Despite Inflammation, Supplemented Essential Amino Acids May Improve Circulating Levels of Albumin and Haemoglobin in Patients after Hip Fractures



Abstract
:1. Introduction
2. Subjects and Methods
2.1. Population and Measures
- (1)
- Anthropometric measurements: body weight (kg) was determined using a mechanical weight lifter; height (m) was calculated from knee height [36]; body mass index (BMI) was calculated as kg/m2; although 70% of patients were able to stand up, we preferred to weigh them by mechanical lifter to avoid instability when they were on the base of the weighing scale.
- (2)
- After overnight fasting, at 7:00 a.m. blood samples were taken from peripheral veins to determine routine variables, which included the measurements of serum/blood protein concentrations (total protein-TP, Alb, prealbumin-preAlb, C-reactive protein (CRP)).
2.2. Nutritional Intake
2.3. Co-Morbidities
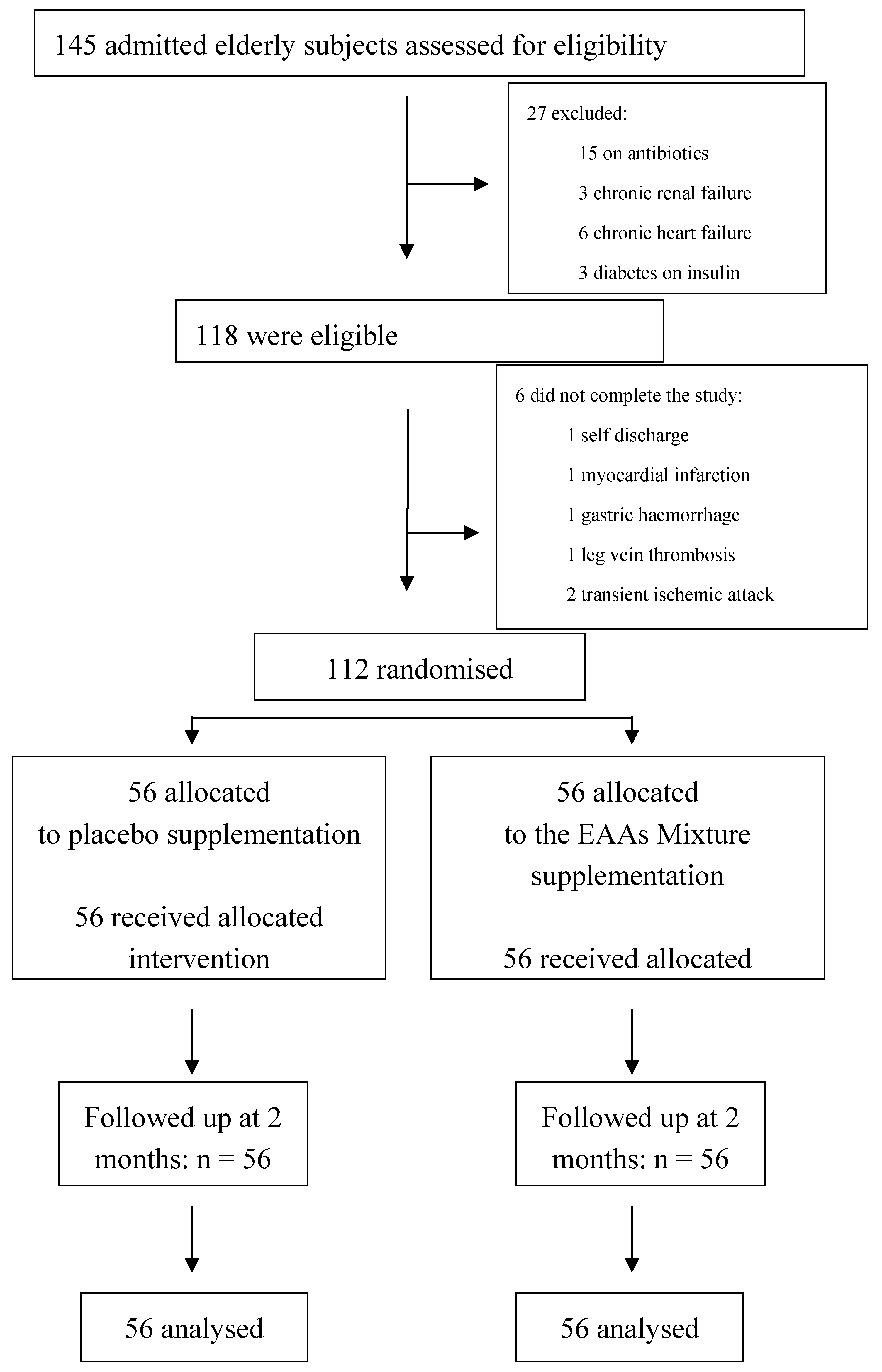
2.4. Patient Randomisation
2.5. A Rehabilitation Protocol
- Range of motion (ROM): a passive and assisted active mobilisation of the limb that had been operated on (15 min)
- Muscle strength:
- -
- isotonic and isometric exercises, neuromuscular facilitation of the sural triceps muscles (three sets of 10 repetitions; 15 min)
- -
- isotonic exercise and against resistance of: (1) abdominal trunk muscles to contrast the anteversion of the pelvis and (2) Gluteus maximus muscle to restore leg extension movement; (3) Gluteus medius and minimus muscles to keep the pelvis static and to be able to walk without oscillation (3 sets of 10 repetitions; 15 min)
- Assisted gait training with the use of walking sticks (10 min).
