Biomonitoring of Multiple Mycotoxins in Urine by GC–MS/MS: A Pilot Study on Patients with Esophageal Cancer in Golestan Province, Northeastern Iran

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Results and Discussion
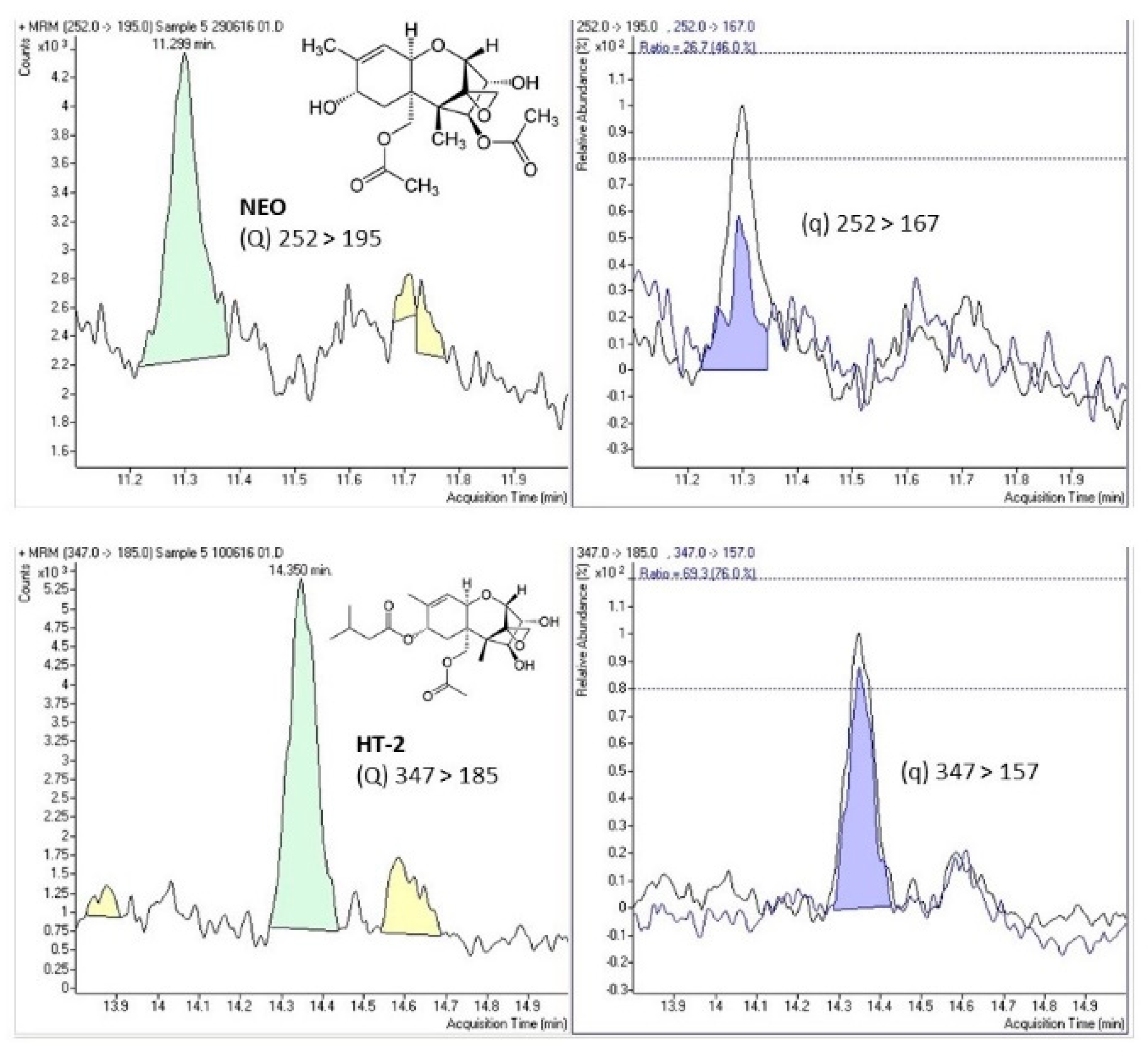
Sample Analyses
3. Conclusions
4. Material and Methods
4.1. Standards
4.2. Chemicals and Reagents
4.3. Sampling
4.4. Sample Preparation
4.4.1. Extraction
4.4.2. Derivatization
4.5. GC–MS/MS Analysis
4.6. Creatinine Analysis
4.7. Method Validation
4.8. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marin, S.; Ramos, A.J.; Cano-Sancho, G.; Sanchis, V. Mycotoxins: Occurrence, toxicology, and exposure assessment. Food Chem. Toxicol. 2013, 60, 218–237. [Google Scholar] [CrossRef]
- Oluwafemi, F.; Odebiyi, T.; Kolapo, A. Occupational aflatoxin exposure among feed mill workers in Nigeria. World Mycotoxin J. 2012, 5, 385–389. [Google Scholar] [CrossRef]
- Cortinovis, C.; Pizzo, F.; Spicer, L.J.; Caloni, F. Fusarium mycotoxins: Effects on reproductive function in domestic animals—A review. Theriogenology 2013, 80, 557–564. [Google Scholar] [CrossRef] [PubMed]
- El Khoury, A.; Atoui, A. Ochratoxin A: General overview and actual molecular status. Toxins 2010, 2, 461–493. [Google Scholar] [CrossRef] [Green Version]
- IARC. Monographs on the Evaluation of Carcinogenic Risks to Humans. Some Traditional Herbal Medicines, Some Mycotoxins, Naphthalene and Styrene; IARC Press: Lyon, France, 2002; Volume 82, pp. 1–556. [Google Scholar]
- Franco, L.T.; Petta, T.; Rottinghaus, G.E.; Bordin, K.; Gomes, G.A.; Alvito, P.; Assunção, R.; Oliveira, C.A.F. Assessment of mycotoxin exposure and risk characterization using occurrence data in foods and urinary biomarkers in Brazil. Food Chem. Toxicol. 2019, 128, 21–34. [Google Scholar] [CrossRef] [PubMed]
- Anukul, N.; Vangnai, K.; Mahakarnchanakul, W. Significance of regulation limits in mycotoxin contamination in Asia and risk management programs at the national level. J. Food Drug Anal. 2013, 21, 227–241. [Google Scholar] [CrossRef] [Green Version]
- Escrivá, L.; Font, G.; Manyes, L.; Berrada, H. Studies on the Presence of Mycotoxins in Biological Samples: An Overview. Toxins 2017, 9, 251. [Google Scholar] [CrossRef] [Green Version]
- Solfrizzo, M.; Gambacorta, L.; Warth, B.; White, K.; Srey, C.; Sulyok, M.; Krska, R.; Gong, Y.Y. Comparison of single and multi-analyte methods based on LC-MS/MS for mycotoxin biomarker determination in human urine. World Mycotoxin J. 2013, 6, 355–366. [Google Scholar] [CrossRef]
