Use of AbobotulinumtoxinA in Adults with Cervical Dystonia: A Systematic Literature Review




Abstract
:1. Introduction
2. Methods
3. Results
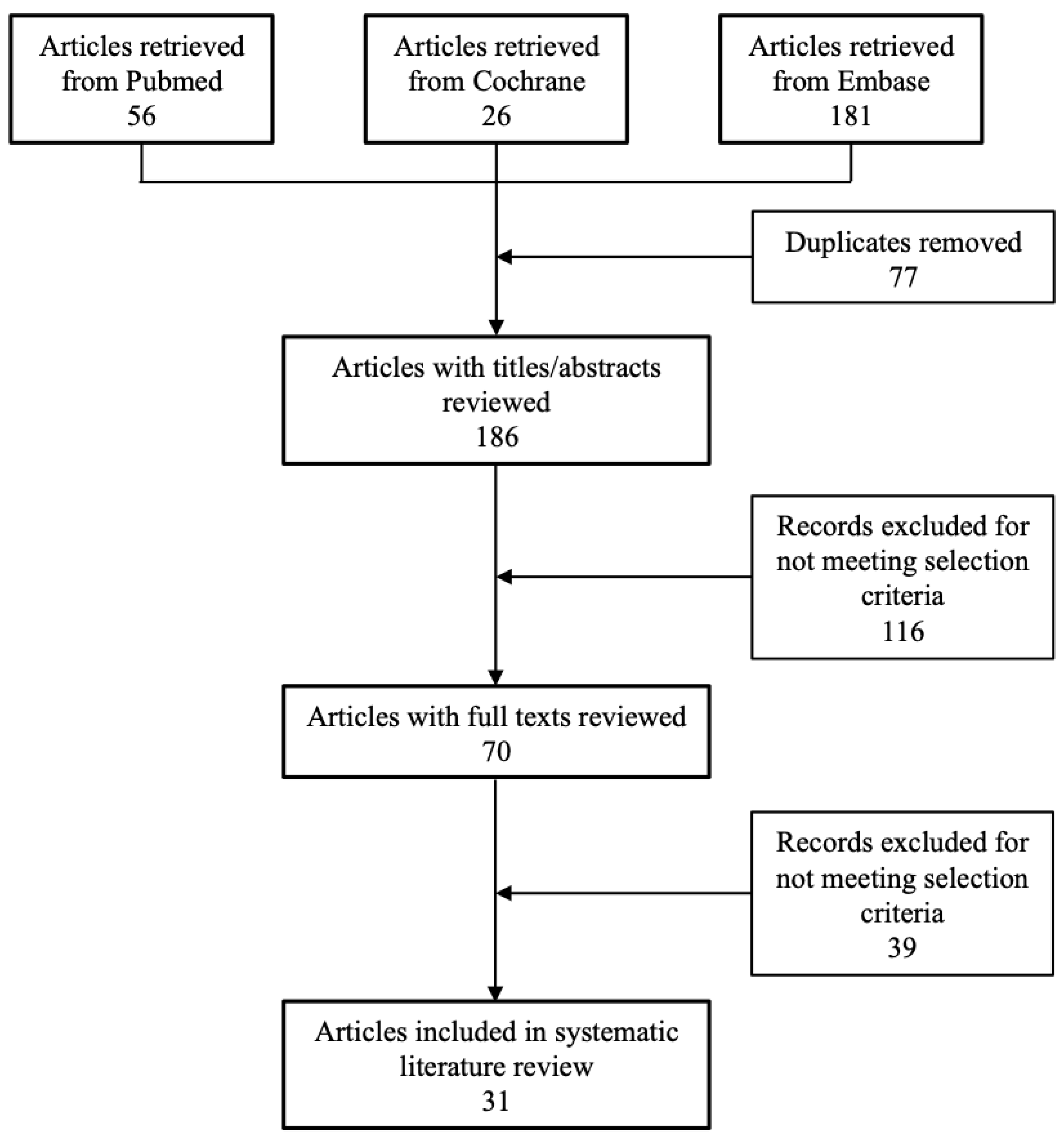
3.1. Identified Studies and Quality Assessment
3.2. Efficacy
3.2.1. Placebo-Controlled Studies
3.2.2. Active-Controlled Studies
3.2.3. Patient-Reported Outcomes
3.3. Safety
3.4. Health Economic Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethical Standards
Data Availability
References
- Jinnah, H.A.; Berardelli, A.; Comella, C.; Defazio, G.; Delong, M.R.; Factor, S.; Galpern, W.R.; Hallett, M.; Ludlow, C.L.; Perlmutter, J.S.; et al. The focal dystonias: Current views and challenges for future research. Mov. Disord. 2013, 28, 926–943. [Google Scholar] [CrossRef] [PubMed]
- Defazio, G.; Jankovic, J.; Giel, J.L.; Papapetropoulos, S. Descriptive epidemiology of cervical dystonia. Tremor Other Hyperkinet. Mov. 2013, 3, tre-03-193-4374-4372. [Google Scholar] [CrossRef]
- Simpson, D.M.; Blitzer, A.; Brashear, A.; Comella, C.; Dubinsky, R.; Hallett, M.; Jankovic, J.; Karp, B.; Ludlow, C.L.; Miyasaki, J.M.; et al. Assessment: Botulinum neurotoxin for the treatment of movement disorders (an evidence-based review): Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology 2008, 70, 1699–1706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albanese, A.; Abbruzzese, G.; Dressler, D.; Duzynski, W.; Khatkova, S.; Marti, M.J.; Mir, P.; Montecucco, C.; Moro, E.; Pinter, M.; et al. Practical guidance for CD management involving treatment of botulinum toxin: A consensus statement. J. Neurol. 2015, 262, 2201–2213. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Schünemann, H.; Oxman, A.; Vist, G.; Higgins, J.; Deeks, J.; Glasziou, G. Interpreting Results and Drawing Conclusions. In Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0. 2011. Available online: https://handbook-5-1.cochrane.org/index.htm#chapter_12/12_interpreting_results_and_drawing_conclusions.htm (accessed on 11 July 2020).
