Potential Applications of DNA, RNA and Protein Biomarkers in Diagnosis, Therapy and Prognosis for Colorectal Cancer: A Study from Databases to AI-Assisted Verification


Abstract
:1. Introduction
2. Results
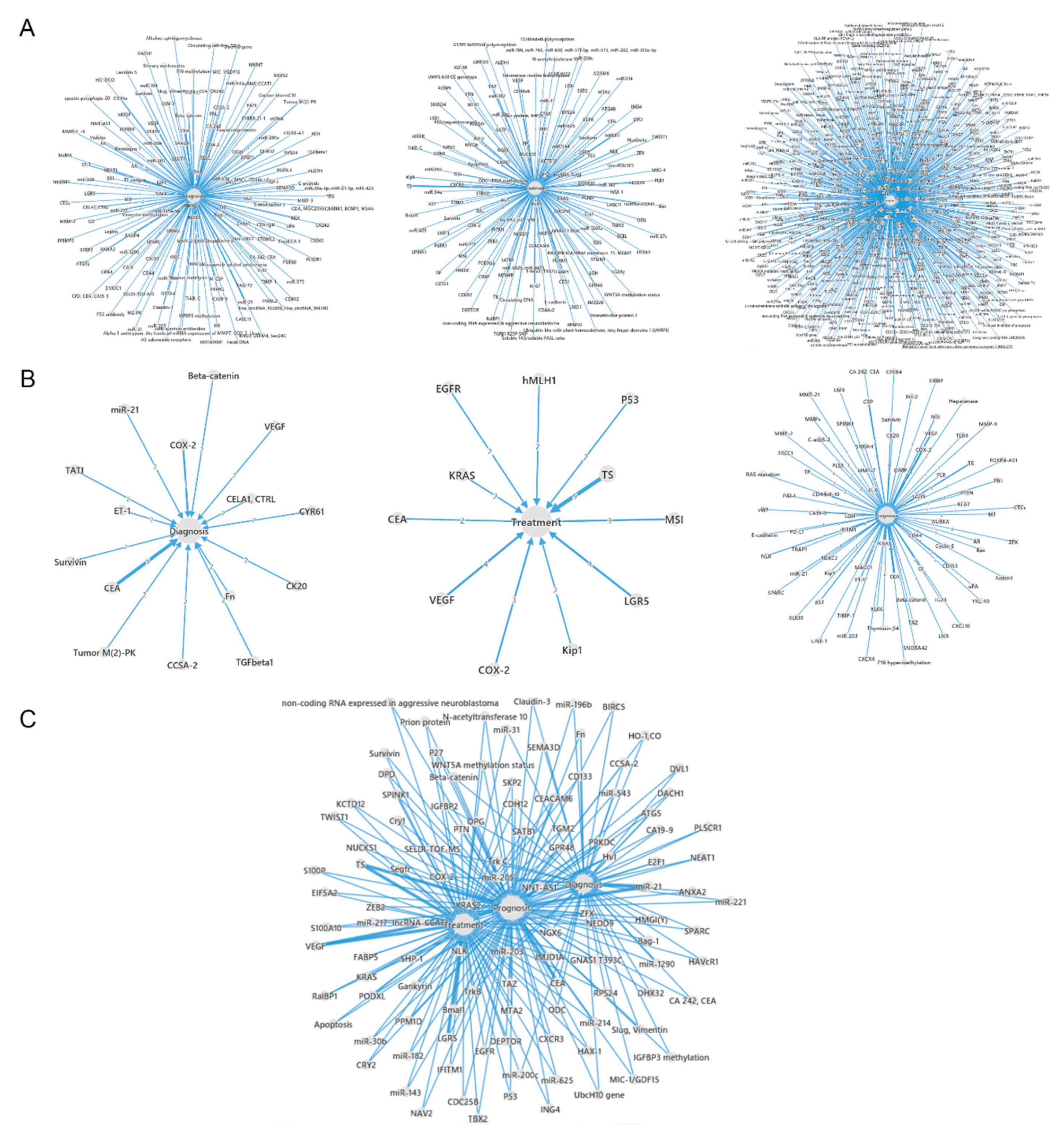
2.1. Applications of CRC Biomarkers and Their Interactions in Cancer Diagnosis, Therapy and Prognosis
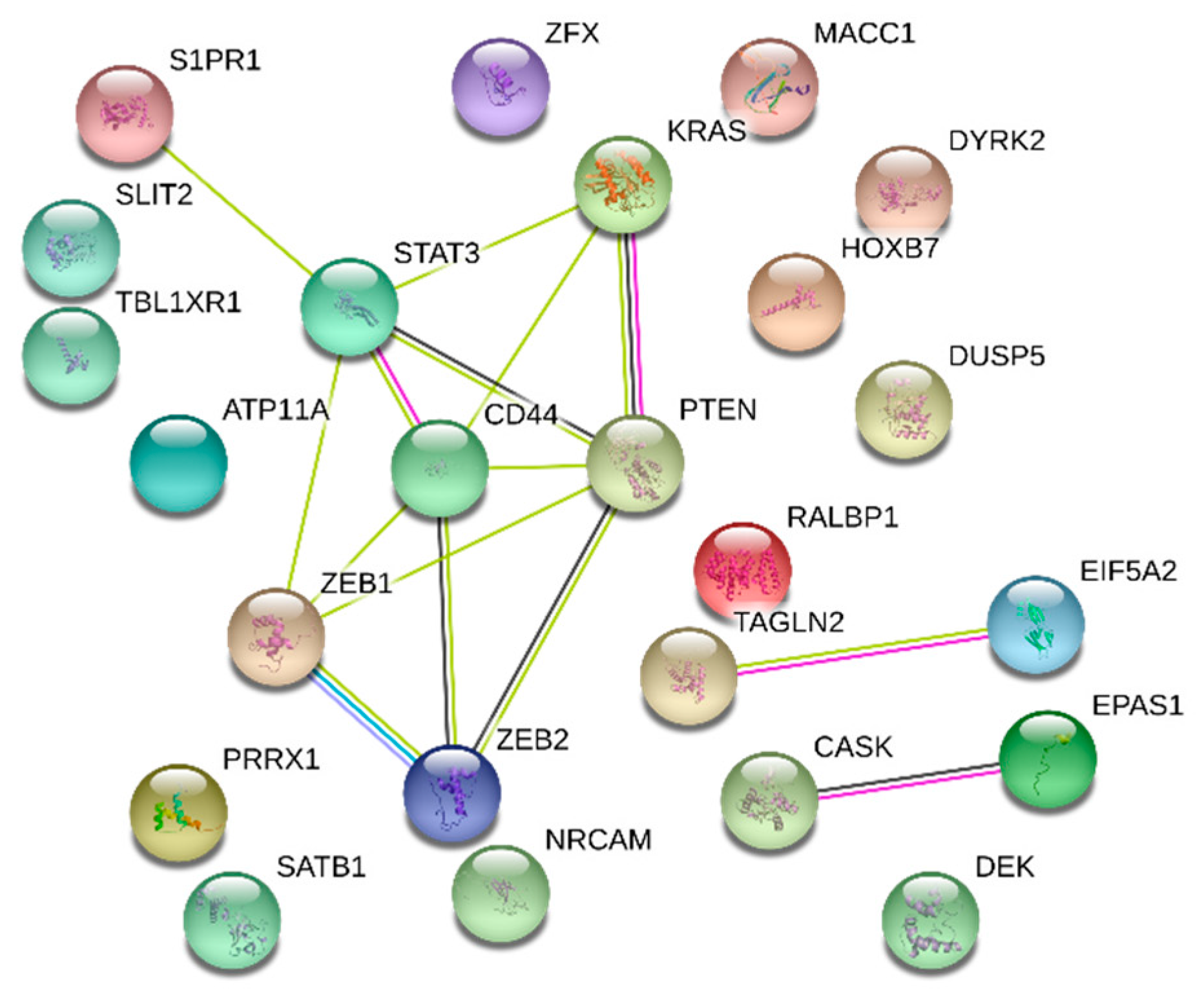
2.2. Applications of PPI Networks for CRC Diagnostic, Therapeutic and Prognostic Protein Biomarkers
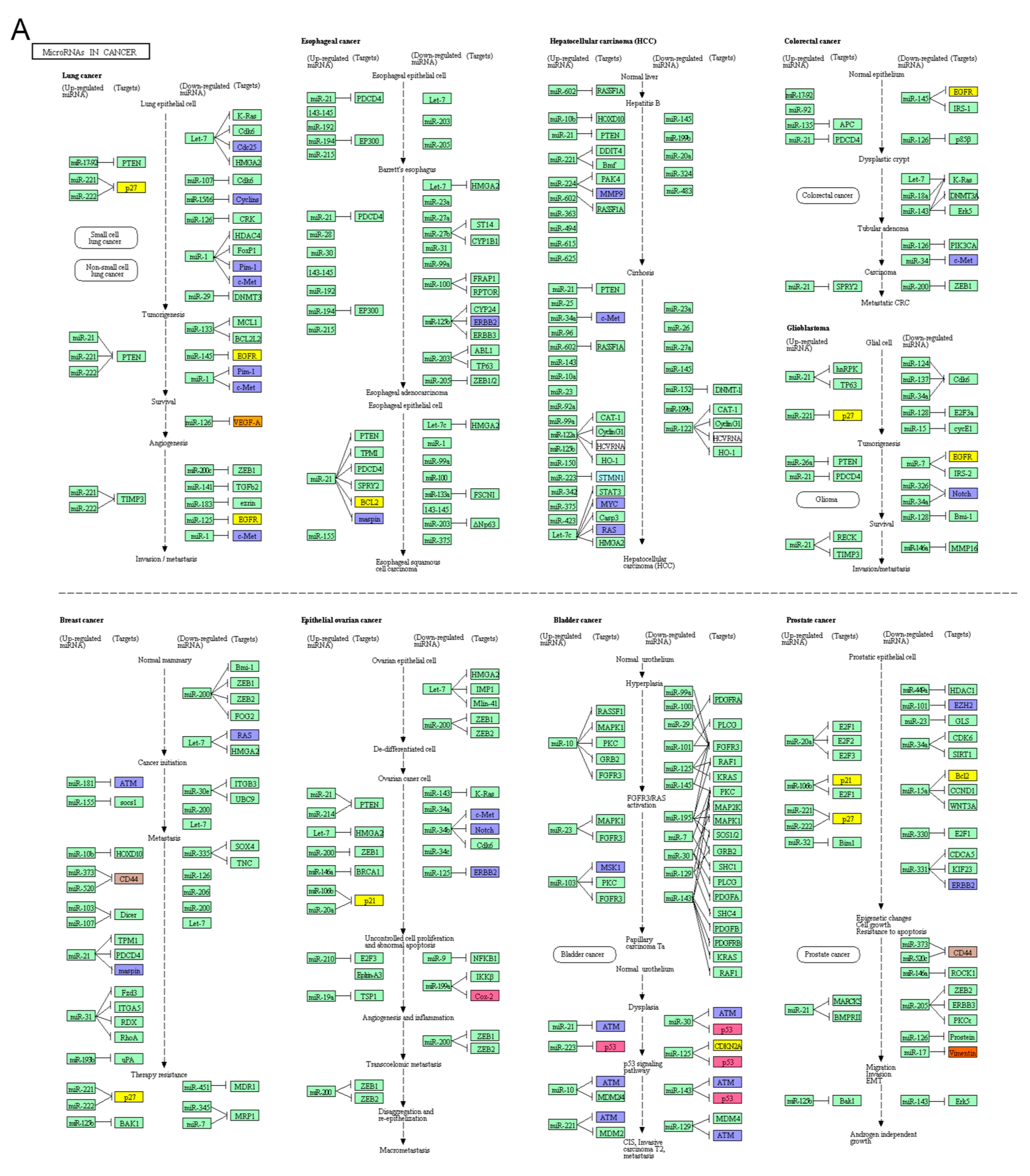
