3.1. Validation of Junction Pressure and Estimation of Correction Factor
To quantify the contribution of RBCs to blood flow, it was necessary to obtain two mechanical properties (i.e., blood viscosity and junction pressure). Here, both blood properties were obtained by analyzing the interface in the coflowing channel.
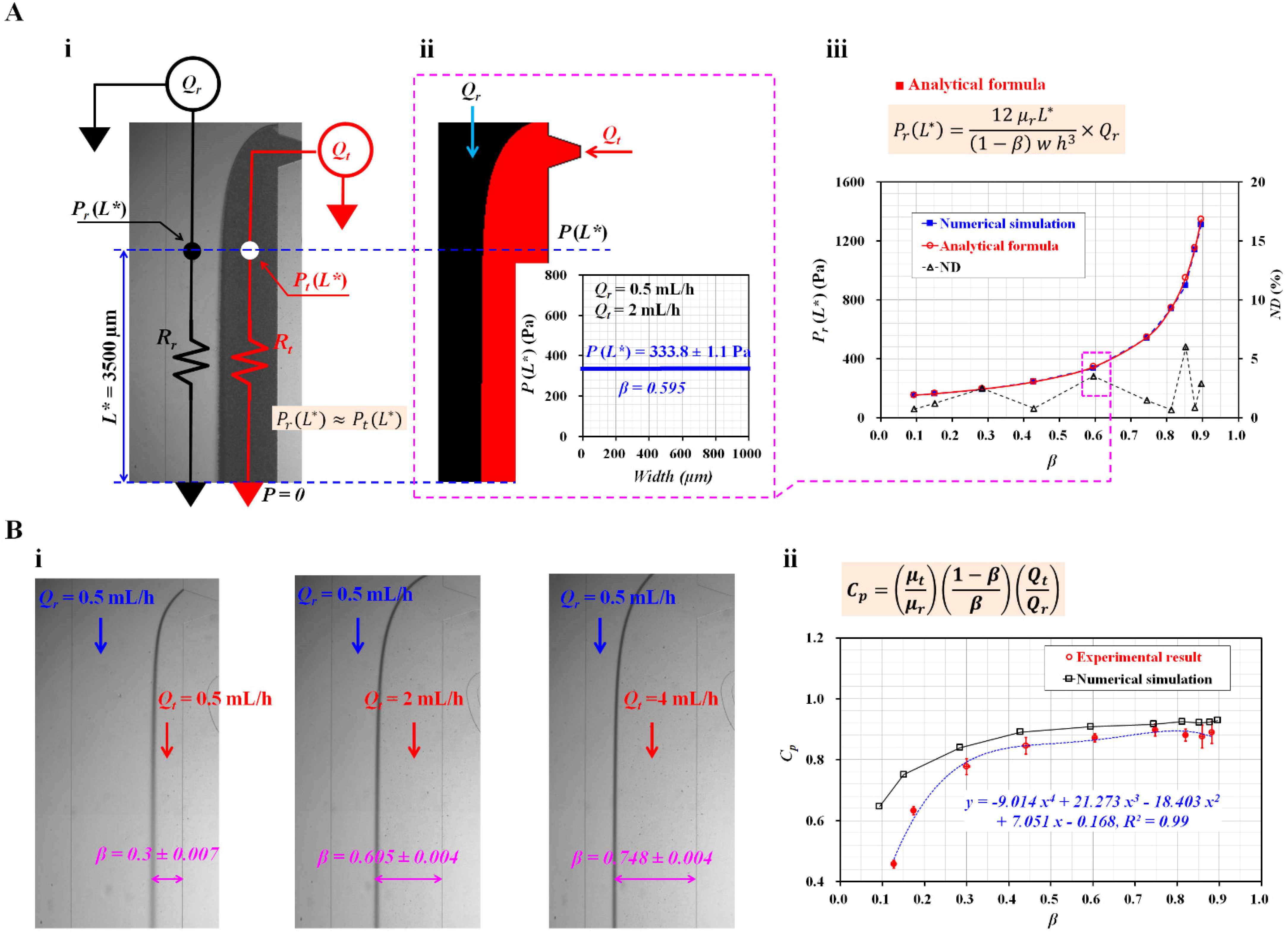
Figure 2(A-i) shows the discrete fluidic circuit model of the two fluids partially flowing in the coflowing channel. The coflowing channel was represented by two fluidic resistances (
Rr,
Rt) connected in parallel. The flow rates of the reference and test fluids were denoted as
Qr and
Qt, respectively. The junction pressure at a distance (
L* = 3500 µm) from the outlet (or the ground) was denoted as
Pr (
L*) for the reference fluid stream and
Pt (
L*) for the test fluid stream. According to a previous study [
27], the analytical expression for each junction pressure is given as:
In Equation (2), the correction factor (
CP) was used to compensate for the difference between the real physical boundary and the mathematical modeling boundary.
µr and
µt denoted viscosities of reference fluid and test fluid, respectively. Additionally, w represented the channel width of the coflowing channel. As the coflowing channel had straight and rectangular channels, both streams had the same pressure (i.e.,
Pr (
L*) ≈
Pt (
L*)). Based on Equations (1) and (2), the correction factor (
CP) was derived as:
To validate the analytical expressions for the junction pressure (i.e., Equations (1) and (2)), numerical simulations were conducted using a commercial software (CFD-ACE+, Ver. 2021, ESI Group, Paris, France). The test and reference fluids were selected as 1× PBS and 30% glycerin solutions, respectively. The corresponding viscosities of each fluid were assumed to be
µr = 3 cP (reference fluid) and
µt = 1 cP (test fluid) [
28]. The flow rate of each fluid was set to
Qr = 0.5 mL/h and
Qt = 2 mL/h.
