Botulinum Neurotoxin Injection for the Treatment of Recurrent Temporomandibular Joint Dislocation with and without Neurogenic Muscular Hyperactivity


Abstract
:1. Introduction
2. Results
3. Discussion
3.1. Limitations
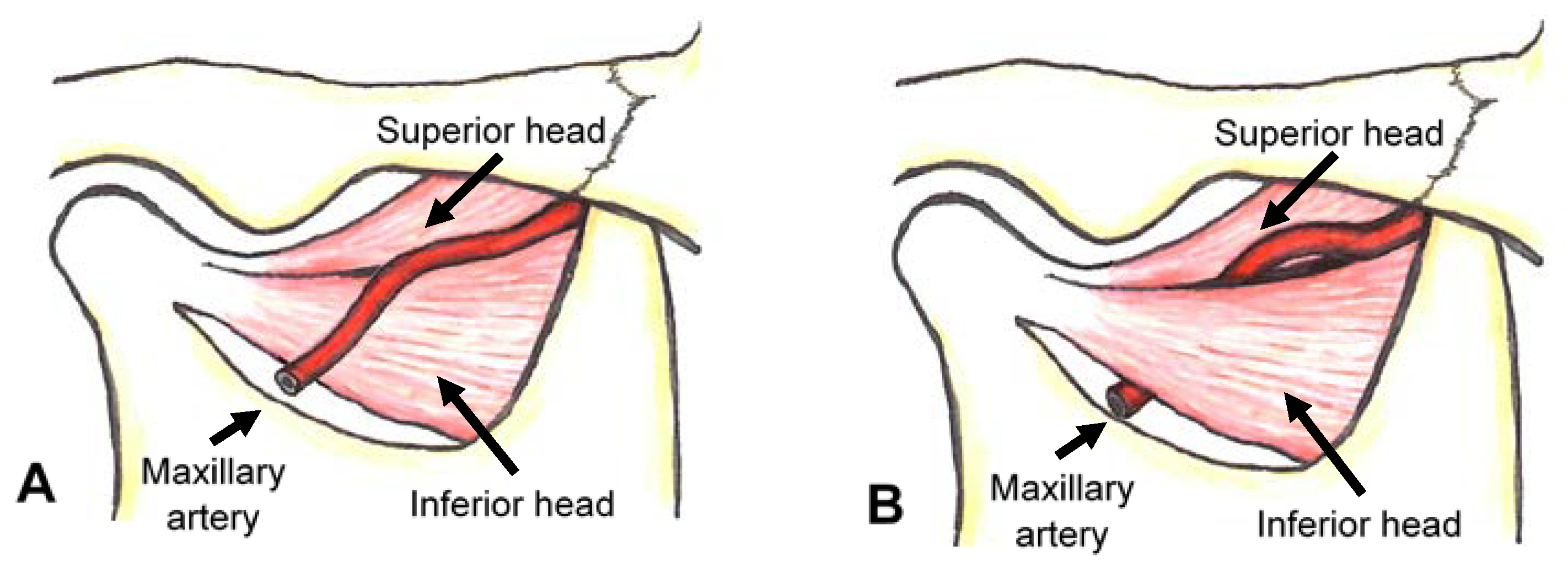
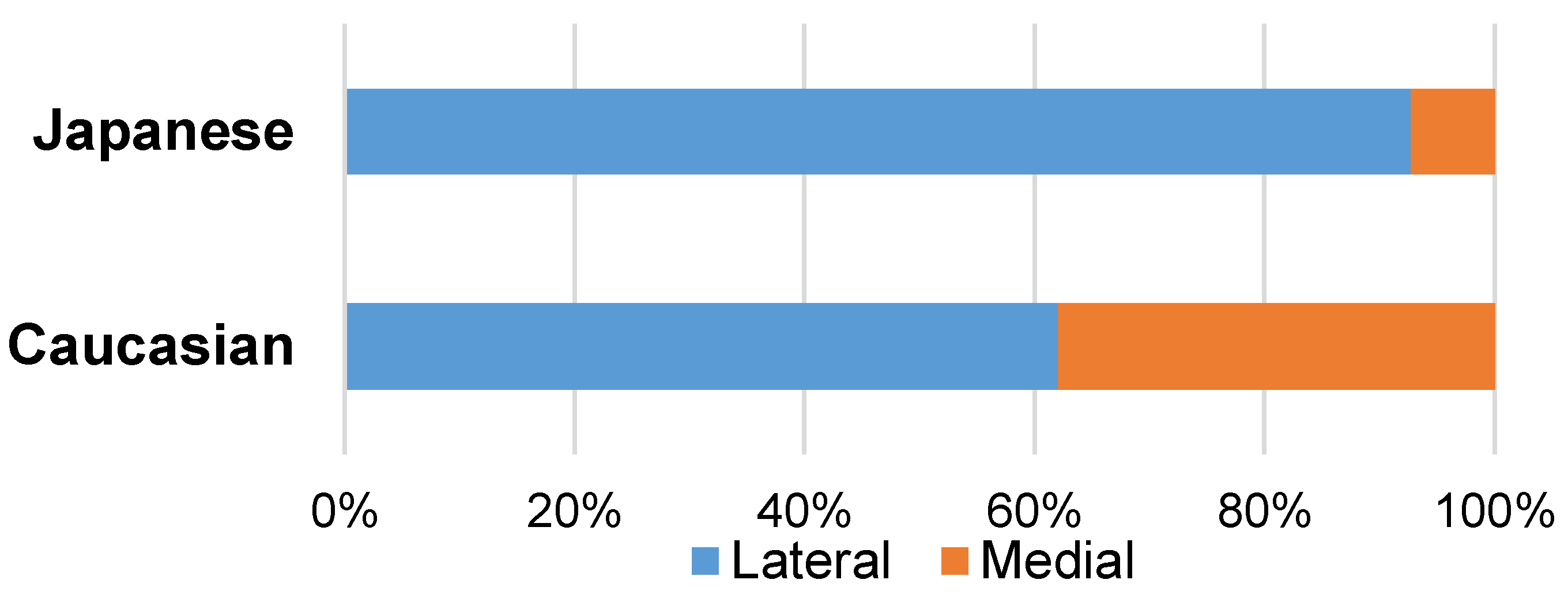
3.2. Local Anatomy for Safe Injection
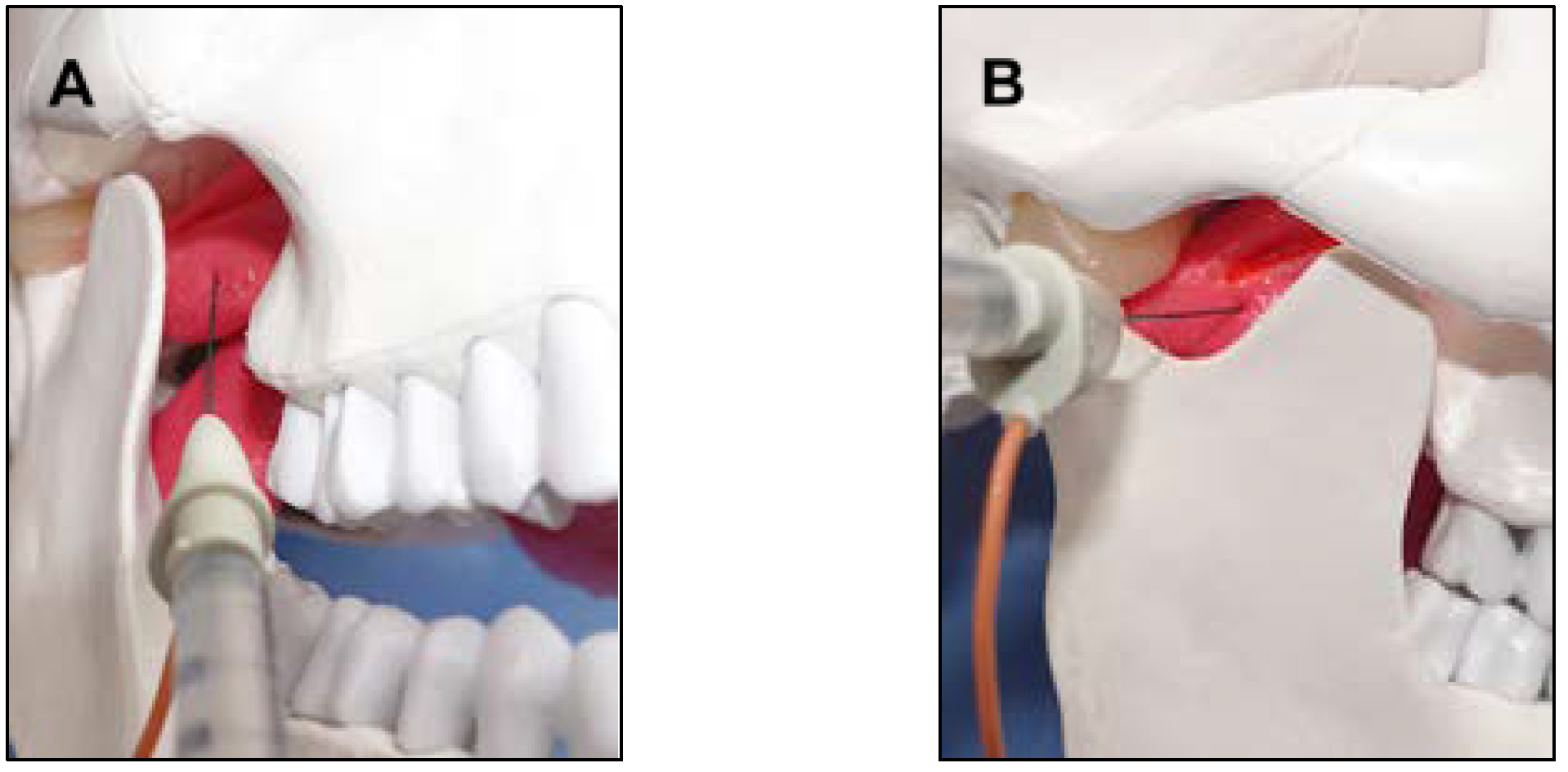
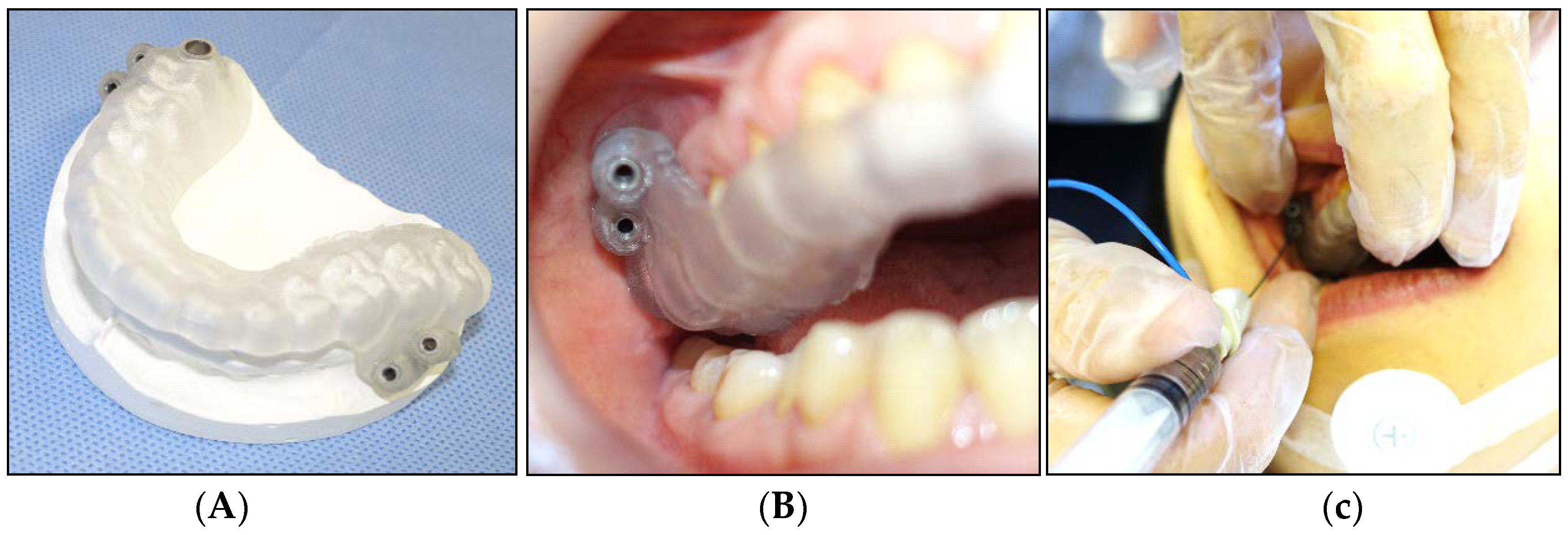
3.3. Injection Methods into the Lateral Pterygoid Muscle
3.4. BoNT Therapy for Recurrent Temporomandibular Joint Dislocation
3.5. Differences in the Pathophysiology between Neurogenic and Habitual Dislocation
4. Conclusions
5. Materials and Methods
5.1. Patients
5.2. Botulinum Neurotoxin (BoNT) Therapy
5.3. Statistical Analysis
Acknowledgments
Conflicts of Interest
References
- Simpson, L.L. The origin, structure, and pharmacologic activity of botulinum toxin. Pharmacol. Rev. 1981, 33, 155–188. [Google Scholar] [PubMed]
- Jankovic, J.; Brin, M.F. Therapeutic uses of botulinum toxin. N. Engl. J. Med. 1991, 324, 1186–1194. [Google Scholar] [PubMed]
- Truong, D.D.; Stenner, A.; Reichel, G. Current clinical applications of botulinum toxin. Curr. Pharm. Des. 2009, 15, 3671–3680. [Google Scholar] [CrossRef] [PubMed]
- Hallett, M.; Albanese, A.; Dressler, D.; Segal, K.R.; Simpson, D.M.; Truong, D.; Jankovic, J. Evidence-based review and assessment of botulinum neurotoxin for the treatment of movement disorders. Toxicon 2013, 67, 94–114. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, J. An update on new and unique uses of botulinum toxin in movement disorders. Toxicon 2017. [Google Scholar] [CrossRef] [PubMed]
- Comella, C.L. Systematic review of botulinum toxin treatment for oromandibular dystonia. Toxicon 2018. [Google Scholar] [CrossRef] [PubMed]
- Laskawi, R. The use of botulinum toxin in head and face medicine: An interdisciplinary field. Head Face Med. 2008, 4, 5. [Google Scholar] [CrossRef] [PubMed]