- Poewe, W.; Deuschl, G.; Nebe, A.; Feifel, E.; Wissel, J.; Benecke, R.; Kessler, K.R.; Ceballos-Baumann, A.O.; Ohly, A.; Oertel, W.; et al. What is the optimal dose of botulinum toxin A in the treatment of cervical dystonia? Results of a double blind, placebo controlled, dose ranging study using Dysport. German Dystonia Study Group. J. Neurol. Neurosurg. Psychiatry 1998, 64, 13–17. [Google Scholar] [CrossRef] [Green Version]
- Wissel, J.; Kanovsky, P.; Ruzicka, E.; Bares, M.; Hortova, H.; Streitova, H.; Jech, R.; Roth, J.; Brenneis, C.; Muller, J.; et al. Efficacy and safety of a standardised 500 unit dose of Dysport (clostridium botulinum toxin type A haemaglutinin complex) in a heterogeneous cervical dystonia population: Results of a prospective, multicentre, randomised, double-blind, placebo-controlled, parallel group study. J. Neurol. 2001, 248, 1073–1078. [Google Scholar]
- Truong, D.; Duane, D.D.; Jankovic, J.; Singer, C.; Seeberger, L.C.; Comella, C.L.; Lew, M.F.; Rodnitzky, R.L.; Danisi, F.O.; Sutton, J.P.; et al. Efficacy and safety of botulinum type A toxin (Dysport) in cervical dystonia: Results of the first US randomized, double-blind, placebo-controlled study. Mov. Disord. 2005, 20, 783–791. [Google Scholar] [CrossRef]
- Lew, M.F.; Brashear, A.; Dashtipour, K.; Isaacson, S.; Hauser, R.A.; Maisonobe, P.; Snyder, D.; Ondo, W. A 500 U/2 mL dilution of abobotulinumtoxinA vs. placebo: Randomized study in cervical dystonia. Int. J. Neurosci. 2018, 128, 619–626. [Google Scholar] [CrossRef]
- Poewe, W.; Burbaud, P.; Castelnovo, G.; Jost, W.H.; Ceballos-Baumann, A.O.; Banach, M.; Potulska-Chromik, A.; Ferreira, J.J.; Bihari, K.; Ehler, E.; et al. Efficacy and safety of abobotulinumtoxinA liquid formulation in cervical dystonia: A randomized-controlled trial. Mov. Disord. 2016, 31, 1649–1657. [Google Scholar] [CrossRef]
- Truong, D.; Brodsky, M.; Lew, M.; Brashear, A.; Jankovic, J.; Molho, E.; Orlova, O.; Timerbaeva, S. Long-term efficacy and safety of botulinum toxin type A (Dysport) in cervical dystonia. Parkinsonism Relat. Disord. 2010, 16, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Jen, M.-H.; Kurth, H.; Iheanacho, I.; Dinet, J.; Gabriel, S.; Wasiak, R.; Jost, W. Improvement of SF-36 scores in cervical dystonia patients—Is there a treatment effect when evaluating subscales? Basal Ganglia 2014, 4, 75–80. [Google Scholar] [CrossRef]
- Mordin, M.; Masaquel, C.; Abbott, C.; Copley-Merriman, C. Factors affecting the health-related quality of life of patients with cervical dystonia and impact of treatment with abobotulinumtoxinA (Dysport): Results from a randomised, double-blind, placebo-controlled study. BMJ Open 2014, 4, e005150. [Google Scholar] [CrossRef]
- Odergren, T.; Hjaltason, H.; Kaakkola, S.; Solders, G.; Hanko, J.; Fehling, C.; Marttila, R.J.; Lundh, H.; Gedin, S.; Westergren, I.; et al. A double blind, randomised, parallel group study to investigate the dose equivalence of Dysport and Botox in the treatment of cervical dystonia. J. Neurol. Neurosurg. Psychiatry 1998, 64, 6–12. [Google Scholar] [CrossRef] [Green Version]
- Laubis-Herrmann, U.; Fries, K.; Topka, H. Low-dose botulinum toxin-a treatment of cervical dystonia—A double-blind, randomized pilot study. Eur. Neurol. 2002, 47, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Ranoux, D.; Gury, C.; Fondarai, J.; Mas, J.; Zuber, M. Respective potencies of Botox and Dysport: A double blind, randomised, crossover study in cervical dystonia. J. Neurol. Neurosurg. Psychiatry 2002, 72, 459–462. [Google Scholar] [CrossRef]
- Yun, J.Y.; Kim, J.W.; Kim, H.T.; Chung, S.J.; Kim, J.M.; Cho, J.W.; Lee, J.Y.; Lee, H.N.; You, S.; Oh, E.; et al. Dysport and Botox at a ratio of 2.5:1 units in cervical dystonia: A double-blind, randomized study. Mov. Disord. 2015, 30, 206–213. [Google Scholar] [CrossRef]
- Barbosa, P.M.; Rodrigues, G.R.; de Oliveira, D.S.; de Souza, C.P.; Tumas, V. Comparison between Dysport and Prosigne in the treatment of cervical dystonia. Clin. Neuropharmacol. 2015, 38, 221–226. [Google Scholar] [CrossRef]
- Bigalke, H.; Wohlfarth, K.; Irmer, A.; Dengler, R. Botulinum A toxin: Dysport improvement of biological availability. Exp. Neurol. 2001, 168, 162–170. [Google Scholar] [CrossRef]
- Van den Bergh, P.; Francart, J.; Mourin, S.; Kollmann, P.; Laterre, E.C. Five-year experience in the treatment of focal movement disorders with low-dose Dysport botulinum toxin. Muscle Nerve 1995, 18, 720–729. [Google Scholar] [CrossRef]
- Kessler, K.R.; Skutta, M.; Benecke, R. Long-term treatment of cervical dystonia with botulinum toxin A: Efficacy, safety, and antibody frequency. German Dystonia Study Group. J. Neurol. 1999, 246, 265–274. [Google Scholar] [CrossRef]
- Jamieson, D.R.S.; Mann, A.C. Long-term follow-up by video of cervical dystonia treated with botulinum toxin. Eur. J. Neurol. 1997, 4, 443–447. [Google Scholar] [CrossRef]
- Hefter, H.; Benecke, R.; Erbguth, F.; Jost, W.; Reichel, G.; Wissel, J. An open-label cohort study of the improvement of quality of life and pain in de novo cervical dystonia patients after injections with 500 U botulinum toxin A (Dysport). BMJ Open 2013, 3. [Google Scholar] [CrossRef] [Green Version]
