Analysis of Circulating Tumor Cells in Patients with Non-Metastatic High-Risk Prostate Cancer before and after Radiotherapy Using Three Different Enumeration Assays

 , , , ,
, , , ,  ,
,  and
and 
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
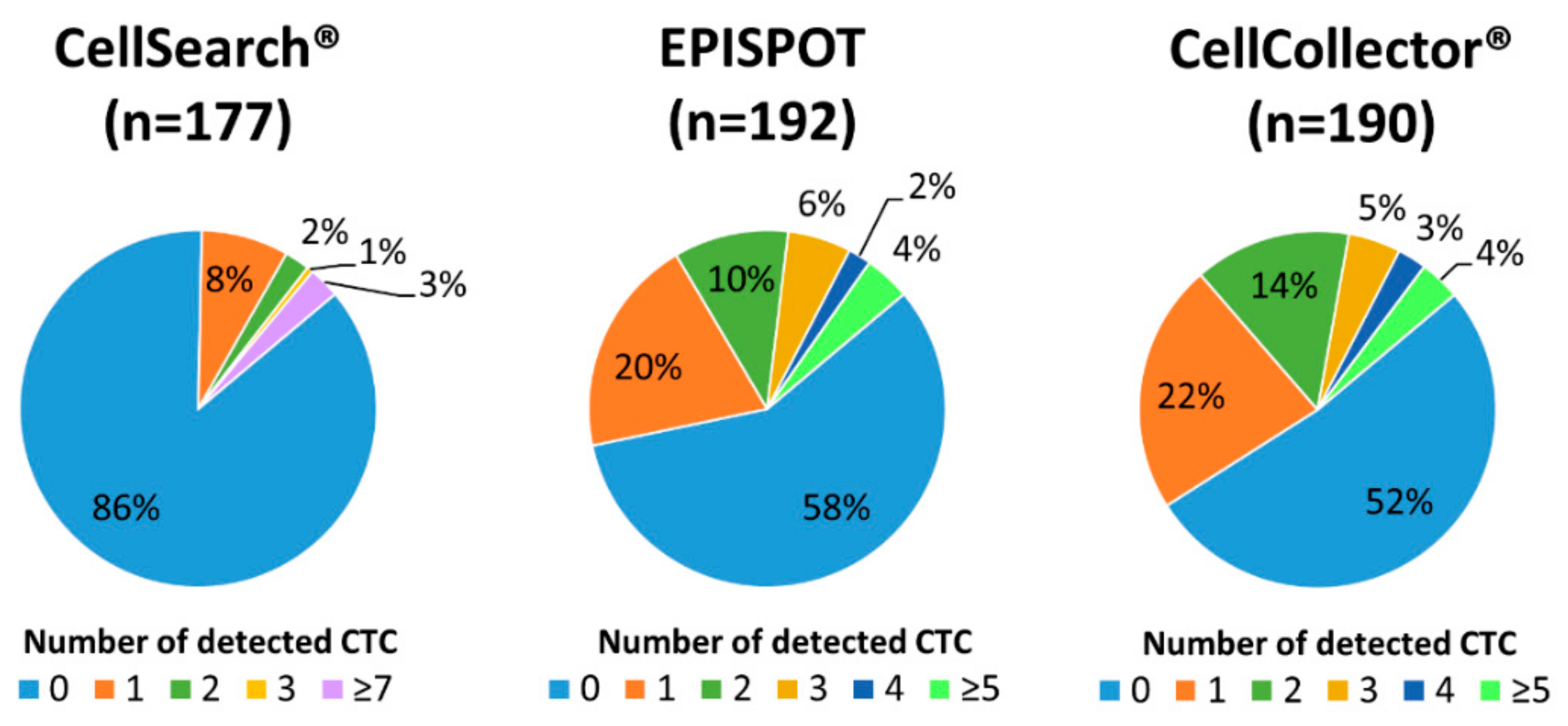
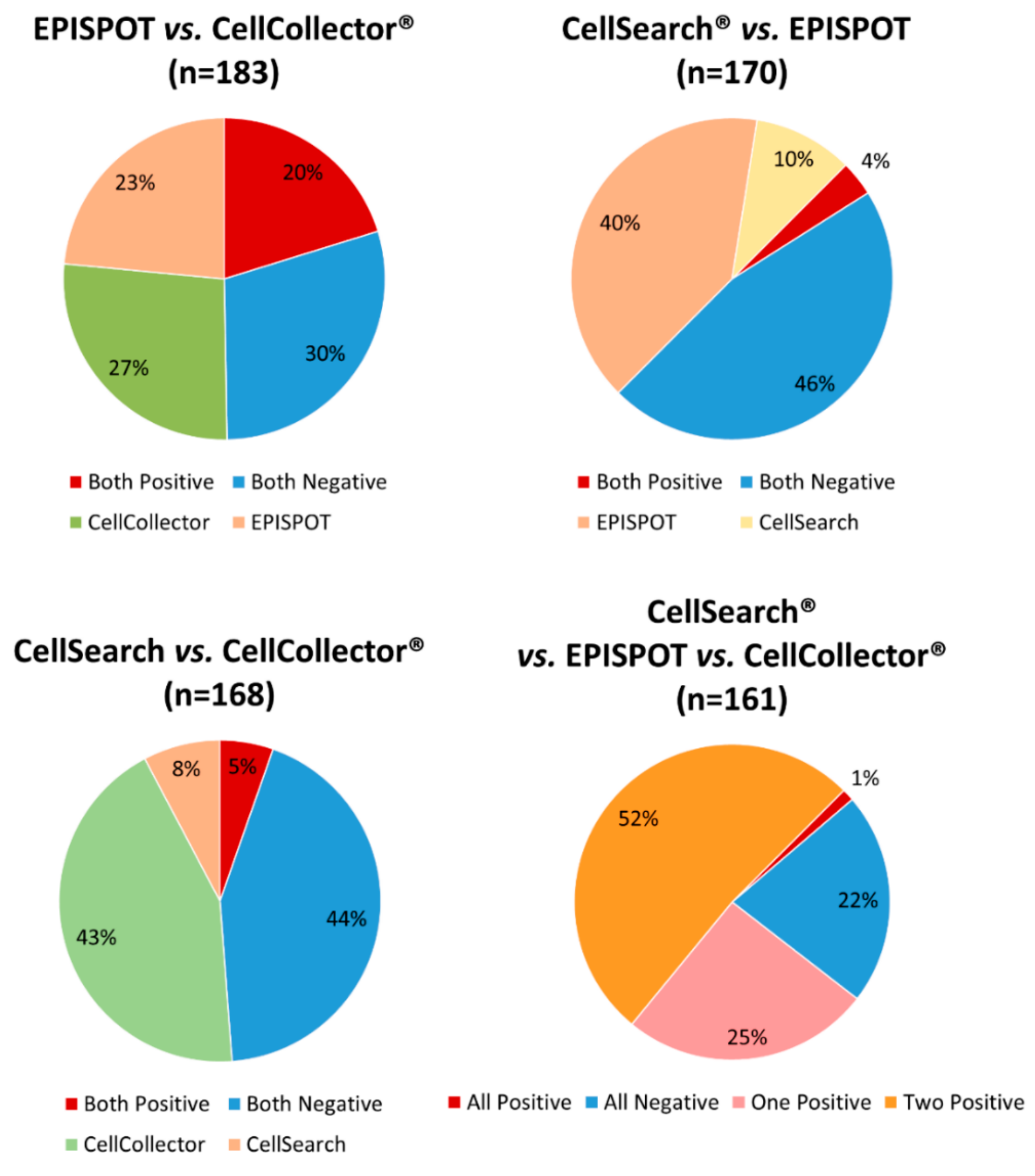
2.2. Comparison of CTC Detection Rate Obtained with Three Assays
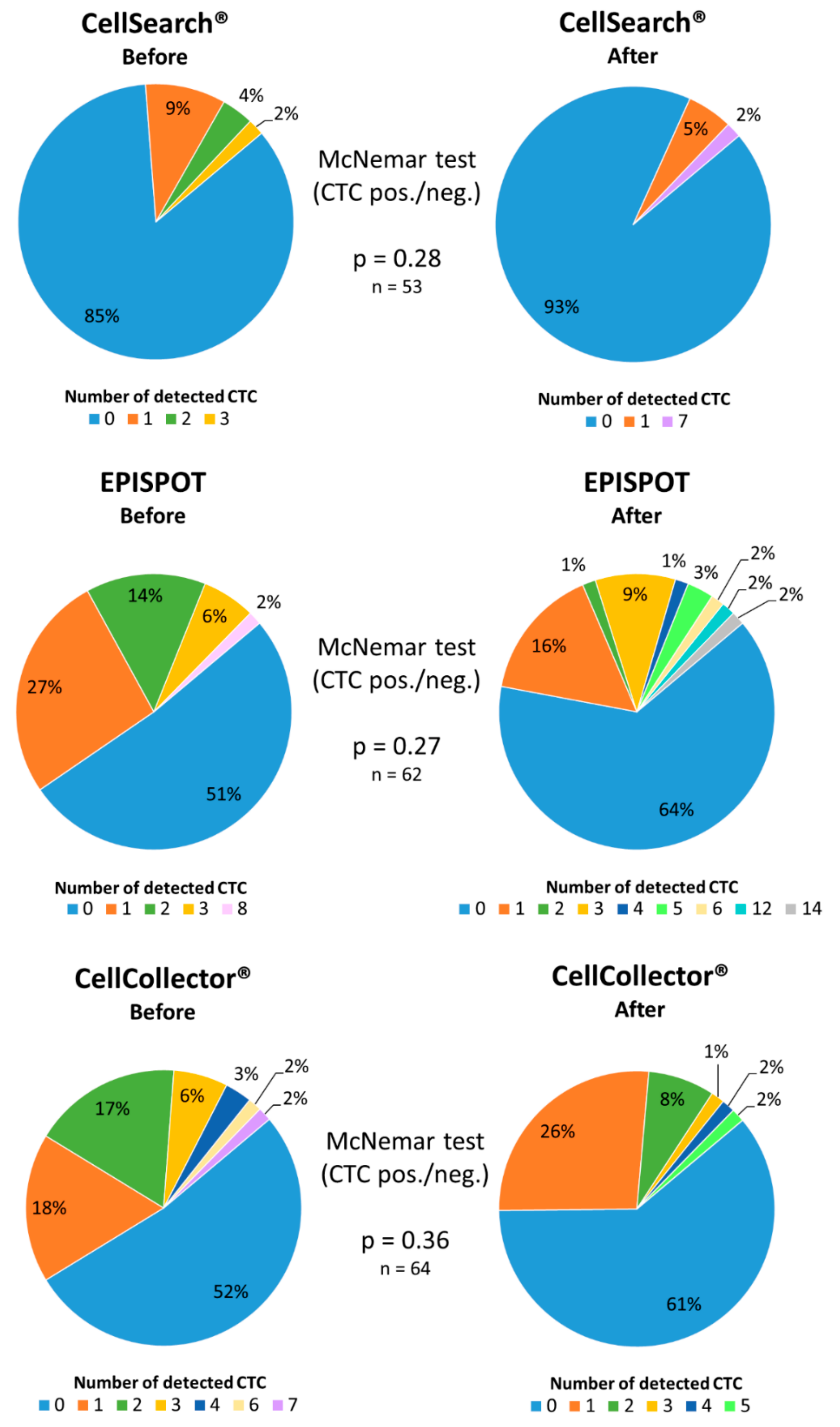
2.3. Analysis of Matched Blood Samples before and after Radiotherapy
2.4. Correlation Between CTC Count and Clinical Parameters
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. CTC Isolation and Detection
4.2.1. CellSearch® System
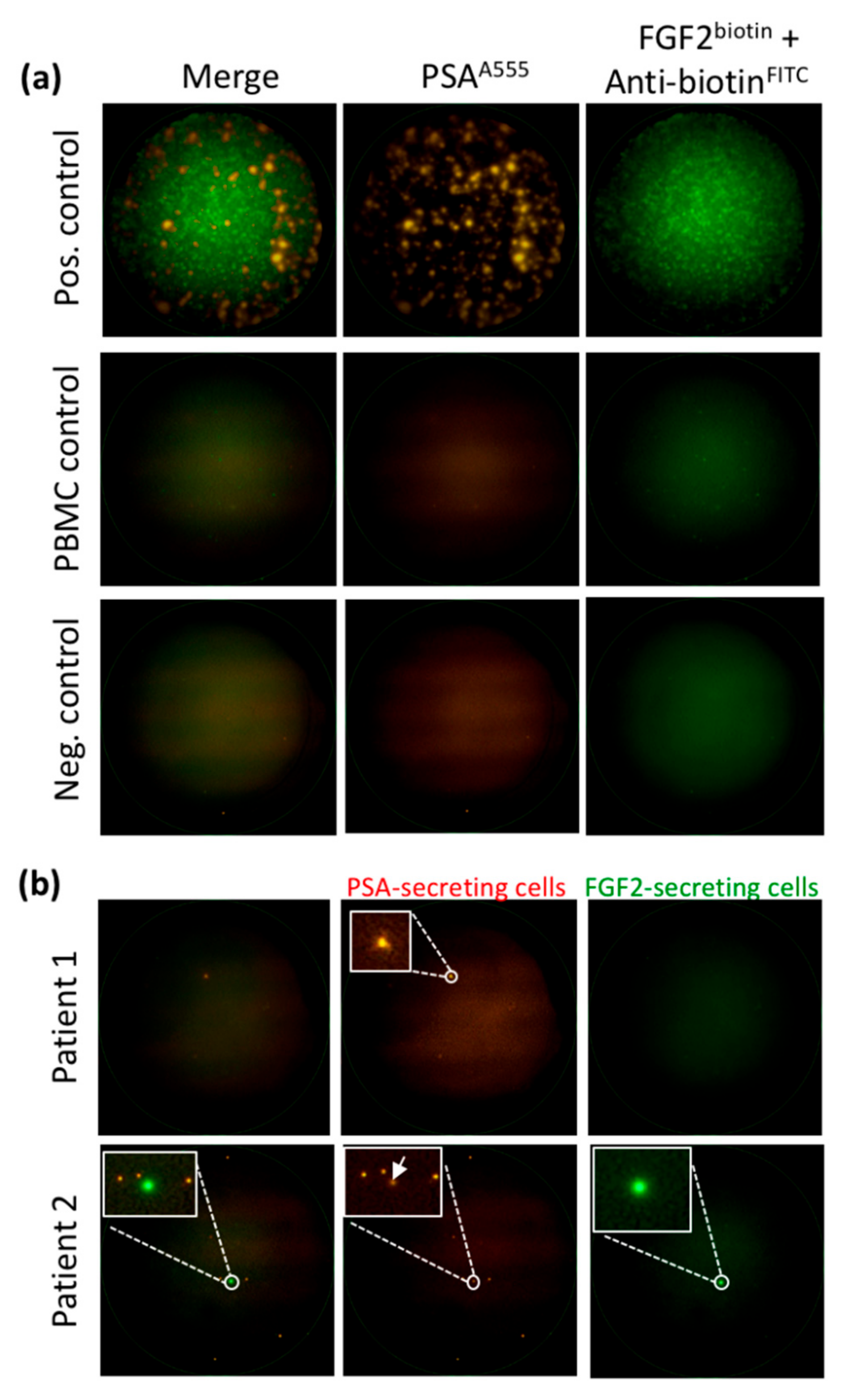
4.2.2. Dual Fluoro-EPISPOTPSA/FGF2 Assay
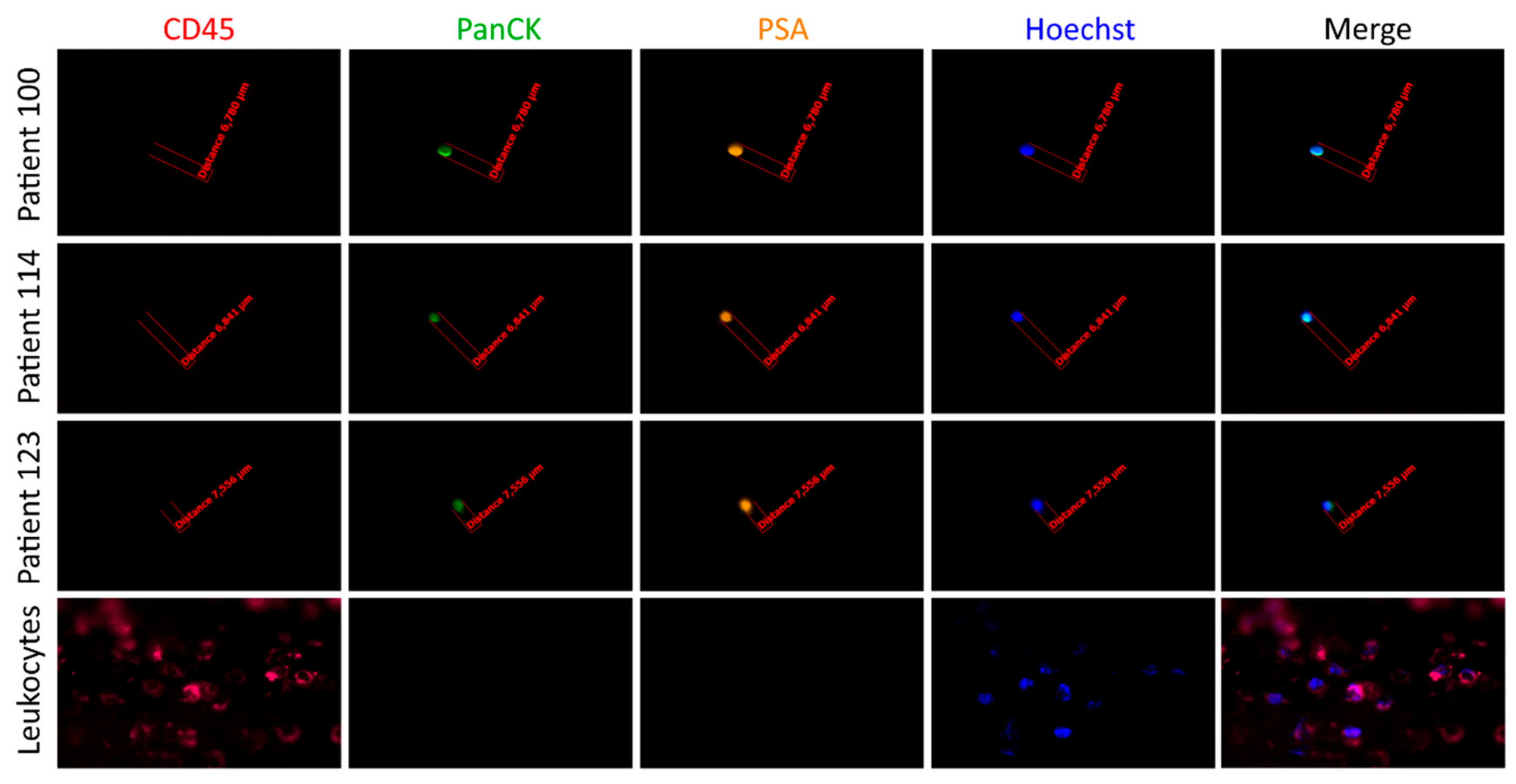
4.2.3. CellCollector®
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Scher, H.I.; Morris, M.J.; Larson, S.; Heller, G. Validation and clinical utility of prostate cancer biomarkers. Nat. Rev. Clin. Oncol. 2013, 10, 225–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, A.J.; Autio, K.A.; Roach, M.; Scher, H.I. High-risk prostate cancer-classification and therapy. Nat. Rev. Clin. Oncol. 2014, 11, 308–323. [Google Scholar] [CrossRef] [PubMed]
- Carter, H.B. Differentiation of lethal and non lethal prostate cancer: PSA and PSA isoforms and kinetics. Asian J. Androl. 2012, 14, 355–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andriole, G.L., Jr. PSA screening and prostate cancer risk reduction. Urol. Oncol. 2012, 30, 936–937. [Google Scholar] [CrossRef] [PubMed]
- Dimakakos, A.; Armakolas, A.; Koutsilieris, M. Novel tools for prostate cancer prognosis, diagnosis, and follow-up. Biomed Res. Int. 2014, 2014, 890697. [Google Scholar] [CrossRef] [PubMed]
- Wolters, T.; van der Kwast, T.H.; Vissers, C.J.; Bangma, C.H.; Roobol, M.; Schroder, F.H.; van Leenders, G.J.L.H. False-negative prostate needle biopsies: Frequency, histopathologic features, and follow-up. Am. J. Surg. Pathol. 2010, 34, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Thalgott, M.; Rack, B.; Horn, T.; Heck, M.M.; Eiber, M.; Kubler, H.; Retz, M.; Gschwend, J.E.; Andergassen, U.; Nawroth, R. Detection of circulating tumor cells in locally advanced high-risk prostate cancer during neoadjuvant chemotherapy and radical prostatectomy. Anticancer Res. 2015, 35, 5679–5685. [Google Scholar]
- Thalgott, M.; Rack, B.; Maurer, T.; Souvatzoglou, M.; Eiber, M.; Kress, V.; Heck, M.M.; Andergassen, U.; Nawroth, R.; Gschwend, J.E.; et al. Detection of circulating tumor cells in different stages of prostate cancer. J. Cancer Res. Clin. Oncol. 2013, 139, 755–763. [Google Scholar] [CrossRef] [PubMed]
- Alix-Panabieres, C.; Pantel, K. Clinical applications of circulating tumor cells and circulating tumor DNA as liquid biopsy. Cancer Discov. 2016, 6, 479–491. [Google Scholar] [CrossRef] [PubMed]
- Coumans, F.A.W.; Ligthart, S.T.; Uhr, J.W.; Terstappen, L.W.M.M. Challenges in the enumeration and phenotyping of CTC. Clin. Cancer Res. 2012, 18, 5711–5718. [Google Scholar] [CrossRef] [PubMed]
- Rack, B.; Schindlbeck, C.; Juckstock, J.; Andergassen, U.; Hepp, P.; Zwingers, T.; Friedl, T.W.P.; Lorenz, R.; Tesch, H.; Fasching, P.A.; et al. Circulating tumor cells predict survival in early average-to-high risk breast cancer patients. J. Natl. Cancer Inst. 2014, 106. [Google Scholar] [CrossRef] [PubMed]
- Janni, W.J.; Rack, B.; Terstappen, L.W.M.M.; Pierga, J.-Y.; Taran, F.-A.; Fehm, T.; Hall, C.; de Groot, M.R.; Bidard, F.-C.; Friedl, T.W.P.; et al. Pooled analysis of the prognostic relevance of circulating tumor cells in primary breast cancer. Clin. Cancer Res. 2016, 22, 2583–2593. [Google Scholar] [CrossRef] [PubMed]
