Vonoprazan-Based Third-Line Therapy Has a Higher Eradication Rate against Sitafloxacin-Resistant Helicobacter pylori

Abstract
:1. Introduction
2. Methods
2.1. Patients and Study Design
2.2. Statistics
3. Results
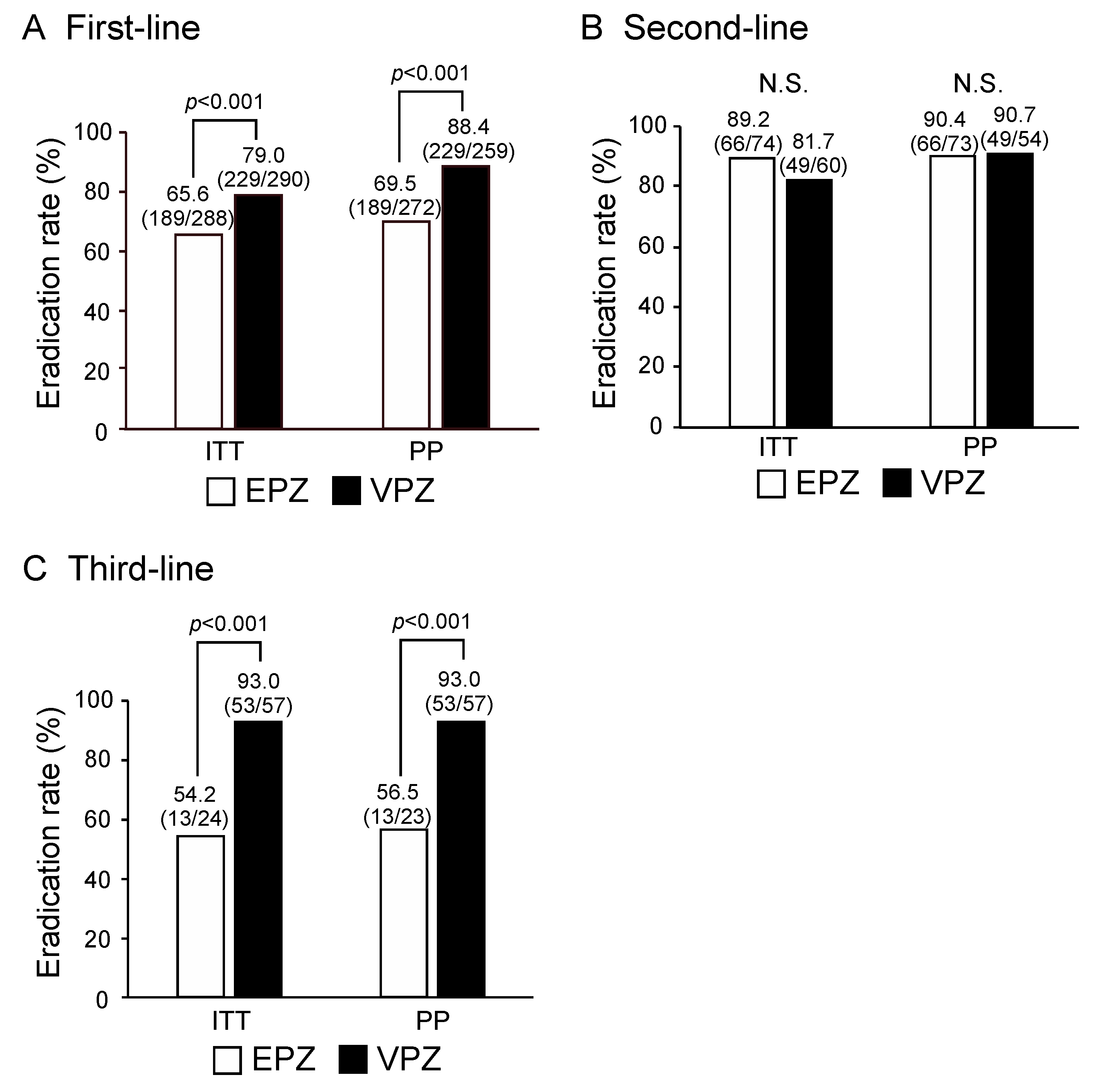
3.1. Overall Success Rates of First- and Third-Line H. Pylori Eradication Are Significantly Higher for VPZ-Based Therapy Than for EPZ-Based Triple Therapy
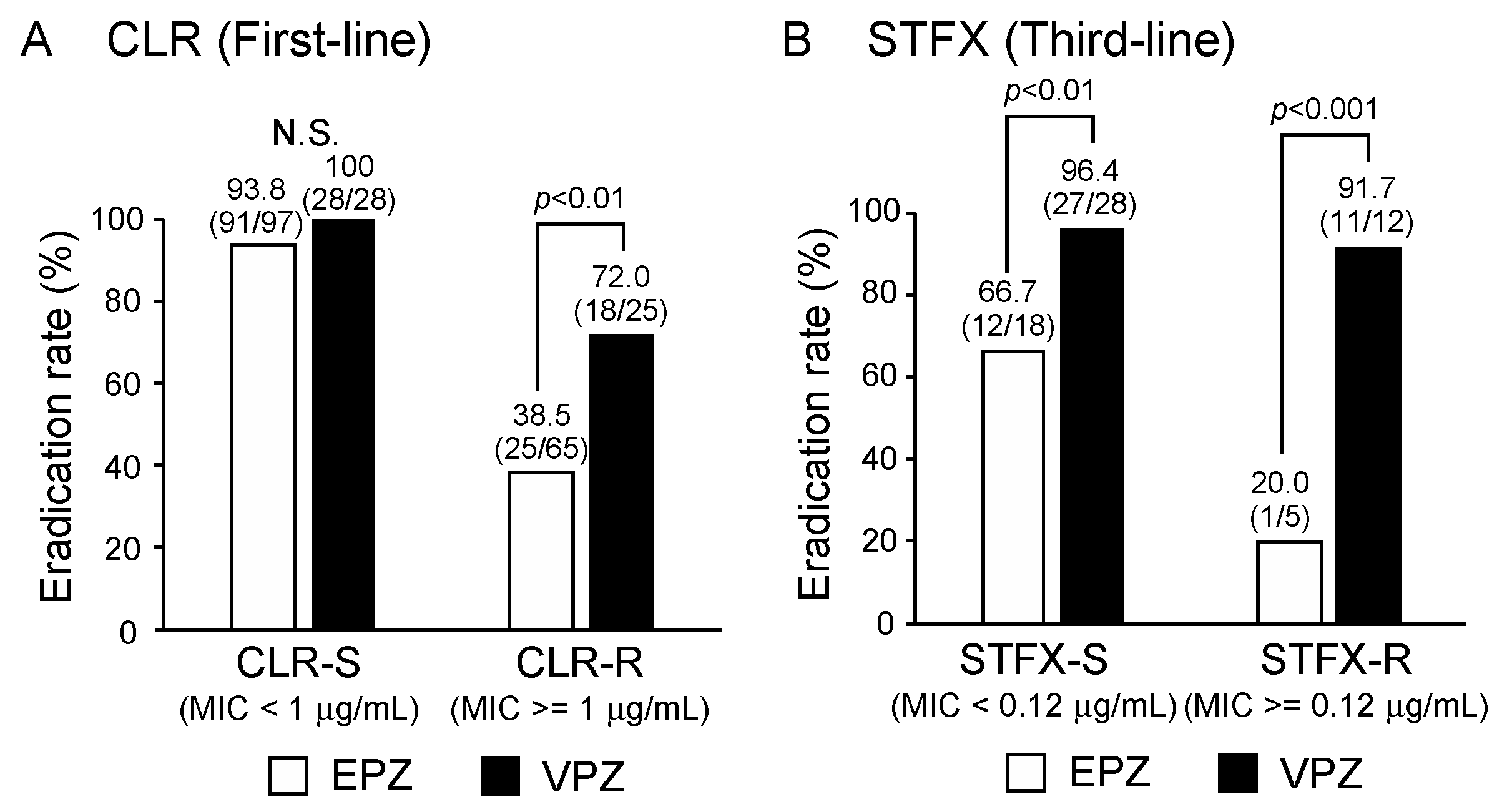
3.2. Success Rates for First- and Third-Line Eradication of CLR-Resistant H. Pylori Are Significantly Higher for VPZ-Based Therapy Than for EPZ-Based Triple Therapy
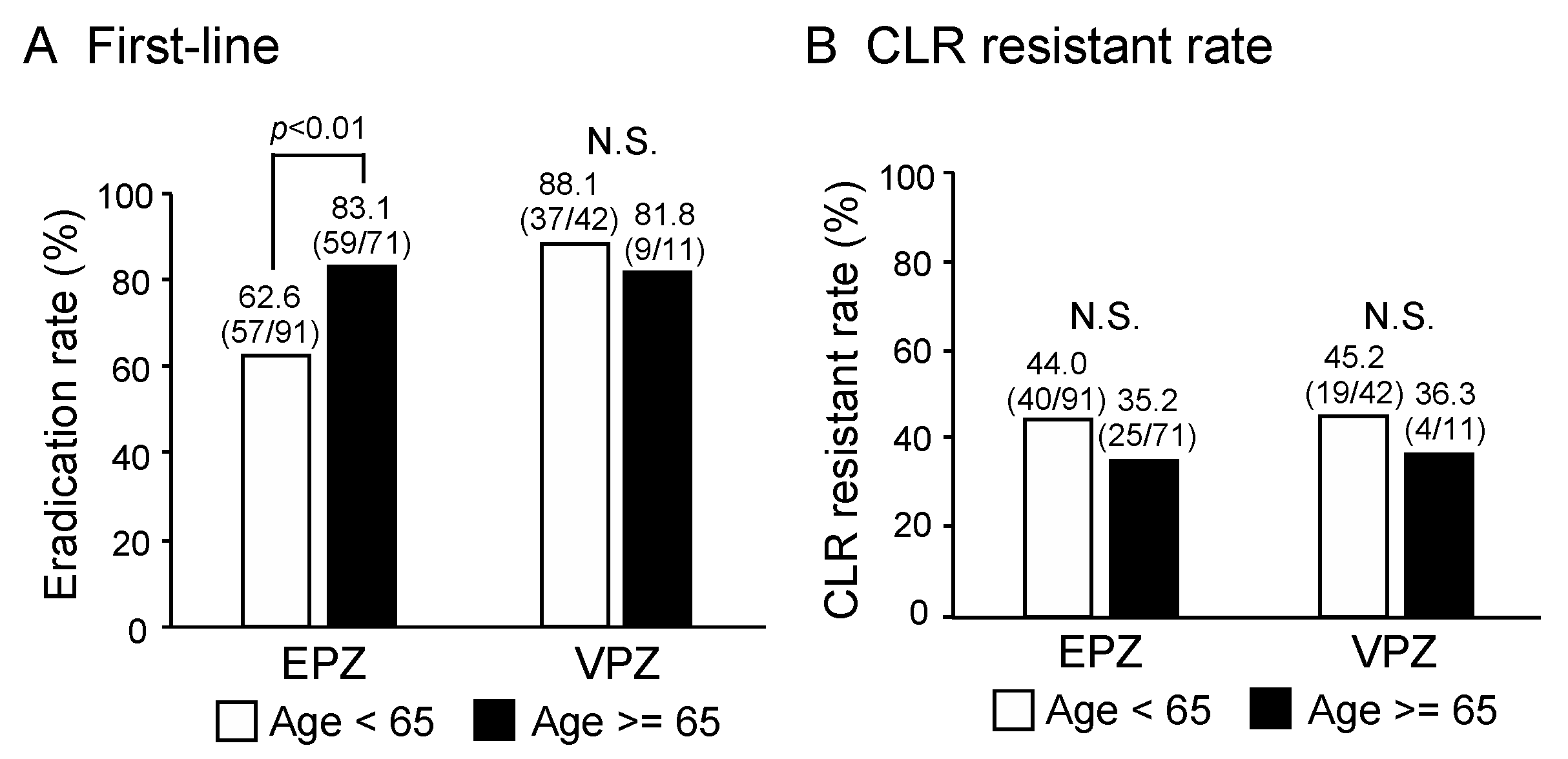
3.3. Patient Age Does Not Affect the Eradication Rate Achieved by VPZ-Based First-Line Therapy, Whereas That for EPZ-Based Therapy Is Lower in Patients under 65 Years of Age
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Suzuki, H.; Hibi, T.; Marshall, B.J. Helicobacter pylori: Present status and future prospects in Japan. J. Gastroenterol. 2007, 42, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Cover, T.L.; Blaser, M.J. Helicobacter pylori in health and disease. Gastroenterology 2009, 136, 1863–1873. [Google Scholar] [CrossRef] [PubMed]
- Saito, Y.; Suzuki, H.; Tsugawa, H.; Suzuki, S.; Matsuzaki, J.; Hirata, K.; Hibi, T. Dysfunctional gastric emptying with down-regulation of muscle-specific microRNAs in Helicobacter pylori-infected mice. Gastroenterology 2011, 140, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Saito, Y.; Suzuki, H.; Tsugawa, H.; Imaeda, H.; Matsuzaki, J.; Hirata, K.; Hosoe, N.; Nakamura, M.; Mukai, M.; Saito, H.; et al. Overexpression of miR-142-5p and miR-155 in gastric mucosa-associated lymphoid tissue (MALT) lymphoma resistant to Helicobacter pylori eradication. PLoS ONE 2012, 7, e47396. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H.; Moayyedi, P. Helicobacter pylori infection in functional dyspepsia. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Fukase, K.; Kato, M.; Kikuchi, S.; Inoue, K.; Uemura, N.; Okamoto, S.; Terao, S.; Amagai, K.; Hayashi, S.; Asaka, M.; et al. Effect of eradication of Helicobacter pylori on incidence of metachronous gastric carcinoma after endoscopic resection of early gastric cancer: An open-label, randomised controlled trial. Lancet 2008, 372, 392–397. [Google Scholar] [CrossRef]
- Suzuki, H.; Nishizawa, T.; Hibi, T. Helicobacter pylori eradication therapy. Future Microbiol. 2010, 5, 639–648. [Google Scholar] [CrossRef] [PubMed]
- Saito, Y.; Serizawa, H.; Kato, Y.; Nakano, M.; Nakamura, M.; Saito, H.; Suzuki, H.; Kanai, T. First-line eradication for Helicobacter pylori-positive gastritis by esomeprazole-based triple therapy is influenced by CYP2C19 genotype. World J. Gastroenterol. 2015, 21, 13548–13554. [Google Scholar] [CrossRef] [PubMed]
- Murakami, K.; Sakurai, Y.; Shiino, M.; Funao, N.; Nishimura, A.; Asaka, M. Vonoprazan, a novel potassium-competitive acid blocker, as a component of first-line and second-line triple therapy for Helicobacter pylori eradication: A phase III, randomised, double-blind study. Gut 2016, 65, 1439–1446. [Google Scholar] [CrossRef] [PubMed]
- Noda, H.; Noguchi, S.; Yoshimine, T.; Goji, S.; Adachi, K.; Tamura, Y.; Izawa, S.; Ebi, M.; Yamamoto, S.; Ogasawara, N.; et al. A novel potassium-competitive acid blocker improves the efficacy of clarithromycin-containing 7-day triple therapy against Helicobacter pylori. J. Gastrointestin. Liver Dis. 2016, 25, 283–288. [Google Scholar] [PubMed]