- Hefter, H.; Kupsch, A.; Mungersdorf, M.; Paus, S.; Stenner, A.; Jost, W. A botulinum toxin A treatment algorithm for de novo management of torticollis and laterocollis. BMJ Open 2011, 1, e000196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brefel-Courbon, C.; Simonetta-Moreau, M.; More, C.; Rascol, O.; Clanet, M.; Montastruc, J.L.; Lapeyre-Mestre, M. A pharmacoeconomic evaluation of botulinum toxin in the treatment of spasmodic torticollis. Clin. Neuropharmacol. 2000, 23, 203–207. [Google Scholar] [CrossRef] [PubMed]
- Misra, V.P.; Ehler, E.; Zakine, B.; Maisonobe, P.; Simonetta-Moreau, M. Factors influencing response to Botulinum toxin type A in patients with idiopathic cervical dystonia: Results from an international observational study. BMJ Open 2012, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trosch, R.M.; Espay, A.J.; Truong, D.; Gil, R.; Singer, C.; LeWitt, P.A.; Lew, M.F.; Tagliati, M.; Adler, C.H.; Chen, J.J.; et al. Multicenter observational study of abobotulinumtoxinA neurotoxin in cervical dystonia: The ANCHOR-CD registry. J. Neurol. Sci. 2017, 376, 84–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bentivoglio, A.R.; Di Stasio, E.; Mulas, D.; Cerbarano, M.L.; Ialongo, T.; Laurienzo, A.; Petracca, M. Long-Term Abobotulinumtoxin a treatment of cervical dystonia. Neurotox. Res. 2017, 32, 291–300. [Google Scholar] [CrossRef]
- Hefter, H.; Spiess, C.; Rosenthal, D. Very early reduction in efficacy of botulinum toxin therapy for cervical dystonia in patients with subsequent secondary treatment failure: A retrospective analysis. J. Neural Transm. 2014, 121, 513–519. [Google Scholar] [CrossRef] [Green Version]
- Dodel, R.C.; Kirchner, A.; Koehne-Volland, R.; Kunig, G.; Ceballos-Baumann, A.; Naumann, M.; Brashear, A.; Richter, H.P.; Szucs, T.D.; Oertel, W.H. Costs of treating dystonias and hemifacial spasm with botulinum toxin A. Pharmacoeconomics 1997, 12, 695–706. [Google Scholar] [CrossRef]
- Finsterer, J.; Fuchs, I.; Mamoli, B. Quantitative electromyography-guided botulinum toxin treatment of cervical dystonia. Clin. Neuropharmacol. 1997, 20, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, B.; Buhr, N.; Bigalke, H.; Krampfl, K.; Dengler, R.; Kollewe, K. A long-term follow-up of botulinum toxin A in cervical dystonia. Neurol. Res. 2009, 31, 463–466. [Google Scholar] [CrossRef] [PubMed]
- Haussermann, P.; Marczoch, S.; Klinger, C.; Landgrebe, M.; Conrad, B.; Ceballos-Baumann, A. Long-term follow-up of cervical dystonia patients treated with botulinum toxin A. Mov. Disord. 2004, 19, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, A.; Magar, R.; Findley, L.; Larsen, J.P.; Pirtosek, Z.; Ruzicka, E.; Jech, R.; Slawek, J.; Ahmed, F. Retrospective evaluation of the dose of Dysport and BOTOX in the management of cervical dystonia and blepharospasm: The REAL DOSE study. Mov. Disord. 2005, 20, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Rystedt, A.; Nyholm, D.; Naver, H. Clinical experience of dose conversion ratios between 2 botulinum toxin products in the treatment of cervical dystonia. Clin. Neuropharmacol. 2012, 35, 278–282. [Google Scholar] [CrossRef] [PubMed]
- Vivancos-Matellano, F.; Ybot-Gorrin, I.; Diez-Tejedor, E. A 17-year experience of abobotulinumtoxina in cervical dystonia. Int. J. Neurosci. 2012, 122, 354–357. [Google Scholar] [CrossRef]
- Jost, W.H.; Hefter, H.; Stenner, A.; Reichel, G. Rating scales for cervical dystonia: A critical evaluation of tools for outcome assessment of botulinum toxin therapy. J. Neural Transm. (Vienna) 2013, 120, 487–496. [Google Scholar] [CrossRef] [Green Version]
- Consky, E.; Basinski, A.; Belle, L.; Ranawaya, R.; Lang, A. The Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS): Assessment of validity and inter-rater reliability (abstract). Neurology 1990, 40, 445. [Google Scholar] [CrossRef]
- Trosch, R.M.; Shillington, A.C.; English, M.L.; Marchese, D. A retrospective, single-center comparative cost analysis of OnabotulinumtoxinA and AbobotulinumtoxinA for cervical dystonia treatment. J. Manag. Care Spec. Pharm. 2015, 21, 854–860. [Google Scholar] [CrossRef]
- Muthukumar, M.; Desai, K.; Abogunrin, S.; Harrower, T.; Gabriel, S.; Dinet, J. Cost-effectiveness analysis of abobotulinumtoxinA for the treatment of cervical dystonia in the United Kingdom. Clinicoecon. Outcomes Res. 2017, 9, 211–229. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Reference | Patients, n | aboBoNT-A Dose | Efficacy Outcomes | Safety | PROs |
|---|---|---|---|---|---|
| Poewe et al., 1998 [7] | aboBoNT-A 250 U, n = 19; 500 U, n = 16; 1000 U, n = 18 Placebo, n = 20 (All BoNT-naïve) | 250, 500, or 1000 U | Mean modified Tsui score week 4: statistically significant difference vs. placebo for 500 U and 1000 U dose groups (p < 0.05) | ≥1 TEAE: aboBoNT-A 250 U, 37%; 500 U, 65%; 1000 U, 83%; placebo: 25% Most common TEAEs (250 U, 500 U, 1000 U, placebo, respectively): dysphagia (21%, 29%, 39%, 10%), neck weakness (11%, 12%, 56%, 0%), dry mouth (21%, 18%, 33%, 5%), injection-site discomfort (5%, 18%, 28%, 10%) | Subjective global improvement >50% (placebo, 250 U, 500 U, 1000 U, respectively): week 2: 10%, 11%, 25%, 22% week 4: 10%, 16%, 25%, 44% * week 8: 11%, 11%, 38% *, 50% * |