Figure 2(A-ii) shows the interface in the coflowing channel. The right panel shows the variations in
P(
L*) along the channel width. As expected, the junction pressure remained unchanged along the channel width. Both the streams had the same junction pressure at a specific location. The junction pressure and interface were obtained as
P(
L*) = 333.8 ± 1.1 Pa and
β = 0.595, respectively. For convenience, the junction pressure without a correction factor (
CP) (i.e., Equation (1)) was employed to validate the analytical expression in the coflowing channel.
Figure 2(A-iii) shows the variations in
Pr (
L*) obtained by the numerical simulation and the analytical formula with respect to
β. The normalized difference (ND, Δ) was obtained by comparing the junction pressures obtained by the numerical simulation (■) and the analytical formula (○). The results indicate that the junction pressure increased significantly when the interface moved from the left wall (
β = 0) to the right wall (
β = 1). It increased significantly from 154 to 1346 Pa. In addition, ND was less than 6% when the interface was located from
β = 0.1 to
β = 0.9. From the results, Equation (1) could be used to obtain the junction pressure in the coflowing channel consistently.
To obtain blood viscosity in the coflowing channel, it was necessary to obtain the correction factor (
CP) with the experimental approach. The flow rate of the reference fluid was set at 0.5 mL/h. According to a previous study [
29], the correction factor was influenced by the sectional dimensions of the rectangular channel (i.e., width, depth), and the reference fluid. Thus, it was necessary to recalculate the correction factor. Here, the microfluidic channel was newly designed, and a 30% glycerin solution was selected as the reference fluid. PBS (1×) was used as the test fluid.
Figure 2(B-i) shows the captured microscopic images for representing the variations in the interface with respect to the flow rate of the test fluid (
Qt) (
Qt = 0.5, 2, and 4 mL/h). The corresponding interfaces of each flow rate were obtained as
β = 0.3 ± 0.007 (
Qt = 0.5 mL/h), 0.605 ± 0.004 (
Qt = 2 mL/h), and 0.748 ± 0.004 (
Qt = 4 mL/h). Using Equation (3),
CP was then calculated at various flow rates of the test fluid.
Figure 2(B-ii) shows the
CP from the numerical simulation (□) and experiments (○) with respect to
β. The
CP tended to decrease when the interface was located near the left wall. At
β < 0.3, there was a significant deviation between the simulated and experimental results. However, the
CP increased gradually at
β > 0.4. There was a slight difference between these results. Here, based on the variations in
CP obtained from the experimental results, a linear regression technique (EXCEL
TM, Microsoft, Redmond, WA, USA) was conducted to obtain the polynomial expression for
CP as a function of
β. The linear regression analysis gave a correction factor as
Cp = −9.014
β4 + 21.273
β3 − 18.403
β2 + 7.051
β − 0.168 (
R2 = 0.99). By substituting the polynomial expression of
CP into Equation (3), the analytical formula of the viscosity of test fluid is given as:
The blood viscosity was then obtained by substituting the interface (β) into Equation (4).
3.2. Contributions of RBC Sedimentation for Control Blood
In previous studies, a driving blood syringe was set in the vertical direction (i.e., upright or inverted). In addition, the hematocrit was set to relatively lower levels than the normal level of 45% (i.e., 0.1% [
17], 20% [
11], 25% [
30], and 30% [
21,
31]). The hematocrit of the blood tended to increase over time when the blood was supplied from the bottom region of the syringe into the microfluidic device. However, in this study, the blood syringe was set in the horizontal direction. It was expected that the RBC sedimentation might exhibit different patterns over time because of the different installation direction of the blood syringe. The hematocrit of the blood tended to decrease continuously over time after the blood entered the microfluidic channel. Here, instead of RBC aggregation-enhanced blood, control blood was tested to evaluate the contributions of hematocrit to blood flow under RBC sedimentation of the control blood in the blood syringe. The hematocrit of the control blood was adjusted to Hct = 20%, 25%, 30%, and 40% by adding normal RBCs into autologous plasma. The contributions of the hematocrits were evaluated experimentally by changing the hematocrit level, in which the diluent was fixed to the same plasma.