- Turner, P.C.; Flannery, B.; Isitt, C.; Ali, M.; Pestka, J. The role of biomarkers in evaluating human health concerns from fungal contaminants in food. Nutr. Res. Rev. 2012, 25, 162–179. [Google Scholar] [CrossRef] [Green Version]
- Warth, B.; Sulyok, M.; Krska, R. LC-MS/MS-based multibiomarker approaches for the assessment of human exposure to mycotoxins. Anal. Bioanal. Chem. 2013, 405, 5687–5695. [Google Scholar] [CrossRef] [Green Version]
- Muñoz, K.; Blaszkewicz, M.; Degen, G.H. Simultaneous analysis of ochratoxin A and its major metabolite ochratoxin alpha in plasma and urine for an advanced biomonitoring of the mycotoxin. J. Chrom. B 2010, 878, 2623–2629. [Google Scholar] [CrossRef]
- Escrivá, L.; Manyes, L.; Font, G.; Berrada, H. Mycotoxin Analysis of Human Urine by LC-MS/MS: A Comparative Extraction Study. Toxins 2017, 9, 330. [Google Scholar] [CrossRef] [Green Version]
- Roshandel, G.; Sadjadi, A.; Aarabi, M.; Keshtkar, A.; Sedaghat, S.M.; Nouraie, S.M.; Semnani, S.; Malekzadeh, R. Cancer incidence in Golestan province: Report of an ongoing population-based cancer registry in Iran between 2004 and 2008. Arch. Iran. Med. 2012, 15, 196–200. [Google Scholar]
- Kachala, R. Systematic review: Epidemiology of oesophageal cancer in Sub-Saharan Africa. Malawi. Med. J. 2010, 22, 65–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamangar, F.; Malekzadeh, R.; Dawsey, S.M.; Saidi, F. Esophageal cancer in Northeastern Iran: a review. Arch Iran Med. 2007, 10, 70–82. [Google Scholar]
- Xue, K.S.; Tang, L.; Sun, G.; Wang, S.; Hu, X.; Wang, J.S. Mycotoxin exposure is associated with increased risk of esophageal squamous cell carcinoma in Huaian area, China. BMC Cancer 2019, 19, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, F.; Cole, P.; Mi, Z.; Xing, L.Y. Corn and wheat-flour consumption and mortality from esophageal cancer in shanxi, China. Int. J. Cancer 1993, 53, 902–906. [Google Scholar] [CrossRef] [PubMed]
- Van Rensburg, S.J. Epidemiologic and dietary evidence for a specific nutritional predisposition to esophageal cancer. J. Natl. Cancer Inst. 1981, 67, 243–251. [Google Scholar] [PubMed]
- Kigen, G.; Busakhala, N.; Kamuren, Z.; Rono, H.; Kimalat, W.; Njiru, E. Factors associated with the high prevalence of oesophageal cancer in Western Kenya: A review. Infect. Agents Cancer 2017, 12, 59. [Google Scholar] [CrossRef] [Green Version]
- Simonato, L.; Franceschi, S.; Zambon, P. A population at high risk for esophageal cancer in the north-east of Italy. Mutat. Res. Rev. Mutat. 2000, 462, 355–363. [Google Scholar] [CrossRef]
- Come, J.; Cambaza, E.; Ferreira, R.; da Costa, J.M.C.; Carrilho, C.; Santos, L.L. Esophageal cancer in Mozambique: Should mycotoxins be a concern? Pan. Afr. Med. J. 2019, 33, 187. [Google Scholar] [CrossRef]