- Riethdorf, S.; Muller, V.; Loibl, S.; Nekljudova, V.; Weber, K.; Huober, J.; Fehm, T.; Schrader, I.; Hilfrich, J.; Holms, F.; et al. Prognostic impact of circulating tumor cells for breast cancer patients treated in the neoadjuvant “Geparquattro” trial. Clin. Cancer Res. 2017, 23, 5384–5393. [Google Scholar] [CrossRef] [PubMed]
- Bidard, F.-C.; Michiels, S.; Riethdorf, S.; Mueller, V.; Esserman, L.J.; Lucci, A.; Naume, B.; Horiguchi, J.; Gisbert-Criado, R.; Sleijfer, S.; et al. Circulating tumor cells in breast cancer patients treated by neoadjuvant chemotherapy: A meta-analysis. J. Natl. Cancer Inst. 2018, 110, 560–567. [Google Scholar] [CrossRef] [PubMed]
- Hong, B.; Zu, Y. Detecting circulating tumor cells: Current challenges and new trends. Theranostics 2013, 3, 377–394. [Google Scholar] [CrossRef] [PubMed]
- Cristofanilli, M.; Hayes, D.F.; Budd, G.T.; Ellis, M.J.; Stopeck, A.; Reuben, J.M.; Doyle, G.V.; Matera, J.; Allard, W.J.; Miller, M.C.; et al. Circulating tumor cells: A novel prognostic factor for newly diagnosed metastatic breast cancer. J. Clin. Oncol. 2005, 23, 1420–1430. [Google Scholar] [CrossRef] [PubMed]
- Andreopoulou, E.; Yang, L.-Y.; Rangel, K.M.; Reuben, J.M.; Hsu, L.; Krishnamurthy, S.; Valero, V.; Fritsche, H.A.; Cristofanilli, M. Comparison of assay methods for detection of circulating tumor cells in metastatic breast cancer: AdnaGen AdnaTest BreastCancer select/detect versus Veridex CellSearch system. Int. J. Cancer 2012, 130, 1590–1597. [Google Scholar] [CrossRef] [PubMed]
- Pluim, D.; Devriese, L.A.; Beijnen, J.H.; Schellens, J.H.M. Validation of a multiparameter flow cytometry method for the determination of phosphorylated extracellular-signal-regulated kinase and DNA in circulating tumor cells. Cytometry A 2012, 81, 664–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagrath, S.; Sequist, L.V.; Maheswaran, S.; Bell, D.W.; Irimia, D.; Ulkus, L.; Smith, M.R.; Kwak, E.L.; Digumarthy, S.; Muzikansky, A.; et al. Isolation of rare circulating tumour cells in cancer patients by microchip technology. Nature 2007, 450, 1235–1239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stott, S.L.; Hsu, C.-H.; Tsukrov, D.I.; Yu, M.; Miyamoto, D.T.; Waltman, B.A.; Rothenberg, S.M.; Shah, A.M.; Smas, M.E.; Korir, G.K.; et al. Isolation of circulating tumor cells using a microvortex-generating herringbone-chip. Proc. Natl. Acad. Sci. USA 2010, 107, 18392–18397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khoo, B.L.; Warkiani, M.E.; Tan, D.S.-W.; Bhagat, A.A.S.; Irwin, D.; Lau, D.P.; Lim, A.S.T.; Lim, K.H.; Krisna, S.S.; Lim, W.-T.; et al. Clinical validation of an ultra high-throughput spiral microfluidics for the detection and enrichment of viable circulating tumor cells. PLoS ONE 2014, 9, e99409. [Google Scholar] [CrossRef] [PubMed]
- Autebert, J.; Coudert, B.; Champ, J.; Saias, L.; Guneri, E.T.; Lebofsky, R.; Bidard, F.-C.; Pierga, J.-Y.; Farace, F.; Descroix, S.; et al. High purity microfluidic sorting and analysis of circulating tumor cells: Towards routine mutation detection. Lab Chip 2015, 15, 2090–2101. [Google Scholar] [CrossRef] [PubMed]
- Winer-Jones, J.P.; Vahidi, B.; Arquilevich, N.; Fang, C.; Ferguson, S.; Harkins, D.; Hill, C.; Klem, E.; Pagano, P.C.; Peasley, C.; et al. Circulating tumor cells: Clinically relevant molecular access based on a novel CTC flow cell. PLoS ONE 2014, 9, e86717. [Google Scholar] [CrossRef] [PubMed]
