Physical Activity and Gastric Cancer Risk in Patients with and without Helicobacter pylori Infection in A Korean Population: A Hospital-Based Case-Control Study


Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
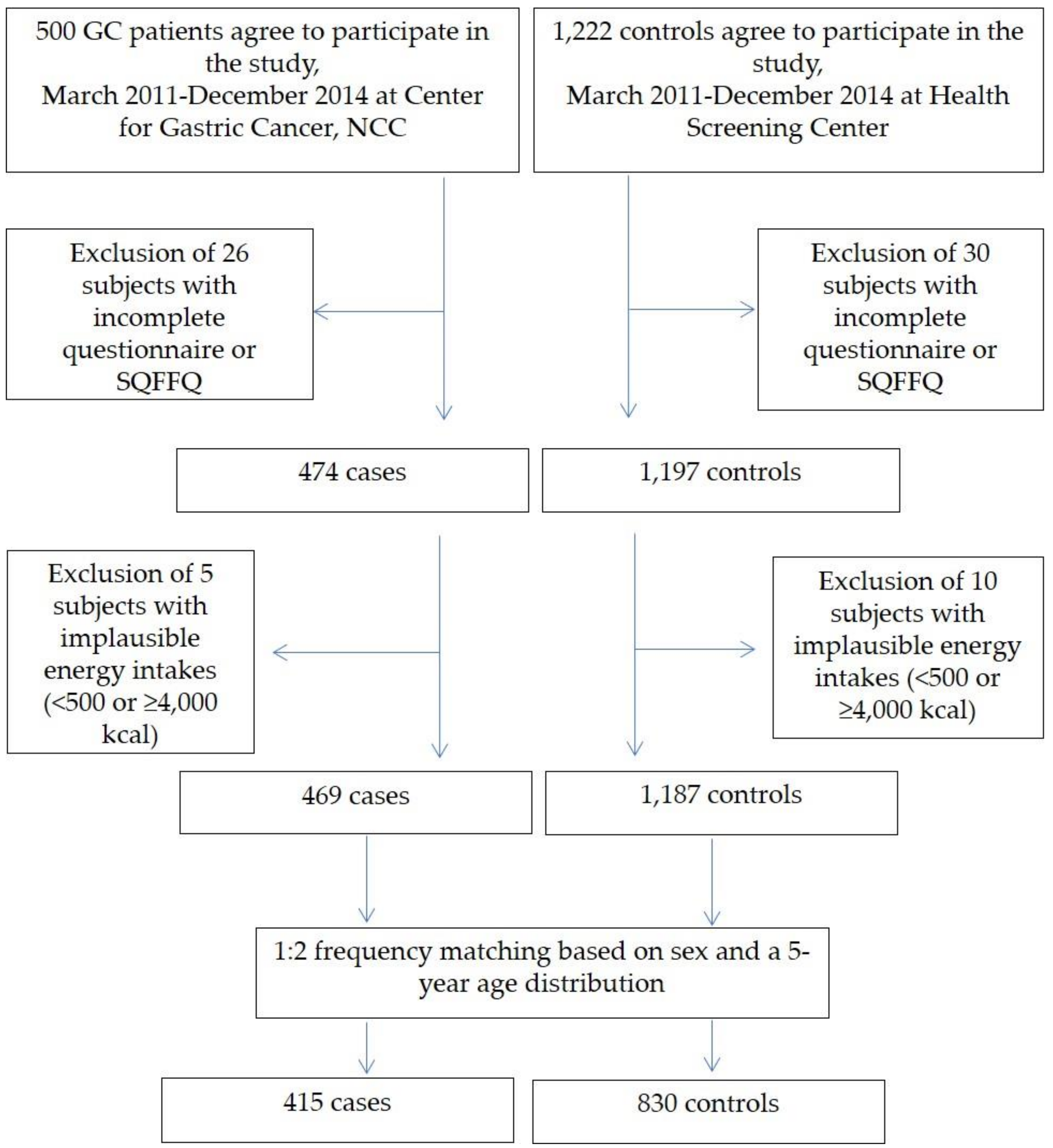
4.1. Study Population
4.2. Data Collection
4.3. Assessment of PA: International Physical Activity Questionnaire–Short Form (IPAQ-SF)
4.4. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 1–31. [Google Scholar] [CrossRef]
- Den Hoed, C.M.; Kuipers, E.J. Gastric cancer: How can we reduce the incidence of this disease? Curr. Gastroenterol. Rep. 2016, 18, 34. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Karim-Kos, H.E.; Coebergh, J.W.; Byrnes, G.; Antilla, A.; Ferlay, J.; Renehan, A.G.; Forman, D.; Soerjomataram, I. Recent trends in incidence of five common cancers in 26 European countries since 1988: Analysis of the European cancer observatory. Eur. J. Cancer 2015, 51, 1164–1187. [Google Scholar] [CrossRef] [PubMed]
- Forman, D.; Bray, F.; Brewster, D.; Gombe Mbalawa, C.; Kohler, B.; Piñeros, M.; Steliarova-Foucher, E.; Swaminathan, R.; Ferlay, J. Cancer Incidence in Five Continents, Vol. X (Electronic Version); IARC: Lyon, France, 2013. [Google Scholar]
- Jung, K.-W.; Won, Y.-J.; Kong, H.-J.; Lee, E.S. Cancer statistics in Korea: Incidence, mortality, survival, and prevalence in 2015. Cancer Res. Treat. 2018, 50, 303–316. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.-W.; Won, Y.-J.; Kong, H.-J.; Lee, E.S. Prediction of cancer incidence and mortality in Korea, 2018. Cancer Res. Treat. 2018, 50, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [PubMed]
- Tsugane, S. Salt, salted food intake, and risk of gastric cancer: Epidemiologic evidence. Cancer Sci. 2005, 96, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonequi, P.; Meneses-González, F.; Correa, P.; Rabkin, C.S.; Camargo, M.C. Risk factors for gastric cancer in Latin America: A meta-analysis. Cancer Causes Control 2013, 24, 217–231. [Google Scholar] [CrossRef] [PubMed]
- Tramacere, I.; Negri, E.; Pelucchi, C.; Bagnardi, V.; Rota, M.; Scotti, L.; Islami, F.; Corrao, G.; La Vecchia, C.; Boffetta, P. A meta-analysis on alcohol drinking and gastric cancer risk. Ann. Oncol. 2011, 23, 28–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crew, K.D.; Neugut, A.I. Epidemiology of gastric cancer. World J. Gastroenterol. 2006, 12, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Brenner, H.; Rothenbacher, D.; Arndt, V. Epidemiology of Stomach Cancer. Methods Mol. Biol. 2009, 472, 467–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagini, S. Carcinoma of the stomach: A review of epidemiology, pathogenesis, molecular genetics and chemoprevention. World J. Gastrointest. Oncol. 2012, 4, 156–169. [Google Scholar] [CrossRef] [PubMed]
- Key, T.J.; Schatzkin, A.; Willett, W.C.; Allen, N.E.; Spencer, E.A.; Travis, R.C. Diet, nutrition and the prevention of cancer. Public Health Nutr. 2004, 7, 187–200. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.Y.; Derakhshan, M.H. Environmental and lifestyle risk factors of gastric cancer. Arch. Iran. Med. 2013, 16, 358–365. [Google Scholar] [PubMed]
- Fock, K.M.; Katelaris, P.; Sugano, K.; Ang, T.L.; Hunt, R.; Talley, N.J.; Lam, S.K.; Xiao, S.D.; Tan, H.J.; Wu, C.Y. Second Asia–Pacific consensus guidelines for helicobacter pylori infection. J. Gastroenterol. Hepatol. 2009, 24, 1587–1600. [Google Scholar] [CrossRef] [PubMed]