- Alizadeh, A.M.; Rohandel, G.; Roudbarmohammadi, S.; Roudbary, M.; Sohanaki, H.; Ghiasian, S.A.; Taherkhani, A.; Semnani, S.; Aghasi, M. Fumonisin B1 Contamination of Cereals and Risk of Esophageal Cancer in a High-Risk Area in Northeastern Iran. Asian. Pac. J. Cancer P 2012, 13, 2625–2628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghasemi-Kebria, F.; Joshaghani, H.; Taheri, N.S.; Semnani, S.; Aarabi, M.; Salamat, F.; Roshandel, G. Aflatoxin contamination of wheat flour and the risk of esophageal cancer in a high risk area in Iran. Cancer Epidemiol. 2013, 37, 290–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Ruyck, K.; Huybrechts, I.; Yang, S.; Arcella, D.; Claeys, L.; Abbeddou, S.; De Keyzer, W.; De Vries, J.; Ocke, M.; Ruprich, J.; et al. Mycotoxin exposure assessments in a multi-center European validation study by 24-h dietary recall and biological fluid sampling. Environ. Int. 2020, 137, 105539. [Google Scholar] [CrossRef]
- Warth, B.; Petchkongkaew, A.; Sulyok, M.; Krska, R. Utilising an LC-MS/MS-based multi-biomarker approach to assess mycotoxin exposure in the Bangkok metropolitan area and surrounding provinces. Food Add. Cont Part A 2014, 31, 2040–2046. [Google Scholar] [CrossRef] [PubMed]
- Gerding, J.; Cramer, B.; Humpf, H.U. Determination of mycotoxin exposure in Germany using an LC-MS/MS multibiomarker approach. Mol. Nutr. Food Res. 2014, 58, 2358–2368. [Google Scholar] [CrossRef] [PubMed]
- Abia, W.A.; Warth, B.; Sulyok, M.; Krska, R.; Tchana, A.N.; Njobeh, P.B.; Dutton, M.F.; Moundipa, P.F. Determination of multi-mycotoxin occurrence in cereals, nuts and their products in Cameroon by liquid chromatography tandem mass spectrometry (LC-MS/MS). Food Control 2013, 31, 438–453. [Google Scholar] [CrossRef]
- Wallin, S.; Hardie, L.J.; Kotova, N.; Warensjö, E.; Nälsén, C.; Ridefelt, P.; Turner, P.C.; White, K.L.M. Biomonitoring study of deoxynivalenol exposure and association with typical cereal consumption in Swedish adults. World Mycotoxin J. 2013, 6, 439–448. [Google Scholar] [CrossRef]
- Brera, C.; De Santis, B.; Debegnach, F.; Miano, B.; Moretti, G.; Lanzone, A.; G Del Sordo, G.; Buonsenso, D.; Chiaretti, A.; Hardie, L.; et al. Experimental study of deoxynivalenol biomarkers in urine. EFSA Supp. Publ. 2015, 12, 818E. [Google Scholar] [CrossRef] [Green Version]
- Turner, P.C.; Burley, V.J.; Rothwell, J.A.; White, K.L.; Cade, J.E.; Wild, C.P. Deoxynivalenol: Rationale for the development and application of urinary biomarker. Food Addit. Cont. Part A 2008, 25, 864–871. [Google Scholar] [CrossRef] [Green Version]