- Matsumoto, H.; Shiotani, A.; Katsumata, R.; Fujita, M.; Nakato, R.; Murao, T.; Ishii, M.; Kamada, T.; Haruma, K.; Graham, D.Y. Helicobacter pylori eradication with proton pump inhibitors or potassium-competitive acid blockers: The effect of clarithromycin resistance. Dig. Dis. Sci. 2016, 61, 3215–3220. [Google Scholar] [CrossRef]
- Clinical Breakpoints for Bacteria. Available online: http://www.eucast.org/clinical_breakpoints (accessed on 18 January 2019).
- Matsuzaki, J.; Suzuki, H.; Nishizawa, T.; Hirata, K.; Tsugawa, H.; Saito, Y.; Okada, S.; Fukuhara, S.; Hibi, T. Efficacy of sitafloxacin-based rescue therapy for Helicobacter pylori after failures of first- and second-line therapies. Antimicrob. Agents Chemother. 2012, 56, 1643–1645. [Google Scholar] [CrossRef]
- Mori, H.; Suzuki, H.; Matsuzak, J.; Masaoka, T.; Kanai, T. Acquisition of double mutation in gyrA caused high resistance to sitafloxacin in Helicobacter pylori after unsuccessful eradication with sitafloxacin-containing regimens. United European Gastroenterol. J. 2018, 6, 391–397. [Google Scholar] [CrossRef]
- Hori, Y.; Imanishi, A.; Matsukawa, J.; Tsukimi, Y.; Nishida, H.; Arikawa, Y.; Hirase, K.; Kajino, M.; Inatomi, N. 1-[5-(2-Fluorophenyl)-1-(pyridin-3-ylsulfonyl)-1H-pyrrol-3-yl]-N-methylmethanamine monofumarate (TAK-438), a novel and potent potassium-competitive acid blocker for the treatment of acid-related diseases. J. Pharmacol. Exp. Ther. 2010, 335, 231–238. [Google Scholar] [CrossRef]
- Tsujimae, M.; Yamashita, H.; Hashimura, H.; Kano, C.; Shimoyama, K.; Kanamori, A.; Matsumoto, K.; Koizumi, A.; Momose, K.; Eguchi, T.; et al. A comparative study of a new class of gastric acid suppressant agent named vonoparazan versus esomeprazole for the eradication of Helicobacter pylori. Digestion 2016, 94, 240–246. [Google Scholar] [CrossRef]