2.3. CRC Biomarkers in Pathway in Cancer and miRNAs in Cancer Pathway
2.4. miRNAs and Proteins Biomarkers for CRC Diagnosis, Therapy and Prognosis
2.5. Prognostic DNA Biomarkers in CRC
2.6. Verifications of Protein Biomarkers in Diagnosis and Prognosis
3. Discussion
4. Materials and Methods
4.1. Data Collection and Construction of the CRC Biomarker Application Networks
4.2. Systematic Analysis for the CRC Protein Biomarkers
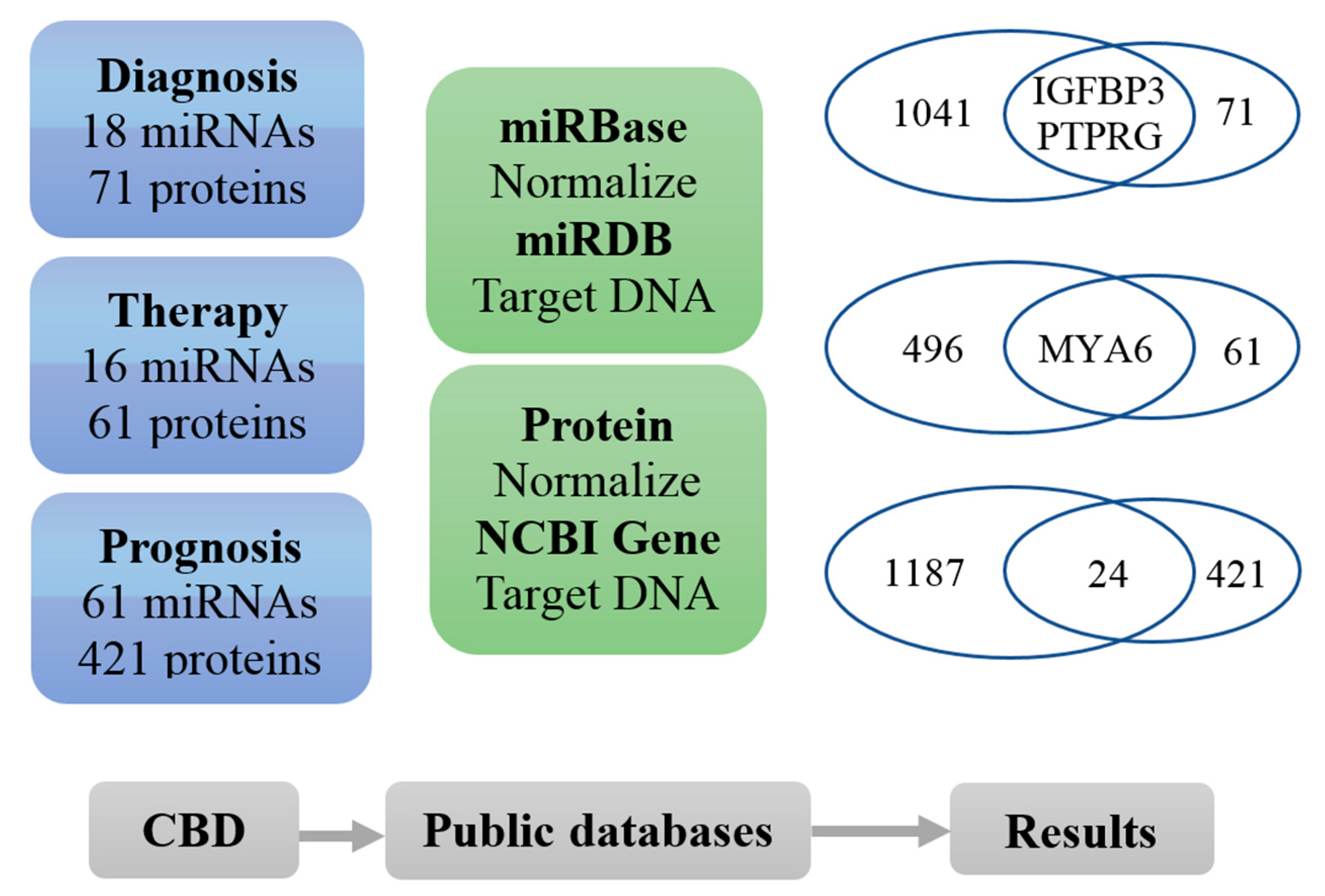
4.3. Overlapping Analysis of miRNA and Protein Biomarkers
4.4. AI-assisted Verification
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fedewa, S.A.; Ahnen, D.J.; Meester, R.G.S.; Barzi, A. Colorectal cancer statistics, 2017. CA Cancer J. Clin. 2017, 67, 177–193. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.; Jones, E.; Vidart, V.; Kuppen, P.J.; Conti, J.A.; Francis, N.K. Biomarkers for early detection of colorectal cancer and polyps: Systematic review. Cancer Epidemiol. Biomark. Prev. 2014, 23, 1712–1728. [Google Scholar] [CrossRef] [PubMed]
- SEER. Available online: http://seer.cancer.gov/statfacts/html/colorect.html (accessed on 31 January 2019).