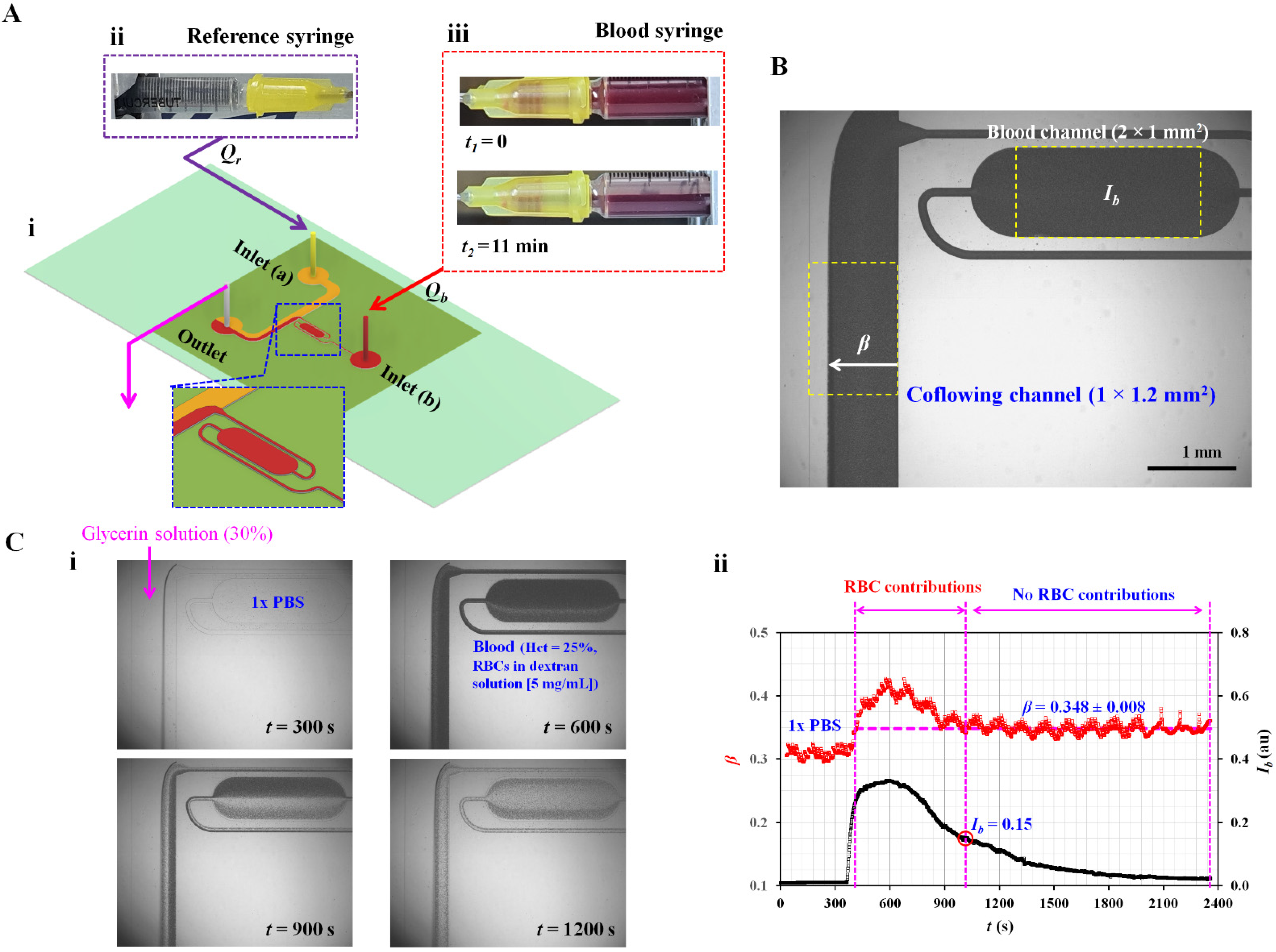
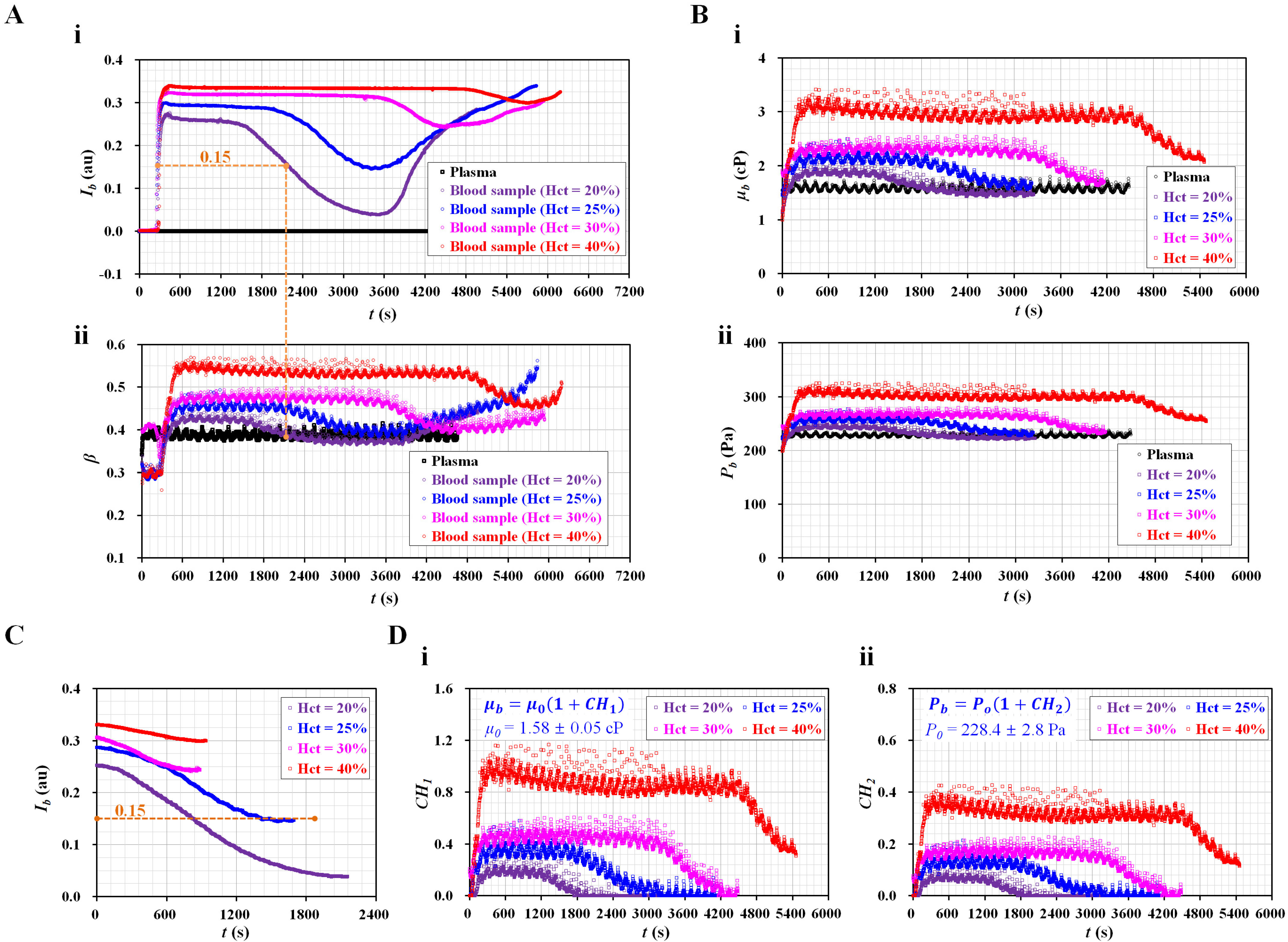
Figure 3(A-i) shows the temporal variations in
Ib with respect to Hct. Consequently,
Ib remained for a certain duration after the blood entered the blood channel. The value of flat
Ib increased substantially at higher levels of Hct ranging from 20% to 30%. A smaller difference was observed between Hct = 30% and Hct = 40%. The period of flat
Ib increased gradually with increasing Hct ranging from 20% to 40%. As shown in
Figure 1(A-iii), RBC sedimentation caused a decrease in
Ib because the hematocrit decreased over time. Pure plasma had a zero value of
Ib. When the minimum value of
Ib was greater than zero, RBCs still flowed into the blood channel, even for blood (Hct = 20%). The minimum value of
Ib tended to increase at higher hematocrit values. After the diluent flowed into the blood channel for a certain duration, the RBCs entered the channel again. This caused
Ib to increase gradually over time.