- Cai, H.; Ye, F.; Michel, A.; Murphy, G.; Sasazuki, S.; Taylor, P.R.; Qiao, Y.-L.; Park, S.K.; Yoo, K.-Y.; Jee, S.H. Helicobacter pylori blood biomarker for gastric cancer risk in east Asia. Int. J. Epidemiol. 2016, 45, 774–781. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.; Kim, N. Diagnosis and management of high risk group for gastric cancer. Gut Liver 2015, 9, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Campbell, P.T.; Sloan, M.; Kreiger, N. Physical activity and stomach cancer risk: The influence of intensity and timing during the lifetime. Eur. J. Cancer 2007, 43, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Samad, A.K.; Taylor, R.S.; Marshall, T.; Chapman, M.A. A meta-analysis of the association of physical activity with reduced risk of colorectal cancer. Colorectal. Dis. 2005, 7, 204–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyle, T.; Keegel, T.; Bull, F.; Heyworth, J.; Fritschi, L. Physical activity and risks of proximal and distal colon cancers: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2012, 104, 1548–1561. [Google Scholar] [CrossRef] [PubMed]
- McTiernan, A. Physical activity and the prevention of breast cancer. Medscape Women's Health 2000, 5, E1. [Google Scholar] [PubMed]
- Tardon, A.; Lee, W.J.; Delgado-Rodriguez, M.; Dosemeci, M.; Albanes, D.; Hoover, R.; Blair, A. Leisure-time physical activity and lung cancer: A meta-analysis. Cancer Causes Control 2005, 16, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Matthews, C.E.; Xu, W.H.; Zheng, W.; Gao, Y.T.; Ruan, Z.X.; Cheng, J.R.; Xiang, Y.B.; Shu, X.O. Physical activity and risk of endometrial cancer: A report from the shanghai endometrial cancer study. Cancer Epidemiol. Biomark. Prev. 2005, 14, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Steindorf, K. The role of physical activity in primary cancer prevention. Eur. Rev. Aging Phys. Act. 2013, 10, 33–36. [Google Scholar] [CrossRef]
- Leitzmann, M.; Powers, H.; Anderson, A.S.; Scoccianti, C.; Berrino, F.; Boutron-Ruault, M.-C.; Cecchini, M.; Espina, C.; Key, T.J.; Norat, T. European code against cancer 4th edition: Physical activity and cancer. Cancer Epidemiol. 2015, 39, S46–S55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayán, C.; Cancela, J.; Molina, A.; Fernández, T.; Martín, V. Methodological issues when analysing the role of physical activity in gastric cancer prevention: A critical review. Eur. Rev. Aging Phys. Act. 2013, 10, 7–13. [Google Scholar] [CrossRef]
- Nieman, D.; Nehlsen-Cannarella, S.; Markoff, P.; Balk-Lamberton, A.; Yang, H.; Chritton, D.; Lee, J.; Arabatzis, K. The effects of moderate exercise training on natural killer cells and acute upper respiratory tract infections. Int. J. Sports Med. 1990, 11, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Cannon, J.G.; Kluger, M.J. Exercise enhances survival rate in mice infected with Salmonella typhimurium. Proc. Soc. Exp. Biol. Med. 1984, 175, 518–521. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.; Kohut, M.; Colbert, L.; Jackson, D.; Ghaffar, A.; Mayer, E. Exercise, alveolar macrophage function, and susceptibility to respiratory infection. J. Appl. Physiol. 1997, 83, 1461–1466. [Google Scholar] [CrossRef] [PubMed]
- Kohut, M.L.; Davis, J.M.; Jackson, D.; Colbert, L.; Strasner, A.; Essig, D.; Pate, R.R.; Ghaffar, A.; Mayer, E.P. The role of stress hormones in exercise-induced suppression of alveolar macrophage antiviral function. J. Neuroimmunol. 1998, 81, 193–200. [Google Scholar] [CrossRef]
- Leitzmann, M.F.; Koebnick, C.; Freedman, N.D.; Park, Y.; Ballard-Barbash, R.; Hollenbeck, A.; Schatzkin, A.; Abnet, C.C. Physical activity and esophageal and gastric carcinoma in a large prospective study. Am. J. Prev. Med. 2009, 36, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.C.; Lee, I.-M.; Weiderpass, E.; Campbell, P.T.; Sampson, J.N.; Kitahara, C.M.; Keadle, S.K.; Arem, H.; de Gonzalez, A.B.; Hartge, P. Association of leisure-time physical activity with risk of 26 types of cancer in 1.44 million adults. JAMA Intern. Med. 2016, 176, 816–825. [Google Scholar] [CrossRef] [PubMed]