- Solfrizzo, M.; Gambacorta, L.; Visconti, A. Assessment of multi-mycotoxin exposure in southern Italy by urinary multi-biomarker determination. Toxins 2014, 6, 523–538. [Google Scholar] [CrossRef]
- Rodríguez-Carrasco, Y.; Moltó, J.C.; Mañes, J.; Berrada, H. Exposure assessment approach through mycotoxin/creatinine ratio evaluation in urine by GC-MS/MS. Food Chem. Toxicol. 2014, 72, 69–75. [Google Scholar] [CrossRef]
- Vidal, A.; Bouzaghnane, N.; De Saeger, S.; De Boevre, M. Human Mycotoxin Biomonitoring: Conclusive Remarks on Direct or Indirect Assessment of Urinary Deoxynivalenol. Toxins 2020, 12, 139. [Google Scholar] [CrossRef] [Green Version]
- Martins, C.; Vidal, A.; De Boevre, M.; De Saeger, S.; Nunes, C.; Torres, D.; Goios, A.; Lopes, C.; Assunção, R.; Alvito, P. Exposure assessment of Portuguese population to multiple mycotoxins: The human biomonitoring approach. Int. J. Hyg. Environ. Health 2019, 222, 913–925. [Google Scholar] [CrossRef]
- Shephard, G.S.; Burger, H.M.; Gambacorta, L.; Gong, Y.Y.; Krska, R.; Rheeder, J.P.; Solfrizzo, M.; Srey, C.; Sulyok, M.; Visconti, A.; et al. Multiple mycotoxin exposure determined by urinary biomarkers in rural subsistence farmers in the former Transkei, South Africa. Food Chem. Toxicol. 2013, 62, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Fan, K.; Xu, J.; Jiang, K.; Liu, X.; Meng, J.; Di Mavungu, J.D.; Guo, W.; Zhang, Z.; Jing, J.; Li, H.; et al. Determination of multiple mycotoxins in paired plasma and urine samples to assess human exposure in Nanjing, China. Environ. Polut. 2019, 248, 865–873. [Google Scholar] [CrossRef]
- Turner, P.C.; Gong, Y.Y.; Pourshams, A.; Jafari, E.; Routledge, M.N.; Malekzadeh, R.; Wild, C.P.; Boffetta, P. A pilot survey for Fusarium mycotoxin biomarkers in women from Golestan northern Iran. World Mycotoxin J. 2012, 5, 195–199. [Google Scholar] [CrossRef]
- De Santis, B.; Debegnach, F.; Miano, B.; Moretti, G.; Sonego, E.; Chiaretti, A.; Buonsenso, D.; Brera, C. Determination of Deoxynivalenol Biomarkers in Italian Urine Samples. Toxins 2019, 11, 441. [Google Scholar] [CrossRef] [Green Version]
- Wallin, S.; Gambacorta, L.; Kotova, N.; Lemming, E.W.; Nälsén, C.; Solfrizzo, M.; Olsen, M. Biomonitoring of concurrent mycotoxin exposure among adults in Sweden through urinary multi-biomarker analysis. Food Chem. Toxicol. 2015, 83, 133–139. [Google Scholar] [CrossRef]
- Cunha, S.C.; Fernandes, J.O. Development and validation of a gas chromatography–mass spectrometry method for determination of deoxynivalenol and its metabolites in human urine. Food Chem. Toxicol. 2012, 50, 1019–1026. [Google Scholar] [CrossRef]