- Brenner, H.; Kloor, M.; Pox, C.P. Colorectal cancer. Lancet 2014, 383, 1490–1502. [Google Scholar] [CrossRef]
- Center, M.M.; Jemal, A.; Smith, R.A.; Ward, E. Worldwide variations in colorectal cancer. CA Cancer J. Clin. 2009, 59, 366–378. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.H.; Bode, A.M.; Dong, Z. Precision medicine: The foundation of future cancer therapeutics. NPJ Precis. Oncol. 2017, 1, 12. [Google Scholar] [CrossRef] [PubMed]
- Henry, N.L.; Hayes, D.F. Cancer biomarkers. Mol. Oncol. 2012, 6, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Sun, X.F.; Cao, Y.; Ye, B.; Peng, Q.; Liu, X.; Shen, B.; Zhang, H. CBD: A biomarker database for colorectal cancer. Database 2018. [Google Scholar] [CrossRef]
- Schirripa, M.; Lenz, H.J. Biomarker in Colorectal Cancer. Cancer J. 2016, 22, 156–164. [Google Scholar] [CrossRef]
- Lin, Y.; Qian, F.; Shen, L.; Chen, F.; Chen, J.; Shen, B. Computer-aided biomarker discovery for precision medicine: Data resources, models and applications. Brief. Bioinform. 2017. [Google Scholar] [CrossRef]
- Lobdell, D.T.; Mendola, P. Development of a biomarkers database for the National Children’s Study. Toxicol. Appl. Pharmacol. 2005, 206, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Yerlikaya, S.; Broger, T.; MacLean, E.; Pai, M.; Denkinger, C.M. A tuberculosis biomarker database: The key to novel TB diagnostics. Int. J. Infect. Dis. 2017, 56, 253–257. [Google Scholar] [CrossRef] [PubMed]
- Yang, I.S.; Ryu, C.; Cho, K.J.; Kim, J.K.; Ong, S.H.; Mitchell, W.P.; Kim, B.S.; Oh, H.B.; Kim, K.H. IDBD: Infectious disease biomarker database. Nucleic Acids Res. 2008, 36, D455–D460. [Google Scholar] [CrossRef]
- Dai, H.J.; Wu, J.C.; Lin, W.S.; Reyes, A.J.; Dela Rosa, M.A.; Syed-Abdul, S.; Tsai, R.T.; Hsu, W.L. LiverCancerMarkerRIF: A liver cancer biomarker interactive curation system combining text mining and expert annotations. Database 2014. [Google Scholar] [CrossRef] [PubMed]
- Osumi, H.; Shinozaki, E.; Suenaga, M.; Matsusaka, S.; Konishi, T.; Akiyoshi, T.; Fujimoto, Y.; Nagayama, S.; Fukunaga, Y.; Ueno, M.; et al. RAS mutation is a prognostic biomarker in colorectal cancer patients with metastasectomy. Int. J. Cancer 2016, 139, 803–811. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.F.; Carstensen, J.M.; Zhang, H.; Stal, O.; Wingren, S.; Hatschek, T.; Nordenskjold, B. Prognostic significance of cytoplasmic p53 oncoprotein in colorectal adenocarcinoma. Lancet 1992, 340, 1369–1373. [Google Scholar] [CrossRef]
- Wang, M.J.; Ping, J.; Li, Y.; Adell, G.; Arbman, G.; Nodin, B.; Meng, W.J.; Zhang, H.; Yu, Y.Y.; Wang, C.; et al. The prognostic factors and multiple biomarkers in young patients with colorectal cancer. Sci Rep. 2015, 5, 10645. [Google Scholar] [CrossRef] [PubMed]
- Pathak, S.; Meng, W.J.; Nandy, S.K.; Ping, J.; Bisgin, A.; Helmfors, L.; Waldmann, P.; Sun, X.F. Radiation and SN38 treatments modulate the expression of microRNAs, cytokines and chemokines in colon cancer cells in a p53-directed manner. Oncotarget 2015, 6, 44758–44780. [Google Scholar] [CrossRef]
- Sun, X.F.; Ekberg, H.; Zhang, H.; Carstensen, J.M.; Nordenskjold, B. Overexpression of ras is an independent prognostic factor in colorectal adenocarcinoma. APMIS 1998, 106, 657–664. [Google Scholar] [CrossRef]
- Sun, X.F.; Bartik, Z.; Zhang, H. Bcl-2 expression is a prognostic factor in the subgroups of patients with colorectal cancer. Int. J. Oncol. 2003, 23, 1439–1443. [Google Scholar] [CrossRef]
- Iseki, Y.; Shibutani, M.; Maeda, K.; Nagahara, H.; Ikeya, T.; Hirakawa, K. Significance of E-cadherin and CD44 expression in patients with unresectable metastatic colorectal cancer. Oncol. Lett. 2017, 14, 1025–1034. [Google Scholar] [CrossRef] [PubMed]