- Psaltopoulou, T.; Ntanasis-Stathopoulos, I.; Tzanninis, I.-G.; Kantzanou, M.; Georgiadou, D.; Sergentanis, T.N. Physical activity and gastric cancer risk: A systematic review and meta-analysis. Clin. J. Sport Med. 2016, 26, 445–464. [Google Scholar] [CrossRef] [PubMed]
- Behrens, G.; Jochem, C.; Keimling, M.; Ricci, C.; Schmid, D.; Leitzmann, M.F. The association between physical activity and gastroesophageal cancer: Systematic review and meta-analysis. Eur. J. Epidemiol. 2014, 29, 151–170. [Google Scholar] [CrossRef] [PubMed]
- Abioye, A.I.; Odesanya, M.O.; Abioye, A.I.; Ibrahim, N.A. Physical activity and risk of gastric cancer: A meta-analysis of observational studies. Br. J. Sports Med. 2014, 49, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Yu, C.; Li, Y. Physical activity and risks of esophageal and gastric cancers: A meta-analysis. PLoS ONE 2014, 9, e88082. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Varayil, J.E.; Devanna, S.; Murad, M.H.; Iyer, P.G. Physical activity is associated with reduced risk of gastric cancer: A systematic review and meta-analysis. Cancer Prev. Res. 2014, 7, 12–22. [Google Scholar] [CrossRef] [PubMed]
- World Cancer Research Fund International, Continuous Updated Project. Diet, Nutrition Physical Activity and Stomach Cancer. Revised 2018. Available online: http://www.Wcrf.Org/int/continuous-update-project/cup-findings-reports/stomach-cancer (accessed on 21st May 2018).
- AICR. World Cancer Research Fund/American Institute for Cancer Research Food, Nutrition, Physical Activity and the Prevention of Cancer: A Global Perspective; American Institute for Cancer Research: Washington, DC, USA, 2007. [Google Scholar]
- Huerta, J.M.; Navarro, C.; Chirlaque, M.-D.; Tormo, M.-J.; Steindorf, K.; Buckland, G.; Carneiro, F.; Johnsen, N.F.; Overvad, K.; Stegger, J. Prospective study of physical activity and risk of primary adenocarcinomas of the oesophagus and stomach in the epic (European prospective investigation into cancer and nutrition) cohort. Cancer Causes Control 2010, 21, 657–669. [Google Scholar] [CrossRef] [PubMed]
- Inoue, M.; Yamamoto, S.; Kurahashi, N.; Iwasaki, M.; Sasazuki, S.; Tsugane, S. Daily total physical activity level and total cancer risk in men and women: Results from a large-scale population-based cohort study in Japan. Am. J. Epidemiol. 2008, 168, 391–403. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.-M. Physical activity and cancer prevention—Data from epidemiologic studies. Med. Sci. Sports Exerc. 2003, 35, 1823–1827. [Google Scholar] [CrossRef] [PubMed]
- Huerta, J.M.; Chirlaque, M.D.; Molina, A.J.; Amiano, P.; Martín, V.; Fernández-Villa, T.; Pérez-Gómez, B.; Moreno, V.; Burgui, R.; Gómez-Acebo, I.; et al. Physical activity domains and risk of gastric adenocarcinoma in the MCC-spain case-control study. PLoS ONE 2017, 12, e0179731. [Google Scholar] [CrossRef] [PubMed]
- Keum, N.; Bao, Y.; Smith-Warner, S.A.; Orav, J.; Wu, K.; Fuchs, C.S.; Giovannucci, E.L. Association of physical activity by type and intensity with digestive system cancer risk. JAMA Oncol. 2016, 2, 1146–1153. [Google Scholar] [CrossRef] [PubMed]