| Wissel et al., 2001 [8] | aboBoNT-A, n = 35 (BoNT-A-naïve, n = 11) Placebo, n = 33 (BoNT-A-naïve, n = 10) | 500 U | Tsui mean score: aboBoNT-A, baseline (mean ± SD): 11.1 ± 1.7; weeks 4 and 8 (adjusted mean ± SEM): 6.5 ± 0.63 and 7.7 ± 0.58, respectively. Placebo, baseline (mean ± SD): 11.5 ± 1.8; weeks 4 and 8 (adjusted mean ±SEM): 9.5 ± 0.67 and 10.1 ± 0.62, respectively. Between-group comparison, week 4: p = 0.001; week 8: p = 0.002 | ≥1 TEAE: aboBoNT-A, 43%; placebo: 27% Most common TEAEs: dry mouth, neck muscle weakness, dysphagia, cold, and injection-site pain No serious TEAEs were reported TEAEs were more frequent in BoNT-A treatment–naïve than non-naïve patients: aboBoNT-A group, 7/11 (64%) naïve patients reported 15 TEAEs; 8/24 (33%) non-naïve patients reported 11 TEAEs. Placebo group, 3/10 (30%) naïve patients reported 7 TEAEs; 7/23 (30%) non-naïve patients reported 9 TEAEs | Pain score reduction, OR aboBoNT-A vs. placebo, week 4: 3.3, 95% CI: 1.2 to 9.4, p = 0.024; week 8: 2.1, 95% CI: 0.8 to 5.6, p = 0.152 Symptom improvement, OR aboBoNT-A vs. placebo, week 4: 8.5, 3.1 to 23.0, p < 0.001; week 8: 6.8, 95% CI: 2.5 to 18.3, p < 0.001 |
| Truong et al., 2005 [9] | aboBoNT-A, n = 37 (BoNT-naïve, n = 9) Placebo, n = 43 (BoNT-naïve, n = 12) | 500 U (range 400–500 U) | Primary: TWSTRS total score (change from baseline) week 4: aboBoNT-A, −9.9; placebo, −3.8. Difference in adjusted mean changes (ANCOVA): −6.0, 95% CI: −10.6 to −1.3; p = 0.013 Other: Difference in adjusted mean changes (ANCOVA), 8 weeks: −5.8; 95% CI: −9.9 to −1.6; p = 0.007. 12 weeks: −4.3; 95% CI: −8.2 to −0.4; p = 0.030 | ≥1 TEAE: aboBoNT-A, 92%; placebo, 79% Most common TEAEs: neck/shoulder pain (aboBoNT-A, 38%; placebo, 30%), injection-site pain (aboBoNT-A, 38%; placebo, 23%), tiredness (aboBoNT-A, 35%; placebo, 30%), headache (aboBoNT-A, 24%; placebo, 23%), dry mouth (aboBoNT-A, 22%; placebo, 19%), neck muscle weakness (aboBoNT-A, 16%; placebo, 12%), and dysphagia (aboBoNT-A, 16%; placebo, 9%) | Patient-assessed change in SD signs and symptoms, aboBoNT-A vs. placebo, week 4: 15.0; 95% CI: 6.3 to 23.7; p < 0.001; week 8: 12.9, 95% CI: 4.9 to 20.9; p = 0.002; week 12: 8.4; 95% CI: 1.2 to 15.5, p = 0.022 VAS pain score, week 4: −11.4, 95% CI: −21.3 to −1.5, p = 0.024; week 8: −8.8, 95% CI: −16.4 to −1.1, p = 0.025; week 12: −2.2, 95% CI: −8.3 to 3.9, p = 0.480 |
| Lew et al., 2018 [10] | aboBoNT-A, n = 89 (BoNT-naïve, n = 32) Placebo, n = 45 (BoNT-naïve, n = 16) | Mean: 451.8 U; median: 500 U | Primary: TWSTRS total score, weighted treatment difference from baseline, week 4: −8.3; 95% CI: −12.17 to −4.47 (p < 0.001) Subgroup analysis: BoNT-naïve vs. previously treated statistically significant differences in TWSTRS total score vs. baseline Other: TWSTRS total score, weighted treatment difference vs. baseline at week 2: −5.4; 95% CI: −8.76 to −2.12 (p = 0.002) | ≥1 TEAE: aboBoNT-A, 40.9%; placebo, 22.2% Serious TEAEs: aboBoNT-A, 4.5%; placebo, 2.2% Most common TEAEs: dysphagia (aboBoNT-A, 9.1%; placebo, 0%), muscular weakness (aboBoNT-A, 9.1%; placebo, 0%), neck pain (aboBoNT-A, 8.0%; placebo, 0%), headache (aboBoNT-A, 5.7%; placebo, 0%) | PGIC, CD rated as “much improved” or “very much improved,” week 4: aboBoNT-A, 38.4%; placebo, 11.1% Week 2: aboBoNT-A, 23.6%; placebo, 6.8% CDIP-58 total score: No statistically significant differences between aboBoNT-A and placebo; head and neck domain: aboBoNT-A, −15.9; placebo, −5.8 (ANOVA p = 0.016) |
| Poewe et al., 2016 [11] | aboBoNT-A solution for injection, n = 156 (BoNT-naïve, n = 36); dry formulation, n = 159 (BoNT-naïve, n = 40) Placebo, n = 54 (BoNT-naïve, n = 14) (Open-label extension with aboBoNT-A solution for injection, n = 333) | 500 U | Primary: TWSTRS total score (change from baseline), week 4: significant reduction in both aboBoNT-A groups vs. placebo (p < 0.0001) (actual values not stated) Non-inferiority of aboBoNT-A solution for injection vs. dry formulation was not established TWSTRS total score, weeks 2 and 8: Significant improvements in both aboBoNT-A groups vs. placebo TWSTRS total score, week 12: Significant improvements in the aboBoNT-A dry formulation group TWSTRS subscale scores, treatment difference vs. baseline, week 4: Significant reduction in both aboBoNT-A groups vs. placebo (p < 0.0001) (actual values not reported) Other: A post hoc analysis that excluded results from outlier centers (due to heterogeneity) met the non-inferiority criteria Efficacy maintained through open-label phase (up to 4 cycles) | ≥1 TEAE, cycle 1: aboBoNT-A solution for injection, 42.5%; dry formulation, 37.8%; placebo: 25.5% Severe TEAEs, cycle 1: aboBoNT-A solution for injection, 3.3%; dry formulation, 5.1%; placebo: 0% Most common TEAEs, cycle 1 (aboBoNT-A solution for injection, dry formulation, placebo, respectively): dysphagia (3.3%, 7.1%, 0%), nasopharyngitis (5.9%, 2.6%, 1.8%), injection-site pain (3.9%, 3.2%, 1.8%), neck pain (2.6%, 3.8%, 1.8%), and headache (3.9%, 1.9%, 1.8%) | CDIP-58 total score, least squares mean reduction, week 4 vs. baseline: aboBoNT-A solution for injection, −9.5; dry formulation, −11.2; placebo, −0.9 (p < 0.0001 for active groups vs. placebo) Statistically significant reductions in mean VAS pain scores and symptoms in aboBoNT-A groups vs. placebo. VAS pain score, week 4 vs. baseline: aboBoNT-A solution for injection vs. placebo, p < 0.005; dry formulation vs. placebo, p < 0.0001. Dry formulation vs. placebo at weeks 8 and 12 vs. placebo: p < 0.005 and p < 0.05, respectively |
