Clinical Characteristics of Osimertinib Responder in Non-Small Cell Lung Cancer Patients with EGFR-T790M Mutation

 , , , and
, , , and
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
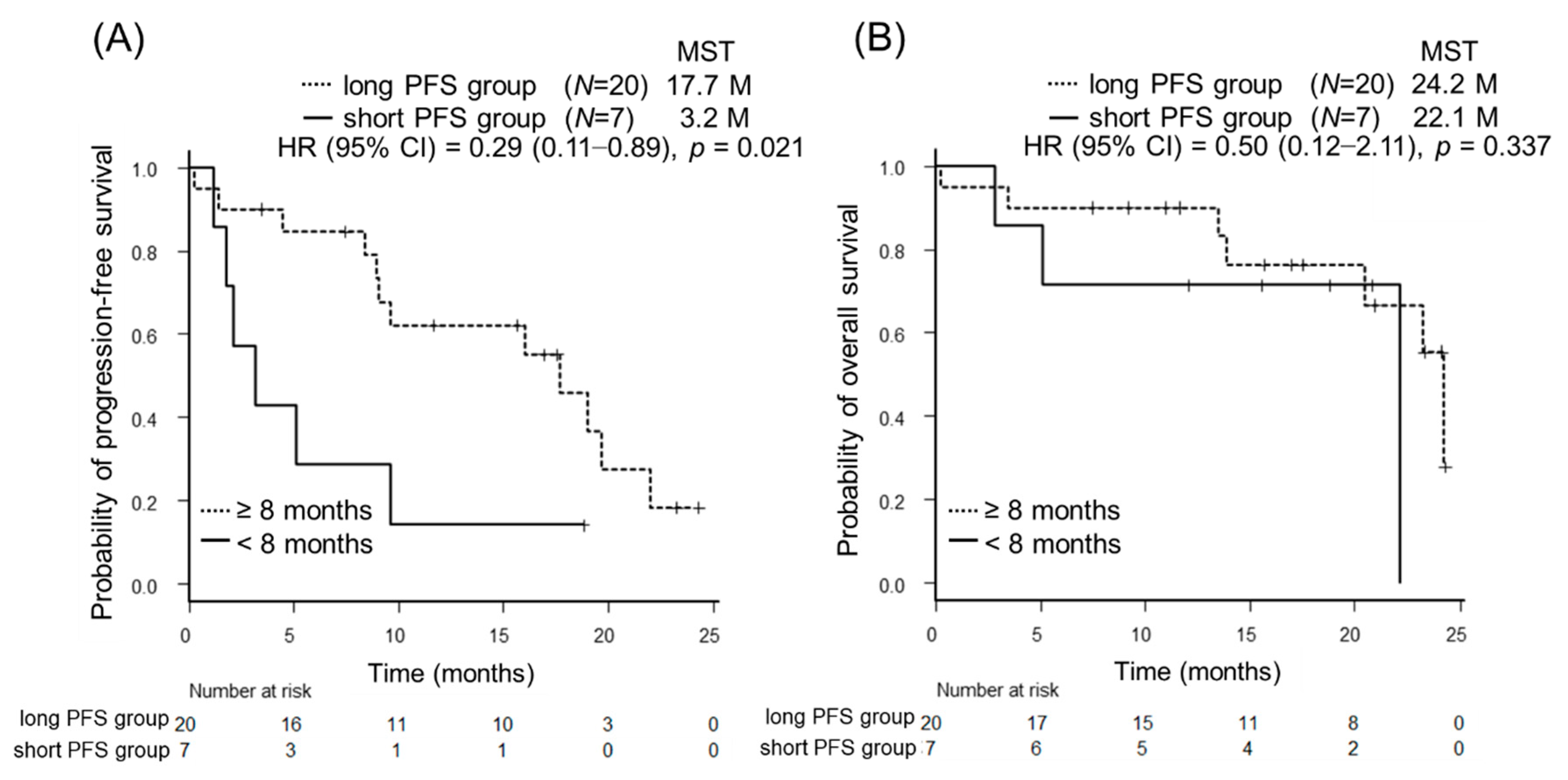
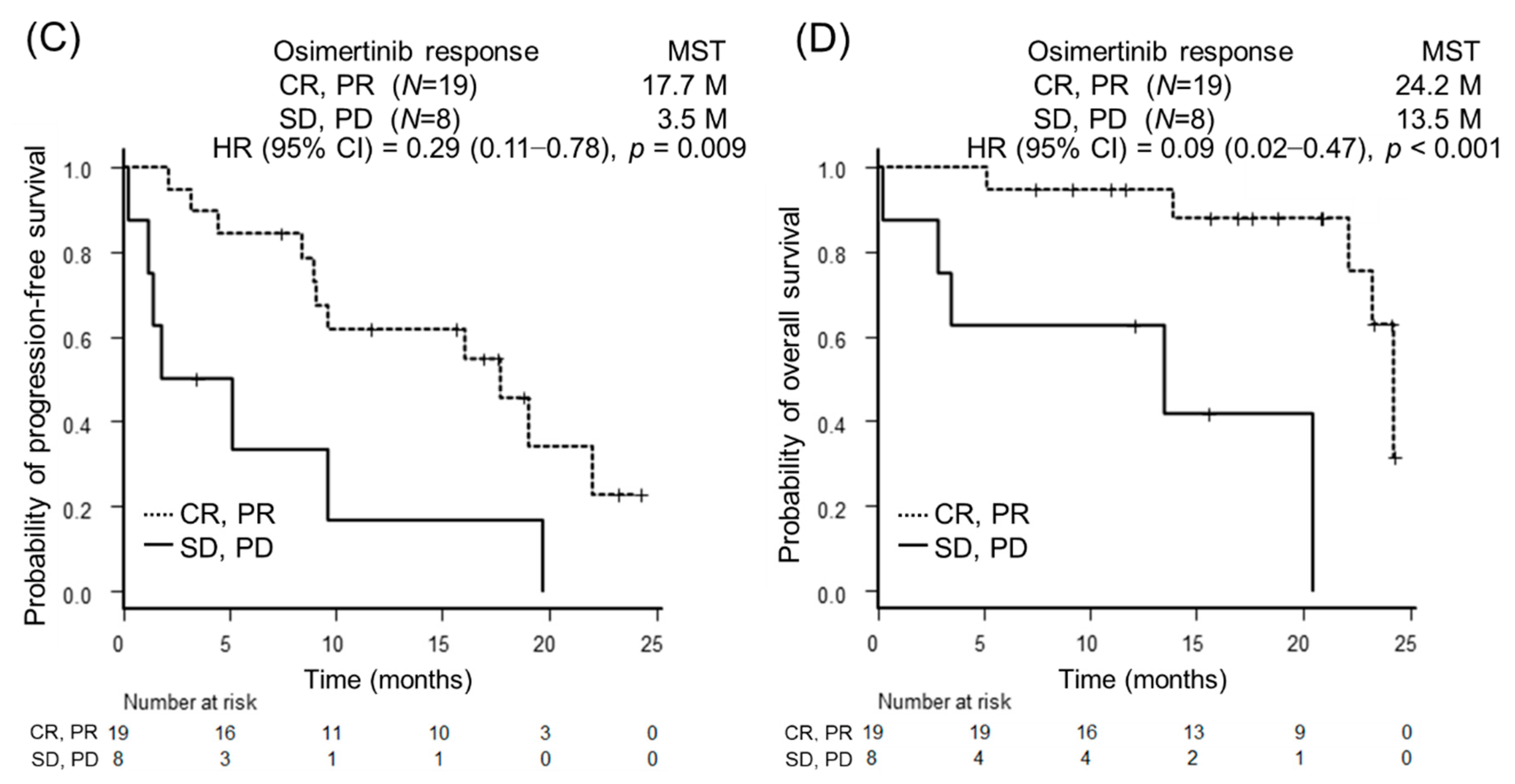
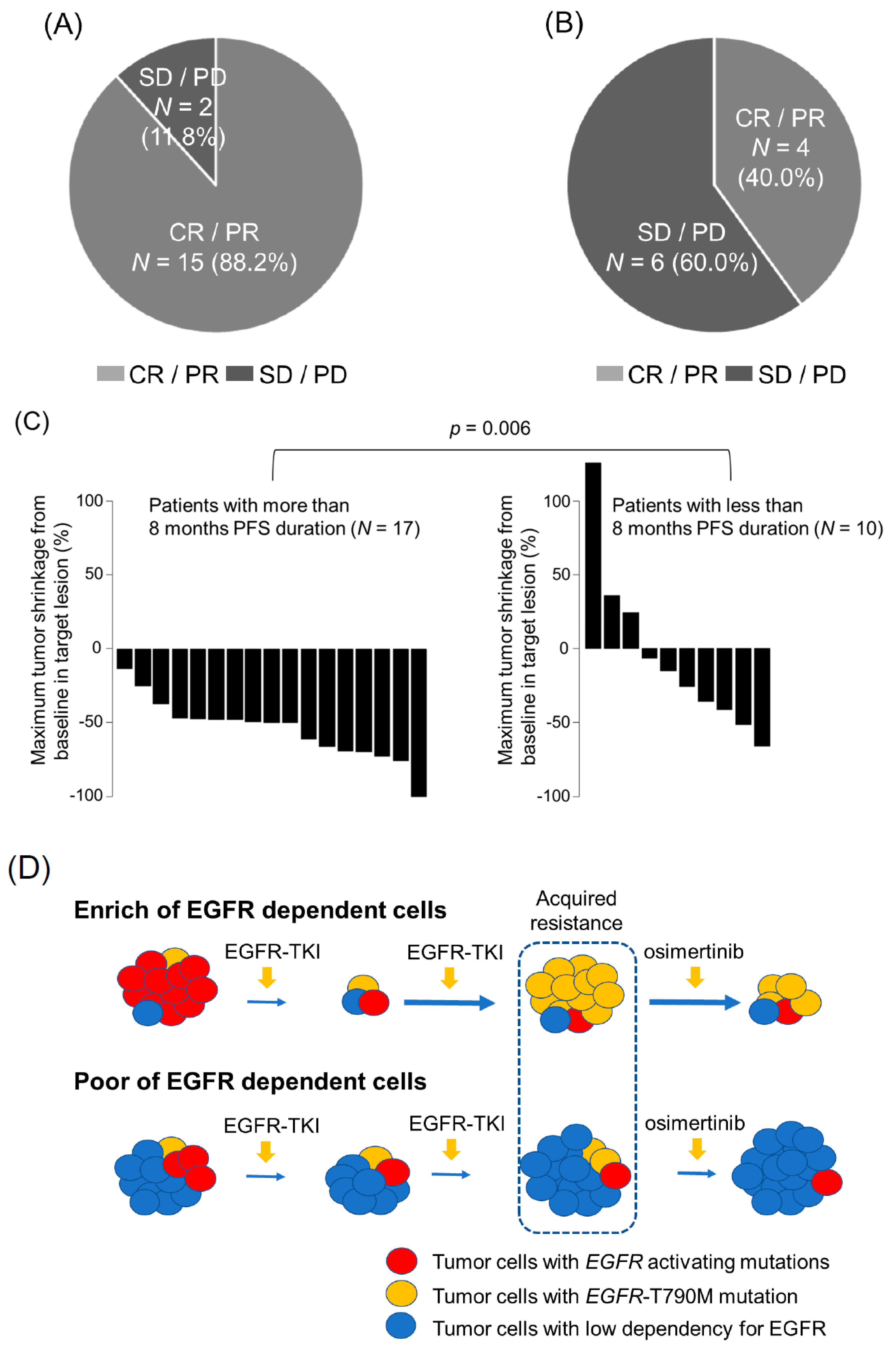
2.2. Predictor Factors in Osimertinib Treatment
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. EGFR Mutation Analysis
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Maemondo, M.; Inoue, A.; Kobayashi, K.; Sugawara, S.; Oizumi, S.; Isobe, H.; Gemmam, A.; Harada, M.; Yoshizawa, H.; Kinoshita, I.; et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N. Engl. J. Med. 2010, 362, 2380–2388. [Google Scholar] [CrossRef] [PubMed]
- Sequist, L.V.; Yang, J.C.; Yamamoto, N.; O’Byrne, K.; Hirsh, V.; Mok, T.; Geater, S.L.; Orlov, S.; Tsai, C.M.; Boyer, M.; et al. Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J. Clin. Oncol. 2013, 31, 3327–3334. [Google Scholar] [CrossRef] [PubMed]
- Sequist, L.V.; Waltman, B.A.; Dias-Santagata, D.; Digumarthy, S.; Turke, A.B.; Fidias, P.; Bergethon, K.; Shaw, A.T.; Gettinger, S.; Cosper, A.K.; et al. Genotypic and histological evolution of lung cancers acquiring resistance to EGFR inhibitors. Sci. Transl Med. 2011, 3, 75ra26. [Google Scholar] [CrossRef] [PubMed]
- Yano, S.; Takeuchi, S.; Nakagawa, T.; Yamada, T. Ligand-triggered resistance to molecular targeted drugs in lung cancer: Roles of hepatocyte growth factor and epidermal growth factor receptor ligands. Cancer Sci. 2012, 103, 1189–1194. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.G.; Liu, Y.N.; Tsai, M.F.; Chang, Y.L.; Yu, C.J.; Yang, P.C.; Yang, J.C.H.; Wen, Y.F.; Shih, J.Y. The mechanism of acquired resistance to irreversible EGFR tyrosine kinase inhibitor-afatinib in lung adenocarcinoma patients. Oncotarget 2016, 7, 12404–12413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mok, T.S.; Wu, Y.L.; Ahn, M.J.; Garassino, M.C.; Kim, H.R.; Ramalingam, S.S.; Shepherd, F.A.; He, Y.; Akamatsu, H.; Theelen, W.S.M.E.; et al. Osimertinib or Platinum-Pemetrexed in EGFR T790M-Positive Lung Cancer. N. Engl. J. Med. 2017, 376, 629–640. [Google Scholar] [CrossRef] [PubMed]
- Soria, J.C.; Ohe, Y.; Vansteenkiste, J.; Reungwetwattana, T.; Chewaskulyong, B.; Lee, K.H.; Dechaphunkul, A.; Imamura, F.; Nogami, N.; Kurata, T.; et al. Osimertinib in Untreated EGFR-Mutated Advanced Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Ariyasu, R.; Nishikawa, S.; Uchibori, K.; Oh-Hara, T.; Yoshizawa, T.; Dotsu, Y.; Koyama, J.; Saikia, M.; Sonodaa, T.; Kitazonoa, S.; et al. High ratio of T790M to EGFR activating mutations correlate with the osimertinib response in non-small-cell lung cancer. Lung Cancer 2018, 117, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Yoshimura, A.; Yamada, T.; Okura, N.; Takeda, T.; Furutani, W.; Kubota, Y.; Shiotsu, S.; Hiranuma, O.; Nishioka, N.; Chihara, Y.; et al. The impact of the tumor shrinkage by initial EGFR inhibitors according to the detection of EGFR-T790M mutation in patients with non-small cell lung cancer harboring EGFR mutations. BMC Cancer 2018, 18, 1241. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, Y.; Mitsudomi, T. Not all epidermal growth factor receptor mutations in lung cancer are created equal: Perspectives for individualized treatment strategy. Cancer Sci. 2016, 107, 1179–1186. [Google Scholar] [CrossRef] [PubMed]
- Kohsaka, S.; Nagano, M.; Ueno, T.; Suehara, Y.; Hayashi, T.; Shimada, N.; Takahashi, K.; Suzuki, K.; Takamochi, K.; Takahashi, F.; et al. A method of high-throughput functional evaluation of EGFR gene variants of unknown significance in cancer. Sci. Transl. Med. 2017, 9, eaan6566. [Google Scholar] [CrossRef] [PubMed]