Figure 3(A-ii) shows the temporal variations in
β with respect to Hct. The interface (
β) exhibited trends similar to those of
Ib. Specifically,
β tended to increase at higher levels of hematocrit. The period of flat
β increased at a higher hematocrit. Interestingly, the two blood types (i.e., Hct = 20% and 25%) had minimum β similar to that of pure plasma (i.e., RBC-free diluent). As shown in
Figure 3(A-i), when
Ib decreased to less than 0.15, the RBCs did not contribute to varying the
β. Namely, small populations of RBCs (i.e., extremely lower hematocrit) did not have an influence on the interface in the coflowing channel. For that reason, when small RBCs or RBC-free diluent came into the coflowing channel, the
β decreased to the same value of β for pure plasma. However, when the blood syringe was filled with blood with higher levels of hematocrit, ESR occurred over time. Diluent was not separated completely from blood during the ESR in the syringe. Thus, large populations of RBCs came into the microfluidic device. The minimum
β had higher than that of plasma. Although the minimum value of
Ib increased significantly at higher Hct values,
β did not exhibit a substantial difference (i.e.,
Ib < 0.15). Based on the threshold of image intensity (i.e.,
Ib = 0.15), it was possible to separate the contributions of RBCs (
Ib > 0.15) and diluents (
Ib < 0.15) by analyzing the temporal variations in
β.
Figure 3(B-i) shows the temporal variations in blood viscosity (
µb) with respect to Hct. As expected,
µb increased significantly at higher levels of Hct. After the period of constant blood viscosity, RBC sedimentation caused a decrease in
µb over time. After an elapse of a certain time, the diluent was removed from the blood. Then, the diluents of the two blood samples (Hct = 20%, 25%) flowed into the coflowing channel. The viscosity of the diluent (i.e., plasma) exhibited similar values for two bloods:
µ0 = 1.58 ± 0.05 cP. By substituting the temporal variations in
β (
Figure 3(A-ii)) into Equation (1), the blood junction pressure was then obtained with respect to the hematocrit.
Figure 3(B-ii) shows the temporal variations in blood junction pressure (
Pb) with respect to Hct. The
Pb gradually increased at a higher level of hematocrit. RBC sedimentation resulted in decreasing
Pb significantly. When the two blood diluents (Hct = 20% and 25%) flowed into the coflowing channel, both diluents (i.e., plasma) had the same junction pressure of
P0 = 228.4 ± 2.8 Pa. From these results, the contributions of the RBCs and diluent were determined, especially for the control blood with low hematocrit (Hct = 20% or 25%). In other words, it would be necessary for the control blood to be adjusted to a low hematocrit to obtain viscosity or junction pressure for the diluent and RBCs.
Based on conventional quantification [
18],
Ib was recollected from the time at which it began to decrease to the time when it tended to increase again.
Figure 3C shows the temporal variations in
Ib with respect to the hematocrit. As expected, the blood with a low hematocrit contributed significantly to decreasing
Ib over time. RBC sedimentation decreased with increasing Hct, ranging from 20% to 40%. However, blood flow (
Ib < 0.15) did not affect the contribution of RBCs to the mechanical properties (i.e., viscosity, junction pressure). When
Ib was greater than 0.15, the two blood samples (Hct = 20%, 25%) exhibited similar trends in
Ib. For the remaining two blood samples (Hct = 30%, 40%), the variation in
Ib decreased at a higher level of hematocrit. Thus, to consider the contribution of RBCs in the blood in terms of
Ib, it is necessary to select suitable data for quantifying RBC sedimentation. However, as shown in
Figure 3(A-i), before
Ib began to decrease, it remained unchanged over time (i.e.,
Ib > 0.15). The period of flat image intensity (i.e.,
TESR) tended to increase with increasing hematocrit [
32]. Thus, it would be better to quantify RBC sedimentation compared with conventional quantification (
IESR) [
32]. As a limitation,
Ib did not provide enough information on the hematocrit from a mechanical point of view.
To quantify RBC sedimentation in the blood syringe, blood viscosity and junction pressure were obtained by analyzing the interface in the coflowing channel. Based on Einstein’s empirical expression for rigid spheres (i.e.,
µ =
µf [1 + 2.5 Φ];
µf: the viscosity of the suspending fluid, and Φ: the volume fraction) [
33], two formulas (i.e.,
µb =
µ0 [1 +
CH1] and
Pb =
P0 [1 +
CH2]) were suggested to evaluate the contributions of hematocrit and diluent in terms of blood viscosity and blood junction pressure. Here, the subscripts
b and
o denote blood and plasma (or RBC-free diluent), respectively. Namely,
µ0 and
P0 denoted viscosity and pressure of the diluent, respectively. The effect of the hematocrit on blood flow was evaluated using two coefficients (
CH1 and
CH2). Here, the image intensity of the blood flow should be greater than 0.15. Otherwise, for
Ib < 0.15,
CH1 = 0 and
CH2 = 0.