- Persaud, R.; Garas, G.; Silva, S.; Stamatoglou, C.; Chatrath, P.; Patel, K. An evidence-based review of botulinum toxin (Botox) applications in non-cosmetic head and neck conditions. J. R. Soc. Med. Short Rep. 2013, 4, 10. [Google Scholar] [CrossRef] [PubMed]
- Undt, G. Temporomandibular joint eminectomy for recurrent dislocation. Atlas Oral Maxillofac. Surg. Clin. N. Am. 2011, 19, 189–206. [Google Scholar] [CrossRef] [PubMed]
- Kamiyama, M. An electromyographic study on the function of the external pterygoid muscle. Kokubyo Gakkai Zasshi 1958, 25, 576–595. [Google Scholar] [CrossRef]
- Mahan, P.E.; Wilkinson, T.M.; Gibbs, C.H.; Mauderli, A.; Brannon, L.S. Superior and inferior bellies of the lateral pterygoid muscle EMG activity at basic jaw position. J. Prosthet. Dent. 1983, 50, 710–718. [Google Scholar] [CrossRef]
- Widmalm, S.E.; Lillie, J.H.; Ash, M.M., Jr. Anatomical and electromyographic studies of the lateral pterygoid muscle. J. Oral Rehabil. 1987, 14, 429–446. [Google Scholar] [CrossRef] [PubMed]
- Koole, P.; Beenhakker, F.; Brongersma, A.J.; Boering, G. A standardized technique for the placement of electrodes in the two heads of the lateral pterygoid muscle. J. Craniomand. Pract. 1990, 8, 154–162. [Google Scholar] [CrossRef]
- Yoshida, K.; Fukuda, Y.; Takahashi, R.; Nishiura, K.; Inoue, H. A method for inserting the EMG electrode into the superior head of the human lateral pterygoid muscle. J. Jpn. Prosthodont. Soc. 1992, 36, 88–93. [Google Scholar] [CrossRef]
- Yoshida, K. An electromyographic study on the superior head of the lateral pterygoid muscle during mastication from the standpoint of condylar movement. J. Jpn. Prosthodont. Soc. 1992, 36, 110–120. [Google Scholar] [CrossRef]