- Shephard, R.J. Cancers of the esophagus and stomach: Potential mechanisms behind the beneficial influence of physical activity. Clin. J. Sport Med. 2017, 27, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Amedei, A.; Munari, F.; Bella, C.D.; Niccolai, E.; Benagiano, M.; Bencini, L.; Cianchi, F.; Farsi, M.; Emmi, G.; Zanotti, G.; et al. Helicobacter pylori secreted peptidyl prolyl cis, trans-isomerase drives Th17 inflammation in gastric adenocarcinoma. Intern. Emerg. Med. 2014, 9, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Woods, J.A.; Davis, J.M.; Smith, J.A.; Nieman, D.C. Exercise and cellular innate immune function. Med. Sci. Sports Exerc. 1999, 31, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Koelwyn, G.J.; Wennerberg, E.; Demaria, S.; Jones, L.W. Exercise in regulation of inflammation-immune axis function in cancer initiation and progression. Oncology 2015, 29, 908–920. [Google Scholar] [PubMed]
- Forner, M.; Collazos, M.; Barriga, C.; De la Fuente, M.; Rodriguez, A.; Ortega, E. Effect of age on adherence and chemotaxis capacities of peritoneal macrophages. Influence of physical activity stress. Mech. Ageing Dev. 1994, 75, 179–189. [Google Scholar] [CrossRef]
- Michna, H. The human macrophage system: Activity and functional morphology. Bibl. Anat. 1988, 31, 1–84. [Google Scholar]
- Ortega, E.; Forner, M.; Barriga, C. Exercise-induced stimulation of murine macrophage chemotaxis: Role of corticosterone and prolactin as mediators. J. Physiol. 1997, 498, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Forner, M.; Barriga, C.; Ortega, E. Exercise-induced stimulation of murine macrophage phagocytosis may be mediated by thyroxine. J. Appl. Physiol. 1996, 80, 899–903. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.; Dai, J.; Zhang, M.; Hu, Z.; Shen, H. Potentially functional COX-2−1195G>A polymorphism increases the risk of digestive system cancers: A meta-analysis. J. Gastroenterol. Hepatol. 2010, 25, 1042–1050. [Google Scholar] [CrossRef] [PubMed]
- Kunzmann, A.T.; Mallon, K.P.; Hunter, R.F.; Cardwell, C.R.; McMenamin, Ú.C.; Spence, A.D.; Coleman, H.G. Physical activity, sedentary behaviour and risk of oesophago-gastric cancer: A prospective cohort study within UK biobank. United Eur. Gastroenterol. J. 2018. [Google Scholar] [CrossRef]
- Friedenreich, C.M.; Orenstein, M.R. Physical activity and cancer prevention: Etiologic evidence and biological mechanisms. J. Nutr. 2002, 132, 3456S–3464S. [Google Scholar] [CrossRef] [PubMed]
- Sjödahl, K.; Jia, C.; Vatten, L.; Nilsen, T.; Hveem, K.; Lagergren, J. Body mass and physical activity and risk of gastric cancer in a population-based cohort study in Norway. Cancer Epidemiol. Biomark. Prev. 2008, 17, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Woo, H.D.; Lee, J.; Choi, I.J.; Kim, C.G.; Lee, J.Y.; Kwon, O.; Kim, J. Dietary flavonoids and gastric cancer risk in a Korean population. Nutrients 2014, 6, 4961–4973. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.; Woo, H.D.; Lee, J.; Choi, I.J.; Kim, Y.W.; Sung, J.; Kim, J. Dietary folate, one-carbon metabolism-related genes, and gastric cancer risk in Korea. Mol. Nutr. Food Res. 2016, 60, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Hoang, B.V.; Lee, J.; Choi, I.J.; Kim, Y.-W.; Ryu, K.W.; Kim, J. Effect of dietary vitamin C on gastric cancer risk in the Korean population. World J. Gastroenterol. 2016, 22, 6257–6267. [Google Scholar] [CrossRef] [PubMed]
