol. Ther. 2005, 22, 1079–1089. [Google Scholar] [CrossRef] [PubMed]
- Botta, F.; Giannini, E.; Romagnoli, P.; Fasoli, A.; Malfatti, F.; Chiarbonello, B.; Testa, E.; Risso, D.; Colla, G.; Testa, R. MELD scoring system is useful for predicting prognosis in patients with liver cirrhosis and is correlated with residual liver function: A European study. Gut 2003, 52, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Periyalwar, P.; Dasarathy, S. Malnutrition in cirrhosis: Contribution and consequences of sarcopenia on metabolic and clinical responses. Clin. Liver Dis. 2012, 16, 95–131. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Landi, F.; Schneider, S.M.; Zúñiga, C.; Arai, H.; Boirie, Y.; Chen, L.K.; Fielding, R.A.; Martin, F.C.; Michel, J.P.; et al. Prevalence of and interventions for sarcopenia in ageing adults: A systematic review. Report of the International Sarcopenia Initiative (EWGSOP and IWGS). Age Ageing 2014, 43, 748–759. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, M.; Gow, P.J.; Grossmann, M.; Angus, P.W. Review article: Sarcopenia in cirrhosis—Aetiology, implications and potential therapeutic interventions. Aliment. Pharmacol. Ther. 2016, 43, 765–777. [Google Scholar] [CrossRef] [PubMed]
- Hanai, T.; Shiraki, M.; Nishimura, K.; Ohnishi, S.; Imai, K.; Suetsugu, A.; Takai, K.; Shimizu, M.; Moriwaki, H. Sarcopenia impairs prognosis of patients with liver cirrhosis. Nutrition 2015, 31, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Shiraki, M.; Hiramatsu, A.; Moriya, K.; Hino, K.; Nishiguchi, S. JSH guidelines for sarcopenia in liver disease (first edition): Recommendation from the working group for creation of sarcopenia assessment criteria in the JSH. Hepatol. Res. 2016, 46, 951–963. [Google Scholar] [CrossRef] [PubMed]
- Santilli, V.; Bernetti, A.; Mangone, M.; Paoloni, M. Clinical definition of sarcopenia. Clin. Cases Miner. Bone Metab. 2014, 11, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Nardelli, S.; Lattanzi, B.; Torrisi, S.; Greco, F.; Farcomeni, A.; Gioia, S.; Merli, M.; Riggio, O. Sarcopenia is Risk Factor for Development of Hepatic Encephalopathy After Transjugular Intrahepatic Portosysthemic Shunt Placement. Clin. Gastroenterol. Hepatol. 2017, 15, 934–936. [Google Scholar] [CrossRef] [PubMed]
- Itoh, S.; Shirabe, K.; Matsumoto, Y.; Yoshiya, S.; Muto, J.; Harimoto, N.; Yamashita, Y.; Ikegami, T.; Yoshizumi, T.; Nishie, A.; et al. Effect of body composition on outcomes after hepatic resection for hepatocellular carcinoma. Ann. Surg. Oncol. 2014, 21, 3063–3068. [Google Scholar] [CrossRef] [PubMed]
- Carrara, G.; Pecorelli, N.; De Cobelli, F.; Cristel, G.; Damascelli, A.; Beretta, L.; Braga, M. Preoperative sarcopenia determinants in pancreatic cancer patients. Clin. Nutr. 2016. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, N.; Nakagawa, H.; Kudo, Y.; Tateishi, R.; Taguri, M.; Watadani, T.; Nakagomi, R.; Kondo, M.; Nakatsuka, T.; Minami, T.; et al. Sarcopenia, intramuscular fat deposition, and visceral adiposity independently predict the outcomes of hepatocellular carcinoma. J. Hepatol. 2015, 63, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, C.L.; Huang, D.D.; Pang, W.Y.; Zhou, C.J.; Wang, S.L.; Lou, N.; Ma, L.L.; Yu, Z.; Shen, X. Sarcopenia is an Independent Predictor of Severe Postoperative Complications and Long-Term Survival after Radical Gastrectomy for Gastric Cancer: Analysis from a Large-Scale Cohort. Medicine 2016, 95, e3164. [Google Scholar] [CrossRef] [PubMed]