- Yamada, S.; Kawakami, T.; Nakatsugawa, Y.; Suzuki, T.; Fujii, H.; Tomatsuri, N.; Nakamura, H.; Sato, H.; Okuyama, Y.; Kimura, H.; et al. Usefulness of vonoprazan, a potassium ion-competitive acid blocker, for primary eradication of Helicobacter pylori. World J. Gastrointest. Pharmacol. Ther. 2016, 7, 550–555. [Google Scholar] [CrossRef]
- Nishizawa, T.; Maekawa, T.; Watanabe, N.; Harada, N.; Hosoda, Y.; Yoshinaga, M.; Yoshio, T.; Ohta, H.; Inoue, S.; Toyokawa, T.; et al. Clarithromycin Versus Metronidazole as First-line Helicobacter pylori Eradication: A Multicenter, Prospective, Randomized Controlled Study in Japan. J. Clin. Gastroenterol. 2015, 49, 468–471. [Google Scholar] [CrossRef] [PubMed]
- Sue, S.; Shibata, W.; Sasaki, T.; Kaneko, H.; Irie, K.; Kondo, M.; Maeda, S. Randomized trial of vonoprazan-based versus proton-pump inhibitor-based third-line triple therapy with sitafloxacin for Helicobacter pylori. J. Gastroenterol. Hepatol. 2018. [Google Scholar] [CrossRef]
- Marcus, E.A.; Inatomi, N.; Nagami, G.T.; Sachs, G.; Scott, D.R. The effects of varying acidity on Helicobacter pylori growth and the bactericidal efficacy of ampicillin. Aliment Pharmacol. Ther. 2012, 36, 972–979. [Google Scholar] [CrossRef] [PubMed]
- Mamori, S.; Higashida, A.; Kawara, F.; Ohnishi, K.; Takeda, A.; Senda, E.; Ashida, C.; Yamada, H. Age-dependent eradication of Helicobacter pylori in Japanese patients. World J. Gastroenterol. 2010, 16, 4176–4179. [Google Scholar] [CrossRef] [PubMed]