- Harb, W.; Fan, A.; Tran, T.; Danila, D.C.; Keys, D.; Schwartz, M.; Ionescu-Zanetti, C. Mutational analysis of circulating tumor cells using a novel microfluidic collection device and qPCR Assay. Transl. Oncol. 2013, 6, 528–538. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Fusi, A.; Klopocki, E.; Schmittel, A.; Tinhofer, I.; Nonnenmacher, A.; Keilholz, U. Negative enrichment by immunomagnetic nanobeads for unbiased characterization of circulating tumor cells from peripheral blood of cancer patients. J. Transl. Med. 2011, 9, 70. [Google Scholar] [CrossRef]
- Lara, O.; Tong, X.; Zborowski, M.; Farag, S.S.; Chalmers, J.J. Comparison of two immunomagnetic separation technologies to deplete T cells from human blood samples. Biotechnol. Bioeng. 2006, 94, 66–80. [Google Scholar] [CrossRef]
- Scher, H.I.; Jia, X.; de Bono, J.S.; Fleisher, M.; Pienta, K.J.; Raghavan, D.; Heller, G. Circulating tumour cells as prognostic markers in progressive, castration-resistant prostate cancer: A reanalysis of IMMC38 trial data. Lancet Oncol. 2009, 10, 233–239. [Google Scholar] [CrossRef]
- Scheel, C.; Weinberg, R.A. Cancer stem cells and epithelial-mesenchymal transition: Concepts and molecular links. Semin. Cancer Biol. 2012, 22, 396–403. [Google Scholar] [CrossRef]
- Wang, L.; Balasubramanian, P.; Chen, A.P.; Kummar, S.; Evrard, Y.A.; Kinders, R.J. Promise and limits of the CellSearch platform for evaluating pharmacodynamics in circulating tumor cells. Semin. Oncol. 2016, 43, 464–475. [Google Scholar] [CrossRef] [Green Version]
- Andree, K.C.; van Dalum, G.; Terstappen, L.W.M.M. Challenges in circulating tumor cell detection by the CellSearch system. Mol. Oncol. 2016, 10, 395–407. [Google Scholar] [CrossRef]
- Sharma, S.; Zhuang, R.; Long, M.; Pavlovic, M.; Kang, Y.; Ilyas, A.; Asghar, W. Circulating tumor cell isolation, culture, and downstream molecular analysis. Biotechnol. Adv. 2018, 36, 1063–1078. [Google Scholar] [CrossRef] [PubMed]
- Alix-Panabieres, C.; Pantel, K. Liquid biopsy in cancer patients: Advances in capturing viable CTCs for functional studies using the EPISPOT assay. Expert Rev. Mol. Diagn. 2015, 15, 1411–1417. [Google Scholar] [CrossRef] [PubMed]
- Gorges, T.M.; Penkalla, N.; Schalk, T.; Joosse, S.A.; Riethdorf, S.; Tucholski, J.; Lucke, K.; Wikman, H.; Jackson, S.; Brychta, N.; et al. Enumeration and molecular characterization of tumor cells in lung cancer patients using a novel in vivo device for capturing circulating tumor cells. Clin. Cancer Res. 2016, 22, 2197–2206. [Google Scholar] [CrossRef] [PubMed]
- Kuske, A.; Gorges, T.M.; Tennstedt, P.; Tiebel, A.-K.; Pompe, R.; Preisser, F.; Prues, S.; Mazel, M.; Markou, A.; Lianidou, E.; et al. Improved detection of circulating tumor cells in non-metastatic high-risk prostate cancer patients. Sci. Rep. 2016, 6, 39736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kruck, S.; Gakis, G.; Stenzl, A. Disseminated and circulating tumor cells for monitoring chemotherapy in urological tumors. Anticancer Res. 2011, 31, 2053–2057. [Google Scholar]
- Alix-Panabieres, C. EPISPOT assay: Detection of viable DTCs/CTCs in solid tumor patients. Recent Results Cancer Res. 2012, 195, 69–76. [Google Scholar] [CrossRef]
- Markou, A.; Lazaridou, M.; Paraskevopoulos, P.; Chen, S.; Swierczewska, M.; Budna, J.; Kuske, A.; Gorges, T.M.; Joosse, S.A.; Kroneis, T.; et al. Multiplex gene expression profiling of in vivo isolated circulating tumor cells in high-risk prostate cancer patients. Clin. Chem. 2018, 64, 297–306. [Google Scholar] [CrossRef]