| Truong et al., 2010 [12] HRQoL analyses (SF-36): Jen et al. 2014 [13] | aboBoNT-A, n = 55 (BoNT-naïve, n = 10) Placebo, n = 61 (BoNT-naïve, n = 10) | 500 U (open-label extension, mean cycle 1, 502 U; cycle 2, 643 U; cycle 3, 716 U; cycle 4, 776 U) | Primary: TWSTRS total score (change from baseline) week 4: (RCT phase), mean (± SEM): aboBoNT-A, −15.6 ± 2.0; placebo, −6.7 ± 2.0 (p < 0.001) Other: TWSTRS total score (change from baseline), week 12: (RCT phase), mean (± SEM): aboBoNT-A, −9.1 ± 1.7; placebo, −4.9 ± 1.7 (p = 0.019) Post hoc efficacy analysis showed no clinically meaningful difference (not defined) for BoNT-naïve vs. non-naïve group Open-label extension: Mean changes in TWSTRS total scores from treatment cycle baseline were −16.2, −11.4, −10.8, and −11.3 for cycles 1–4, respectively. (Greater improvements in cycle 1 than subsequent cycles reflect higher treatment cycle baseline scores at cycle 1 than cycles 2–4) | ≥1 TEAE: aboBoNT-A, 47%; placebo, 44%. Most TEAEs were mild or moderate Most common TEAE: dysphagia; RCT phase, aboBoNT-A, 9%; placebo, 0%; open-label phase, cycle 1, 12%; cycle 2, 13%; cycle 3, 6%; cycle 4, 10% | SF-36 mental health (change from baseline) week 8, aboBoNT-A vs. placebo: not statistically significant (p = 0.061). SF-36 physical health, (change from baseline) week 8, aboBoNT-A vs. placebo: not statistically significant due to hierarchical structure (p = 0.002) Statistically significant improvements in aboBoNT-A vs. placebo for VAS pain at weeks 4, 8, and 12 (p < 0.001, p < 0.001, and p = 0.007, respectively) HRQoL analyses (Jen et al.): SF-36, week 8 vs. baseline: No significant differences for vitality, social functioning, or mental health For domain scores, aboBoNT-A was more likely than placebo to show improvement for physical functioning (OR = 1.6; p = 0.01), role-emotional (OR = 2.4; p = 0.0001), and mental health (OR = 1.5; p = 0.007) |
| Mordin et al., 2014 [14] | Includes only patients who completed the RCT phase: aboBoNT-A, n = 45; placebo, n = 38) | 500 U | Efficacy previously reported in Truong et al. 2010 HRQoL assessed by the SF-36 Health Survey (SF-36) at weeks 0 and 8 | Safety previously reported in Truong et al. 2010 | HRQoL analyses: SF-36 (change from baseline) week 8: Physical functioning: aboBoNT-A, +8.2; placebo, −1.9 (p = 0.018) Role-physical: aboBoNT-A, +16.6; placebo, +3.2 (p = 0.008) Bodily pain: aboBoNT-A, +13.9; placebo, +2.9 (p = 0.010) General health: aboBoNT-A, +3.2; placebo, −2.5 (p = 0.030) Role-emotional: aboBoNT-A, +9.5; placebo, +4.3 (p = 0.030) |
| Article | Patients, n | Doses | Efficacy Outcomes | Safety | PROs |
|---|---|---|---|---|---|
| Odergren et al., 1998 [15] | aboBoNT-A, n = 38 onaBoNT-A, n = 35 | aboBoNT-A, 500 U (mean dose ± SD, 477 U ± 131; range, 240–720) onaBoNT-A, 100 U (mean dose ± SD, 152 U ± 45; range, 70–240) | Primary: Tsui score (mean ± SD), week 12 or at re-treatment (if earlier than week 12): aboBoNT-A, 4.8 ± 2.4; onaBoNT-A, 5.8 ± 2.6; difference not statistically significant after adjustment for baseline and center effects Mean time to re-treatment: aboBoNT-A, 84 days (range, 56–122); onaBoNT-A, 81 days (range, 49–111); difference not statistically significant Patients treated prior to week 12: aboBoNT-A, 26%; onaBoNT-A, 32% Patients treated after week 12: aboBoNT-A, 13%; onaBoNT-A, 9% | ≥1 TEAE: aboBoNT-A, 58%; onaBoNT-A, 69% Most common TEAEs: dysphagia (aboBoNT-A, 16%; onaBoNT-A, 11%), pharyngitis (aboBoNT-A, 11%; onaBoNT-A, 11%), headache (aboBoNT-A, 8%; onaBoNT-A, 17%), fatigue (aboBoNT-A, 8%; onaBoNT-A, 11%), and upper respiratory tract infection (aboBoNT-A, 8%; onaBoNT-A, 9%) Most TEAEs (>90%) were mild or moderate in severity TEAEs possibly or probably related to study medication, aboBoNT-A: 32% of patients; onaBoNT-A: 26%. Most common = dysphagia | Not reported |
| Laubis-Hermann et al., 2002 [16] | aboBoNT-A recommended dose, n = 15 aboBoNT-A low-dose, n = 16 | aboBoNT-A recommend-ded dose, 500 MU (mean dose, 547 MU; range, 350–700) aboBoNT-A low-dose, 125 MU (mean dose, 130 MU; range, 63–188) | TWSTRS total score vs. baseline at week 4: aboBoNT-A recommended dose: 5.6 ± 8.1 (p < 0.02); aboBoNT-A low-dose: 4.4 ± 5.6 (p < 0.01) Subscale scores: aboBoNT-A recommended dose: statistically significant improvements for disability and pain; aboBoNT-A low-dose: statistically significant improvements for disability and severity No statistically significant difference between treatments for the TWSTRS total or subscales scores | Not reported | Improvements in overall CD symptoms, magnitude of maximal effect (up to 5 days following injection): aboBoNT-A recommended dose, “striking improvement”: 21%; “marked response”: 36%; “moderate response”: 29%. aboBoNT-A low-dose, “striking improvement”: 0%; “marked response”: 53%; “moderate response”: 20% Degree of improvement after injection: aboBoNT-A recommended dose, “marked improvement”: 77%; “mild improvement”: 23%. aboBoNT-A low-dose, “marked improvement”: 50%; “moderate improvement”: 29%; “mild improvement”: 14%; “no improvement”: 7% |