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Variable Changes during the Rehabilitation Phase
4. Discussion
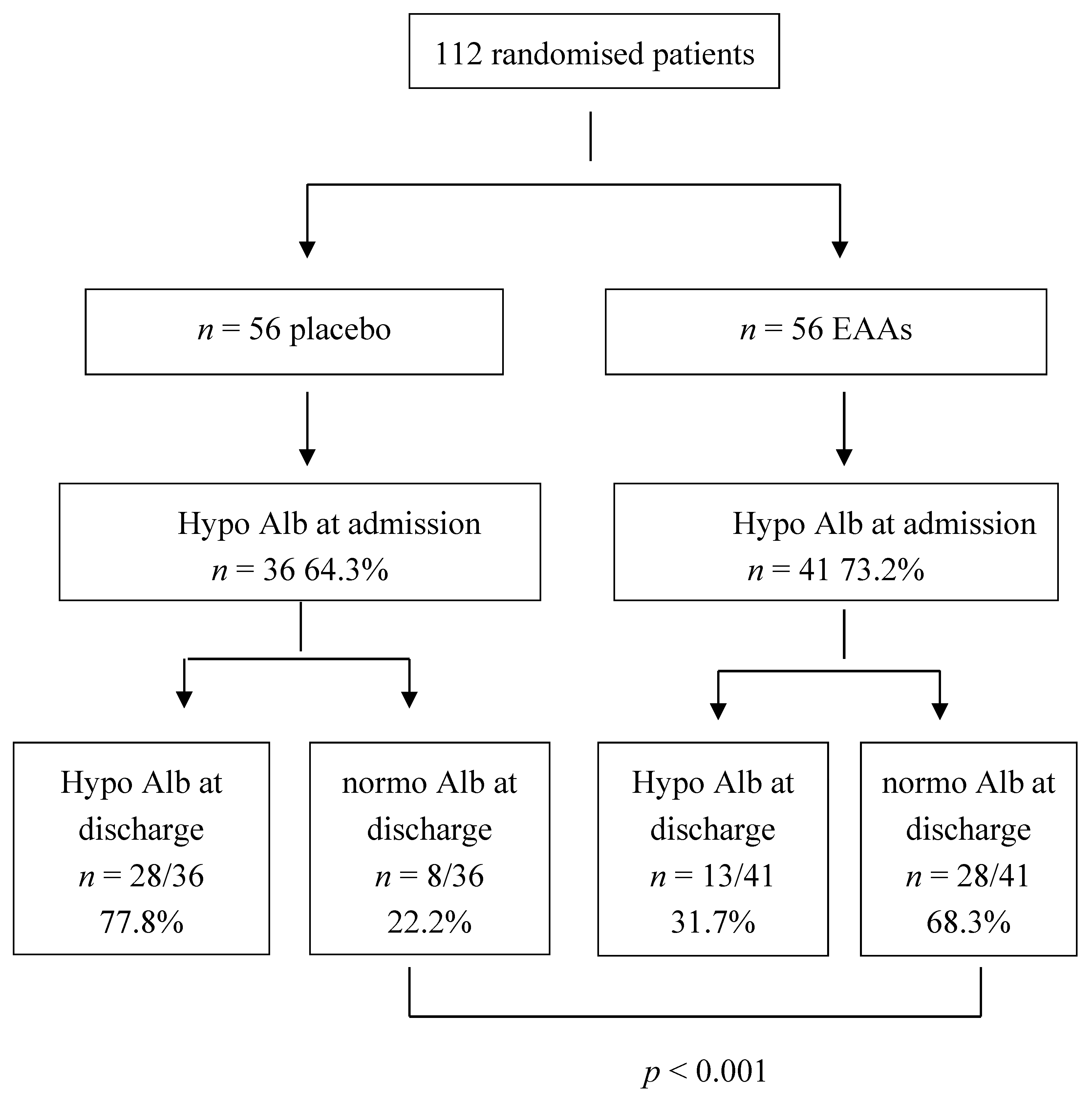
4.1. Baseline Circulating Proteins
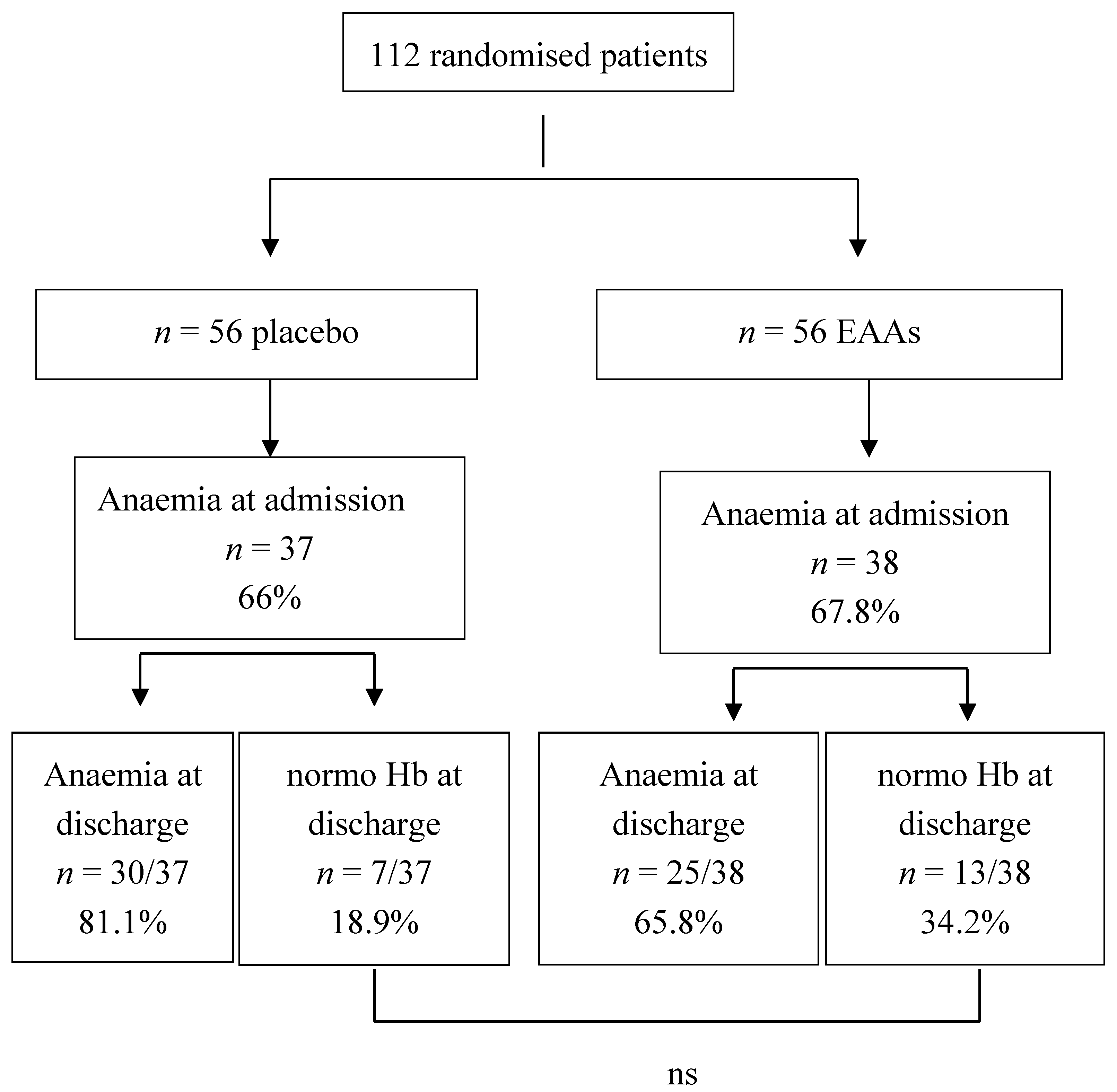
4.2. EAA-Associated Improvements in Alb and HB
5. Clinical Implications
6. Conclusions
7. Limitations
Author Contributions
Conflicts of Interest
References and Note
- Doweiko, J.P.; Nompleggi, D.J. The role of albumin in human physiology and pathophysiology, Part III: Albumin and disease states. JPEN 1991, 15, 476–483. [Google Scholar] [CrossRef] [PubMed]
- Visser, M.; Kritchevsky, S.B.; Newman, A.B.; Goodpaster, B.H.; Tylavsky, F.A.; Nevitt, M.C.; Harris, T.B. Lower serum albumin concentration and change in muscle mass: The health, aging and body composition study. Am. J. Clin. Nutr. 2005, 82, 531–537. [Google Scholar] [PubMed]
- Zuliani, G.; Romagnoni, F.; Volpato, S.; Soattin, L.; Leoci, V.; Bollini, M.C.; Buttarello, M.; Lotto, D.; Fellin, R. Nutritional parameters, body composition, and progression of disability in older disabled residents living in nursing homes. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, 212–216. [Google Scholar] [CrossRef]
- Corti, M.C.; Guralnik, J.M.; Salive, M.E.; Sorkin, J.D. Serum albumin level and physical disability as predictors of mortality in older persons. JAMA 1994, 272, 1036–1042. [Google Scholar] [CrossRef] [PubMed]
- Mendez, C.M.; McClain, C.J.; Marsano, L.S. Albumin therapy in clinical practice. Nutr. Clin. Pract. 2005, 20, 314–320. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.F.; Moxness, K.; Meister, J.; Burritt, M.F. The sensitivity and specificity of nutrition-related variables in relationship to the duration of hospital stay and the rate of complications. Mayo Clin. Proc. 1984, 59, 477–483. [Google Scholar] [CrossRef]
- Rich, M.W.; Keller, A.J.; Schechtman, K.B.; Marshall, W.G.; Kouchoukos, N.T. Increased complications and prolonged hospital stay in elderly cardiac surgical patients with low serum albumin. Am. J. Cardiol. 1989, 63, 714–718. [Google Scholar] [CrossRef]
- Sahyoun, N.R.; Jacques, P.F.; Dallal, G.; Russell, R.M. Use of albumin as a predictor of mortality in community dwelling and institutionalized elderly populations. J. Clin. Epidemiol. 1996, 49, 981–988. [Google Scholar] [CrossRef]
- Mizrahi, E.H.; Fleissig, Y.; Arad, M.; Blumstein, T.; Adunsky, A. Admission albumin levels and functional outcome of elderly hip fracture patients: Is it that important? Aging Clin. Exp. Res. 2007, 19, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Aquilani, R.; Boselli, M.; Baiardi, P.; Pasini, E.; Iadarola, P.; Verri, M.; Viglio, S.; Condini, A.; Boschi, F. Is stroke rehabilitation a metabolic problem? Brain Inj. 2014, 28, 161–173. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Penninx, B.W.; Lauretani, F.; Russo, C.R.; Carter, C.; Bandinelli, S.; Atkinson, H.; Onder, G.; Pahor, M.; Ferrucci, L. Hemoglobin levels and skeletal muscle: Results from the In CHIANTI study. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Penninx, B.W.; Guralnik, J.M.; Onder, G.; Ferrucci, L.; Wallace, R.B.; Pahor, M. Anemia and decline in physical performance among older persons. Am. J. Med. 2003, 115, 104–110. [Google Scholar] [CrossRef]