- Yoshida, K. Masticatory muscle responses associated with unloading of biting force during food crushing. J. Oral Rehabil. 1998, 25, 830–837. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K. Eigenschaften der Kaumuskelaktivität während verschiedenen Unterkieferbewegungen bei Patienten mit Diskusverlagerung ohne Reposition. Stomatologie 1999, 96, 107–121. [Google Scholar]
- Murray, G.M.; Bhutada, M.; Peck, C.C.; Phanachet, I.; Sae-Lee, D.; Whittle, T. The human lateral pterygoid muscle. Arch. Oral Biol. 2007, 52, 377–380. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Kaji, R.; Takagi, A.; Iizuka, T. Customized EMG needle insertion guide for the muscle afferent block of jaw-deviation and jaw-opening dystonias. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1999, 88, 664–669. [Google Scholar] [CrossRef]
- Møller, E.; Bakke, M.; Dalager, T.; Werdelin, L.M. Oromandibular dystonia involving the lateral pterygoid muscles: Four cases with different complexity. Mov. Disord. 2007, 22, 785–790. [Google Scholar] [CrossRef] [PubMed]
- Mendes, R.A.; Upton, L.G. Management of dystonia of the lateral pterygoid muscle with botulinum toxin A. Br. J. Oral Maxillofac. Surg. 2008, 47, 481–483. [Google Scholar] [CrossRef] [PubMed]
- Martos-Díaz, P.; Rodríguez-Campo, F.J.; Bances-Del Castillo, R.; Altura-Guillén, O.; Cho-Lee, G.Y.; de la-Plata, M.M.; Escorial-Hernandez, V. Lateral pterygoid muscle dystonia. A new technique for treatment with botulinum toxin guided by electromyography and arthroscopy. Med. Oral Pathol. Oral Cir. Bucal 2011, 16, e96–e99. [Google Scholar] [CrossRef]
- Moscovich, M.; Chen, Z.P.; Rodriguez, R. Successful treatment of open jaw and jaw deviation dystonia with botulinum toxin using a simple intraoral approach. J. Clin. Neurosci. 2015, 22, 594–596. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, Y.; Yoshida, K.; Inoue, H.; Suwa, F.; Ohta, Y. An experimental study on inserting an EMG electrode to the superior head of the human lateral pterygoid muscle. J. Jpn. Prosthodont. Soc. 1990, 34, 902–908. [Google Scholar] [CrossRef]