- Theil, G.; Fischer, K.; Weber, E.; Medek, R.; Hoda, R.; Lucke, K.; Fornara, P. The use of a new cellcollector to isolate circulating tumor cells from the blood of patients with different stages of prostate cancer and clinical outcomes—A proof-of-concept study. PLoS ONE 2016, 11, e0158354. [Google Scholar] [CrossRef]
- Alix-Panabieres, C.; Rebillard, X.; Brouillet, J.-P.; Barbotte, E.; Iborra, F.; Segui, B.; Maudelonde, T.; Jolivet-Reynaud, C.; Vendrell, J.-P. Detection of circulating prostate-specific antigen-secreting cells in prostate cancer patients. Clin. Chem. 2005, 51, 1538–1541. [Google Scholar] [CrossRef]
- Alix-Panabieres, C.; Vendrell, J.-P.; Pelle, O.; Rebillard, X.; Riethdorf, S.; Muller, V.; Fabbro, M.; Pantel, K. Detection and characterization of putative metastatic precursor cells in cancer patients. Clin. Chem. 2007, 53, 537–539. [Google Scholar] [CrossRef]
- Loh, J.; Jovanovic, L.; Lehman, M.; Capp, A.; Pryor, D.; Harris, M.; Nelson, C.; Martin, J. Circulating tumor cell detection in high-risk non-metastatic prostate cancer. J. Cancer Res. Clin. Oncol. 2014, 140, 2157–2162. [Google Scholar] [CrossRef] [PubMed]
- Lucci, A.; Hall, C.S.; Lodhi, A.K.; Bhattacharyya, A.; Anderson, A.E.; Xiao, L.; Bedrosian, I.; Kuerer, H.M.; Krishnamurthy, S. Circulating tumour cells in non-metastatic breast cancer: A prospective study. Lancet Oncol. 2012, 13, 688–695. [Google Scholar] [CrossRef]
- Gazzaniga, P.; Gianni, W.; Raimondi, C.; Gradilone, A.; Lo Russo, G.; Longo, F.; Gandini, O.; Tomao, S.; Frati, L. Circulating tumor cells in high-risk nonmetastatic colorectal cancer. Tumour Biol. 2013, 34, 2507–2509. [Google Scholar] [CrossRef] [PubMed]
- Reeh, M.; Effenberger, K.E.; Koenig, A.M.; Riethdorf, S.; Eichstadt, D.; Vettorazzi, E.; Uzunoglu, F.G.; Vashist, Y.K.; Izbicki, J.R.; Pantel, K.; et al. Circulating tumor cells as a biomarker for preoperative prognostic staging in patients with esophageal cancer. Ann. Surg. 2015, 261, 1124–1130. [Google Scholar] [CrossRef] [PubMed]
- Karl, A.; Tritschler, S.; Hofmann, S.; Stief, C.G.; Schindlbeck, C. Perioperative search for circulating tumor cells in patients undergoing radical cystectomy for bladder cancer. Eur. J. Med. Res. 2009, 14, 487–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez-Lorencio, M.I.; Ramirez, P.; Saenz, L.; Martinez Sanchez, M.V.; de La Orden, V.; Mediero-Valeros, B.; Veganzones-De-Castro, S.; Baroja-Mazo, A.; Revilla Nuin, B.; Gonzalez, M.R.; et al. Comparison of two types of liquid biopsies in patients with hepatocellular carcinoma awaiting orthotopic liver transplantation. Transplant. Proc. 2015, 47, 2639–2642. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, J.-M.; Fehm, T.; Orsini, M.; Cayrefourcq, L.; Maudelonde, T.; Pantel, K.; Alix-Panabieres, C. Prognostic relevance of viable circulating tumor cells detected by EPISPOT in metastatic breast cancer patients. Clin. Chem. 2014, 60, 214–221. [Google Scholar] [CrossRef]
- Pantel, K.; Alix-Panabieres, C.; Riethdorf, S. Cancer micrometastases. Nat. Rev. Clin. Oncol. 2009, 6, 339–351. [Google Scholar] [CrossRef]
- Alix-Panabieres, C.; Vendrell, J.-P.; Slijper, M.; Pelle, O.; Barbotte, E.; Mercier, G.; Jacot, W.; Fabbro, M.; Pantel, K. Full-length cytokeratin-19 is released by human tumor cells: a potential role in metastatic progression of breast cancer. Breast Cancer Res. 2009, 11, R39. [Google Scholar] [CrossRef]
- Deneve, E.; Riethdorf, S.; Ramos, J.; Nocca, D.; Coffy, A.; Daures, J.-P.; Maudelonde, T.; Fabre, J.-M.; Pantel, K.; Alix-Panabieres, C. Capture of viable circulating tumor cells in the liver of colorectal cancer patients. Clin. Chem. 2013, 59, 1384–1392. [Google Scholar] [CrossRef]