- Fuchs, Z.; Blumstein, T.; Novikov, I.; Walter-Ginzburg, A.; Lyanders, M.; Gindin, J.; Habot, B.; Modan, B. Morbidity, comorbidity, and their association with disability among community-dwelling oldest-old in Israel. J. Gerontol. A Biol. Sci. Med. Sci. 1998, 53, 447–455. [Google Scholar] [CrossRef]
- Penninx, B.W.; Pahor, M.; Cesari, M.; Corsi, A.M.; Woodman, R.C.; Bandinelli, S.; Guralnik, J.M.; Ferrucci, L. Anemia is associated with disability and decreased physical performance and muscle strength in the elderly. J. Am. Geriatr. Soc. 2004, 52, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Boogaerts, M.; Coiffier, B.; Kainz, C.; Epoetin Beta QOL Working Group. Impact of epoetin beta on quality of life in patients with malignant disease. Br. J. Cancer 2003, 88, 988–995. [Google Scholar] [CrossRef] [PubMed]
- Izaks, G.J.; Westendorp, R.G.; Knook, D.L. The definition of anemia in older persons. JAMA 1999, 281, 1714–1717. [Google Scholar] [CrossRef] [PubMed]
- Makipour, S.; Kanapuru, B.; Ershler, W.B. Unexplained anemia in the elderly. Semin. Hematol. 2008, 45, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Gruson, K.I.; Aharonoff, G.B.; Egol, K.A.; Zuckerman, J.D.; Koval, K.J. The relationship between admission hemoglobin level and outcome after hip fracture. J. Orthop. Trauma 2002, 16, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Halm, E.A.; Wang, J.J.; Boockvar, K.; Penrod, J.; Silberzweig, S.B.; Magaziner, J.; Koval, K.J.; Siu, A.L. The effect of perioperative anemia on clinical and functional outcomes in patients with hip fracture. J. Orthop. Trauma 2004, 18, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Foss, N.B.; Kristensen, M.T.; Kehlet, H. Anaemia impedes functional mobility after hip fracture surgery. Age Ageing 2008, 37, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Foss, N.B.; Kristensen, M.T.; Kehlet, H. Prediction of postoperative morbidity, mortality and rehabilitation in hip fracture patients: The cumulated ambulation score. Clin. Rehabil. 2006, 20, 701–708. [Google Scholar] [CrossRef] [PubMed]
- Salive, M.E.; Cornoni-Huntley, J.; Phillips, C.L.; Guralnik, J.M.; Cohen, H.J.; Ostfeld, A.M.; Wallace, R.B. Serum albumin in older persons: Relationship with age and health status. J. Clin. Epidemiol. 1992, 45, 213–221. [Google Scholar] [CrossRef]
- Adunsky, A.; Arad, M.; Blumstein, T.; Weitzman, A.; Mizrahi, E.H. Discharge hemoglobin and functional outcome of elderly hip fractured patients undergoing rehabilitation. Eur. J. Phys. Rehabil. Med. 2008, 417–422. [Google Scholar]
- Su, H.; Aharonoff, G.B.; Zuckerman, J.D.; Egol, K.A.; Koval, K.J. The relation between discharge hemoglobin and outcome after hip fracture. Am. J. Orthop. 2004, 33, 576–580. [Google Scholar] [PubMed]
- Culleton, B.F.; Manns, B.J.; Zhang, J.; Tonelli, M.; Klarenbach, S.; Hemmelgarn, B.R. Impact of anemia on hospitalization and mortality in older adults. Blood 2006, 107, 3841–3846. [Google Scholar] [CrossRef] [PubMed]