- Yoshida, K. How do I inject botulinum toxin into the lateral and medial pterygoid muscles? Mov. Disord. Clin. Pract. 2017, 4, 285. [Google Scholar] [CrossRef]
- Yoshida, K. Computer-aided design/computer-assisted manufacture-derived needle guide for injection of botulinum toxin into the lateral pterygoid muscle in patients with oromandibular dystonia. J. Oral Facial Pain Headache 2018, in press. [Google Scholar]
- Long, J.J. The relation of the internal maxillary artery to the external pterygoid muscle. Collective investigation in the anatomical department of Trinity college, Dublin. Trans. R. Acad. Med. Irel. 1890, 8, 520–521. [Google Scholar]
- Thomson, A. Report of the committee of collective investigation of the Anatomical Society of Great Britain and Ireland for the year 1889–1890. J. Anat. Physiol. 1891, 25, 89–101. [Google Scholar]
- Lauber, H. Ueber einige Varietäten im Verlaufe der Arteria maxillaris interna. Anat. Anz. 1901, 19, 444–448. [Google Scholar]
- Adachi, B. Das Arteriensystem der Japaner; Kyoto University: Kyoto, Japan, 1928; Volume 1, pp. 85–96. [Google Scholar]
- Fujita, T. Über einen Fall von beiderseitig medial vom N. mandibularis verlaufender A. maxillaries interna, nebst einer Statistik der verlaufsvariatioon der Arterie. J. Stomatol. Soc. Jpn. 1932, 6, 250–252. [Google Scholar] [CrossRef]
- Lasker, G.W.; Opdyke, D.L.; Miller, H. The position of the internal maxillary artery and its questionable relation to the cephalic index. Anat. Rec. 1951, 109, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Kijima, N. On distribution of the artery over the mandibular-joint. Med. J. Kagoshima Univ. 1958, 10, 71–83. [Google Scholar]
- Križan, Z. Beirträge zur deskriptiven und topographischen Anatomie der A. maxillaris. Acta Anat. 1960, 41, 319–333. [Google Scholar] [CrossRef] [PubMed]