| Ranoux et al., 2002 [17] | Total N = 54 (3-period cross-over study with sequential treatment) onaBoNT-A, n = 51 aboBoNT-A at a 1:3 onaBoNT-A to aboBoNT-A dose ratio, n = 51 aboBoNT-A at a 1:4 onaBoNT-A to aboBoNT-A dose ratio, n = 52 | onaBoNT-A at the usually effective dose (defined as the dose at which a satisfactory response was achieved in the previous two treatments) | Tsui mean score, week 4: onaBoNT-A, 3.22; aboBoNT-A 1:3 ratio, 4.32; aboBoNT-A 1:4 ratio, 4.89. onaBoNT-A vs. aboBoNT-A 1:3 ratio, p = 0.02; onaBoNT-A vs. aboBoNT-A 1:4 ratio, p = 0.01 TWSTRS pain score: onaBoNT-A vs. aboBoNT-A 1:3 ratio, p = 0.04; onaBoNT-A vs. aboBoNT-A 1:4 ratio, p = 0.02 Mean duration of action vs. onaBoNT-A: 7 days longer with aboBoNT-A 1:3 ratio (p = 0.58), 25 days longer with aboBoNT-A 1:4 ratio (p = 0.02) No significant differences between two aboBoNT-A groups | ≥1 TEAE: onaBoNT-A, 18%; aboBoNT-A 1:3 ratio: 33%; aboBoNT-A 1:4 ratio: 36% Most common TEAE: dysphagia (onaBoNT-A, 3%; aboBoNT-A 1:3 ratio: 16%; aboBoNT-A 1:4 ratio: 17%) No TEAE severe enough for study withdrawal | Not reported |
| Yun et al., 2015 [18] | aboBoNT-A and onaBoNT-A at 2.5:1.0 dose ratio, n = 94 (4-week washout period between the 16-week treatment cycles) | aboBoNT-A: 361.04 U ± 657.91 (range, 200–400) onaBoNT-A: 144.41 U ± 623.16 (range, 80–160) | Tsui mean score, week 4: aboBoNT-A, 4.0 ± 3.9; onaBoNT-A, 4.8 ± 4.1 (p = 0.091) TWSTRS total and subscale scores: differences not statistically significant | ≥1 TEAE: aboBoNT-A, 14.9%; onaBoNT-A, 20.2% Most common TEAEs: neck muscle weakness (aboBoNT-A, 9.6%; onaBoNT-A, 13.8%), dysphagia (aboBoNT-A, 6.4%; onaBoNT-A, 12.8%), and neck/shoulder pain (aboBoNT-A, 2.1%; onaBoNT-A, 7.4%) | Not reported |
| Barbosa et al., 2015 [19] | aboBoNT-A, n = 14 Lanzhou BTX-A, n = 20 | Equivalency ratio of 3 U of aboBoNT-A per 1 U of Lanzhou BTX-A | Primary: TWSTRS total score (change from baseline), week 4: aboBoNT-A, −12.78, 95% CI: −6.68 to −18.88; p = 0.001. Lanzhou BTX-A: −9.98; 95% CI: −6.38 to −13.58; p <0.001. No statistically significant difference between treatments (p = 0.38) Other: Statistically significant (p < 0.05) decreases from baseline in all TWSTRS subscale scores with both treatments; no statistically significant differences between treatments. Similar results observed for last injection (≤5 injections over 13 months) | Most common TEAEs in both treatment groups: dysphagia (27.3%), injection-site pain (4.5%), muscle weakness (1.3%) No statistically significant differences between aboBoNT-A and Lanzhou BTX-A groups regarding occurrence of TEAEs With the exception of one dysphagia event after the fourth injection, all dysphagia events with aboBoNT-A were mild (n = 22) | After first treatment, improvement for >3 months: aboBoNT-A, 14%; Lanzhou BTX-A: 25%. Improvement for 2–3 months: aboBoNT-A, 71%; Lanzhou BTX-A: 45% After fifth treatment, improvement for >3 months: aboBoNT-A, 55%; Lanzhou BTX-A: 50%. Improvement for 2–3 months: aboBoNT-A, 45%; Lanzhou BTX-A: 50% |
| Bigalke et al., 2001 [20] | aboBoNT-A Group A, n = 8; Group B, n = 38. Groups differed regarding monitoring and examinations | Group A, first 3× high dose (658 U ± 232), then ≥3× low dose (262 U ± 68) Group B, first 3× high dose (550 U ± 233), then 3× low dose (235 U ± 100) | Group A: Investigator-assessed symptom severity, beginning of relief and duration of improvement deemed as effective with high dose as with low dose Group B: Improvement rating, beginning of relief, and duration of improvement deemed as effective with high dose as with low dose | TEAEs, Group A, high dose: neck weakness, n = 4 patients; dysphagia, n = 1. Low-dose: none TEAEs, Group B, high-dose: neck weakness, n = 21 patients; dysphagia, n = 15; pain, n = 11; dysphonia, n = 4. Low-dose: neck weakness, n = 6; dysphagia, n = 1; pain, n = 4 | Not reported |
| Article | Study Type; Patients, n | Doses | Efficacy Outcomes | Safety | PROs |
|---|---|---|---|---|---|
| Van den Bergh et al., 1995 [21] | Open-label study; with CD, n = 28 | aboBoNT-A, mean ± SD dose per treatment cycle: 384 MU ± 188 (range: 63–1045) | 38-point composite score (based on: subjective rating 0–5, a Tsui score, and a video score), before treatment: 18.9 ± 4.4 (range 8.6–26.2); at peak improvement: 5.2 ± 3.0 (range 0–13.3) Last treatment (mean: 5 cycles) vs. first treatment, pre-treatment scores: –40% (p < 0.0001); post-treatment scores: –35% (p = 0.03) | Mild dysphagia in 2 patients with rotatocollis | Complete pain relief: 67% of patients; >50% pain relief: 25% of patients |
| Kessler et al., 1999 [22] | Prospective study, n = 303 | aboBoNT-A, mean per treatment: 778 ± 253 U | Greatest reduction in modified Tsui score after first injection (baseline median, 10; after injection median, 6; change from baseline, ‒3.7). Continued improvement (though less pronounced) through 6 injections. Tsui scores generally consistent after sixth injection, with median Tsui score of 4 before the 15th injection. Reduction in Tsui score statistically significant over first 6 injections (p < 0.0001) | ≥1 TEAE: 75% of patients TEAEs considered possibly related to treatment: 22% of treatments (685 of 3088 sessions) Most common TEAE: dysphagia (77.1% of all TEAEs), with most events mild or moderate in severity (87%) Other common TEAEs included neck muscle weakness (17.2% of all TEAEs), dry mouth (9.9%), neck pain (4.7%), voice changes (4.2%) | Not reported |