- Ferrucci, L.; Balducci, L. Anemia of aging: The role of chronic inflammation and cancer. Semin. Hematol. 2008, 45, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Atti, A.R.; Palmer, K.; Volpato, S.; Zuliani, G.; Winblad, B.; Fratiglioni, L. Anaemia increases the risk of dementia in cognitively intact elderly. Neurobiol. Aging 2006, 27, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Penninx, B.W.; Pluijm, S.M.; Lips, P.; Woodman, R.; Miedema, K.; Guralnik, J.M.; Deeg, D.J. Late-life anemia is associated with increased risk of recurrent falls. J. Am. Geriatr. Soc. 2005, 53, 2106–2111. [Google Scholar] [CrossRef] [PubMed]
- Patterson, B.M.; Cornell, C.N.; Carbone, B.; Levine, B.; Chapman, D. Protein depletion and metabolic stress in elderly patients who have a fracture of the hip. J. Bone Jt. Surg. Am. 1992, 74, 251–260. [Google Scholar] [CrossRef]
- Liu, Z.; Long, W.; Fryburg, D.A.; Barrett, E.J. The regulation of body and skeletal muscle protein metabolism by hormones and amino acids. J. Nutr. 2006, 136, 212S–217S. [Google Scholar] [PubMed]
- Rittig, N.; Thomsen, H.H.; Bach, E.; Jørgensen, J.O.; Møller, N. Hormone and cytokine responses to repeated endotoxin exposures-no evidence of endotoxin tolerance after 5 weeks in humans. Shock 2015, 44, 32–35. [Google Scholar] [CrossRef] [PubMed]
- Dal Negro, R.W.; Aquilani, R.; Bertacco, S.; Boschi, F.; Micheletto, C.; Tognella, S. Comprehensive effects of supplemented essential amino acids in patients with severe COPD and sarcopenia. Monaldi Arch. Chest Dis. 2010, 73, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Rondanelli, M.; Opizzi, A.; Antoniello, N.; Boschi, F.; Iadarola, P.; Pasini, E.; Aquilani, R.; Dioguardi, F.S. Effect of essential amino acid supplementation on quality of life, amino acid profile and strength in institutionalized elderly patients. Clin. Nutr. 2011, 30, 571–577. [Google Scholar] [CrossRef] [PubMed]
- Bolasco, P.; Cupisti, A.; Locatelli, F.; Caria, S.; Kalantar-Zadeh, K. Dietary management of incremental transition to dialysis therapy: Once-weekly hemodialysis combined with low-protein diet. J. Ren. Nutr. 2016, 26, 352–359. [Google Scholar] [CrossRef] [PubMed]
- Aquilani, R.; Zuccarelli, G.C.; Dioguardi, F.S.; Baiardi, P.; Frustaglia, A.; Rutili, C.; Comi, E.; Catani, M.; Iadarola, P.; Viglio, S.; et al. Effects of oral amino acid supplementation on long-term-care-acquired infections in elderly patients. Arch. Gerontol. Geriatr. 2011, 52, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Chumlea, W.C.; Roche, A.F.; Steinbaugh, M.L. Estimating stature from knee height for persons 60 to 90 years of age. J. Am. Geriatr. Soc. 1985, 33, 116–120. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Aquilani, R.; Opasich, C.; Gualco, A.; Verri, M.; Testa, A.; Pasini, E.; Viglio, S.; Iadarola, P.; Pastoris, O.; Dossena, M.; et al. Adequate energy-protein intake is not enough to improve nutritional and metabolic status in muscle-depleted patients with chronic heart failure. Eur. J. Heart Fail. 2008, 10, 1127–1135. [Google Scholar] [CrossRef] [PubMed]
- Quarta Revisione dei livelli di Assunzione di Riferimento di Nutrienti (LARN) e di Energia per la popolazione italiana. 2014.