- Janne, P.A.; Yang, J.C.; Kim, D.W.; Planchard, D.; Ohe, Y.; Ramalingam, S.S.; Ahn, M.J.; Kim, S.W.; Su, W.C.; Horn, L.; et al. AZD9291 in EGFR inhibitor-resistant non-small-cell lung cancer. N. Engl. J. Med. 2015, 372, 1689–1699. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Yan, B.; Zhang, Y.; Xu, J.; Qiao, R.; Dong, Y.; Zhang, B.; Zhao, Y.; Zhang, L.; Qian, J.; et al. Different characteristics and survival in non-small cell lung cancer patients with primary and acquired EGFR T790M mutation. Int. J. Cancer 2018. [Google Scholar] [CrossRef] [PubMed]
- Offin, M.; Rizvi, H.; Tenet, M.; Ni, A.; Sanchez-Vega, F.; Li, B.T.; Drilon, A.; Kris, M.G.; Rudin, C.M.; Schultz, N.; et al. Tumor Mutation Burden and Efficacy of EGFR-Tyrosine Kinase Inhibitors in Patients with EGFR-Mutant Lung Cancers. Clin. Cancer Res. 2018, 25, 1063–1069. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.H.; Hsiue, E.H.; Lee, J.H.; Lin, C.C.; Liao, W.Y.; Ho, C.C.; Shih, J.Y.; Yu, C.J.; Yang, C.H. Best Response According to RECIST During First-line EGFR-TKI Treatment Predicts Survival in EGFR Mutation-positive Non-Small-cell Lung Cancer Patients. Clin. Lung Cancer 2018, 19, e361–e372. [Google Scholar] [CrossRef] [PubMed]
- Thress, K.S.; Paweletz, C.P.; Felip, E.; Cho, B.C.; Stetson, D.; Dougherty, B.; Lai, Z.; Markovets, A.; Vivancos, A.; Kuang, Y.; et al. Acquired EGFR C797S mutation mediates resistance to AZD9291 in non-small cell lung cancer harboring EGFR T790M. Nat Med. 2015, 21, 560–562. [Google Scholar] [CrossRef] [PubMed]