- Harimoto, N.; Shirabe, K.; Yamashita, Y.I.; Ikegami, T.; Yoshizumi, T.; Soejima, Y.; Ikeda, T.; Maehara, Y.; Nishie, A.; Yamanaka, T. Sarcopenia as a predictor of prognosis in patients following hepatectomy for hepatocellular carcinoma. Br. J. Surg. 2013, 100, 1523–1530. [Google Scholar] [CrossRef] [PubMed]
- Antoun, S.; Borget, I.; Lanoy, E. Impact of sarcopenia on the prognosis and treatment toxicities in patients diagnosed with cancer. Curr. Opin. Support Palliat. Care 2013, 7, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Iritani, S.; Imai, K.; Takai, K.; Hanai, T.; Ideta, T.; Miyazaki, T.; Suetsugu, A.; Shiraki, M.; Shimizu, M.; Moriwaki, H. Skeletal muscle depletion is an independent prognostic factor for hepatocellular carcinoma. J. Gastroenterol. 2015, 50, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Kamachi, S.; Mizuta, T.; Otsuka, T.; Nakashita, S.; Ide, Y.; Miyoshi, A.; Kitahara, K.; Eguchi, Y.; Ozaki, I.; Anzai, K. Sarcopenia is a risk factor for the recurrence of hepatocellular carcinoma after curative treatment. Hepatol. Res. 2016, 46, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Okamoto, T.; Fujishita, T.; Katsura, M.; Akamine, T.; Takamori, S.; Morodomi, Y.; Tagawa, T.; Shoji, F.; Maehara, Y. Clinical implications of sarcopenia in patients undergoing complete resection for early non-small cell lung cancer. Lung Cancer 2016, 101, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Harimoto, N.; Yoshizumi, T.; Shimokawa, M.; Sakata, K.; Kimura, K.; Itoh, S.; Ikegami, T.; Ikeda, T.; Shirabe, K.; Maehara, Y. Sarcopenia is a poor prognostic factor following hepatic resection in patients 70 years of age and older with hepatocellular carcinoma. Hepatol. Res. 2016, 46, 1247–1255. [Google Scholar] [CrossRef] [PubMed]
- Hamaguchi, Y.; Kaido, T.; Okumura, S.; Kobayashi, A.; Hammad, A.; Tamai, Y.; Inagaki, N.; Uemoto, S. Proposal for new diagnostic criteria for low skeletal muscle mass based on computed tomography imaging in Asian adults. Nutrition 2016, 32, 1200–1205. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus Report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Dasarathy, S. Consilience in sarcopenia of cirrhosis. J. Cachexia Sarcopenia Muscle 2012, 3, 225–237. [Google Scholar] [CrossRef] [PubMed]
- Montano-Loza, A.J. Clinical relevance of sarcopenia in patients with cirrhosis. World J. Gastroenterol. 2014, 20, 8061–8071. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Zheng, R.Q.; Kim, S.R.; Okabe, Y.; Osaki, Y.; Iijima, H.; Itani, T.; Kasugai, H.; Kanematsu, M.; Ito, K.; et al. Diagnostic accuracy of imaging for liver cirrhosis compared to histologically proven liver cirrhosis. A multicenter collaborative study. Intervirology 2008, 51, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Zarski, J.P.; Sturm, N.; Guechot, J.; Paris, A.; Zafrani, E.S.; Asselah, T.; Boisson, R.C.; Bosson, J.L.; Guyader, D.; Renversez, J.C.; et al. Comparison of nine blood tests and transient elastography for liver fibrosis in chronic hepatitis C: The ANRS HCEP-23 study. J. Hepatol. 