- Soeters, P.B.; Grimble, R.F. Dangers, and benefits of the cytokine mediated response to injury and infection. Clin. Nutr. 2009, 28, 583–596. [Google Scholar] [CrossRef] [PubMed]
- Margarson, M.P.; Soni, N. Serum albumin: Touchstone or totem? Anaesthesia 1998, 53, 789–803. [Google Scholar] [CrossRef] [PubMed]
- Rothschild, M.A.; Oratz, M.; Schreiber, S.S. Serum albumin. Hepatology 1988, 8, 385–401. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, R.N.; Koehler, K.M.; Romero, L.; Garry, P.J. Serum albumin is associated with skeletal muscle in elderly men and women. Am. J. Clin. Nutr. 1996, 64, 552–558. [Google Scholar] [PubMed]
- Bastow, M.D.; Rawlings, J.; Allison, S.P. Benefits of supplementary tube feeding after fractured neck of femur: A randomised controlled trial. Br. Med. J. Clin. Res. Ed. 1983, 287, 1589–1592. [Google Scholar] [CrossRef] [PubMed]
- Kendall, S.J.; Weir, J.; Aspinall, R.; Henderson, D.; Rosson, J. Erythrocyte transfusion causes immunosuppression after total hip replacement. Clin. Orthop. Relat. Res. 2000, 381, 145–155. [Google Scholar] [CrossRef]
- Theusinger, O.M.; Spahn, D.R. Perioperative blood conservation strategies for major spine surgery. Best Pract. Res. Clin. Anaesthesiol. 2016, 30, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Kimball, S.R.; Fabian, J.R.; Pavitt, G.D.; Hinnebusch, A.G.; Jefferson, L.S. Regulation of guanine nucleotide exchange through phosphorylation of eukaryotic initiation factor eIF2alpha. Role of the alpha and delta-subunits of eiF2b. J. Biol. Chem. 1998, 273, 12841–12845. [Google Scholar] [PubMed]
- Wang, X.; Campbell, L.E.; Miller, C.M.; Proud, C.G. Amino acid availability regulates p70S6 kinase and multiple translation factors. Biochem. J. 1998, 334, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Fafournoux, P.; Bruhat, A.; Jousse, C. Amino acid regulation of gene expression. Biochem. J. 2000, 351, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Dillon, E.L.; Sheffield-Moore, M.; Paddon-Jones, D.; Gilkison, C.; Sanford, A.P.; Casperson, S.L.; Jiang, J.; Chinkes, D.L.; Urban, R.J. Amino acid supplementation increases lean body mass, basal muscle protein synthesis, and insulin-like growth factor-I expression in older women. J. Clin. Endocrinol. Metab. 2009, 94, 1630–1637. [Google Scholar] [CrossRef] [PubMed]
- May, P.E.; Barber, A.; D’Olimpio, J.T.; Hourihane, A.; Abumrad, N.N. Reversal of cancer-related wasting using oral supplementation with a combination of beta-hydroxy-beta-methylbutyrate, arginine, and glutamine. Am. J. Surg. 2002, 183, 471–479. [Google Scholar] [CrossRef]
- Smith, H.J.; Mukerji, P.; Tisdale, M.J. Attenuation of proteasome-induced proteolysis in skeletal muscle by {beta}-hydroxy-{beta}-methylbutyrate in cancer-induced muscle loss. Cancer Res. 2005, 65, 277–283. [Google Scholar] [PubMed]
- Rothschild, M.A.; Oratz, M.; Mongelli, J.; Fishman, L.; Schreiber, S.S. Amino acid regulation of albumin synthesis. J. Nutr. 1969, 98, 395–403. [Google Scholar] [PubMed]
- Boselli, M.; Aquilani, R.; Baiardi, P.; Dioguardi, F.S.; Guarnaschelli, C.; Achilli, M.P.; Arrigoni, N.; Iadarola, P.; Verri, M.; Viglio, S.; et al. Supplementation of essential amino acids may reduce the occurrence of infections in rehabilitation patients with brain injury. Nutr. Clin. Pract. 2012, 27, 99–113. [Google Scholar] [CrossRef] [PubMed]
- Mizrahi, E.H.; Fleissig, Y.; Arad, M.; Blumstein, T.; Adunsky, A. Rehabilitation outcome of hip fracture patients: The importance of a positive albumin gain. Arch. Gerontol. Geriatr. 2008, 47, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Paddon-Jones, D.; Short, K.R.; Campbell, W.W.; Volpi, E.; Wolfe, R.R. Role of dietary protein in the sarcopenia of aging. Am. J. Clin. Nutr. 2008, 87, 1562S–1566S. [Google Scholar] [PubMed]
- Paddon-Jones, D.; Wolfe, R.R.; Ferrando, A.A. Amino acid supplementation for reversing bed rest and steroid myopathies. J. Nutr. 2005, 135, 1809–1812. [Google Scholar]
- Solerte, S.B.; Gazzaruso, C.; Bonacasa, R.; Rondanelli, M.; Zamboni, M.; Basso, C.; Locatelli, E.; Schifino, N.; Giustina, A.; Fioravanti, M. Nutritional supplements with oral amino acid mixtures increases whole-body lean mass and insulin sensitivity in elderly subjects with sarcopenia. Am. J. Cardiol. 2008, 101, 69E–77E. [Google Scholar] [CrossRef] [PubMed]
- Gaskill, P.; Kabat, D. Unexpectedly large size of globin messenger ribonucleic acid. Proc. Natl. Acad. Sci. USA 1971, 68, 72–75. [Google Scholar] [CrossRef] [PubMed]
- Rittig, N.; Bach, E.; Thomsen, H.H.; Johannsen, M.; Jørgensen, J.O.; Richelsen, B.; Jessen, N.; Møller, N. Amino acid supplementation is anabolic during the acute phase of endotoxin-induced inflammation: A human randomized crossover trial. Clin. Nutr. 2016, 35, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, L.C.; Chien, S.L.; Huang, M.S.; Tseng, H.F.; Chang, C.K. Anti-inflammatory and anticatabolic effects of short-term beta-hydroxy-beta-methylbutyrate supplementation on chronic obstructive pulmonary disease patients in intensive care unit. Asia Pac. J. Clin. Nutr. 2006, 15, 544–550. [Google Scholar] [PubMed]