- Dicken, B.; Saunders, L.; Jhangri, G.; De Gara, C.; Cass, C.; Andrews, S.; Hamilton, S. Gastric cancer: Establishing predictors of biologic behavior with use of population-based data. Ann. Surg. Oncol. 2004, 11, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Ahn, Y.; Kwon, E.; Shim, J.; Park, M.; Joo, Y.; Kimm, K.; Park, C.; Kim, D. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur. J. Clin. Nutr. 2007, 61, 1435–1441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, C.L.; Marshall, A.L.; Sjorstrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Ortiz, A.; Tirado, M.; Hughes, D.C.; Gonzalez, V.; Song, J.; Mama, S.K.; Basen-Engquist, K. Relationship between physical activity, disability, and physical fitness profile in sedentary latina breast cancer survivors. Physiother. Theory Pract. 2018, 34, 783–794. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.; Stewart, S.M. Validity of the international physical activity questionnaire short form (IPAQ-SF): A systematic review. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanda, B.; Vistad, I.; Haakstad, L.A.H.; Berntsen, S.; Sagedal, L.R.; Lohne-Seiler, H.; Torstveit, M.K. Reliability and concurrent validity of the international physical activity questionnaire short form among pregnant women. BMC Sports Sci. Med. Rehabil. 2017, 9, 7. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | All (n = 1245) | Male (n = 810) | Female (n = 435) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Control group (n = 830) | Case group (n = 415) | p-value b | Control group (n = 540) | Case group (n = 270) | p-value b | Control group (n = 290) | Casegroup (n = 145) | p-value b | |
| Age (y) | 53.7 ± 9.0 | 53.8 ± 9.3 | 0.892 | 54.8 ± 8.4 | 54.9 ± 8.7 | 0.905 | 51.6 ± 9.8 | 51.7 ± 9.9 | 0.942 |
| <50 | 285 (34.3) | 139 (33.5) | 0.767 | 153 (28.33) | 77 (28.5) | 0.956 | 132 (45.5) | 62 (42.8) | 0.585 |
| ≥50 | 545 (65.7) | 276 (66.5) | 387 (71.7) | 193 (71.5) | 158 (54.5) | 83 (57.2) | |||
| Gender [n (%)] | 0.9999 | ||||||||
| Male | 540 (65.1) | 270 (65.1) | |||||||
| Female | 290 (34.9) | 145 (34.9) | |||||||
| Body mass index (kg/m²) [n (%)] | 23.9 ± 2.9 | 23.9 ± 3.0 | 0.627 | 24.4 ± 2.7 | 24.2 ± 3.0 | 0.390 | 23.1 ± 3.1 | 23.2 ± 3.0 | 0.788 |
| <23 | 314 (37.8) | 159 (38.3) | 0.975 | 161 (29.8) | 91 (33.7) | 0.509 | 153 (52.8) | 68 (46.9) | 0.533 |
| 23–25 | 249 (30.0) | 122 (29.4) | 170 (31.5) | 78 (28.9) | 79 (27.2) | 44 (30.3) | |||
| ≥25 | 266 (32.1) | 133 (32.1) | 209 (38.7) | 101 (37.4) | 57 (19.7) | 32 (22.1) | |||
| Missing | 1 (0.1) | 1 (0.2) | 0 (0.0) | 0 (0.0) | 1 (0.3) | 1 (0.7) | |||
| Smoking status [n (%)] | <0.001 | <0.001 | 0.021 | ||||||
| Current smoker | 162 (19.5) | 128 (30.8) | 157 (29.1) | 121 (44.8) | 5 (1.7) | 7 (4.8) | |||
| Ex-smoker | 284 (34.2) | 119 (28.7) | 277 (51.3) | 110 (40.7) | 7 (2.4) | 9 (6.2) | |||
| Non-smoker | 384 (46.3) | 167 (40.2) | 106 (19.6) | 39 (14.4) | 278 (95.9) | 128 (88.3) | |||
| Missing | 0 (0.0) | 1 (0.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.7) | |||
| Alcohol consumption [n (%)] | 0.243 | 0.282 | 0.819 | ||||||
| Current drinker | 534 (64.3) | 254 (61.2) | 404 (74.8) | 193 (71.5) | 130 (44.8) | 61 (42.1) | |||
| Ex-drinker | 60 (7.2) | 41 (9.9) | 47 (8.7) | 33 (12.2) | 13 (4.5) | 8 (5.5) | |||
| Non-drinker | 236 (28.4) | 119 (28.7) | 89 (16.5) | 44 (16.3) | 147 (50.7) | 75 (51.7) | |||
| Missing | 0 (0.0) | 1 (0.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 1 (0.7) | |||
| First-degree family history of gastric cancer | <0.001 | 0.003 | 0.114 | ||||||
| Yes | 103 (12.4) | 82 (19.8) | 74 (13.7) | 60 (22.2) | 29 (10.0) | 22 (15.2) | |||
| No | 725 (87.4) | 332 (80.0) | 464 (85.9) | 209 (77.4) | 261 (90.0) | 123 (84.8) | |||
| Missing | 2 (0.2) | 1 (0.2) | 2 (0.4) | 1 (0.4) | 0 (0.0) | 0 (0.0) | |||
| Regular exercise [n (%)] | <0.001 | <0.001 | <0.001 | ||||||
| Yes | 466 (56.1) | 147 (35.4) | 303 (56.1) | 109 (40.4) | 163 (56.2) | 38 (26.2) | |||
| No | 361 (43.4) | 268 (64.6) | 234 (43.3) | 161 (59.6) | 127 (43.8) | 107 (73.8) | |||
| Missing | 3 (0.4) | 0 (0.0) | 3 (0.6) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |||