2012, 56, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Tsochatzis, E.A.; Gurusamy, K.S.; Ntaoula, S.; Cholongitas, E.; Davidson, B.R.; Burroughs, A.K. Elastography for the diagnosis of severity of fibrosis in chronic liver disease: A meta-analysis of diagnostic accuracy. J. Hepatol. 2011, 54, 650–659. [Google Scholar] [CrossRef] [PubMed]
- Kumada, H.; Okanoue, T.; Onji, M.; Moriwaki, H.; Izumi, N.; Tanaka, E.; Chayama, K.; Sakisaka, S.; Takehara, T.; Oketani, M.; et al. Guidelines for the treatment of chronic hepatitis and cirrhosis due to hepatitis C virus infection for the fiscal year 2008 in Japan. Hepatol. Res. 2010, 40, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Kappus, M.R.; Mendoza, M.S.; Nguyen, D.; Medici, V.; McClave, S.A. Sarcopenia in Patients with Chronic Liver Disease: Can It Be Altered by Diet and Exercise? Curr. Gastroenterol. Rep. 2016, 18, 43. [Google Scholar] [CrossRef] [PubMed]
- Heagerty, P.J.; Zheng, Y. Survival model predictive accuracy and ROC curves. Biometrics 2005, 61, 92–105. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver; European Organisation for Research and Treatment of Cancer. EASL-EORTC Clinical Practice guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2012, 56, 908–943. [Google Scholar]
- Kudo, M.; Izumi, N.; Kokudo, N.; Matsui, O.; Sakamoto, M.; Nakashima, O.; Kojiro, M.; Makuuchi, M.; HCC Expert Panel of Japan Society of Hepatology. Management of hepatocellular carcinoma in Japan: Consensus-Based Clinical Practice Guidelines proposed by the Japan Society of Hepatology (JSH) 2010 updated version. Dig Dis. 2011, 29, 339–364. [Google Scholar] [CrossRef] [PubMed]
- Asahina, Y.; Tsuchiya, K.; Tamaki, N.; Hirayama, I.; Tanaka, T.; Sato, M.; Yasui, Y.; Hosokawa, T.; Ueda, K.; Kuzuya, T.; et al. Effect of aging on risk for hepatocellular carcinoma in chronic hepatitis C virus infection. Hepatology 2010, 52, 518–527. [Google Scholar] [CrossRef] [PubMed]
- Osaki, Y.; Nishikawa, H. Treatment for hepatocellular carcinoma in Japan over the last three decades: Our experience and published work review. Hepatol Res. 2015, 45, 59–74. [Google Scholar] [CrossRef] [PubMed]
- Davuluri, G.; Krokowski, D.; Guan, B.J.; Kumar, A.; Thapaliya, S.; Singh, D.; Hatzoglou, M.; Dasarathy, S. Metabolic adaptation of skeletal muscle to hyperammonemia drives the beneficial effects of l-leucine in cirrhosis. J. Hepatol. 2016, 65, 929–937. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, M.; Grossmann, M.; Hoermann, R.; Angus, P.W.; Gow, P.J. Testosterone therapy increases muscle mass in men with cirrhosis and low testosterone: A randomised controlled trial. J. Hepatol. 2016, 65, 906–913. [Google Scholar] [CrossRef] [PubMed]
- Dasarathy, S. Cause and management of muscle wasting in chronic liver disease. Curr. Opin. Gastroenterol. 2016, 32, 159–165. [Google Scholar] [CrossRef] [PubMed]