- Baldissarro, E.; Aquilani, R.; Boschi, F.; Baiardi, P.; Iadarola, P.; Fumagalli, M.; Pasini, E.; Verri, M.; Dossena, M.; Gambino, A.; et al. The hip functional retrieval after elective surgery may be enhanced by supplemented essential amino acids. Biomed. Res. Int. 2016, 2016, 931–952. [Google Scholar] [CrossRef] [PubMed]
- Vidal-Casariego, A.; Calleja-Fernández, A.; de Urbina-González, J.J.; Cano-Rodríguez, I.; Cordido, F.; Ballesteros-Pomar, M.D. Efficacy of glutamine in the prevention of acute radiation enteritis: A randomized controlled trial. JPEN 2014, 38, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Klimberg, V.S.; Souba, W.W.; Dolson, D.J.; Salloum, R.M.; Hautamaki, R.D.; Plumley, D.A.; Mendenhall, W.M.; Bova, F.J.; Khan, S.R.; Hackett, R.L. Prophylactic glutamine protects the intestinal mucosa from radiation injury. Cancer 1990, 66, 62–68. [Google Scholar] [CrossRef]
- Bellows, C.F.; Jaffe, B.M. Glutamine is essential for nitric oxide synthesis by murine macrophages. J. Surg. Res. 1999, 86, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Shinozaki, M.; Saito, H.; Muto, T. Excess glutamine exacerbates trinitrobenzenesulfonic acid-induced colitis in rats. Dis. Colon Rectum 1997, 40, 59–63. [Google Scholar] [CrossRef]
- Ferrucci, L.; Guralnik, J.M.; Bandinelli, S.; Semba, R.D.; Lauretani, F.; Corsi, A.; Ruggiero, C.; Ershler, W.B.; Longo, D.L. Unexplained anaemia in older persons is characterised by low erythropoietin and low levels of pro-inflammatory markers. Br. J. Haematol. 2007, 136, 849–855. [Google Scholar] [CrossRef] [PubMed]
- Ferrucci, L.; Guralnik, J.M.; Woodman, R.C.; Bandinelli, S.; Lauretani, F.; Corsi, A.M.; Chaves, P.H.; Ershler, W.B.; Longo, D.L. Proinflammatory state and circulating erythropoietin in persons with and without anemia. Am. J. Med. 2005, 118, 1288. [Google Scholar] [CrossRef] [PubMed]
- Chahal, H.S.; Drake, W.M. The endocrine system and ageing. J. Pathol. 2007, 211, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Bellelli, G.; Magnifico, F.; Trabucchi, M. Outcomes at 12 months in a population of elderly patients discharged from a rehabilitation unit. J. Am. Med. Dir. Assoc. 2008, 9, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Dybkaer, R.; Lauritzen, M.; Krakauer, R. Relative reference values for clinical chemical and haematological quantities in ‘healthy’ elderly people. Acta Med. Scand. 1981, 209, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.L. Anemia in the elderly. Am. Fam. Physician 2000, 62, 1565–1572. [Google Scholar] [PubMed]
- Dodd, S.L.; Powers, S.K.; Brooks, E.; Crawford, M.P. Effects of reduced O2 delivery with anemia, hypoxia, or ischemia on peak VO2 and force in skeletal muscle. J. Appl. Physiol. 1993, 74, 186–191. [Google Scholar] [PubMed]
- Olivares, M.; Hertrampf, E.; Capurro, M.T.; Wegner, D. Prevalence of anemia in elderly subjects living at home: Role of micronutrient deficiency and inflammation. Eur. J. Clin. Nutr. 2000, 54, 834–839. [Google Scholar] [CrossRef] [PubMed]
- Hepple, R.T. Skeletal muscle: Microcirculatory adaptation to metabolic demand. Med. Sci. Sports Exerc. 2000, 32, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Anker, S.D.; Ponikowski, P.P.; Clark, A.L.; Leyva, F.; Rauchhaus, M.; Kemp, M.; Teixeira, M.M.; Hellewell, P.G.; Hooper, J.; Poole-Wilson, P.A.; et al. Cytokines and neurohormones relating to body composition alterations in the wasting syndrome of chronic heart failure. Eur. Heart J. 1999, 20, 683–693. [Google Scholar] [CrossRef] [PubMed]
- García-Martínez, C.; López-Soriano, F.J.; Argilés, J.M. Acute treatment with tumour necrosis factor-alpha induces changes in protein metabolism in rat skeletal muscle. Mol. Cell. Biochem. 1993, 125, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Deveci, D.; Marshall, J.M.; Egginton, S. Relationship between capillary angiogenesis, fiber type, and fiber size in chronic systemic hypoxia. Am. J. Physiol. Heart Circ. Physiol. 2001, 281, 241–252. [Google Scholar]
- Kasuya, H.; Kawashima, A.; Namiki, K.; Shimizu, T.; Takakura, K. Metabolic profiles of patients with subarachnoid hemorrhage treated by early surgery. Neurosurgery 1998, 42, 1268–1274. [Google Scholar] [CrossRef] [PubMed]
- Li, J.J.; Fang, C.H. C-reactive protein is not only an inflammatory marker but also a direct cause of cardiovascular diseases. Med. Hypotheses. 2004, 62, 499–506. [Google Scholar] [CrossRef] [PubMed]
- De Maat, M.P.; Trion, A. C-reactive protein as a risk factor versus risk marker. Curr. Opin. Lipidol. 2004, 15, 651–657. [Google Scholar]
- Von Haehling, S.; Steinbeck, L.; Doehner, W.; Springer, J.; Anker, S.D. Muscle wasting in heart failure: An overview. Int. J. Biochem. Cell Biol. 2013, 45, 2257–2265. [Google Scholar] [CrossRef] [PubMed]