- Ikakura, K. On the origin course and distribution of the maxillary artery in Japanese. Kouku Kaibou Kenkyu 1961, 18, 91–122. [Google Scholar]
- Lurje, A. On the topographical anatomy of the internal maxillary artery. Acta Anat. 1947, 2, 219–231. [Google Scholar] [CrossRef]
- Takarada, T. Anatomical studies on the maxillary artery. J. Tokyo Dent. Coll. Soc. 1958, 53, 1–20. [Google Scholar]
- Skopakoff, C. Über die Variabilität im Verlauf der A. maxillaris. Anat. Anz. 1968, 123, 534–546. [Google Scholar] [PubMed]
- Czerwiński, F. Variability of the course of external carotid artery and its rami in man in the light of anatomical and radiological studies. Folia Morphol. 1981, 40, 449–453. [Google Scholar]
- Iwamoto, S.; Konishi, M.; Takahashi, Y.; Kimura, K. Some variations in the course of the maxillary artery. J. Natl. Def. Med. Coll. 1981, 6, 75–78. [Google Scholar]
- Sashi, R. X-ray anatomy of the maxillary artery. Akita J. Med. 1990, 16, 817–831. [Google Scholar]
- Tsuda, K. Three-dimensional analysis of arteriographs of the maxillary artery in man—Part 1: The maxillary artery and its branches. J. Jpn. PRS 1991, 11, 188–198. [Google Scholar]
- Otake, I.; Kageyama, I.; Mataga, I. Clinical anatomy of the maxillary artery. Okajima Folia Anat. Jpn. 2011, 87, 155–164. [Google Scholar] [CrossRef]
- Maeda, S.; Aizawa, Y.; Kumaki, K.; Kageyama, I. Variations in the course of the maxillary artery in Japanese adults. Anat. Sci. Int. 2012, 87, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Daelen, B.; Thorwirth, V.; Koch, A. Botulinumtoxin bei habituellen Luxationen Behandlung einer rezidivierenden Kiefergelenksluxation mit Botulinumtoxin A. Mund Kiefer Gesichtschirurgie Mag. 1995, 22, 11–12. [Google Scholar]
- Daelen, B.; Thorwirth, V.; Koch, A. Treatment of recurrent dislocation of the temporomandibular joint with type A botulinum toxin. Int. J. Oral Maxillofac. Surg. 1997, 26, 458–460. [Google Scholar] [CrossRef]