- Schwarzenbach, H.; Alix-Panabieres, C.; Muller, I.; Letang, N.; Vendrell, J.-P.; Rebillard, X.; Pantel, K. Cell-free tumor DNA in blood plasma as a marker for circulating tumor cells in prostate cancer. Clin. Cancer Res. 2009, 15, 1032–1038. [Google Scholar] [CrossRef] [PubMed]
- Saucedo-Zeni, N.; Mewes, S.; Niestroj, R.; Gasiorowski, L.; Murawa, D.; Nowaczyk, P.; Tomasi, T.; Weber, E.; Dworacki, G.; Morgenthaler, N.G.; et al. A novel method for the in vivo isolation of circulating tumor cells from peripheral blood of cancer patients using a functionalized and structured medical wire. Int. J. Oncol. 2012, 41, 1241–1250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strati, A.; Markou, A.; Parisi, C.; Politaki, E.; Mavroudis, D.; Georgoulias, V.; Lianidou, E. Gene expression profile of circulating tumor cells in breast cancer by RT-qPCR. BMC Cancer 2011, 11, 422. [Google Scholar] [CrossRef] [PubMed]
- Galena, H.J. Complications occurring from diagnostic venipuncture. J. Fam. Pract. 1992, 34, 582–584. [Google Scholar] [PubMed]
- Fischer, J.C.; Niederacher, D.; Topp, S.A.; Honisch, E.; Schumacher, S.; Schmitz, N.; Zacarias Fohrding, L.; Vay, C.; Hoffmann, I.; Kasprowicz, N.S.; et al. Diagnostic leukapheresis enables reliable detection of circulating tumor cells of nonmetastatic cancer patients. Proc. Natl. Acad. Sci. USA 2013, 110, 16580–16585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Toom, E.E.; Verdone, J.E.; Gorin, M.A.; Pienta, K.J. Technical challenges in the isolation and analysis of circulating tumor cells. Oncotarget 2016, 7, 62754–62766. [Google Scholar] [CrossRef] [Green Version]
- Barriere, G.; Fici, P.; Gallerani, G.; Fabbri, F.; Zoli, W.; Rigaud, M. Circulating tumor cells and epithelial, mesenchymal and stemness markers: Characterization of cell subpopulations. Ann. Transl. Med. 2014, 2, 109. [Google Scholar] [CrossRef]
- Mazel, M.; Jacot, W.; Pantel, K.; Bartkowiak, K.; Topart, D.; Cayrefourcq, L.; Rossille, D.; Maudelonde, T.; Fest, T.; Alix-Panabieres, C. Frequent expression of PD-L1 on circulating breast cancer cells. Mol. Oncol. 2015, 9, 1773–1782. [Google Scholar] [CrossRef] [Green Version]
- Strati, A.; Koutsodontis, G.; Papaxoinis, G.; Angelidis, I.; Zavridou, M.; Economopoulou, P.; Kotsantis, I.; Avgeris, M.; Mazel, M.; Perisanidis, C.; et al. Prognostic significance of PD-L1 expression on circulating tumor cells in patients with head and neck squamous cell carcinoma. Ann. Oncol. 2017, 28, 1923–1933. [Google Scholar] [CrossRef]
- Kulasinghe, A.; Kenny, L.; Punyadeera, C. Circulating tumour cell PD-L1 test for head and neck cancers. Oral Oncol. 2017, 75, 6–7. [Google Scholar] [CrossRef]
- Dhar, M.; Wong, J.; Che, J.; Matsumoto, M.; Grogan, T.; Elashoff, D.; Garon, E.B.; Goldman, J.W.; Sollier Christen, E.; Di Carlo, D.; et al. Evaluation of PD-L1 expression on vortex-isolated circulating tumor cells in metastatic lung cancer. Sci. Rep. 2018, 8, 2592. [Google Scholar] [CrossRef] [PubMed]
- Martin, O.A.; Anderson, R.L.; Russell, P.A.; Cox, R.A.; Ivashkevich, A.; Swierczak, A.; Doherty, J.P.; Jacobs, D.H.M.; Smith, J.; Siva, S.; et al. Mobilization of viable tumor cells into the circulation during radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Vilalta, M.; Rafat, M.; Giaccia, A.J.; Graves, E.E. Recruitment of circulating breast cancer cells is stimulated by radiotherapy. Cell Rep. 2014, 8, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.-Y.; Oskarsson, T.; Acharyya, S.; Nguyen, D.X.; Zhang, X.H.-F.; Norton, L.; Massague, J. Tumor self-seeding by circulating cancer cells. Cell 2009, 139, 1315–1326. [Google Scholar] [CrossRef] [PubMed]