- Ning, S.; Wei, W.; Li, J.; Hou, B.; Zhong, J.; Xie, Y.; Liu, H.; Mo, X.; Chen, J.; Zhang, L. Clinical significance and diagnostic capacity of serum TK1, CEA, CA 19-9 and CA 72-4 levels in gastric and colorectal cancer patients. J. Cancer 2018, 9, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Yuan, X.; Chen, J.; Lin, Y.; Li, Y.; Xu, L.; Chen, L.; Hua, H.; Shen, B. Network Biomarkers Constructed from Gene Expression and Protein-Protein Interaction Data for Accurate Prediction of Leukemia. J. Cancer 2017, 8, 278–286. [Google Scholar] [CrossRef]
- McGuire, A.; Brown, J.A.; Kerin, M.J. Metastatic breast cancer: The potential of miRNA for diagnosis and treatment monitoring. Cancer Metastasis. Rev. 2015, 34, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Shin, V.Y.; Chu, K.M. MiRNA as potential biomarkers and therapeutic targets for gastric cancer. World J. Gastroenterol. 2014, 20, 10432–10439. [Google Scholar] [CrossRef] [PubMed]
- De Robertis, M.; Poeta, M.L.; Signori, E.; Fazio, V.M. Current understanding and clinical utility of miRNAs regulation of colon cancer stem cells. Semin. Cancer Biol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Xiao, J.; Jing, Z.C.; Ellinor, P.T.; Liang, D.; Zhang, H.; Liu, Y.; Chen, X.; Pan, L.; Lyon, R.; Liu, Y.; et al. MicroRNA-134 as a potential plasma biomarker for the diagnosis of acute pulmonary embolism. J. Transl. Med. 2011, 9, 159. [Google Scholar] [CrossRef]
- Rong, H.; Liu, T.B.; Yang, K.J.; Yang, H.C.; Wu, D.H.; Liao, C.P.; Hong, F.; Yang, H.Z.; Wan, F.; Ye, X.Y.; et al. MicroRNA-134 plasma levels before and after treatment for bipolar mania. J. Psychiatr. Res. 2011, 45, 92–95. [Google Scholar] [CrossRef]
- Wang, X.; Luo, Y.; Liu, S.; Tan, L.; Wang, S.; Man, R. MicroRNA-134 plasma levels before and after treatment with valproic acid for epilepsy patients. Oncotarget 2017, 8, 72748–72754. [Google Scholar] [CrossRef]
- O’Brien, K.; Lowry, M.C.; Corcoran, C.; Martinez, V.G.; Daly, M.; Rani, S.; Gallagher, W.M.; Radomski, M.W.; MacLeod, R.A.; O’Driscoll, L. miR-134 in extracellular vesicles reduces triple-negative breast cancer aggression and increases drug sensitivity. Oncotarget 2015, 6, 32774–32789. [Google Scholar] [CrossRef]
- Wang, T.; Lv, M.; Shen, S.; Zhou, S.; Wang, P.; Chen, Y.; Liu, B.; Yu, L.; Hou, Y. Cell-free microRNA expression profiles in malignant effusion associated with patient survival in non-small cell lung cancer. PLoS ONE 2012, 7, e43268. [Google Scholar] [CrossRef]
- Lu, G.; Sun, Y.; An, S.; Xin, S.; Ren, X.; Zhang, D.; Wu, P.; Liao, W.; Ding, Y.; Liang, L. MicroRNA-34a targets FMNL2 and E2F5 and suppresses the progression of colorectal cancer. Exp. Mol. Pathol. 2015, 99, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.; Huang, Z.; Zhu, D.; Zhou, X.; Shan, X.; Qi, L.W.; Wu, L.; Cheng, W.; Zhu, J.; Zhang, L.; et al. A panel of microRNA signature in serum for colorectal cancer diagnosis. Oncotarget 2017, 8, 17081–17091. [Google Scholar] [CrossRef] [PubMed]
- Carpelan-Holmstrom, M.A.; Haglund, C.H.; Roberts, P.J. Differences in serum tumor markers between colon and rectal cancer. Comparison of CA 242 and carcinoembryonic antigen. Dis. Colon Rectum. 1996, 39, 799–805. [Google Scholar] [CrossRef] [PubMed]
- Han, M.; Liew, C.T.; Zhang, H.W.; Chao, S.; Zheng, R.; Yip, K.T.; Song, Z.Y.; Li, H.M.; Geng, X.P.; Zhu, L.X.; et al. Novel blood-based, five-gene biomarker set for the detection of colorectal cancer. Clin. Cancer Res. 2008, 14, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Komuro, Y.; Watanabe, T.; Tsurita, G.; Muto, T.; Nagawa, H. Evaluating the combination of molecular prognostic factors in tumor radiosensitivity in rectal cancer. Hepatogastroenterology 2005, 52, 666–671. [Google Scholar]
- Nakajima, T.E.; Yamada, Y.; Shimoda, T.; Matsubara, J.; Kato, K.; Hamaguchi, T.; Shimada, Y.; Okayama, Y.; Oka, T.; Shirao, K. Combination of O6-methylguanine-DNA methyltransferase and thymidylate synthase for the prediction of fluoropyrimidine efficacy. Eur. J. Cancer 2008, 44, 400–407. [Google Scholar] [CrossRef]