Figure 3(D-i) shows the temporal variations in
CH1 with respect to Hct. As a result, the four types of blood had significantly different trends for
CH1 when compared with
Ib (
Figure 3C). In addition,
CH1 tended to increase at a higher level of Hct.
Figure 3(D-ii) shows the temporal variations in
CH2 with respect to Hct. The
CH2 exhibited similar variations in
CH1. In conclusion, the two coefficients (
CH1,
CH2) provided quantitative information on RBC sedimentation in the blood syringe in terms of blood viscosity and blood junction pressure.
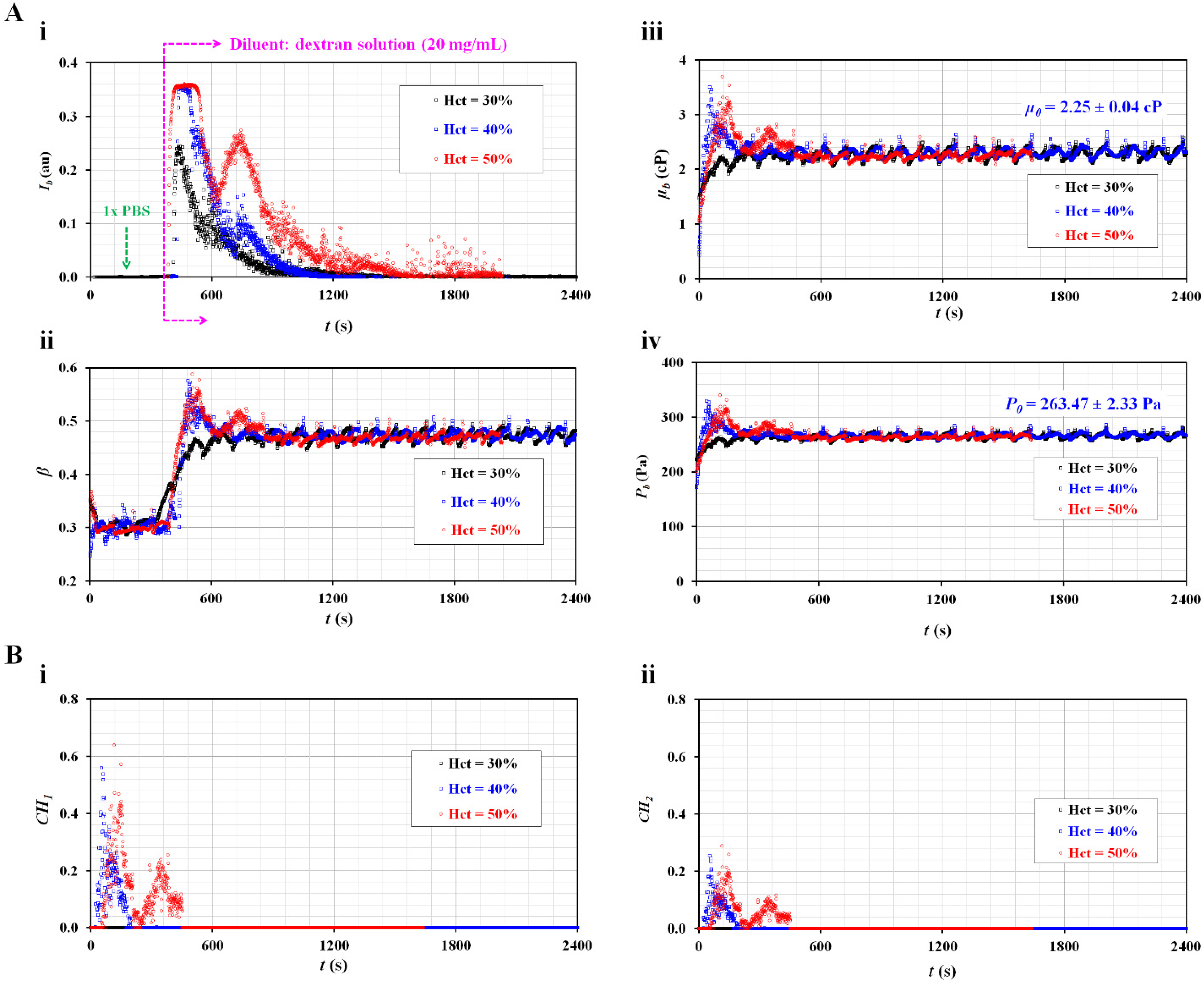
3.3. Contributions of RBC Sedimentation for Maximum RBC-Aggregated Blood
To accelerate RBC sedimentation in the blood syringe, the dextran solution was added into normal blood. Based on previous studies on physiological and pathological conditions [
2,
34], the maximum concentration of dextran solution was set at 20 mg/mL. To determine the contribution of hematocrit, the hematocrit was adjusted to Hct = 30%, 40%, and 50% by adding normal RBCs to the allowable concentration of the dextran solution.
Figure 4(A-i) shows the temporal variations in
Ib with respect to Hct.
Ib increased substantially when the blood flowed into the blood channel. Thereafter, RBC sedimentation significantly caused a decrease in
Ib over time. When compared with the control blood (
Figure 3(A-i)), the dextran solution caused a considerable decrease in the duration of flat image intensity. The
Ib of the blood (Hct = 30%) decreased substantially over time without a flat image intensity. That is, the
Ib decreased substantially at lower hematocrits.