- Lowes, L.E.; Lock, M.; Rodrigues, G.; D’Souza, D.; Bauman, G.; Ahmad, B.; Venkatesan, V.; Allan, A.L.; Sexton, T. Circulating tumour cells in prostate cancer patients receiving salvage radiotherapy. Clin. Transl. Oncol. 2012, 14, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Tombal, B.; van Cangh, P.J.; Loric, S.; Gala, J.-L. Prognostic value of circulating prostate cells in patients with a rising PSA after radical prostatectomy. Prostate 2003, 56, 163–170. [Google Scholar] [CrossRef]
- Yin, X.-D.; Yuan, X.; Xue, J.-J.; Wang, R.; Zhang, Z.-R.; Tong, J.-D. Clinical significance of carcinoembryonic antigen-, cytokeratin 19-, or survivin-positive circulating tumor cells in the peripheral blood of esophageal squamous cell carcinoma patients treated with radiotherapy. Dis. Esophagus 2012, 25, 750–756. [Google Scholar] [CrossRef]
- Dorsey, J.F.; Kao, G.D.; MacArthur, K.M.; Ju, M.; Steinmetz, D.; Wileyto, E.P.; Simone, C.B.; Hahn, S.M. Tracking viable circulating tumor cells (CTCs) in the peripheral blood of non-small cell lung cancer (NSCLC) patients undergoing definitive radiation therapy: Pilot study results. Cancer 2015, 121, 139–149. [Google Scholar] [CrossRef]
- Prcic, A.; Begic, E.; Hiros, M. Usefulness of total PSA value in prostate diseases diagnosis. Acta Inform. Med. 2016, 24, 156–161. [Google Scholar] [CrossRef]
- Turk, H.; Celik, O.; Un, S.; Yoldas, M.; Isoglu, C.S.; Karabicak, M.; Ergani, B.; Koc, G.; Zorlu, F.; Ilbey, Y.O. Predictive factors for biochemical recurrence in radical prostatectomy patients. Cent. Eur. J. Urol. 2015, 68, 404–409. [Google Scholar] [CrossRef] [Green Version]
- Grossfeld, G.D.; Latini, D.M.; Lubeck, D.P.; Mehta, S.S.; Carroll, P.R. Predicting recurrence after radical prostatectomy for patients with high risk prostate cancer. J. Urol. 2003, 169, 157–163. [Google Scholar] [CrossRef]
- Geara, F.B.; Bulbul, M.; Khauli, R.B.; Andraos, T.Y.; Abboud, M.; Al Mousa, A.; Sarhan, N.; Salem, A.; Ghatasheh, H.; Alnsour, A.; et al. Nadir PSA is a strong predictor of treatment outcome in intermediate and high risk localized prostate cancer patients treated by definitive external beam radiotherapy and androgen deprivation. Radiat. Oncol. 2017, 12, 149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, S.K.; Nam, J.S.; Na, W.; Oh, J.J.; Yoon, C.Y.; Jeong, C.W.; Kim, H.J.; Byun, S.-S.; Lee, S.E. Younger patients have poorer biochemical outcome after radical prostatectomy in high-risk prostate cancer. Asian J. Androl. 2011, 13, 719–723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davies, N.M.; Gaunt, T.R.; Lewis, S.J.; Holly, J.; Donovan, J.L.; Hamdy, F.C.; Kemp, J.P.; Eeles, R.; Easton, D.; Kote-Jarai, Z.; et al. The effects of height and BMI on prostate cancer incidence and mortality: A Mendelian randomization study in 20,848 cases and 20,214 controls from the PRACTICAL consortium. Cancer Causes Control 2015, 26, 1603–1616. [Google Scholar] [CrossRef] [PubMed]
- Haque, R.; Van Den Eeden, S.K.; Wallner, L.P.; Richert-Boe, K.; Kallakury, B.; Wang, R.; Weinmann, S. Association of body mass index and prostate cancer mortality. Obes. Res. Clin. Pract. 2014, 8, e374–e381. [Google Scholar] [CrossRef]
- Xie, B.; Zhang, G.; Wang, X.; Xu, X. Body mass index and incidence of nonaggressive and aggressive prostate cancer: A dose-response meta-analysis of cohort studies. Oncotarget 2017, 8, 97584–97592. [Google Scholar] [CrossRef] [PubMed]