- Minari, R.; Bordi, P.; Tiseo, M. Third-generation epidermal growth factor receptor-tyrosine kinase inhibitors in T790M-positive non-small cell lung cancer: Review on emerged mechanisms of resistance. Trans. Lung Cancer Res. 2016, 5, 695–708. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Yang, N.; Ou, Q.; Xiang, Y.; Jiang, T.; Wu, X.; Bao, H.; Tong, X.; Wang, X.; Shao, Y.W.; et al. Investigating Novel Resistance Mechanisms to Third-Generation EGFR Tyrosine Kinase Inhibitor Osimertinib in Non-Small Cell Lung Cancer Patients. Clin. Cancer Res. 2018, 24, 3097–3107. [Google Scholar] [CrossRef] [PubMed]
- Akamatsu, H.; Koh, Y.; Ozawa, Y.; Fujimoto, D.; Hata, A.; Katakami, N.; Tomii, K.; Shimokawa, T.; Yamamoto, N. Osimertinib With Ramucirumab in EGFR-mutated, T790M-positive Patients With Progression During EGFR-TKI Therapy: Phase Ib Study. Clin. Lung Cancer 2018, 19, e871–e874. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, H.; Yamada, T.; Wang, R.; Tanimura, K.; Adachi, Y.; Nishiyama, A.; Tanimoto, A.; Takeuchi, S.; Araujo, L.H.; Boroni, M.; et al. AXL confers intrinsic resistance to osimertinib and advances the emergence of tolerant cells. Nat. Commun. 2019, 10, 259. [Google Scholar] [CrossRef] [PubMed]
- Oxnard, G.R.; Hu, Y.; Mileham, K.F.; Husain, H.; Costa, D.B.; Tracy, P.; Feeney, N.; Sholl, L.M.; Dahlberg, S.E.; Redig, A.J.; et al. Assessment of Resistance Mechanisms and Clinical Implications in Patients With EGFR T790M-Positive Lung Cancer and Acquired Resistance to Osimertinib. JAMA Oncology. 2018, 4, 1527–1537. [Google Scholar] [CrossRef] [PubMed]
- Ma, G.; Zhang, J.; Jiang, H.; Zhang, N.; Yin, L.; Li, W.; Zhou, Q. Epidermal growth factor receptor T790M mutation as a prognostic factor in EGFR-mutant non-small cell lung cancer patients that acquired resistance to EGFR tyrosine kinase inhibitors. Oncotarget 2017, 8, 99429–99437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urata, Y.; Katakami, N.; Morita, S.; Kaji, R.; Yoshioka, H.; Seto, T.; Iwamoto, Y.; Kanehara, M.; Fujimoto, D.; Ikeda, N.; et al. Randomized Phase III Study Comparing Gefitinib With Erlotinib in Patients With Previously Treated Advanced Lung Adenocarcinoma: WJOG 5108L. J. Clin. Oncol. 