- Domijan, A.M.; Peraica, M.; Vrdoljak, A.L.; Radić, B.; Zlender, V.; Fuchs, R. The involvement of oxidative stress in ochratoxin A and fumonisin B 1 toxicity in rats. Mol. Nut. Food Res. 2007, 51, 1147–1151. [Google Scholar] [CrossRef]
- Johnson, N.M.; Qian, G.; Xu, L.; Tietze, D.; Marroquin-Cardona, A.; Robinson, A.; Rodriguez, M.; Kaufman, L.; Cunningham, K.; Wittmer, J.; et al. Aflatoxin and PAH exposure biomarkers in a U.S. population with a high incidence of hepatocellular carcinoma. Sci. Total Environ. 2010, 408, 6027–6031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Njumbe Ediage, E.; Di Mavungu, J.D.; Song, S.; Wu, A.; Van Peteghem, C.; De Saeger, S. A direct assessment of mycotoxin biomarkers in human urine samples by liquid chromatography tandem mass spectrometry. Anal. Chim. Acta 2012, 741, 58–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Commission. Guidance Document on Identification of Mycotoxins in Food and Feed. SANTE/12089 /2016. 2016. Available online: https://ec.europa.eu/food/sites/food/files/safety/docs/cs_contaminants_sampling_guid-doc-ident-mycotoxins.pdf (accessed on 1 January 2017).



{kind=link}
{kind=link}
| Population Group | Parameters | DON | NEO | T-2 | HT-2 |
|---|---|---|---|---|---|
| Control (n = 10) | Positive samples | 1 | 4 | - | 1 |
| Incidence (%) | 10 | 40 | - | 10 | |
| Min ± SD (µg/L) | - | 10.57 ± 0.33 | - | - | |
| Max ± SD (µg/L) | - | 22.53 ± 2.39 | - | ||
| Mean ± SD (µg/L) | 8.42 ± 1.21 | 14.15 ± 5.72 | - | 23.97 ± 9.97 | |
| Corrected mean (µg/g creat) | 5.90 | 10.45 | - | 16.81 | |
| Esophageal cancer (n = 17) | Positive samples | - | 1 | 1 | 3 |
| Incidence (%) | - | 5.8 | 5.8 | 17.6 | |
| Min ± SD (µg/L) | - | - | - | 18.91 ± 3.05 | |
| Max ± SD (µg/L) | - | - | - | 50.38 ± 22.54 | |
| Mean ± SD (µg/L) | - | 12.90 ± 3.87 | 50.09 ± 7.51 | 36.52 ± 16.07 | |
| Corrected mean (µg/g creat) | - | 9.09 | 44.70 | 29.09 |
| Mycotoxin(s) | Incidence (%) | Sample Group | Ʃ Mycotoxin Concentrations (µg/L) | Ʃ Mycotoxin Concentrations (µg/g Creatinine) |
|---|---|---|---|---|
| Binary Combination | ||||
| NEO/HT-2 | 1/27 (3.7) | Case | 63.27 | 44.58 |
| T2/HT-2 | 1/27 (3.7) | Case | 90.38 | 79.13 |
| Ternary Combination | ||||
| DON/NEO/HT2 | 1/27 (3.7) | Control | 42.82 | 30.04 |
| Mycotoxin | RT (min) | Quantitation Transition (CE, eV) | Quantitation Transition Dt (ms) | Confirmation Transition (Collision Energy, eV) | Confirmation Transition Dt (ms) | Ion Ratio (%) |
|---|---|---|---|---|---|---|
| DON | 8.39 | 392 > 259 (10) | 25 | 407 > 197 (10) | 25 | 41.6 |