| Educational level [n (%)] | <0.001 | <0.001 | <0.001 | ||||||
| Middle school | 119 (14.3) | 142 (34.2) | 71 (13.2) | 91 (33.7) | 48 (16.6) | 51 (35.2) | |||
| High school | 253 (30.5) | 174 (41.9) | 140 (25.9) | 112 (41.5) | 113 (38.9) | 62 (42.8) | |||
| College or more | 426 (51.3) | 97 (23.4) | 301 (55.7) | 66 (24.4) | 125 (43.1) | 31 (21.4) | |||
| Missing | 32 (3.9) | 2 (0.5) | 28 (5.2) | 1 (0.4) | 4 (1.4) | 1 (0.7) | |||
| Occupation [n (%)] | <0.001 | 0.009 | 0.002 | ||||||
| Group 1: Professionals, administrative management | 156 (18.8) | 70 (16.9) | 117 (21.7) | 59 (21.9) | 39 (13.5) | 11 (7.6) | |||
| Group 2: Office, sales, and service positions | 266 (32.1) | 122 (29.4) | 203 (37.6) | 81 (30.0) | 63 (21.7) | 41 (28.3) | |||
| Group 3:Agriculture, laborer | 128 (15.4) | 104 (25.1) | 111 (20.6) | 83 (30.7) | 17 (5.9) | 21 (14.5) | |||
| Group 4:Unemployment and others | 277 (33.4) | 117 (28.2) | 106 (19.6) | 46 (17.0) | 171 (58.9) | 71 (49.0) | |||
| Missing | 3 (0.4) | 2 (0.5) | 3 (0.6) | 1 (0.4) | 0 (0.0) | 1 (0.7) | |||
| Marital status [n (%)] | 0.611 | 0.475 | 0.975 | ||||||
| Married | 716 (86.3) | 361 (87.0) | 478 (88.5) | 243 (90.0) | 238 (82.1) | 118 (81.4) | |||
| Others (single, divorced, separated, widowed, cohabitating) | 113 (13.6) | 52 (12.5) | 61 (11.3) | 26 (9.6) | 52 (17.9) | 26 (17.9) | |||
| Missing | 1 (0.1) | 2 (0.5) | 1 (0.2) | 1 (0.4) | 0 (0.0) | 1 (0.7) | |||
| Monthly income [n (%)] a | <0.001 | <0.001 | 0.016 | ||||||
| <200 | 149 (18.0) | 133 (32.1) | 85 (15.7) | 85 (31.5) | 64 (22.1) | 48 (33.1) | |||
| 200–400 | 341 (41.1) | 148 (35.7) | 232 (43.0) | 106 (39.3) | 109 (37.6) | 42 (28.9) | |||
| ≥400 | 273 (32.9) | 96 (23.1) | 168 (31.1) | 55 (20.4) | 105 (36.2) | 41 (28.3) | |||
| Missing | 67 (8.1) | 38 (9.2) | 55 (10.2) | 24 (8.9) | 12 (4.1) | 14 (9.7) | |||
| H. pylori infection | <0.001 | <0.001 | <0.001 | ||||||
| Positive | 486 (58.6) | 382 (92.1) | 333 (61.7) | 252 (93.3) | 153 (52.8) | 130 (89.7) | |||
| Negative | 320 (38.6) | 33 (8.0) | 187 (34.6) | 18 (6.7) | 133 (45.9) | 15 (10.3) | |||
| Missing | 24 (2.9) | 0 (0.0) | 20 (3.7) | 0 (0.0) | 4 (1.4) | 0 (0.0) | |||
| Supplements use [n (%)] | 0.094 | 0.193 | 0.291 | ||||||
| Yes | 527 (63.5) | 243 (58.6) | 329 (60.9) | 152 (56.3) | 198 (68.3) | 91 (62.8) | |||
| No | 298 (35.9) | 169 (40.7) | 206 (38.2) | 116 (43.0) | 92 (31.7) | 53 (36.6) | |||
| Missing | 5 (0.6) | 3 (0.7) | 5 (0.9) | 2 (0.7) | 0 (0.0) | 1 (0.7) | |||
| Lauren’s classification | |||||||||
| Intestinal | NA | 158 (38.1) | NA | NA | 132 (48.9) | NA | NA | 26 (17.9) | NA |
| Diffuse | NA | 164 (39.5) | NA | 77 (28.5) | NA | 87 (60.0) | |||
| Mixed | NA | 59 (14.2) | NA | 40 (14.8) | NA | 19 (13.1) | |||
| Intermediate | NA | 4 (1.0) | NA | 3 (1.1) | NA | 1 (0.7) | |||
| Missing | NA | 30 (7.2) | NA | 18 (6.7) | NA | 12 (8.3) | |||
| IPAQ categorical score | 0.005 | 0.026 | 0.152 | ||||||
| Low | 273 (32.9) | 175 (42.2) | 163 (30.2) | 106 (39.3) | 110 (37.9) | 69 (47.6) | |||
| Moderate | 309 (37.2) | 128 (30.8) | 191 (35.4) | 77 (28.5) | 118 (40.7) | 51 (35.2) | |||
| High | 248 (29.9) | 112 (27.0) | 186 (34.4) | 87 (32.2) | 62 (21.4) | 25 (17.2) | |||
| IPAQ Continuous Score c | |||||||||
| Walking MET min/week | 1203.0 ± 1133.6 | 973.3 ± 1129.8 | 0.001 | 1260.2 ± 1153.3 | 1042.1 ± 1182.7 | 0.015 | 1096.1 ± 1089.9 | 845.8 ± 1016.4 | 0.026 |
| Moderate MET min/week | 599.7 ± 1021.5 | 608.6 ± 1174.8 | 0.897 | 700.6 ± 1103.7 | 668.0 ± 1242.9 | 0.720 | 411.5 ± 816.2 | 498.4 ± 1032.4 | 0.385 |
| Vigorous MET min/week | 951.9 ± 1775.8 | 962.4 ± 2047.3 | 0.929 | 1169.0 ± 1970.2 | 1276.9 ± 2342.7 | 0.518 | 540.2 ± 1234.0 | 377.2 ± 1126.5 | 0.186 |