Figure 4(A-ii) shows the temporal variations in
β with respect to Hct. The
β of the blood (Hct = 30%) reached a steady value without a peak. Blood RBCs did not have an influence on the blood flow. However, the remaining two blood samples (Hct = 40% and 50%) had peak values of
β. RBCs in the blood caused an increase in
β. However, the
β reached a steady value early.
Figure 4(A-iii) shows the temporal variations in
µb with respect to Hct. Within a specific time, when the image intensity was less than 0.15, the viscosity of the diluent was
µ0 = 2.25 ± 0.04 cP.
As shown in
Figure 4(A-ii), the blood viscosity increased for a short period for the two blood samples (Hct = 40%, 50%). The viscosity of blood (Hct = 30%) was the same as that of the diluent (C
dex = 20 mg/mL).
Figure 4(A-iv) shows the temporal variations in
Pb with respect to Hct. The junction pressure of the diluent was determined to be
P0 = 263.47 ± 2.33 Pa. The trends of
Pb were similar to those of
µb.
Based on the temporal variations in
µb and
Pb as shown in
Figure 4(A-iii, A-iv), the two coefficients (
CH1 and
CH2) were obtained over time.
Figure 4(B-i) shows the temporal variations in
CH1 with respect to Hct.
CH1 remained zero for the blood (Hct = 30%). However, the
CH1 of the blood (Hct = 50%) was higher than that of the blood (Hct = 40%).
Figure 4(B-ii) shows the temporal variations in
CH2 with respect to Hct. Consequently, the variation in
CH2 was similar to that of
CH1. The results indicate that blood (Hct = 40% or 50%) exhibited the effects of RBC sedimentation when RBCs were added into a specific concentration of dextran solution (20 mg/mL). However, blood (Hct = 30%) was not found to be effective for detecting the contributions of RBC sedimentation in blood syringes. In the succeeding experiments, the hematocrit was set to 50% by adding RBCs into dextran solutions of various concentrations.
3.4. Quantitative Comparison between the Proposed and Conventional Methods for RBC Aggregation-Enhanced Blood
Based on the quantitative results as discussed above, the present method was applied to measure the contributions of RBC sedimentation for various concentrations of dextran solution, which has been commonly used to enhance RBC sedimentation or RBC aggregation in blood. By referring to previous studies [
2,
34], five different kinds of dextran solution were prepared by setting the concentration of dextran solution to C