- St-Onge, M.P. Relationship between body composition changes and changes in physical function and metabolic risk factors in aging. Curr. Opin. Clin. Nutr. Metab. Care 2005, 8, 523–528. [Google Scholar] [PubMed]
- Syddall, H.; Evandrou, M.; Cooper, C.; Sayer, A.A. Social inequalities in grip strength, physical function, and falls among community dwelling older men and women: Findings from the Hertfordshire Cohort Study. J. Aging Health 2009, 21, 913–939. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Number or Average ± SD | Male (n = 205) | Female (n = 178) | p Value (Male vs. Female) |
|---|---|---|---|---|
| Age (years) | 65.2 ± 10.3 | 64.1 ± 10.8 | 66.4 ± 9.5 | 0.0403 |
| Body mass index (kg/m2) | 23.3 ± 3.9 | 23.4 ± 3.8 | 23.2 ± 4.0 | 0.6028 |
| Skeletal muscle mass index (cm2/m2) | 6.7 ± 1.1 | 7.4 ± 0.9 | 6.0 ± 0.7 | <0.0001 |
| Causes of liver disease | 32/235/116 | 22/122/61 | 10/113/55 | 0.2043 |
| Hepatitis B/Hepatitis C/others | ||||
| Child-Pugh scores, 5/6/7/8/9/10/11 | 186/93/58/28/13/3/2 | 106/42/31/15/6/3/2 | 80/51/27/13/7/0/0 | 0.2587 |
| Total bilirubin (mg/dL) | 1.3 ± 1.1 | 1.3 ± 1.3 | 1.2 ± 0.7 | 0.2319 |
| Serum albumin (g/dL) | 3.7 ± 0.53 | 3.7 ± 0.54 | 3.6 ± 0.51 | 0.3897 |
| Prothrombin time (%) | 77.0 ± 13.8 | 77.5 ± 13.4 | 76.4 ± 14.2 | 0.4532 |
| Platelets (×104/mm3) | 10.6 ± 5.5 | 10.5 ± 5.3 | 10.7 ± 5.7 | 0.8093 |
| Serum sodium (mmol/L) | 139.7 ± 2.5 | 139.3 ± 2.5 | 140.2 ± 2.6 | 0.0004 |
| Serum creatinine (mg/dL) | 0.74 ± 0.51 | 0.84 ± 0.65 | 0.62 ± 0.22 | <0.0001 |
| Total cholesterol (mg/dL) | 154.0 ± 36.8 | 152.8 ± 35.4 | 155.2 ± 38.4 | 0.5250 |
| Triglyceride (mg/dL) | 90.5 ± 45.1 | 95.5 ± 53.0 | 84.8 ± 33.0 | 0.2144 |
| AST (IU/L) | 49.3 ± 34.8 | 49.4 ± 32.3 | 49.2 ± 37.5 | 0.9417 |
| ALT (IU/L) | 42.6 ± 38.9 | 43.9 ± 34.2 | 41.0 ± 43.7 | 0.0951 |
| Fasting blood glucose (mg/dL) | 110.9 ± 34.7 | 114.8 ± 39.9 | 106.4 ± 27.0 | 0.0101 |
| Ascites, yes/no | 44/339 | 25/180 | 19/159 | 0.7484 |
| (a) | |||
| Variables | Number of Each Category | Univariate | |
| p Value | |||
| Age (years) ≥ 70, yes/no | 91/114 | 0.0041 | |
| Cause of liver diseases, B/C/others | 22/122/61 | 0.2746 | |
| SMI ≥ 7.0 cm2/m2, yes/no | 127/78 | <0.0001 | |
| Child-Pugh score ≥ 6, yes/no | 99/106 | 0.0252 | |
| AST ≥ 29 IU/L, yes/no | 146/59 | 0.0150 | |
| ALT ≥ 47 IU/L, yes/no | 63/142 | 0.0407 | |
| Serum albumin ≥ 3.7 g/dL, yes/no | 113/92 | 0.0011 | |
| Total bilirubin ≥ 2.0 mg/dL, yes/no | 29/176 | 0.1539 | |
| Prothrombin time ≥ 77.1%, yes/no | 111/94 | 0.4521 | |
| Platelet count ≥ 9.4 × 104/mm3, yes/no | 101/104 | 0.2360 | |
| Total cholesterol ≥ 124 mg/dL, yes/no | 165/40 | 0.2398 | |
| Triglyceride ≥ 56 mg/dL, yes/no | 170/35 | 0.0649 | |
| Serum sodium ≥ 138 mmol/L, yes/no | 166/39 | 0.0133 | |
| Fasting blood glucose ≥ 97 mg/dL, yes/no | 145/60 | 0.4942 | |
| Serum creatinine ≥ 0.78 mg/dL, yes/no | 84/121 | 0.0088 | |
| Body mass index ≥ 23.4 kg/m2, yes/no | 91/114 | 0.0041 | |
| Ascites, yes/no | 25/180 | 0.0712 | |
| (b) | |||
| Variables | Multivariate Analysis | ||
| Hazard Ratio | 95% CI | p Value | |
| SMI (per one cm2/m2) | 0.571 | 0.416–0.777 | 0.0005 |
| AST (per one IU/L) | 1.005 | 0.987–1.022 | 0.5683 |
| ALT (per one IU/L) | 0.990 | 0.972–1.008 | 0.3002 |
| Child-Pugh score (per one point) | 1.270 | 1.020–1.520 | 0.0424 |