- Chen, H.; Sun, X.; Ge, W.; Qian, Y.; Bai, R.; Zheng, S. A seven-gene signature predicts overall survival of patients with colorectal cancer. Oncotarget 2017, 8, 95054–95065. [Google Scholar] [CrossRef]
- Ge, J.; Chen, Z.; Li, R.; Lu, T.; Xiao, G. Upregulation of microRNA-196a and microRNA-196b cooperatively correlate with aggressive progression and unfavorable prognosis in patients with colorectal cancer. Cancer Cell Int. 2014, 14, 128. [Google Scholar] [CrossRef]
- Tatsuta, S.; Tanaka, S.; Haruma, K.; Yoshihara, M.; Sumii, K.; Kajiyama, G.; Shimamoto, F. Combined expression of urokinase-type plasminogen activator and proliferating cell nuclear antigen at the deepest invasive portion correlates with colorectal cancer prognosis. Int. J. Oncol. 1997, 10, 125–129. [Google Scholar] [CrossRef]
- Hu, Y.; Gaedcke, J.; Emons, G.; Beissbarth, T.; Grade, M.; Jo, P.; Yeager, M.; Chanock, S.J.; Wolff, H.; Camps, J.; et al. Colorectal cancer susceptibility loci as predictive markers of rectal cancer prognosis after surgery. Genes Chromosomes Cancer 2018, 57, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Wang, X. Improving microRNA target prediction by modeling with unambiguously identified microRNA-target pairs from CLIP-ligation studies. Bioinformatics 2016, 32, 1316–1322. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pathway ID | Pathway Description | Counts | FDR |
|---|---|---|---|
| A. KEGG pathway enrichment for diagnosis biomarkers | |||
| 03010 | Ribosome | 6 | 0.00157 |
| 05200 | Pathways in cancer | 8 | 0.00213 |
| 04066 | HIF-1 signalling pathway | 5 | 0.00281 |
| 04310 | Wnt signalling pathway | 5 | 0.00765 |
| 05206 | MicroRNAs in cancer | 5 | 0.00803 |
| 05131 | Shigellosis | 3 | 0.049 |
| B. KEGG pathway enrichment for treatment biomarkers | |||
| 05200 | Pathways in cancer | 15 | 4.52 × 10−13 |
| 05219 | Bladder cancer | 7 | 6.28 × 10−10 |
| 05206 | MicroRNAs in cancer | 9 | 8.43 × 10−9 |
| 05161 | Hepatitis B | 8 | 1.56 × 10−7 |
| 05210 | Colorectal cancer | 6 | 3.78 × 10−7 |
| 04110 | Cell cycle | 7 | 9.35 × 10−7 |
| 05218 | Melanoma | 6 | 9.35 × 10−7 |
| 05215 | Prostate cancer | 6 | 2.7 × 10−6 |
| 05212 | Pancreatic cancer | 5 | 1.48 × 10−5 |
| 05220 | Chronic myeloid leukaemia | 5 | 2.48 × 10−5 |
| C. KEGG pathway enrichment for prognosis biomarkers | |||
| 05206 | MicroRNAs in cancer | 23 | 1.16 × 10−17 |
| 05219 | Bladder cancer | 13 | 1.47 × 10−14 |
| 05200 | Pathways in cancer | 26 | 3.98 × 10−13 |
| 04115 | p53 signalling pathway | 12 | 7.01 × 10−10 |
| 05166 | HTLV-I infection | 18 | 3.39 × 10−8 |
| 04060 | Cytokine-cytokine receptor interaction | 18 | 5.3 × 10−8 |
| 04151 | PI3K-Akt signalling pathway | 20 | 7.36 × 10−8 |
| 05215 | Prostate cancer | 11 | 1.15 × 10−7 |
| 05205 | Proteoglycans in cancer | 16 | 1.28 × 10−7 |
| Pathway ID | Pathway Description | Counts | FDR |
|---|---|---|---|
| A. GO analysis in biological process level for diagnosis biomarkers | |||
| Go:0042327 | Positive regulation of phosphorylation | 20 | 6.22 × 10−9 |
| Go:0045937 | Positive regulation of phosphate metabolic process | 21 | 6.22 × 10−9 |
| Go:0001934 | Positive regulation of protein phosphorylation | 19 | 1.42 × 10−8 |
| Go:0071822 | Protein complex subunit organization | 24 | 1.42 × 10−8 |
| Go:0042127 | Regulation of cell proliferation | 24 | 2.08 × 10−8 |
| Go:0042981 | Regulation of apoptotic process | 23 | 3.65 × 10−8 |
| Go:0048583 | Regulation of response to stimulus | 34 | 4.31 × 10−8 |
| Go:0043933 | Macromolecular complex subunit organization | 27 | 9.8 × 10−8 |
| Go:0043066 | Negative regulation of apoptotic process | 18 | 1.39 × 10−7 |
| Go:0008284 | Positive regulation of cell proliferation | 17 | 4.33 × 10−7 |
| B. GO analysis in biological process level for treatment biomarkers | |||
| GO:0060548 | Negative regulation of cell death | 20 | 7.29 × 10−11 |