- Mastorakos, G.; Chrousos, G.P.; Weber, J.S. Recombinant interleukin-6 activates the hypothalamic-pituitary-adrenal axis in humans. J. Clin. Endocrinol. Metab. 1993, 77, 1690–1694. [Google Scholar] [PubMed]
- Madsen, T.; Skou, H.A.; Hansen, V.E.; Fog, L.; Christensen, J.H.; Toft, E.; Schmidt, E.B. C-reactive protein, dietary n-3 fatty acids, and the extent of coronary artery disease. Am. J. Cardiol. 2001, 88, 1139–1142. [Google Scholar] [CrossRef]
- Devaraj, S.; Jialal, I. Alpha tocopherol supplementation decreases serum C-reactive protein and monocyte interleukin-6 levels in normal volunteers and type 2 diabetic patients. Free Radic. Biol. Med. 2000, 29, 790–792. [Google Scholar] [CrossRef]
- Sierksma, A.; van der Gaag, M.S.; Kluft, C.; Hendriks, H.F. Moderate alcohol consumption reduces plasma C-reactive protein and fibrinogen levels; a randomized, diet-controlled intervention study. Eur. J. Clin. Nutr. 2002, 56, 1130–1136. [Google Scholar] [CrossRef] [PubMed]
- Adams, J.S.; Hewison, M. Unexpected actions of vitamin D: New perspectives on the regulation of innate and adaptive immunity. Nat. Clin. Pract. Endocrinol. Metab. 2008, 4, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro da Silva, F.; Machado, M.C. Antimicrobial peptides: Clinical relevance and therapeutic implications. Peptides 2012, 36, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Pellicane, A.J.; Wysocki, N.M.; Schnitzer, T.J. Prevalence of 25-hydroxyvitamin D deficiency in the outpatient rehabilitation population. Am. J. Phys. Med. Rehabil. 2010, 89, 899–904. [Google Scholar] [CrossRef] [PubMed]
- Quraishi, S.A.; Camargo, C.A. Vitamin D in acute stress and critical illness. Curr. Opin. Clin. Nutr. Metab. Care 2012, 15, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Jeng, L.; Yamshchikov, A.V.; Judd, S.E.; Blumberg, H.M.; Martin, G.S.; Ziegler, T.R.; Tangpricha, V. Alterations in vitamin D status and anti-microbial peptide levels in patients in the intensive care unit with sepsis. J. Transl. Med. 2009, 7, 28. [Google Scholar] [CrossRef] [PubMed]
- Venning, G. Recent developments in vitamin D deficiency and muscle weakness among elderly people. BMJ 2005, 330, 524–526. [Google Scholar] [CrossRef] [PubMed]
- Pfeifer, M.; Begerow, B.; Minne, H.W.; Schlotthauer, T.; Pospeschill, M.; Scholz, M.; Lazarescu, A.D.; Pollähne, W. Vitamin D status, trunk muscle strength, body sway, falls, and fractures among 237 postmenopausal women with osteoporosis. Exp. Clin. Endocrinol. Diabetes 2001, 109, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Simpson, J.L.; Bischoff, F. Cell-free fetal DNA in maternal blood: Evolving clinical applications. JAMA 2004, 291, 1135–1137. [Google Scholar] [CrossRef] [PubMed]
- Rondanelli, M.; Klersy, C.; Terracol, G.; Talluri, J.; Maugeri, R.; Guido, D.; Faliva, M.A.M.; Solerte, B.S.; Fioravanti, M.; Lukaski, H.; et al. Whey protein, amino acids, and vitamin D supplementation with physical activity increases fat-free mass and strength, functionality, and quality of life and decreases inflammation in sarcopenic elderly. Am. J. Clin. Nutr. 2016, 103, 830–840. [Google Scholar] [CrossRef] [PubMed]
- Hedström, M.; Ljungqvist, O.; Cederholm, T. Metabolism and catabolism in hip fracture patients: Nutritional and anabolic intervention-a review. Acta Orthop. 2006, 77, 741–747. [Google Scholar] [CrossRef] [PubMed]
- Magaziner, J.; Simonsick, E.M.; Kashner, T.M.; Hebel, J.R.; Kenzora, J.E. Predictors of functional recovery one year following hospital discharge for hip fracture: A prospective study. J. Gerontol. 1990, 45, 101–107. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| EAA Group | Casein Group | |
|---|---|---|
| Total amino acid (4 g) of which (mg) | ||
| Leucine | 1250 | 380 |
| Valine | 625 | 272 |
| Isoleucine | 625 | 208 |
| Lysine | 650 | 308 |
| Threonine | 350 | 209 |
| Cysteine | 150 | 16 |
| Histidine | 150 | 104 |
| Phenylalanine | 100 | 192 |
| Methionine | 50 | 96.5 |
| Tyrosine | 30 | 209 |
| Tryptophan | 20 | 32 |
| Serine | - | 228 |
| Proline | - | 391.5 |
| Glycine | - | 52 |
| Glutamic acid | - | 801 |
| Aspartic acid | - | 268 |
| Arginine | - | 128 |
| Alanine | - | 105 |
| EAA tot | 3820 | 1801.5 |
| % tot amino acids | 95.5% | 45% |
| BCAA | 2500 | 860 |
| % tot | 62.5% | 21.5% |
| Variables | nv | Placebo Group (n°56) | EAA Supplemented Group (n°56) | p Value |
|---|---|---|---|---|
| Demographic | ||||
| Male/Female | - | 27/29 | 25/31 | 0.3 |
| Age (years) | - | 81.4 ± 8.1 | 83.1 ± 7.5 | 0.15 |
| Anthropometric | ||||
| Body weight (kg) | - | 63.5 ± 18 | 62 ± 16.1 | 0.79 |
| Body Mass Index (BMI) (kg/m2) | - | 25.7 ± 7.9 | 24.9 ± 8.5 | 0.41 |
| Co-morbidity index (scores) | - | 1.8 ± 1.3 | 1.75 ± 1.2 | 0.78 |
| Biohumoral | ||||
| Glucose (mg/dL) | 78–110 | 98 ± 17 | 95 ± 8 | 0.8 |
| Glycated hemoglobin (%) | ≤6 | 6.3 ± 2.7 | 6.1 ± 1.8 | 0.71 |