- Presti, J.C., Jr. Obesity and prostate cancer. Curr. Opin. Urol. 2005, 15, 13–16. [Google Scholar] [CrossRef]
- Cunha, G.R.; Hayward, S.W.; Wang, Y.Z.; Ricke, W.A. Role of the stromal microenvironment in carcinogenesis of the prostate. Int. J. Cancer 2003, 107, 1–10. [Google Scholar] [CrossRef]
- Schiffmann, J.; Karakiewicz, P.I.; Rink, M.; Manka, L.; Salomon, G.; Tilki, D.; Budaus, L.; Pompe, R.; Leyh-Bannurah, S.-R.; Haese, A.; et al. Obesity paradox in prostate cancer: Increased body mass index was associated with decreased risk of metastases after surgery in 13,667 patients. World J. Urol. 2018, 36, 1067–1072. [Google Scholar] [CrossRef]
- Ortmann, U.; Janni, W.; Andergassen, U.; Beck, T.; Beckmann, M.W.; Lichtenegger, W.; Neugebauer, J.K.; Salmen, J.; Schindlbeck, C.; Schneeweiss, A.; et al. Correlation of high body mass index and circulating tumor cell positivity in patients with early-stage breast cancer. J. Clin. Oncol. 2012, 30, 1600. [Google Scholar]
- Fayanju, O.M.; Hall, C.S.; Bauldry, J.B.; Karhade, M.; Valad, L.M.; Kuerer, H.M.; DeSnyder, S.M.; Barcenas, C.H.; Lucci, A. Body mass index mediates the prognostic significance of circulating tumor cells in inflammatory breast cancer. Am. J. Surg. 2017, 214, 666–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bono, J.S.; de Scher, H.I.; Montgomery, R.B.; Parker, C.; Miller, M.C.; Tissing, H.; Doyle, G.V.; Terstappen, L.W.W.M.; Pienta, K.J.; Raghavan, D. Circulating tumor cells predict survival benefit from treatment in metastatic castration-resistant prostate cancer. Clin. Cancer Res. 2008, 14, 6302–6309. [Google Scholar] [CrossRef] [PubMed]
- Scher, H.I.; Heller, G.; Molina, A.; Attard, G.; Danila, D.C.; Jia, X.; Peng, W.; Sandhu, S.K.; Olmos, D.; Riisnaes, R.; et al. Circulating tumor cell biomarker panel as an individual-level surrogate for survival in metastatic castration-resistant prostate cancer. J. Clin. Oncol. 2015, 33, 1348–1355. [Google Scholar] [CrossRef] [PubMed]
- Pantel, K.; Alix-Panabieres, C. Functional studies on viable circulating tumor cells. Clin. Chem. 2016, 62, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Soler, A.; Cayrefourcq, L.; Mazel, M.; Alix-Panabieres, C. EpCAM-Independent enrichment and detection of viable circulating tumor cells using the EPISPOT assay. Methods Mol. Biol. 2017, 1634, 263–276. [Google Scholar] [CrossRef] [PubMed]
- Strilic, B.; Offermanns, S. Intravascular survival and extravasation of tumor cells. Cancer Cell 2017, 32, 282–293. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Overall | CellSearch® System | EPISPOT | CellCollector® | Combined | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CTC Negative | CTC Positive | p-Value | CTC Negative | CTC Positive | p-Value | CTC Negative | CTC Positive | p-Value | CTC Negative | CTC Positive | p-Value | ||
| Patients, n (%) | 131 | 94 (82) | 20 (18) | 67 (54) | 57 (46) | 60 (48) | 66 (52) | 16 (12) | 115 (88) | ||||
| Age, Median (IQR), Min–Max | 68.5, (64.25–72), 51–89 | 68 (64–72) 51–80 | 70.5 (66.75–72.75) 60–89 | 0.15 | 69 (66–72) 53–89 | 66 (63–72) 51–79 | 0.053 | 69 (64–72) 51–89 | 67 (64.25–72) 53–78 | 0.50 | 69, (67.5–72.25), 59–80 | 68, (64–72), 51–89 | 0.22 |
| BMI, Median (IQR), Min–Max | 27.61, (25.6–29.8), 20.45–46.17 | 27.4, (25.5–29.7), 20.8–46.17 | 28.01, (26.8–29.4), 23.2–41.9 | 0.37 | 27.13, (25.5–29.5), 20.8–41.91 | 27.7, (26.03–30.67), 20.45–37.18 | 0.33 | 27.46, (25.24–29.11), 20.45–37.18 | 27.68, (26.17–31.7), 21.51–46.17 | 0.19 | 25.59, (23.5–26.9), 20.8–29.4 | 27.68, (26.12–30.66), 20.45–46.17 | 0.0036 |