2016, 34, 3248–3257. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patients’ Characteristics | N = 27, n, (%) | |
|---|---|---|
| Age | Median (Range) | 78.0 (47.0–88.0) |
| Sex | Male | 9 (33.3) |
| Female | 18 (66.7) | |
| PS | 0, 1 | 25 (92.6) |
| 2 | 2 (7.4) | |
| Histology | Adenocarcinoma | 26 (96.3) |
| Squamous cell carcinoma | 1 (3.7) | |
| Smoking status | Never-smoker | 20 (74.1) |
| Ever-smoker | 4 (14.8) | |
| Current-smoker | 3 (11.1) | |
| Stage | III | 4 (14.8) |
| IV | 13 (48.1) | |
| Postoperative recurrence | 10 (37.0) | |
| EGFR mutation status | Exon 19 deletion | 20 (74.1) |
| Exon 21 L858R mutation | 7 (25.9) | |
| Initial EGFR-TKI | Gefitinib | 17 (63.0) |
| Erlotinib | 6 (22.2) | |
| Afatinib | 4 (14.8) | |
| Initial TKI response | CR, PR | 24 (88.9) |
| SD, PD | 3 (11.1) | |
| Patients’ Characteristics | PFS Duration of Osimertinib ≥ 8 Months | PFS Duration of Osimertinib < 8 Months | p Value | |
|---|---|---|---|---|
| N = 17 | N = 10 | |||
| n (%) | n (%) | |||
| Age | Median (Range) | 78.0 (49.0–88.0) | 71.0 (47.0–83.0) | 0.247 |
| Sex | Male | 5 (29.4) | 4 (40.0) | 0.683 |
| Female | 12 (70.6) | 6 (60.0) | ||
| PS | 0, 1 | 16 (94.1) | 9 (90.0) | 1 |
| 2 | 1 (5.9) | 1 (10.0) | ||
| Histology | Adenocarcinoma | 17 (100.0) | 9 (90.0) | 0.37 |
| Squamous cell carcinoma | 0 (0.0) | 1 (10.0) | ||
| Smoking status | Never-smoker | 12 (70.6) | 8 (80.0) | 0.678 |
| Smoker | 5 (29.4) | 2 (20.0) | ||
| Stage | III | 2 (11.8) | 2 (20.0) | 0.472 |
| IV | 7 (41.2) | 6 (60.0) | ||
| Postoperative recurrence | 8 (47.1) | 2 (20.0) | ||
| EGFR mutation status | Exon 19 deletion | 12 (70.6) | 8 (80.0) | 0.678 |