| Urea nitrogen (mg/dL) | 4.67–23.3 | 24.6 ± 6 | 23 ± 9.1 | 0.69 |
| Creatinine (mg/dL) | 0.5–1.1 | 1.01 ± 0.6 | 1 ± 0.9 | 0.11 |
| Daily nutritional intake | Recommended * | |||
| Energy | ||||
| kcal | - | 1511 ± 345 | 1460 ± 319 | - |
| kcal/kg | 29.4 M 27 F | 23.8 ± 7.2 | 24.1 ± 6.4 | 0.9 |
| Proteins | ||||
| g | - | 58 ± 11 | 57 ± 13 | - |
| g/kg | ≥1.1 | 0.91 ± 0.2 | 0.92 ± 0.3 | 0.89 |
| %Ė | - | 15.3 ± 2.9 | 15.6 ± 3.5 | - |
| Providing EAAs (mg) | ||||
| Lysine | 3810 ± 285 | 4093 ± 457 | 0.7 | |
| Histidine | 1669 ± 180 | 1624 ± 239 | 0.9 | |
| Threonine | 2362 ± 341 | 2258 ± 401 | 0.8 | |
| Valine | 3230 ± 454 | 3347 ± 398 | 0.8 | |
| Isoleucine | 2800 ± 375 | 2899 ± 315 | 0.9 | |
| Leucine | 4900 ± 615 | 4981 ± 585 | 0.9 | |
| Methionine | 1342 ± 302 | 1417 ± 412 | 0.7 | |
| Phenyalanine | 2600 ± 299 | 2757 ± 416 | 0.5 | |
| Tryptophan | 650 ± 72 | 690 ± 122 | 0.6 | |
| Total | 23,363 ± 2780 | 24,066 ± 2954 | 0.7 | |
| % proteins | 40.2 ± 4.8 | 42.2 ± 5.2 | 0.8 | |
| Carbohydrates | ||||
| g | - | 171.5 ± 41 | 179.8 ± 51 | - |
| g/kg | 2.5–4 | 2.7 ± 0.55 | 2.9 ± 0.9 | - |
| %Ė | - | 45.4 ± 10.8 | 49.3 ± 14 | 0.78 |
| Simple sugar | ||||
| g | - | 64.4 ± 4.5 | 65.1 ± 3.2 | - |
| %Ė | <15 | 17 ± 1.2 | 17.8 ± 0.9 | 0.9 |
| Lipids | ||||
| g | - | 66.3 ± 18 | 60.8 ± 16 | - |
| g/kg | ≤1 | 1.04 ± 0.4 | 0.98 ± 0.31 | 0.22 |
| %Ė | <30 | 39.5 ± 2.76 | 40.1 ± 4.9 | 0.85 |
| Saturated | ||||
| g | 17.5 ± 3.9 | 12.1 ± 2.6 | - | |
| %Ė | <10 | 10.4 ± 2.5 | 7.45 ± 3.7 | 0.45 |
| Monounsaturated | ||||
| g | 40 ± 4.3 | 41.5 ± 6.8 | - | |
| %Ė | 23.8 ± 2.5 | 25.6 ± 4.2 | 0.75 | |
| Polyunsaturated | ||||
| g | 8.8 ± 2.9 | 7.2 ± 2.2 | - | |
| %Ė | 5–10 | 5.2 ± 1.7 | 4.4 ± 1.34 | 0.8 |
| Omega 6 | ||||
| g | 7.1 ± 2.8 | 6.1 ± 1.15 | ||
| %Ė | 4–8 | 4.2 ± 0.45 | 3.76 ± 0.71 | 0.65 |
| Omega 3 | ||||
| g | 1.7 ± 0.45 | 1.2 ± 0.6 | ||
| %Ė | 0.5–2 | 0.01 ± 0.002 | 0.007 ± 0.003 | 0.81 |
| Fibre (g) | >25 | 14.8 ± 4.3 | 21.7 ± 9.6 | 0.4 |
| Calcium (mg) | 1200 M; 1200 F | 855 ± 184 | 786 ± 230 | 0.84 |
| Phosphorous (mg) | 700 M; 700 F | 1050 ± 351 | 654 ± 251 | 0.2 |
| Potassium (mg) | 3900 M; 3900 F | 2384 ± 146 | 2185 ± 192 | 0.85 |
| Sodium (mg) | 1200 M; 1200 F | 1354 ± 139 | 1275 ± 235 | 0.78 |
| Iron (mg) | 10 M; 10 F | 10.5 ± 3.7 | 9.8 ± 1.5 | 0.91 |
| Zinc (mg) | 12 M; 9 F | 0.7 ± 0.15 | 0.95 ± 0.21 | 0.30 |
| Thiamin (mg) | 1.2 M; 1.1 F | 1.1 ± 0.1 | 0.99 ± 0.14 | 0.9 |
| Riboflavin (mg) | 1.6 M; 1.3 F | 1.25 ± 0.4 | 1.17 ± 0.15 | 0.75 |
| Niacin (mg) | 18 M; 18 F | 14.7 ± 3.6 | 13.8 ± 2.5 | 0.85 |
| Vitamin A (µg) | 700 M; 600 F | 585 ± 128 | 588 ± 97 | 0.97 |
| Vitamin C (mg) | 105 M; 85 F | 75 ± 21 | 82 ± 32 | 0.88 |
| Water (mL) | - | 854 ± 160 | 794 ± 89 | 0.91 |
| Circulating Proteins | Placebo n = 56 | EAAs n = 56 | p Interaction | ||||
|---|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T0 | T1 | T2 | ||
| Albumin g/dL (n.v. 3.5–5) | 3.45 ± 0.34 | 3.50 ± 0.25 | 3.51 ± 0.34 | 3.47 ± 0.41 | 3.59 ± 0.48 | 3.7 ± 0.52 | =0.038 |
| Haemoglobin g/dL (n.v. ≥12 F; ≥13 M) | 11.8 ± 1.7 | 11.7 ± 1.6 | 11.7 ± 1.6 | 11.4 ± 1.7 | 11.8 ± 1.7 | 12.2 ± 1.6 | =0.008 |
| Prealbumin mg/dL (n.v. 18–38) | 15.9 ± 4 | 15.9 ± 3 | 16.1 ± 4.1 | 15.7 ± 5.7 | 18 ± 7.6 | 17.6 ± 6.1 | =0.3 |
| C-reactive protein mg/dL (n.v. <0.8) | 9.3 ± 6.5 | 16.9 ± 16.1 | 10.1 ± 9.4 | 20 ± 17.8 | 24.5 ± 14.8 | 13.5 ± 9.3 | =0.1 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aquilani, R.; Zuccarelli, G.C.; Condino, A.M.; Catani, M.; Rutili, C.; Del Vecchio, C.; Pisano, P.; Verri, M.; Iadarola, P.; Viglio, S.; et al. Despite Inflammation, Supplemented Essential Amino Acids May Improve Circulating Levels of Albumin and Haemoglobin in Patients after Hip Fractures. Nutrients 2017, 9, 637. https://doi.org/10.3390/nu9060637
Aquilani R, Zuccarelli GC, Condino AM, Catani M, Rutili C, Del Vecchio C, Pisano P, Verri M, Iadarola P, Viglio S, et al. Despite Inflammation, Supplemented Essential Amino Acids May Improve Circulating Levels of Albumin and Haemoglobin in Patients after Hip Fractures. Nutrients. 2017; 9(6):637. https://doi.org/10.3390/nu9060637
Chicago/Turabian StyleAquilani, Roberto, Ginetto Carlo Zuccarelli, Anna Maria Condino, Michele Catani, Carla Rutili, Consiglia Del Vecchio, Pietro Pisano, Manuela Verri, Paolo Iadarola, Simona Viglio, and et al. 2017. "Despite Inflammation, Supplemented Essential Amino Acids May Improve Circulating Levels of Albumin and Haemoglobin in Patients after Hip Fractures" Nutrients 9, no. 6: 637. https://doi.org/10.3390/nu9060637
APA StyleAquilani, R., Zuccarelli, G. C., Condino, A. M., Catani, M., Rutili, C., Del Vecchio, C., Pisano, P., Verri, M., Iadarola, P., Viglio, S., & Boschi, F. (2017). Despite Inflammation, Supplemented Essential Amino Acids May Improve Circulating Levels of Albumin and Haemoglobin in Patients after Hip Fractures. Nutrients, 9(6), 637. https://doi.org/10.3390/nu9060637