| 3-ADON | 9.40 | 392 > 287 (5) | 35 | 467 > 147 (10) | 25 | 47.5 |
| 15-ADON | 9.58 | 392 > 217 (20) | 35 | 392 > 184 (20) | 20 | 35.5 |
| FUS-X | 9.484 | 450 > 260 (10) | 35 | 450 > 245 (20) | 35 | 11.9 |
| NIV | 9.867 | 289 > 73 (15) | 35 | 379 > 73 (15) | 35 | 29.6 |
| NEO | 11.22 | 252 > 195 (10) | 25 | 252 > 167 (15) | 35 | 40.6 |
| T-2 | 13.891 | 399 > 109 (10) | 25 | 399 > 123 (15) | 35 | 81.9 |
| HT-2 | 14.334 | 347 > 185 (10) | 25 | 347 > 157 (10) | 25 | 86.7 |
| ZAN | 14.669 | 449 > 335 (15) | 25 | 307 > 235 (10) | 25 | 59.9 |
| ZON | 15.387 | 462 >333 (20) | 25 | 462 > 151 (20) | 25 | 99.7 |
| Mycotoxin | Linearity (r2) | LOD (µg/L) | LOQ (µg/L) | Matrix Effect (% SSE) | Recovery Range (%) | Intraday Precision Range (%RSD) | Interday Precision Range (%RSD) |
|---|---|---|---|---|---|---|---|
| DON | 0.996 | 0.12 | 0.25 | 23 | 88−97 | 2−4 | 8−10 |
| 3-ADON | 0.992 | 0.25 | 0.5 | 27 | 84−102 | 1−9 | 4−11 |
| 15-ADON | 0.991 | 0.25 | 0.5 | 28 | 77−91 | 2−10 | 3−12 |
| FUS-X | 0.992 | 2 | 4 | 12 | 83−95 | 3−6 | 6−13 |
| NIV | 0.996 | 0.5 | 1 | 6 | 82−95 | 3−7 | 4−7 |
| NEO | 0.999 | 0.25 | 0.5 | 36 | 93−109 | 5−7 | 3−11 |
| T-2 | 0.998 | 0.5 | 1 | 8 | 89−104 | 4−5 | 8−10 |
| HT-2 | 0.999 | 1 | 2 | 28 | 92−105 | 1−6 | 6−9 |
| ZAN | 0.993 | 4 | 8 | 36 | 72−80 | 2−5 | 5−12 |
| ZON | 0.991 | 3 | 6 | 23 | 79−96 | 6−7 | 8−11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niknejad, F.; Escrivá, L.; Adel Rad, K.B.; Khoshnia, M.; Barba, F.J.; Berrada, H. Biomonitoring of Multiple Mycotoxins in Urine by GC–MS/MS: A Pilot Study on Patients with Esophageal Cancer in Golestan Province, Northeastern Iran. Toxins 2021, 13, 243. https://doi.org/10.3390/toxins13040243
Niknejad F, Escrivá L, Adel Rad KB, Khoshnia M, Barba FJ, Berrada H. Biomonitoring of Multiple Mycotoxins in Urine by GC–MS/MS: A Pilot Study on Patients with Esophageal Cancer in Golestan Province, Northeastern Iran. Toxins. 2021; 13(4):243. https://doi.org/10.3390/toxins13040243
Chicago/Turabian StyleNiknejad, Farhad, Laura Escrivá, Khoda Berdi Adel Rad, Masoud Khoshnia, Francisco J. Barba, and Houda Berrada. 2021. "Biomonitoring of Multiple Mycotoxins in Urine by GC–MS/MS: A Pilot Study on Patients with Esophageal Cancer in Golestan Province, Northeastern Iran" Toxins 13, no. 4: 243. https://doi.org/10.3390/toxins13040243
APA StyleNiknejad, F., Escrivá, L., Adel Rad, K. B., Khoshnia, M., Barba, F. J., & Berrada, H. (2021). Biomonitoring of Multiple Mycotoxins in Urine by GC–MS/MS: A Pilot Study on Patients with Esophageal Cancer in Golestan Province, Northeastern Iran. Toxins, 13(4), 243. https://doi.org/10.3390/toxins13040243