- Daelen, B.; Thorwirth, V.; Koch, A. Neurogene Kiefergelenkluxation Definition und Therapie mit Botulinumtoxin. Definition und Therapie mit Botulinumtoxin. Nervenarzt 1997, 68, 346–350. [Google Scholar] [CrossRef] [PubMed]
- Moore, A.P.; Wood, G.D. Medical treatment of recurrent temporomandibular joint dislocation using botulinum toxin A. Br. Dent. J. 1997, 183, 415–417. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, C.M.; Haag, C.; Mühling, J. Treatment of recurrent temporomandibular joint dislocation with intramuscular botulinum toxin injection. Clin. Oral Investig. 2003, 7, 52–55. [Google Scholar] [CrossRef] [PubMed]
- Fu, K.Y.; Chen, H.M.; Sun, Z.P.; Zhang, Z.K.; Ma, X.C. Long-term efficacy of botulinum toxin type A for the treatment of habitual dislocation of the temporomandibular joint. Br. J. Oral Maxillofac. Surg. 2010, 48, 281–284. [Google Scholar] [CrossRef] [PubMed]
- Vázquez Bouso, O.; Forteza González, G.; Mommsen, J.; Grau, V.G.; Rodríguez Fernández, J.; Mateos Micas, M. Neurogenic temporomandibular joint dislocation treated with botulinum toxin: Report of 4 cases. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, e33–e37. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Pérez, D.; García Ruiz-Espiga, P. Recurrent temporomandibular joint dislocation treated with botulinum toxin: Report of 3 cases. J. Oral Maxillofac. Surg. 2004, 62, 244–246. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Iizuka, T. Botulinum toxin treatment for upper airway collapse resulting from temporomandibular joint dislocation due to jaw-opening dystonia. J. Craniomandib. Pract. 2006, 24, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K. Involuntary Movements of the Stomatognathic Region. Available online: https://sites.google.com/site/oromandibulardystoniaenglish/ (accessed on 19 April 2018).