| Jamieson et al., 1997 [23] | Prospective observational study, n = 14 | aboBoNT-A, range, at first post-treatment video: 200–1000 U; at second post-treatment visit: 200–1200; highest dose: 400–1500 | Treatment duration 4 years 5 months to 6 years 7 months. Statistically significant (p < 0.05) difference between early and later post-treatment Tsui scores | Dysphagia: 8/15 patients (53%) treated long term | Not reported |
| Hefter et al., 2013; 2011 [24,25] | Prospective cohort study; aboBoNT-A, n = 503 | aboBoNT-A, 500 U | Tsui score, baseline: 8.4 ± 3.5; (change from baseline), week 4: ‒3.83; 95% CI: 4.01–3.57; p < 0.0001. Statistically significant improvements in all subscale scores Mean increase in symptom improvement: 44.3% (± 34.8%). Improvement sustained through week 12 of treatment cycle | ≥1 TEAE: 41.4% of patients Most common TEAEs: muscular weakness (13.8%), dysphagia (9.9%), and neck pain (6.6%) Most TEAEs (89.7%) were mild or moderate in severity, and 30.1% of TEAEs were considered treatment-related Serious TEAEs: 11 patients (2.1%); 2 considered possibly treatment-related At week 4, 86.7% of investigators and 80.3% of patients rated the tolerability of study medication as “good” or “very good.” Corresponding values at week 12 were 88.8% (investigators) and 85.4% (patients) | CDQ-24 vs. baseline, at week 4: ‒11.1; 95% CI: ‒12.5 to ‒9.6; p < 0.001. At week 12: ‒11.8; 95% CI: ‒13.1 to ‒10.4; p < 0.001. Improvements in all 5 subscales at weeks 4 and 12 (p < 0.001) Statistically significant improvements in patient-reported day-to-day capacities and activities, pain, and duration of pain (rated using an 11-point VAS) at both weeks 4 and 12 (p < 0.001) Pain relief (less or no pain), week 4: 66% of patients; week 12: 74% of patients Change from baseline in CDQ-24 total and subscale scores correlated with change from baseline in Tsui total score |
| Brefel-Courbon et al., 2000 [26] | Prospective; aboBoNT-A, n = 21 | Mean injected aboBoNT-A dose per session: 450 U ± 18 (range, 160–1120 U) | Tsui score, mean at baseline: 18.4; at 1 month after first injection: 10.5 (p < 0.0001) Average of 8.7 weeks of improvement Tsui scores continued to decrease and duration of improvement generally increased through the fifth injection | Most common AEs: dysphagia (45.9%), local pain (25.0%), muscle weakness (12.5%), fatigue (8.3%), and dysphonia (8.3%). None were considered “serious.” None resulted in study dropouts | Patients’ global assessments of treatment effect, after first injection: “marked” improvement, 52%; “moderate” improvement, 33%. For each injection, >60% of patients indicated “moderate” or “marked” improvement NHP: significant improvement in pain domain by end of study (p = 0.02); numerical improvements in domains of social isolation and emotional behavior |
| Misra et al., 2012 [27] | Prospective observational study (interest in CD); n = 404 | aboBoNT-A, median dose, 500 U (10% received ≥1000 U) onaBoNT-A; median dose, 160 U (10% received ≥300 U) | Treatment responders (defined as ≥25% TWSTRS severity scale improvement at visit 2 or 3 vs. visit 1; ≥12 weeks effect duration; no severe TEAEs; and patient-rated CGI score ≥2 at visits 2 and 3), overall: 28.6%; 95% CI: 24.0 to 33.5. aboBoNT-A ~33% and onaBoNT-A ~23% (actual values not reported) | No significant differences between treatment groups for the percentage of patients with ≥1 TEAE, ≥1 severe TEAE, or dysphagia at visit 2 | Not reported |
| Trosch et al., 2017 [28] | Prospective observational study (ANCHOR-CD registry); n = 304 | aboBoNT-A, mean dose: 504 U ± 229; median 500 U, range: 100–1500 U | TWSTRS total score decreased by 27.4% (± 28.9) from baseline to week 4, with a 31.7%, 18.5%, and 25.3% decrease in the TWSTRS severity, disability, and pain subscale scores, respectively. | Seventeen patients (5%) reported a total of 39 TEAEs. Of these patients, 2 with dysphagia and 1 with blurred vision and chewing difficulty withdrew from the study Most common TEAEs: dysphagia (n = 6, 1.7%), muscular weakness (n = 4, 1.2%), neck pain (n = 3, 0.9%), and rhinorrhea (n = 2, 0.6%) Of the 39 TEAEs, n = 31 (79.5%) were assumed related to study drug | Global improvement of change (via PGIC) as “much improved” or “very much improved” at week 4 after cycle 1 injection: 43.6% of patients Global satisfaction subscale of the modified TSQM measure at cycle 1, week 4: 48.7% |
| Bentivoglio et al., 2017 [29] | Retrospective cohort study; aboBoNT-A, n = 39 | Mean injected aboBoNT-A dose per session: 701.5 U (median, 560 U; range, 60–1560 U) | Tsui score, before treatment: 5.7 ± 1.8 points (range, 2‒11); maximum efficacy: 3.5 ± 1.5 points (range, 0‒9); p < 0.01 ≥2-point reduction in Tsui score in 70.9% of the treatments Mean latency: 6.4 ± 3.0 days (range, 1–30) Mean overall duration of the clinical improvement: 93 days (range, 0–300) Median inter-treatment interval: 131 days (95% CI: 87–191) | Most common TEAEs: posterior neck muscle weakness (15.1%), rigidity (2.7%), dysphagia (1.9%), injection-site pain (1.2%) | VAS, mean score before injection: 4.4 ± 1.8 (range 0–8); at maximum efficacy: 1.8 ± 1.6 (range 0–8); p < 0.01 CGA, mean for all treatments: 3.6 ± 1.0 (range 0–6) |