| Total MET min/week | 2671.1 ± 2829.0 | 2460.8 ± 3225.8 | 0.260 | 3040.9 ± 3066.0 | 2896.5 ± 3556.1 | 0.570 | 1979.3 ± 2162.4 | 1652.6 ± 2301.6 | 0.148 |
| Total energy intake (Kcal/day) | 1713.6 ± 545.5 | 1924.1 ± 612.9 | <0.001 | 1760.6 ± 541.5 | 2038.5 ± 634.8 | <0.001 | 1626.0 ± 543.1 | 1711.1 ± 507.0 | 0.116 |
| Regular Exercise | Gastric Cancer Risk | ||||
|---|---|---|---|---|---|
| Control group (%) | Cases group (%) | Model 1 (95% CI) | Model 2 OR (95% CI) | Model 3 OR (95% CI) | |
| All | |||||
| No | 361 (43.7) | 268 (64.6) | 1.00 | 1.00 | 1.00 |
| Yes | 466 (56.4) | 147 (35.4) | 0.43 (0.33–0.54) | 0.47 (0.36–0.62) | 0.52 (0.39–0.69) |
| Males | |||||
| No | 234 (43.6) | 161 (59.6) | 1.00 | 1.00 | 1.00 |
| Yes | 303 (56.4) | 109 (40.4) | 0.52 (0.39–0.70) | 0.65 (0.46–0.91) | 0.73 (0.50–1.05) |
| Females | |||||
| No | 127 (43.8) | 107 (73.8) | 1.00 | 1.00 | 1.00 |
| Yes | 163 (56.2) | 38 (26.2) | 0.28 (0.18–0.43) | 0.30 (0.18–0.48) | 0.34 (0.21–0.57) |
| IPAQ Categorical Score | Gastric Cancer | ||||
|---|---|---|---|---|---|
| Control Group (%) | Case Group (%) | Model 1 (95% CI) | Model 2 OR (95% CI) | Model 3 OR (95% CI) | |
| All | |||||
| Low | 273 (32.9) | 175 (42.2) | 1.00 | 1.00 | 1.00 |
| Moderate | 309 (37.2) | 128 (30.8) | 0.65 (0.49–0.86) | 0.64 (0.47–0.87) | 0.67 (0.48–0.94) |
| High | 248 (29.9) | 112 (27.0) | 0.71 (0.53–0.94) | 0.59 (0.43–0.83) | 0.61 (0.43–0.87) |
| p-trend | 0.067 | 0.007 | 0.014 | ||
| Males | |||||
| Low | 163 (30.2) | 106 (39.3) | 1.00 | 1.00 | 1.00 |
| Moderate | 191 (35.4) | 77 (28.5) | 0.62 (0.43–0.88) | 0.62 (0.41–0.94) | 0.63 (0.41–0.98) |
| High | 186 (34.4) | 87 (32.2) | 0.72 (0.51–1.02) | 0.67 (0.44–1.00) | 0.70 (0.45–1.09) |
| p-trend | 0.213 | 0.141 | 0.262 | ||
| Females | |||||
| Low | 110 (37.9) | 69 (47.6) | 1.00 | 1.00 | 1.00 |
| Moderate | 118 (40.7) | 51 (35.2) | 0.69 (0.44–1.08) | 0.66 (0.41–1.07) | 0.78 (0.46–1.31) |
| High | 62 (21.4) | 25 (17.2) | 0.64 (0.37–1.12) | 0.52 (0.28–0.96) | 0.51 (0.26–0.98) |
| p-trend | 0.119 | 0.038 | 0.043 | ||
| All | Median Range MET min/Week | Gastric Cancer Risk | ||||
|---|---|---|---|---|---|---|
| Control Group (%) | Case Group (%) | Model 1 (95% CI) | Model 2 OR (95% CI) | Model 3 OR (95% CI) | ||
| Low-intensity activity | ||||||
| T1 (0–495) | 198.0 | 237 (29.9) | 182 (46.9) | 1.00 | 1.00 | 1.00 |
| T2 (495–1386) | 792.0 | 274 (34.6) | 92 (23.7) | 0.44 (0.32–0.59) | 0.46 (0.33–0.64) | 0.43 (0.30–0.62) |
| T3 (≥1386) | 2079.0 | 281 (35.5) | 114 (29.4) | 0.53 (0.40–0.71) | 0.45 (0.33–0.62) | 0.46 (0.33–0.65) |
| p-trend | <0.001 | <0.001 | <0.001 | |||
| Moderate-intensity activity | ||||||
| Low (0–480) | 0.0 | 509 (63.7) | 279 (69.4) | 1.00 | 1.00 | 1.00 |
| High (≥480) | 1200.0 | 290 (36.3) | 123 (30.6) | 0.77 (0.60–1.00) | 0.69 (0.52–0.93) | 0.69 (0.51–0.94) |
| p-trend | 0.05 | 0.013 | 0.019 | |||
| Vigorous-intensity activity | ||||||
| Low (0–720) | 0.0 | 536 (66.3) | 302 (73.3) | 1.00 | 1.00 | 1.00 |
| High (≥720) | 1920.0 | 272 (33.7) | 110 (26.7) | 0.72 (0.55–0.93) | 0.58 (0.43–0.78) | 0.61 (0.48–0.84) |
| p-trend | 0.013 | <0.001 | 0.002 | |||
| Total physical activity | ||||||
| T1 (0–990) | 339.0 | 259 (31.4) | 190 (45.9) | 1.00 | 1.00 | 1.00 |
| T2 (990–2970) | 1699.5 | 290 (35.2) | 109 (26.3) | 0.51 (0.38–0.68) | 0.52 (0.38–0.72) | 0.56 (0.40–0.78) |
| T3 (≥2970) | 4878.0 | 275 (33.4) | 115 (27.8) | 0.57 (0.43–0.76) | 0.47 (0.34–0.64) | 0.46 (0.32–0.65) |
| p-trend | 0.001 | <0.001 | <0.001 | |||
| Males | ||||||
| Low-intensity activity | ||||||
| T1 (0–594) | 231.0 | 163 (31.6) | 124 (49.2) | 1.00 | 1.00 | 1.00 |