dex = 5, 7.5, 10, 15, and 20 mg/mL. Based on contributions of hematocrit to ESR, as shown in
Figure 4, the hematocrit of each blood was adjusted to 50% by adding normal RBCs to individual dextran solutions. The flow rates of the two fluids were set to 0.5 mL/h.
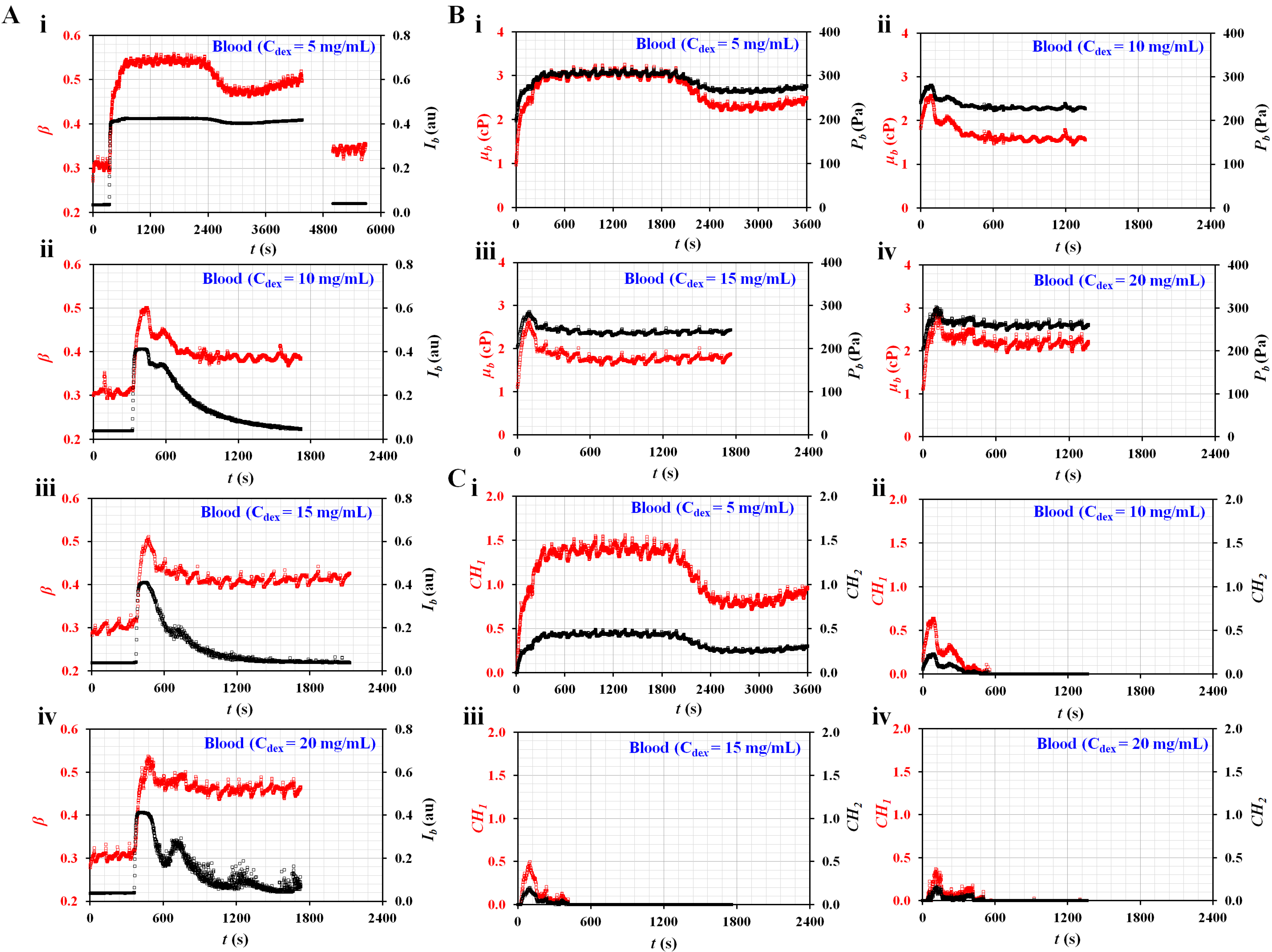
Figure 5A shows the temporal variations in
Ib and
β with respect to the concentrations of dextran solution (C
dex) ((i) C
dex = 5 mg/mL, (ii) C
dex = 10 mg/mL, (iii) C
dex = 15 mg/mL, and (iv) C
dex = 20 mg/mL). Here, the
Ib of the blood (C
dex = 5 mg/mL) did not decrease below 0.15. Thus, after the experiment, a dextran solution without RBCs (C
dex = 5 mg/mL) was tested to obtain
Ib and
β over time. Variations in
β and
Ib were added after
t = 4800 s. It was then possible to obtain
µ0 and
P0 of the diluent (i.e., C
dex = 5 mg/mL). However, the remaining blood samples were separated into blood and diluent. After an elapse of a certain time, the
Ib of each blood decreased to below 0.15. The
µ0 and
P0 of each blood were obtained by analyzing the temporal variations of
β, which remained unchanged over time.
Figure 5B shows the temporal variations in
µb and
Pb with respect to C
dex ((i) C
dex = 5 mg/mL, (ii) C
dex = 10 mg/mL, (iii) C
dex = 15 mg/mL, and (iv) C
dex = 20 mg/mL). Except for the blood (C
dex = 5 mg/mL), the dextran solution contributed to accelerating RBC sedimentation substantially. The viscosity and junction pressure had an early peak value. They remained unchanged for a long time.
Figure 5C shows the temporal variations in
CH1 and
CH2 with respect to C
dex ((i) C
dex = 5 mg/mL, (ii) C
dex = 10 mg/mL, (iii) C
dex = 15 mg/mL, and (iv) C
dex = 20 mg/mL). As a result, the blood (C
dex = 5 mg/mL) had higher values of
CH1 and
CH2 for a longer period than the other bloods. The dextran solution contributed to accelerating RBC sedimentation in the blood syringe. Furthermore, the two coefficients (
CH1 and
CH2) calculated from viscosity and junction pressure exhibited distinctive trends with respect to the concentration of the dextran solution.
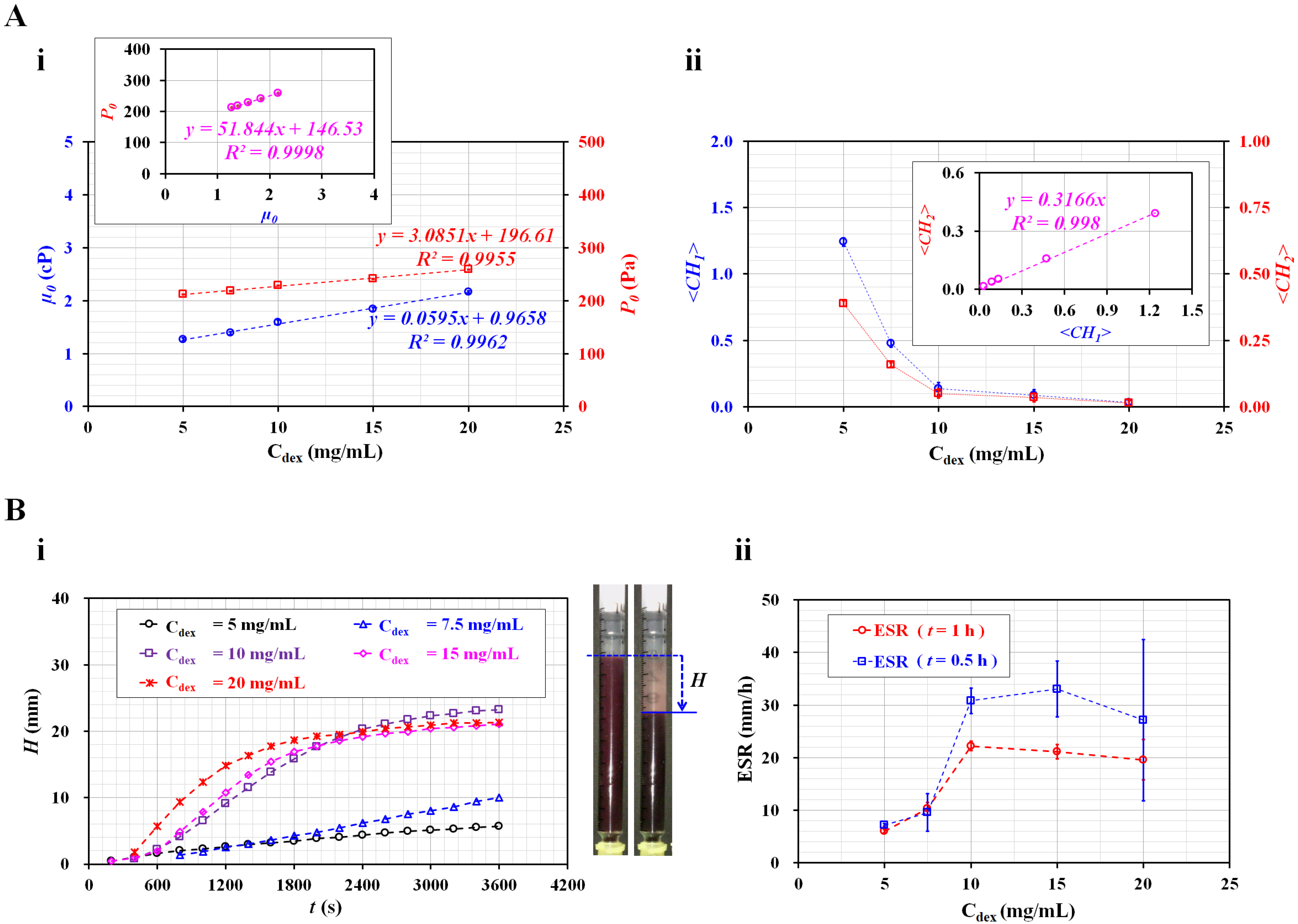
Figure 6A summarizes the variations in four parameters (i.e.,
µ0,
P0, <
CH1>, and <
CH2>) with respect to C
dex. Here, <
CH1> and <
CH2> denote the arithmetic averages of
CH1 and
CH2 obtained for
t = 1500 s (i.e.,
n = 1500).