| Exon 21 L858R mutation | 5 (29.4) | 2 (20.0) | ||
| EGFR-TKI | Gefitinib | 11 (64.7) | 6 (60.0) | 0.195 |
| Erlotinib | 5 (29.4) | 1 (10.0) | ||
| Afatinib | 1 (5.9) | 3 (30.0) | ||
| Re-biopsy site | Intrathoracic | 12 (70.6) | 5 (50.0) | 0.623 |
| Extrathoracic | 2 (11.8) | 3 (30.0) | ||
| Liquid | 3 (17.6) | 2 (20.0) | ||
| Patients’ Characteristics | PFS Duration of Osimertinib ≥ 8 Months | PFS Duration of Osimertinib < 8 Months | p Value | |
|---|---|---|---|---|
| N =17 | N = 10 | |||
| n (%) | n (%) | |||
| PFS duration of initial TKI | ≥8 months | 15 (88.2) | 8 (80.0) | 0.065 |
| <8 months | 2 (11.8) | 2 (20.0) | ||
| Osimertinib response | CR/PR | 15 (88.2) | 4 (40.0) | 0.025 |
| SD/PD | 2 (11.8) | 6 (60.0) | ||
| Osimertinib shrinkage | Median (Range) | 50.0 (13.5–100.0) | 20.6 (−126.4–66.5) | 0.006 |
| Platinum doublet therapy after osimertinib | + | 0 (0.0) | 3 (30.0) | 0.041 |
| - | 17 (100.0) | 7 (70.0) | ||
| Variables | Progression-Free Survival | Overall Survival | ||||||
|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||
| HR, Mean (95% CI) | p Value | HR, Mean (95% CI) | p Value | HR, Mean (95% CI) | p Value | HR, Mean (95% CI) | p Value | |
| Age at detection of T790M (<75/≥75 years) | 1.38 (0.53–3.57) | 0.504 | 0.71 (0.20–2.55) | 0.603 | ||||
| Performance status (0–1/2) | 0.27 (0.06–1.26) | 0.073 | NE | 0.557 | ||||
| Disease stage (postoperative recurrence/ stage III or IV) | 0.31 (0.1–0.95) | 0.03 | 0.41 (0.12–1.41) | 0.16 | 0.30 (0.06–1.41) | 0.105 | ||
| EGFR status (exon19 deletion/exon21 L858R mutation) | 0.84 (0.45–1.58) | 0.177 | 1.53 (0.31–7.42) | 0.597 | ||||
| EGFR-TKI (afatinib/gefitinib, erlotinib) | 3.01 (0.81–11.16) | 0.084 | 4.05 (0.96–17) | 0.039 | 8.15 (1.10–60.38) | 0.04 | ||