| T2 (594–1386) | 792.0 | 163 (31.6) | 43 (17.1) | 0.35 (0.23–0.52) | 0.39 (0.25–0.62) | 0.38 (0.23–0.62) |
| T3 (≥1386) | 2376.0 | 190 (36.8) | 85 (33.7) | 0.59 (0.42–0.83) | 0.57 (0.39–0.85) | 0.60 (0.39–0.91) |
| p-trend | 0.042 | 0.032 | 0.078 | |||
| Moderate-intensity activity | ||||||
| Low (0–720) | 0.0 | 342 (65.8) | 189 (72.4) | 1.00 | 1.00 | 1.00 |
| High (≥720) | 1440 | 178 (34.2) | 72 (27.6) | 0.73 (0.53–1.01) | 0.59 (0.41–0.86) | 0.57 (0.38–0.86) |
| p-trend | 0.061 | 0.006 | 0.006 | |||
| Vigorous-intensity activity | ||||||
| Low (0–960) | 0.0 | 334 (63.1) | 181 (67.5) | 1.00 | 1.00 | 1.00 |
| High (≥960) | 2400 | 195 (36.9) | 87 (32.5) | 0.82 (0.60–1.12) | 0.71 (0.50–1.02) | 0.73 (0.50–1.07) |
| p-trend | 0.220 | 0.065 | 0.109 | |||
| Total physical activity | ||||||
| T1 (0–1188) | 495.0 | 173 (32.2) | 116 (43.1) | 1.00 | 1.00 | 1.00 |
| T2 (1188–3390) | 2079.0 | 184 (34.3) | 71 (26.4) | 0.58 (0.40–0.83) | 0.65 (0.43–0.97) | 0.65 (0.42–1.00) |
| T3 (≥3390) | 5473.5 | 180 (33.5) | 82 (30.5) | 0.68 (0.48–0.97) | 0.62 (0.41–0.93) | 0.62 (0.40–0.96) |
| p-trend | 0.077 | 0.036 | 0.054 | |||
| Females | ||||||
| Low-intensity activity | ||||||
| T1 (0–462) | 198.0 | 89 (32.3) | 62 (45.6) | 1.00 | 1.00 | 1.00 |
| T2 (462–1188) | 660.0 | 83 (30.1) | 39 (28.7) | 0.67 (0.41–1.11) | 0.69 (0.40–1.19) | 0.56 (0.31–1.01) |
| T3 (≥1188) | 1848.0 | 104 (37.7) | 35 (25.7) | 0.48 (0.29–0.80) | 0.44 (0.25–0.76) | 0.44 (0.25–0.81) |
| p-trend | 0.006 | 0.004 | 0.014 | |||
| Moderate-intensity activity | ||||||
| Low (0–240) | 0.0 | 177 (63.4) | 100 (70.9) | 1.00 | 1.00 | 1.00 |
| High (≥240) | 720.0 | 102 (36.6) | 41 (29.1) | 0.71 (0.46–1.10) | 0.66 (0.41–1.05) | 0.72 (0.43–1.20) |
| p-trend | 0.127 | 0.084 | 0.205 | |||
| Vigorous-intensity activity | ||||||
| Low (0–484) | 0.0 | 211 (75.6) | 125 (86.8) | 1.00 | 1.00 | 1.00 |
| High (≥484) | 1440.0 | 68 (24.4) | 19 (13.2) | 0.47 (0.27–0.82) | 0.41 (0.22–0.75) | 0.48 (0.25–0.91) |
| p-trend | 0.008 | 0.004 | 0.026 | |||
| Total physical activity | ||||||
| T1 (0–693) | 234.5 | 92 (32.1) | 64 (44.1) | 1.00 | 1.00 | 1.00 |
| T2 (693–2128) | 1314.0 | 99 (34.5) | 48 (33.1) | 0.69 (0.44–1.12) | 0.75 (0.45–1.25) | 0.87 (0.50–1.51) |
| T3 (≥2128) | 3555.0 | 96 (33.5) | 33 (22.8) | 0.50 (0.30–0.82) | 0.40 (0.23–0.70) | 0.43 (0.23–0.79) |
| p-trend | 0.008 | 0.001 | 0.005 | |||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gunathilake, M.N.; Lee, J.; Jang, A.; Choi, I.J.; Kim, Y.-I.; Kim, J. Physical Activity and Gastric Cancer Risk in Patients with and without Helicobacter pylori Infection in A Korean Population: A Hospital-Based Case-Control Study. Cancers 2018, 10, 369. https://doi.org/10.3390/cancers10100369
Gunathilake MN, Lee J, Jang A, Choi IJ, Kim Y-I, Kim J. Physical Activity and Gastric Cancer Risk in Patients with and without Helicobacter pylori Infection in A Korean Population: A Hospital-Based Case-Control Study. Cancers. 2018; 10(10):369. https://doi.org/10.3390/cancers10100369
Chicago/Turabian StyleGunathilake, Madhawa Neranjan, Jeonghee Lee, Aelee Jang, Il Ju Choi, Young-Il Kim, and Jeongseon Kim. 2018. "Physical Activity and Gastric Cancer Risk in Patients with and without Helicobacter pylori Infection in A Korean Population: A Hospital-Based Case-Control Study" Cancers 10, no. 10: 369. https://doi.org/10.3390/cancers10100369
APA StyleGunathilake, M. N., Lee, J., Jang, A., Choi, I. J., Kim, Y. -I., & Kim, J. (2018). Physical Activity and Gastric Cancer Risk in Patients with and without Helicobacter pylori Infection in A Korean Population: A Hospital-Based Case-Control Study. Cancers, 10(10), 369. https://doi.org/10.3390/cancers10100369