Figure 6(A-i) shows the variations in
µ0 and
P0 of the diluent with respect to C
dex. Viscosity increased linearly with respect to C
dex (
µ0 = 0.0595 C
dex + 0.9658,
R2 = 0.9962). In addition, the junction pressure increased linearly with respect to C
dex (
P0 = 3.0851 C
dex + 196.61,
R2 = 0.9955). The inset shows a scatter plot for evaluating the linear relationship between
P0 and
µ0. As the coefficient of linear regression had a higher value of
R2 = 0.9998, either
P0 or
µ0 can be used effectively to detect differences in the diluent (i.e., concentration of dextran solution).
Figure 6(A-ii) shows the variations in <
CH1> and <
CH2> with respect to C
dex. Both coefficients exhibited consistent variations with respect to C
dex. They decreased substantially between C
dex = 5 and 10 mg/mL. For blood with a higher concentration of C
dex = 10 mg/mL, <
CH1> and <
CH2> decreased gradually with respect to C
dex. The inset shows a scatter plot for validating the linear relationship between <
CH1> and <
CH2>. As the coefficient of linear regression had a relatively high value of
R2 = 0.998, either <
CH1> or <
CH2> can be used to effectively monitor variations in RBC sedimentation in blood syringes.
For comparison with the results obtained using the present method, the ESR was measured with a conventional ESR method. In the modified ESR method, a 1 mL disposable syringe was filled with 1 mL blood, and installed vertically against the gravitational direction.
Figure 6(B-i) shows the temporal variations in RBC sedimentation (
H) with respect to C
dex. The
H tended to increase gradually for three bloods (C
dex = 5, 7.5, and 10 mg/mL). However, for bloods that were higher than C
dex = 10 mg/mL, the
H was saturated above 2400 s, approximately. Subsequently, substantial RBC sedimentation did not occur over time.
The right panel of
Figure 6(B-i) shows snapshots of RBC sedimentation of blood (C
dex = 20 mg/mL) at
t = 0 and 1 h. As the RBC sedimentation saturated before 1 h, two specific periods for calculating the ESR (i.e.,
t = 0.5 h and 1 h) were selected instead of
t = 1 h. Using the conventional ESR method, the ESR was calculated at a falling velocity (mm/h) by measuring the RBC sedimentation during two specific durations (
t) (
t = 0.5 h, 1 h).
Figure 6(B-ii) shows variations in ESR estimated at
t = 0.5 h and 1 h with respect to C
dex. For the ESR obtained at
t = 1 h, the dextran solution (C
dex ≤ 10 mg/mL) contributed to increasing the RBC sedimentation in the blood syringe. For an amount higher than C
dex = 10 mg/mL, the ESR decreased slightly with the increasing dextran solution concentration. As the RBC sedimentation saturated before 1 h, the scattering (or standard deviation) of the ESR was relatively lower. However, when the ESR was quantified at 0.5 h, the ESR showed large fluctuations above C
dex = 10 mg/mL. Compared with previous studies [
11,
20,
31], the results showed consistent trends with respect to the concentration of the dextran solution. Here, as normal RBCs were added to the dextran solution, the diluent (i.e., dextran solution) caused the ESR to increase. In fact, the conventional ESR did not separate the contributions of RBCs and diluent in the blood. Additionally, the conventional ESR was obtained by monitoring the interface between RBCs and diluent in the vertical tube. When compared with the conventional ESR method, the present method provided quantitative information on diluent as well as blood, such as viscosity and junction pressure. In addition, as blood viscosity and blood junction pressure were strongly related to hematocrit, the two coefficients obtained from the two formulas (i.e.,
µb = µ0 [1 +
CH1],
Pb = P0 [1 +
CH2]) could quantify variations in RBC sedimentation in the blood syringe. Thus, it was possible to determine why the blood had a higher ESR level. As a distinctive advantage, the present method can separate the contribution of RBC and diluent in the blood.
As a limitation of this study, the present method was demonstrated using suspended bloods (i.e., healthy RBCs in dextran solution or plasma for validating proof of concept). It was not a generalized study with various bloods collected from patients. In the near future, it will be necessary to validate the performance of the present method with clinical disease bloods [
2,
13,
35,
36]. Furthermore, to improve the portability of the present experimental setup, the two syringe pumps will be replaced by portable micropumps [
37,
38,
39].



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