- Nishizawa, T.; Suzuki, H.; Fujimoto, A.; Kinoshita, H.; Yoshida, S.; Isomura, Y.; Toyoshima, A.; Kanai, T.; Yahagi, N.; Toyoshima, O. Effects of patient age and choice of antisecretory agent on success of eradication therapy for Helicobacter pylori infection. J. Clin. Biochem. Nutr. 2017, 60, 208–210. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Subject | First-Line Triple Therapy | Second-Line Triple Therapy | Third-Line Triple Therapy | |||
|---|---|---|---|---|---|---|
| Regimen | EPZ/AMX/CLR (n = 288) | VPZ/AMX/CLR (n = 290) | EPZ/AMX/MTZ (n = 74) | VPZ/AMX/MTZ (n = 60) | EPZ/AMX/STFX (n = 24) | VPZ/AMX/STFX (n = 57) |
| Age (mean ± SD) | 57.9 ± 12.2 | 60.2 ± 12.6 | 56.1 ± 13.0 | 58.3 ± 11.9 | 48.3 ± 9.88 | 50.7 ± 12.1 |
| Gender (male/female) | 160/128 | 175/115 | 36/38 | 30/30 | 16/8 | 25/32 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saito, Y.; Konno, K.; Sato, M.; Nakano, M.; Kato, Y.; Saito, H.; Serizawa, H. Vonoprazan-Based Third-Line Therapy Has a Higher Eradication Rate against Sitafloxacin-Resistant Helicobacter pylori. Cancers 2019, 11, 116. https://doi.org/10.3390/cancers11010116
Saito Y, Konno K, Sato M, Nakano M, Kato Y, Saito H, Serizawa H. Vonoprazan-Based Third-Line Therapy Has a Higher Eradication Rate against Sitafloxacin-Resistant Helicobacter pylori. Cancers. 2019; 11(1):116. https://doi.org/10.3390/cancers11010116
Chicago/Turabian StyleSaito, Yoshimasa, Kaho Konno, Moeka Sato, Masaru Nakano, Yukako Kato, Hidetsugu Saito, and Hiroshi Serizawa. 2019. "Vonoprazan-Based Third-Line Therapy Has a Higher Eradication Rate against Sitafloxacin-Resistant Helicobacter pylori" Cancers 11, no. 1: 116. https://doi.org/10.3390/cancers11010116
APA StyleSaito, Y., Konno, K., Sato, M., Nakano, M., Kato, Y., Saito, H., & Serizawa, H. (2019). Vonoprazan-Based Third-Line Therapy Has a Higher Eradication Rate against Sitafloxacin-Resistant Helicobacter pylori. Cancers, 11(1), 116. https://doi.org/10.3390/cancers11010116