| GO:0042981 | Regulation of apoptotic process | 21 | 5.27 × 10−9 |
| GO:0009628 | Response to abiotic stimulus | 19 | 8.77 × 10−9 |
| GO:0010941 | Regulation of cell death | 21 | 8.77 × 10−9 |
| GO:0043066 | Negative regulation of apoptotic process | 17 | 8.77 × 10−9 |
| GO:0031325 | Positive regulation of cellular metabolic process | 26 | 8.79 × 10−8 |
| GO:0010604 | Positive regulation of macromolecule metabolic process | 25 | 1.34 × 10−7 |
| GO:0009893 | Positive regulation of metabolic process | 28 | 1.89 × 10−7 |
| GO:0009605 | Response to external stimulus | 21 | 3.8 × 10−7 |
| GO:0048523 | Negative regulation of cellular process | 29 | 4.12 × 10−7 |
| C. GO analysis in biological process level for prognosis biomarkers | |||
| GO:0042127 | Regulation of cell proliferation | 76 | 3.63 × 10−29 |
| GO:0006950 | Response to stress | 100 | 4.56 × 10−21 |
| GO:0048731 | System development | 101 | 1.33 × 10−20 |
| GO:0048522 | Positive regulation of cellular process | 111 | 5.31 × 10−20 |
| GO:0048523 | Negative regulation of cellular process | 105 | 5.31 × 10−20 |
| GO:0031325 | Positive regulation of cellular metabolic process | 88 | 6.82 × 10−20 |
| GO:0048518 | Positive regulation of biological process | 119 | 8.49 × 10−20 |
| GO:0010604 | Positive regulation of macromolecule metabolic process | 84 | 2.55 × 10−19 |
| GO:0048519 | Negative regulation of biological process | 107 | 7.7 × 10−19 |
| GO:0051247 | Positive regulation of protein metabolic process | 60 | 1.19 × 10−18 |
| Pathway ID | Pathway Description | Counts | FDR |
|---|---|---|---|
| A. GO Analysis in molecular function level for diagnosis biomarkers | |||
| GO:0005515 | Protein binding | 44 | 2.81 × 10−10 |
| GO:0005102 | Receptor binding | 20 | 4.2 × 10−7 |
| GO:0042802 | Identical protein binding | 15 | 0.000526 |
| GO:0005488 | Binding | 53 | 0.00127 |
| GO:0001968 | Fibronectin binding | 3 | 0.0307 |
| GO:0005539 | Glycosaminoglycan binding | 6 | 0.0353 |
| GO:0003735 | Structural constituent of ribosome | 5 | 0.0358 |
| GO:0005126 | Cytokine receptor binding | 6 | 0.0358 |
| GO:0032403 | Protein complex binding | 9 | 0.0358 |
| GO:0019899 | Enzyme binding | 14 | 0.0365 |
| B. GO Analysis in molecular function level for treatment biomarkers | |||
| GO:0005515 | Protein binding | 36 | 3.52 × 10−10 |
| GO:0042802 | Identical protein binding | 16 | 8.85 × 10−7 |
| GO:0046983 | Protein dimerization activity | 13 | 1.15 × 10−5 |
| GO:0005488 | Binding | 42 | 0.000317 |
| GO:0019899 | Enzyme binding | 15 | 0.000317 |
| GO:0042803 | Protein homodimerization activity | 10 | 0.000445 |
| GO:0043566 | Structure-specific DNA binding | 7 | 0.00061 |
| GO:0046982 | Protein heterodimerization activity | 7 | 0.00061 |
| GO:0030983 | Mismatched DNA binding | 3 | 0.000839 |
| GO:0004861 | Cyclin-dependent protein serine/threonine kinase inhibitor activity | 3 | 0.00138 |
| C. GO Analysis in molecular function level for prognosis biomarkers | |||
| GO:0005515 | Protein binding | 131 | 4.67 × 10−29 |
| GO:0005102 | Receptor binding | 45 | 1.18 × 10−11 |
| GO:0044877 | Macromolecular complex binding | 44 | 1.98 × 10−11 |
| GO:0005488 | Binding | 160 | 2.91 × 10−9 |
| GO:0042802 | Identical protein binding | 35 | 1.63 × 10−7 |
| GO:0019899 | Enzyme binding | 41 | 5.39 × 10−7 |
| GO:0032403 | Protein complex binding | 25 | 6.42 × 10−7 |
| GO:0003684 | Damaged DNA binding | 9 | 8.98 × 10−6 |
| GO:0043566 | Structure-specific DNA binding | 15 | 1.09 × 10−5 |
| GO:0019900 | Kinase binding | 19 | 9.05 × 10−5 |
| Pathway ID | Pathway Description | Counts | FDR |
|---|---|---|---|
| A. GO analysis in cellular component level for diagnosis biomarkers | |||
| GO:0005615 | Extracellular space | 20 | 1.49 × 10−6 |
| GO:0022627 | Cytosolic small ribosomal subunit | 6 | 1.49 × 10−6 |
| GO:0031982 | Vesicle | 33 | 1.49 × 10−6 |
| GO:0031988 | Membrane-bounded vesicle | 32 | 2.34 × 10−6 |