- Yoshida, K.; Kaji, R.; Kubori, T.; Kohara, N.; Iizuka, T.; Kimura, J. Muscle afferent block for the treatment of oromandibular dystonia. Mov. Disord. 1998, 13, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Kaji, R.; Shibasaki, H.; Iizuka, T. Factors influencing the therapeutic effect of muscle afferent block for oromandibular dystonia and dyskinesia: Implications for their distinct pathophysiology. Int. J. Oral Maxillofac. Surg. 2002, 31, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Iizuka, T. Jaw-deviation dystonia evaluated by movement-related cortical potentials and treated with muscle afferent block. J. Craniomandib. Pract. 2003, 21, 295–300. [Google Scholar] [CrossRef]
- Yoshida, K. Sensory trick splint as a multimodal therapy for oromandibular dystonia. J. Prosthodont. Res. 2018, 62, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K. Surgical intervention for oromandibular dystonia-related limited mouth opening: Long-term follow-up. J. Cranioaxillofac. Surg. 2017, 45, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K. Coronoidotomy as treatment for trismus due to jaw-closing oromandibular dystonia. Mov. Disord. 2006, 21, 1028–1031. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K. Multilingual website and cyberconsultations for oromandibular dystonia. Neurol. Int. 2018, 10, 7536. [Google Scholar] [CrossRef]
- Singer, C.; Papapetropoulos, S. A comparison of jaw-closing and jaw-opening idiopathic oromandibular dystonia. Parkinsonism Relat. Discord. 2006, 12, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Albanese, A.; Bhatia, K.; Bressman, S.B.; Delong, M.R.; Fahn, S.; Fung, V.S.; Hallett, M.; Jankovic, J.; Jinnah, H.A.; Klein, C.; et al. Phenomenology and classification of dystonia: A consensus up date. Mov. Disord. 2013, 28, 863–873. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K. Clinical and phenomelogical characteristics of patients with task-specific lingual dystonia: Possible association with occupation. Front. Neurol. 2017, 8, 649. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Kaji, R.; Kohara, N.; Murase, N.; Ikeda, A.; Shibasaki, H.; Iizuka, T. Movement-related cortical potentials before jaw excursions in patients with oromandibular dystonia. Mov. Disord. 2003, 18, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Brin, M.F.; Blitzer, A.; Herman, S.; Stewart, C. Oromnadibular dystonia: Treatment of 96 patients with botulinum toxin type A. In Therapy with Botulinum-Toxin; Jankovic, J., Hallett, M., Eds.; Marcel Dekker: New York, NY, USA, 1994; pp. 429–435. [Google Scholar]
- Undt, G.; Kerner, C.; Piehslinger, E.; Rasse, M. Treatment of recurrent mandibular dislocation. Part I. Leclerc blocking procedure. Int. J. Oral Maxillofac. Surg. 1997, 26, 92–97. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient No. | Group | Dosage per Time (Units) | Dosage per Side (Units) | Botox Injection (Times) | Follow-Up (Months) |
|---|---|---|---|---|---|
| 1 | N | 25 | 25 | 2 | 12 |
| 2 | N | 50 | 25 | 2 | 6 |
| 3 | N | 50 | 25 | 5 | 36 |
| 4 | N | 50 | 25 | 8 | 38 |
| 5 | N | 50 | 25 | 12 | 48 |
| 6 | N | 50 | 25 | 2 | 12 |
| 7 | N | 50 | 25 | 6 | 28 |
| 8 | N | 50 | 25 | 2 | 29 |
| 9 | N | 50 | 25 | 8 | 52 |
| 10 | N | 50 | 25 | 2 | 45 |
| 11 | N | 50 | 50 | 3 | 51 |
| 12 | N | 50 | 25 | 4 | 59 |
| 13 | N | 50 | 25 | 8 | 75 |
| 14 | N | 50 | 25 | 2 | 26 |
| 15 | N | 50 | 25 | 2 | 15 |
| 16 | N | 50 | 25 | 2 | 13 |
| 17 | N | 50 | 25 | 5 | 31 |
| 18 | N | 50 | 25 | 2 | 19 |
| 19 | N | 50 | 25 | 3 | 10 |
| 20 | N | 75 | 37.5 | 2 | 15 |
| 21 | H | 50 | 50 | 1 | 27 |
| 22 | H | 50 | 25 | 7 | 56 |
| 23 | H | 50 | 25 | 1 | 6 |
| 24 | H | 50 | 25 | 1 | 9 |