| Hefter et al., 2014 [30] | Retrospective cohort study, n = 568 | aboBoNT-A, overall dose not reported; mean dose in group with PSTF: 752 U ± 32; in group without PSTF: 703 U ± 56 | PSTF (≥4 Tsui scores collected during treatment with ≥3 consecutive aboBoNT-A injections): 5.8% of patients; estimated incidence: 1.6% per year (or 14.5% over 9 years) Time of onset of PSTF varied (e.g., after 4 injections, after 38 injections) | Not reported | Not reported |
| Dodel et al., 1997 [31] | Prospective, patients with CD, overall n = 362; aboBoNT-A, n not reported; onaBoNT-A, n not reported | Mean dose per treatment, aboBoNT-A: 732.3 U ± 239.5; onaBoNT-A: 187.3 U ± 68.0 | Onset of effect (days), aboBoNT-A: 9.4 ± 7.7; onaBoNT-A: 5.4 ± 3.1 Duration of effect (weeks), aboBoNT-A: 12.1 ± 5.0; onaBoNT-A: 11.3 ± 3.2 | Not reported separately for CD; overall AE rate, aboBoNT-A: 26%; onaBoNT-A: 15% (p < 0.001) | Patient-rated % response, aboBoNT-A: 64.4 ± 20.1; onaBoNT-A: 73.9 ± 13.6 |
| Finsterer et al., 1997 [32] | Prospective, invasive (EMG), n = 13 | aboBoNT-A, mean per treatment: 223 U (range: 140–320 U) | Turns/s (T/S), pre-injection: 411 (range, 201–746); post-injection: 289 (range, 101–868); p = 0.0001 Amplitude/turn (A/T), pre-injection: 304 µV (range, 137–500); post-injection: 202 µV (range 120–354 µV); p = 0.0001 | No severe side effects. Local and reversible hematoma in 1 patient | 12/13 patients reported a benefit from treatment at 4 weeks (“moderate” improvement, n = 4; “slight” improvement, n = 8; no change, n = 1) |
| Mohammadi et al., 2009 [33] | Database study, overall n = 207; aboBoNT-A, n = 163 onaBoNT-A, n = 44 | aboBoNT-A, mean dose, 389 U ± 144 onaBoNT-A; mean dose, 145 U ± 44 | Mean latency to response, aboBoNT-A: 7.6 ± 3.5 days; onaBoNT-A: 7.7 ± 3.3 days Duration of treatment effect, aboBoNT-A: 11 ± 1.6 weeks; onaBoNT-A: 10 ± 2.4 weeks | Most common side effects: neck muscle weakness (aboBoNT-A: 5%; onaBoNT-A: 7%); dysphagia, mild (aboBoNT-A: 8%; onaBoNT-A: 9%); injection-site pain (aboBoNT-A: 9%; onaBoNT-A: 6%) No severe or systemic side effects Secondary non-response, aboBoNT-A: 3.7%; onaBoNT-A: 4.5% | CGI, aboBoNT-A: 2.5 ± 0.3 weeks; onaBoNT-A: 2.2 ± 0.4 weeks; difference not statistically significant |
| Haussermann et al., 2004 [34] | Longitudinal cohort study, n = 90 | aboBoNT-A, mean per treatment session: 833 MU ± 339 | Secondary non-response in 3/90 patients during follow-up | ≥1 TEAE: n = 34 patients Most common TEAEs: neck weakness (n = 13 patients), mild dysphagia for food (n = 12), general weakness (n = 5) | >60% of patients were still being treated with aboBoNT-A after ≤12 years. Mean score, global subjective rating of effect (–4 = very bad, +4 = very good): 1.93 ± 1.18 |
| Marchetti et al., 2005 [35] | Retrospective observational study of patients switching, overall n = 70; from aboBoNT-A to onaBoNT-A, n = 63; from onaBoNT-A to aboBoNT-A, n = 7 | Mean dose, patients switching from aboBoNT-A to onaBoNT-A: aboBoNT-A, 601 ± 234 U; onaBoNT-A, 130 ± 44 U Mean dose, patients switching from onaBoNT-A to aboBoNT-A: aboBoNT-A, 468 ± 139 U; onaBoNT-A, 112 ± 30 U | Not reported | ≥1 TEAE: aboBoNT-A, n = 37 patients; onaBoNT-A, n = 22 patients Most common TEAEs: dysphagia (aboBoNT-A, n = 19 events; onaBoNT-A, n = 12 events), followed by flu-like symptoms (aboBoNT-A, n = 4 events; onaBoNT-A, n = 0 events) | Not reported |
| Rystedt et al., 2012 [36] | Retrospective study using patient casebook notes, n = 75 | onaBoNT-A then switch to aboBoNT-A Median dose, last 4 onaBoNT-A injections: 97.5 U (range 40–200); first 4 aboBoNT-A injections: 200 U (range 80–420) | Not reported | ≥1 TEAE, last 4 onaBoNT-A treatments: n = 4 patients (5.3%; dysphagia, n = 2; pain and dizziness, n = 2) ≥1 TEAE, first 4 aboBoNT-A treatments: n = 18 patients (24%; dysphagia, n = 8; neck weakness, n = 4; pain, n = 4; dizziness, n = 2; tremor, n = 1; nausea, n = 1) | Patients reporting more effective treatment after switching to aboBoNT-A: n = 12 (16%) Patients reporting worse effect after switching to aboBoNT-A: n = 4 (5%) Patients reporting not feeling any difference at all in effect: n = 59 (79%) |
| Vivancos-Matellano et al., 2012 [37] | Retrospective chart review, n = 37 | Mean dose: 487 U (range 320–650) | 97% of patients maintained treatment response | ≥1 TEAE: 8/37 patients treated with aboBoNT-A (9 TEAEs in total) Most common TEAE: dysphagia, n = 7 patients (18.9%); typically mild in severity One AE led to study discontinuation | Not reported |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fasano, A.; Paramanandam, V.; Jog, M. Use of AbobotulinumtoxinA in Adults with Cervical Dystonia: A Systematic Literature Review. Toxins 2020, 12, 470. https://doi.org/10.3390/toxins12080470
Fasano A, Paramanandam V, Jog M. Use of AbobotulinumtoxinA in Adults with Cervical Dystonia: A Systematic Literature Review. Toxins. 2020; 12(8):470. https://doi.org/10.3390/toxins12080470
Chicago/Turabian StyleFasano, Alfonso, Vijayashankar Paramanandam, and Mandar Jog. 2020. "Use of AbobotulinumtoxinA in Adults with Cervical Dystonia: A Systematic Literature Review" Toxins 12, no. 8: 470. https://doi.org/10.3390/toxins12080470
APA StyleFasano, A., Paramanandam, V., & Jog, M. (2020). Use of AbobotulinumtoxinA in Adults with Cervical Dystonia: A Systematic Literature Review. Toxins, 12(8), 470. https://doi.org/10.3390/toxins12080470