| GO:0005576 | Extracellular region | 36 | 2.74 × 10−6 |
| GO:0044421 | Extracellular region part | 32 | 7.96 × 10−6 |
| GO:0034774 | Secretory granule lumen | 6 | 1.67 × 10−5 |
| GO:0022626 | Cytosolic ribosome | 6 | 8.62 × 10−5 |
| GO:0030141 | Secretory granule | 9 | 8.62 × 10−5 |
| GO:0031093 | Platelet alpha granule lumen | 5 | 8.62 × 10−5 |
| B. GO analysis in cellular component level for treatment biomarkers | |||
| GO:0005829 | Cytosol | 24 | 4.63 × 10−5 |
| GO:0044428 | Nuclear part | 26 | 4.63 × 10−5 |
| GO:0032991 | Macromolecular complex | 27 | 0.000117 |
| GO:0043233 | Organelle lumen | 26 | 0.000117 |
| GO:0043234 | Protein complex | 25 | 0.000117 |
| GO:0044427 | Chromosomal part | 11 | 0.000117 |
| GO:0031981 | Nuclear lumen | 23 | 0.000149 |
| GO:0005654 | Nucleoplasm | 21 | 0.000153 |
| GO:0005694 | Chromosome | 11 | 0.000164 |
| GO:0070013 | Intracellular organelle lumen | 24 | 0.000662 |
| C. GO analysis in cellular component level for prognosis biomarkers | |||
| GO:0005576 | Extracellular region | 96 | 1.33 × 10−10 |
| GO:0005615 | Extracellular space | 46 | 1.62 × 10−10 |
| GO:0044421 | Extracellular region part | 85 | 1.96 × 10−10 |
| GO:0005829 | Cytosol | 72 | 6.05 × 10−8 |
| GO:0005912 | Adherens junction | 23 | 1.13 × 10−7 |
| GO:0005924 | Cell-substrate adherens junction | 21 | 2.33 × 10−7 |
| GO:0043227 | Membrane-bounded organelle | 163 | 3.07 × 10−7 |
| GO:0009986 | Cell surface | 28 | 3.94 × 10−7 |
| GO:0005925 | Focal adhesion | 20 | 6.84 × 10−7 |
| GO:0031982 | Vesicle | 73 | 1.04 × 10−6 |
| Pathway ID | Pathway Description | Counts | FDR |
|---|---|---|---|
| A. KEGG pathway enrichment for overlapping DNA transferred by prognosis biomarkers | |||
| 05206 | MicroRNAs in cancer | 5 | 0.000171 |
| 04068 | FoxO signalling pathway | 3 | 0.0466 |
| 05200 | Pathways in cancer | 4 | 0.0466 |
| B. GO analysis result in biological process level for overlapping DNA transferred by prognosis biomarkers | |||
| GO:0009887 | Organ morphogenesis | 9 | 0.00107 |
| GO:0010468 | Regulation of gene expression | 16 | 0.00107 |
| GO:0010557 | Positive regulation of macromolecule biosynthetic process | 11 | 0.00107 |
| GO:0010628 | Positive regulation of gene expression | 11 | 0.00107 |
| GO:2000112 | Regulation of cellular macromolecule biosynthetic process | 15 | 0.00107 |
| GO:0031328 | Positive regulation of cellular biosynthetic process | 11 | 0.00118 |
| GO:0048514 | Blood vessel morphogenesis | 6 | 0.00514 |
| GO:0010556 | Regulation of macromolecule biosynthetic process | 14 | 0.00588 |
| GO:0010604 | Positive regulation of macromolecule metabolic process | 12 | 0.00608 |
| GO:0001568 | Blood vessel development | 6 | 0.00631 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, X.; Sun, X.-F.; Shen, B.; Zhang, H. Potential Applications of DNA, RNA and Protein Biomarkers in Diagnosis, Therapy and Prognosis for Colorectal Cancer: A Study from Databases to AI-Assisted Verification. Cancers 2019, 11, 172. https://doi.org/10.3390/cancers11020172
Zhang X, Sun X-F, Shen B, Zhang H. Potential Applications of DNA, RNA and Protein Biomarkers in Diagnosis, Therapy and Prognosis for Colorectal Cancer: A Study from Databases to AI-Assisted Verification. Cancers. 2019; 11(2):172. https://doi.org/10.3390/cancers11020172
Chicago/Turabian StyleZhang, Xueli, Xiao-Feng Sun, Bairong Shen, and Hong Zhang. 2019. "Potential Applications of DNA, RNA and Protein Biomarkers in Diagnosis, Therapy and Prognosis for Colorectal Cancer: A Study from Databases to AI-Assisted Verification" Cancers 11, no. 2: 172. https://doi.org/10.3390/cancers11020172
APA StyleZhang, X., Sun, X. -F., Shen, B., & Zhang, H. (2019). Potential Applications of DNA, RNA and Protein Biomarkers in Diagnosis, Therapy and Prognosis for Colorectal Cancer: A Study from Databases to AI-Assisted Verification. Cancers, 11(2), 172. https://doi.org/10.3390/cancers11020172