| Initial EGFR-TKI response (CR, PR/SD, PD) | 0.63 (0.14–2.83) | 0.543 | 4.89 (0.61–39.16) | 0.099 | ||||
| Initial EGFR-TKI PFS (more than 8 months/less than 8 months) | 0.31 (0.11–0.89) | 0.021 | 0.30 (0.10–0.90) | 0.031 | 0.50 (0.12–2.11) | 0.337 | ||
| Re-biopsy (tissue/liquid) | 0.62 (0.17–2.31) | 0.476 | NE | 0.319 | ||||
| Osimetinib response (CR, PR/SD, PD) | 0.29 (0.11–0.78) | 0.009 | 0.44 (0.15–1.33) | 0.15 | 0.09 (0.02–0.47) | <0.001 | 0.02 (0.00–0.27) | 0.002 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshimura, A.; Yamada, T.; Okura, N.; Takeda, T.; Hirose, K.; Kubota, Y.; Shiotsu, S.; Hiranuma, O.; Chihara, Y.; Tamiya, N.; et al. Clinical Characteristics of Osimertinib Responder in Non-Small Cell Lung Cancer Patients with EGFR-T790M Mutation. Cancers 2019, 11, 365. https://doi.org/10.3390/cancers11030365
Yoshimura A, Yamada T, Okura N, Takeda T, Hirose K, Kubota Y, Shiotsu S, Hiranuma O, Chihara Y, Tamiya N, et al. Clinical Characteristics of Osimertinib Responder in Non-Small Cell Lung Cancer Patients with EGFR-T790M Mutation. Cancers. 2019; 11(3):365. https://doi.org/10.3390/cancers11030365
Chicago/Turabian StyleYoshimura, Akihiro, Tadaaki Yamada, Naoko Okura, Takayuki Takeda, Kazuki Hirose, Yutaka Kubota, Shinsuke Shiotsu, Osamu Hiranuma, Yusuke Chihara, Nobuyo Tamiya, and et al. 2019. "Clinical Characteristics of Osimertinib Responder in Non-Small Cell Lung Cancer Patients with EGFR-T790M Mutation" Cancers 11, no. 3: 365. https://doi.org/10.3390/cancers11030365
APA StyleYoshimura, A., Yamada, T., Okura, N., Takeda, T., Hirose, K., Kubota, Y., Shiotsu, S., Hiranuma, O., Chihara, Y., Tamiya, N., Kaneko, Y., Uchino, J., & Takayama, K. (2019). Clinical Characteristics of Osimertinib Responder in Non-Small Cell Lung Cancer Patients with EGFR-T790M Mutation. Cancers, 11(3), 365. https://doi.org/10.3390/cancers11030365