| 25 | H | 50 | 50 | 1 | 10 |
| 26 | H | 50 | 25 | 1 | 9 |
| 27 | H | 50 | 25 | 2 | 12 |
| 28 | H | 50 | 25 | 1 | 47 |
| 29 | H | 50 | 25 | 1 | 53 |
| 30 | H | 50 | 25 | 2 | 15 |
| 31 | H | 50 | 25 | 1 | 14 |
| 32 | H | 50 | 25 | 1 | 65 |
| Mean (SD) | 50.0 (6.4) | 27.7 (7.6) | 3.2 (2.8) | 29.5 (19.9) |
| No. | Group | Age (Years) | Sex | Side | Duration (Months) | Frequency (Times/Week) | Diseases Causing Muscle Hyperactivity | Other Diseases | Denture |
|---|---|---|---|---|---|---|---|---|---|
| 1 | N | 33 | F | Uni | 30 | 1 | OMD, CD | schizophrenia | - |
| 2 | N | 86 | F | Bi | 8 | 21 | corticobasal degeneration, OMD | dementia, HT | + |
| 3 | N | 43 | M | Bi | 36 | 3 | OMD, CD, blepharospasm | depression | - |
| 4 | N | 38 | M | Bi | 180 | 0.5 | PD, generalized dystonia | - | - |
| 5 | N | 30 | M | Bi | 8 | 1 | OMD, CD | schizophrenia | - |
| 6 | N | 53 | M | Bi | 24 | 2 | OMD, WC | - | - |
| 7 | N | 51 | F | Bi | 1 | 3 | OMD, WC, CD | - | - |
| 8 | N | 48 | M | Bi | 120 | 1 | PD, OMD, CD | sleep apnea syndrome | - |
| 9 | N | 66 | M | Bi | 120 | 2 | PD, OMD | depression | - |
| 10 | N | 35 | F | Bi | 36 | 7 | OMD | schizophrenia | - |
| 11 | N | 50 | M | Uni | 6 | 3 | OMD | scoliosis | - |
| 12 | N | 67 | F | Bi | 36 | 7 | generalized dystonia | - | - |
| 13 | N | 29 | F | Bi | 12 | 5 | OMD | depression | - |
| 14 | N | 35 | M | Bi | 10 | 10 | OMD | panic disorder | - |
| 15 | N | 19 | F | Bi | 6 | 3 | OMD, CD, WC | depression | - |
| 16 | N | 42 | M | Bi | 1 | 14 | OMD, CD | dementia | - |
| 17 | N | 21 | M | Bi | 60 | 7 | generalized dystonia | hypoxia, DM | - |
| 18 | N | 84 | F | Bi | 8 | 14 | OMD | dementia, HT | + |
| 19 | N | 64 | M | Bi | 6 | 21 | multiple system atrophy, OMD | - | - |
| 20 | N | 80 | M | Bi | 5 | 2 | progressive supranuclear palsy, OMD | - | + |
| 21 | H | 79 | F | Bi | 3 | 2 | - | dementia, CI, HT | - |
| 22 | H | 87 | F | Uni | 120 | 0.5 | - | CI, HT, heart failure | + |
| 23 | H | 87 | F | Bi | 1 | 1 | - | dementia, osteoporosis, pneumonia | + |
| 24 | H | 84 | F | Bi | 6 | 0.5 | - | dementia | + |
| 25 | H | 98 | F | Uni | 3 | 14 | - | HT | - |
| 26 | H | 86 | F | Bi | 8 | 21 | - | dementia, HT, gastric ulcer | + |
| 27 | H | 84 | M | Bi | 2 | 23 | - | dementia | + |
| 28 | H | 80 | F | Bi | 6 | 14 | - | dementia | + |
| 29 | H | 88 | F | Bi | 84 | 7 | - | dementia, heart failure, breast cancer, depression | - |
| 30 | H | 83 | F | Bi | 3 | 7 | - | dementia, HT, pneumonia | + |
| 31 | H | 85 | F | Bi | 6 | 2 | - | dementia, HT | + |
| 32 | H | 77 | F | Bi | 4 | 14 | - | dementia, HT, CI, cervical spondylosis | - |
| Mean (SD) | 62.3 (24.0) | - | 30.0 (45.3) | 6.7 (6.5) | - | - |
© 2018 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshida, K. Botulinum Neurotoxin Injection for the Treatment of Recurrent Temporomandibular Joint Dislocation with and without Neurogenic Muscular Hyperactivity. Toxins 2018, 10, 174. https://doi.org/10.3390/toxins10050174
Yoshida K. Botulinum Neurotoxin Injection for the Treatment of Recurrent Temporomandibular Joint Dislocation with and without Neurogenic Muscular Hyperactivity. Toxins. 2018; 10(5):174. https://doi.org/10.3390/toxins10050174
Chicago/Turabian StyleYoshida, Kazuya. 2018. "Botulinum Neurotoxin Injection for the Treatment of Recurrent Temporomandibular Joint Dislocation with and without Neurogenic Muscular Hyperactivity" Toxins 10, no. 5: 174. https://doi.org/10.3390/toxins10050174
APA StyleYoshida, K. (2018). Botulinum Neurotoxin Injection for the Treatment of Recurrent Temporomandibular Joint Dislocation with and without Neurogenic Muscular Hyperactivity. Toxins, 10(5), 174. https://doi.org/10.3390/toxins10050174