| Serum sodium (per one mmol/L) | 0.912 | 0.807–1.033 | 0.1481 |
| Serum creatinine (per one mg/dL) | 1.104 | 0.769–1.397 | 0.4914 |
| (a) | |||
| Variables | Number of Each Category | Univariate | |
| p value | |||
| Age (years) ≥ 77, yes/no | 22/156 | 0.0214 | |
| Cause of liver diseases, B/C/others | 10/113/55 | 0.5037 | |
| SMI ≥ 5.4 cm2/m2, yes/no | 139/39 | 0.0076 | |
| Child-Pugh score ≥ 6, yes/no | 98/80 | 0.0009 | |
| AST ≥ 80 IU/L, yes/no | 20/158 | 0.0544 | |
| ALT ≥ 58 IU/L, yes/no | 32/146 | 0.0104 | |
| Serum albumin ≥ 3.4 g/dL, yes/no | 117/61 | 0.0003 | |
| Total bilirubin ≥ 2.3 mg/dL, yes/no | 10/168 | 0.7607 | |
| Prothrombin time ≥ 73.7%, yes/no | 103/75 | 0.0355 | |
| Platelet count ≥ 9.7 ×104/mm3, yes/no | 92/86 | 0.0333 | |
| Total cholesterol ≥ 176 mg/dL, yes/no | 49/129 | 0.0558 | |
| Triglyceride ≥ 72 mg/dL, yes/no | 108/70 | 0.0011 | |
| Serum sodium ≥ 139 mmol/L, yes/no | 143/35 | 0.4064 | |
| Fasting blood glucose ≥ 89 mg/dL, yes/no | 142/36 | 0.2428 | |
| Serum creatinine ≥ 0.63 mg/dL, yes/no | 66/112 | 0.0137 | |
| Body mass index ≥ 23.4 kg/m2, yes/no | 78/100 | 0.0270 | |
| Ascites, yes/no | 19/159 | <0.0001 | |
| (b) | |||
| Variables | Multivariate Analysis | ||
| Hazard ratio | 95% CI | p Value | |
| Age (per one year) | 1.018 | 0.977–1.063 | 0.3998 |
| SMI (per one cm2/m2) | 0.450 | 0.270–0.731 | 0.0016 |
| ALT (per one IU/L) | 0.987 | 0.967–1.107 | 0.0506 |
| Platelet count (per one × 104/mm3) | 0.919 | 0.828–1.008 | 0.0943 |
| Child-Pugh score (per one point) | 1.938 | 1.400–2.690 | <0.0001 |
| Triglyceride (per one mg/dL) | 0.998 | 0.983–1.011 | 0.7760 |
| Serum creatinine (per one mg/dL) | 2.546 | 0.413–10.860 | 0.2545 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishikawa, H.; Enomoto, H.; Ishii, A.; Iwata, Y.; Miyamoto, Y.; Ishii, N.; Yuri, Y.; Hasegawa, K.; Nakano, C.; Nishimura, T.; et al. Comparison of Prognostic Impact between the Child-Pugh Score and Skeletal Muscle Mass for Patients with Liver Cirrhosis. Nutrients 2017, 9, 595. https://doi.org/10.3390/nu9060595
Nishikawa H, Enomoto H, Ishii A, Iwata Y, Miyamoto Y, Ishii N, Yuri Y, Hasegawa K, Nakano C, Nishimura T, et al. Comparison of Prognostic Impact between the Child-Pugh Score and Skeletal Muscle Mass for Patients with Liver Cirrhosis. Nutrients. 2017; 9(6):595. https://doi.org/10.3390/nu9060595
Chicago/Turabian StyleNishikawa, Hiroki, Hirayuki Enomoto, Akio Ishii, Yoshinori Iwata, Yuho Miyamoto, Noriko Ishii, Yukihisa Yuri, Kunihiro Hasegawa, Chikage Nakano, Takashi Nishimura, and et al. 2017. "Comparison of Prognostic Impact between the Child-Pugh Score and Skeletal Muscle Mass for Patients with Liver Cirrhosis" Nutrients 9, no. 6: 595. https://doi.org/10.3390/nu9060595
APA StyleNishikawa, H., Enomoto, H., Ishii, A., Iwata, Y., Miyamoto, Y., Ishii, N., Yuri, Y., Hasegawa, K., Nakano, C., Nishimura, T., Yoh, K., Aizawa, N., Sakai, Y., Ikeda, N., Takashima, T., Takata, R., Iijima, H., & Nishiguchi, S. (2017). Comparison of Prognostic Impact between the Child-Pugh Score and Skeletal Muscle Mass for Patients with Liver Cirrhosis. Nutrients, 9(6), 595. https://doi.org/10.3390/nu9060595