| PSA, Median (IQR), Min–Max | 27.85, (15–35–40.75), 0.5–191 | 28.2 (20–42) 3.89–191 | 25.6 (7–09–40.25) 0.5–172 | 0.26 | 26.795 (10.365–41.15) 0.5–172 | 28.2 (17.6–40) 5–191 | 0.23 | 25 (10.5–41.1) 2.5–191 | 28.5 (22.5–37) 0.5–136.9 | 0.23 | 24.83, (11.78–38.95), 3.9–66 | 28.05, (15.625–40.75), 0.5–191 | 0.49 |
| Biopsy Gleason score; n (%) | |||||||||||||
| 3+3 | 30 (23) | 22 (23.9) | 4 (20) | 0.77 | 13 (19.7) | 15 (26.8) | 0.069 | 13 (22) | 17 (25.8) | 0.14 | 3 (18.8) | 27 (23.9) | 0.35 |
| 3+4 | 40 (31) | 30 (32.6) | 4 (20) | 18 (27.3) | 20 (35.7) | 19 (32.2) | 21 (31.8) | 4 (25) | 36 (31.8) | ||||
| 4+3 | 24 (19) | 19 (20.7) | 2 (10) | 10 (15.2) | 12 (21.4) | 10 (16.9) | 12 (18.2) | 4 (25) | 20 (17.7) | ||||
| ≥4+4 | 35 (28) | 21 (22.8) | 10 (50) | 25 (37.8) | 9 (16.1) | 17 (28.9) | 16 (24.2) | 5 (31.2) | 30 (26.6) | ||||
| Clinical T stage; n (%) | |||||||||||||
| T1a | 1 (0.8) | 0 (0) | 0 (0) | 0.64 | 0 (0) | 1 (1.8) | 0.078 | 0 (0) | 1 (1.6) | 0.24 | 0 (0) | 1 (0.9) | 0.95 |
| T1c | 76 (60.3) | 56 (62.2) | 9 (47.4) | 36 (55.4) | 35 (63.6) | 31 (53.4) | 45 (70.3) | 10 (62.5) | 66 (60) | ||||
| T2a | 10 (7.9) | 6 (6.7) | 3 (15.8) | 4 (6.2) | 6 (10.9) | 7 (12.1) | 3 (4.7) | 1 (6.2) | 9 (8.2) | ||||
| T2b | 3 (2.4) | 3 (3.3) | 0 (0) | 2 (3.1) | 0 (0) | 1 (1.7) | 2 (3.1) | 0 (0) | 3 (2.7) | ||||
| T2c | 23 (18.3) | 16 (17.8) | 4 (21.1) | 13 (20) | 10 (18.2) | 12 (20.7) | 9 (14.1) | 3 (18.8) | 20 (18.2) | ||||
| T3a | 12 (9.5) | 8 (8.9) | 3 (15.8) | 10 (15.4) | 2 (3.6) | 6 (10.3) | 4 (6.2) | 2 (12.5) | 10 (9.1) | ||||
| T3b | 1 (0.8) | 1 (1.1) | 0 (0) | 0 (0) | 1 (1.8) | 1 (1.7) | 0 (0) | 0 (0) | 1 (0.9) | ||||
| Samples Tested | CellSearch® | EPISPOT | CellCollector® |
|---|---|---|---|
| No. of samples tested at baseline | 114 | 124 | 126 |
| No. of samples tested after radiotherapy | 63 | 68 | 64 |
| No. of samples tested at both time points | 53 | 62 | 64 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Budna-Tukan, J.; Świerczewska, M.; Mazel, M.; Cieślikowski, W.A.; Ida, A.; Jankowiak, A.; Antczak, A.; Nowicki, M.; Pantel, K.; Azria, D.; et al. Analysis of Circulating Tumor Cells in Patients with Non-Metastatic High-Risk Prostate Cancer before and after Radiotherapy Using Three Different Enumeration Assays. Cancers 2019, 11, 802. https://doi.org/10.3390/cancers11060802
Budna-Tukan J, Świerczewska M, Mazel M, Cieślikowski WA, Ida A, Jankowiak A, Antczak A, Nowicki M, Pantel K, Azria D, et al. Analysis of Circulating Tumor Cells in Patients with Non-Metastatic High-Risk Prostate Cancer before and after Radiotherapy Using Three Different Enumeration Assays. Cancers. 2019; 11(6):802. https://doi.org/10.3390/cancers11060802
Chicago/Turabian StyleBudna-Tukan, Joanna, Monika Świerczewska, Martine Mazel, Wojciech A. Cieślikowski, Agnieszka Ida, Agnieszka Jankowiak, Andrzej Antczak, Michał Nowicki, Klaus Pantel, David Azria, and et al. 2019. "Analysis of Circulating Tumor Cells in Patients with Non-Metastatic High-Risk Prostate Cancer before and after Radiotherapy Using Three Different Enumeration Assays" Cancers 11, no. 6: 802. https://doi.org/10.3390/cancers11060802
APA StyleBudna-Tukan, J., Świerczewska, M., Mazel, M., Cieślikowski, W. A., Ida, A., Jankowiak, A., Antczak, A., Nowicki, M., Pantel, K., Azria, D., Zabel, M., & Alix-Panabières, C. (2019). Analysis of Circulating Tumor Cells in Patients with Non-Metastatic High-Risk Prostate Cancer before and after Radiotherapy Using Three Different Enumeration Assays. Cancers, 11(6), 802. https://doi.org/10.3390/cancers11060802