Postoperative Management in Patients with Pheochromocytoma and Paraganglioma

 ,
, 

Abstract
:1. Introduction
2. Catecholamines and Adrenoceptors
3. Cardiovascular Complications Related to PPGLs
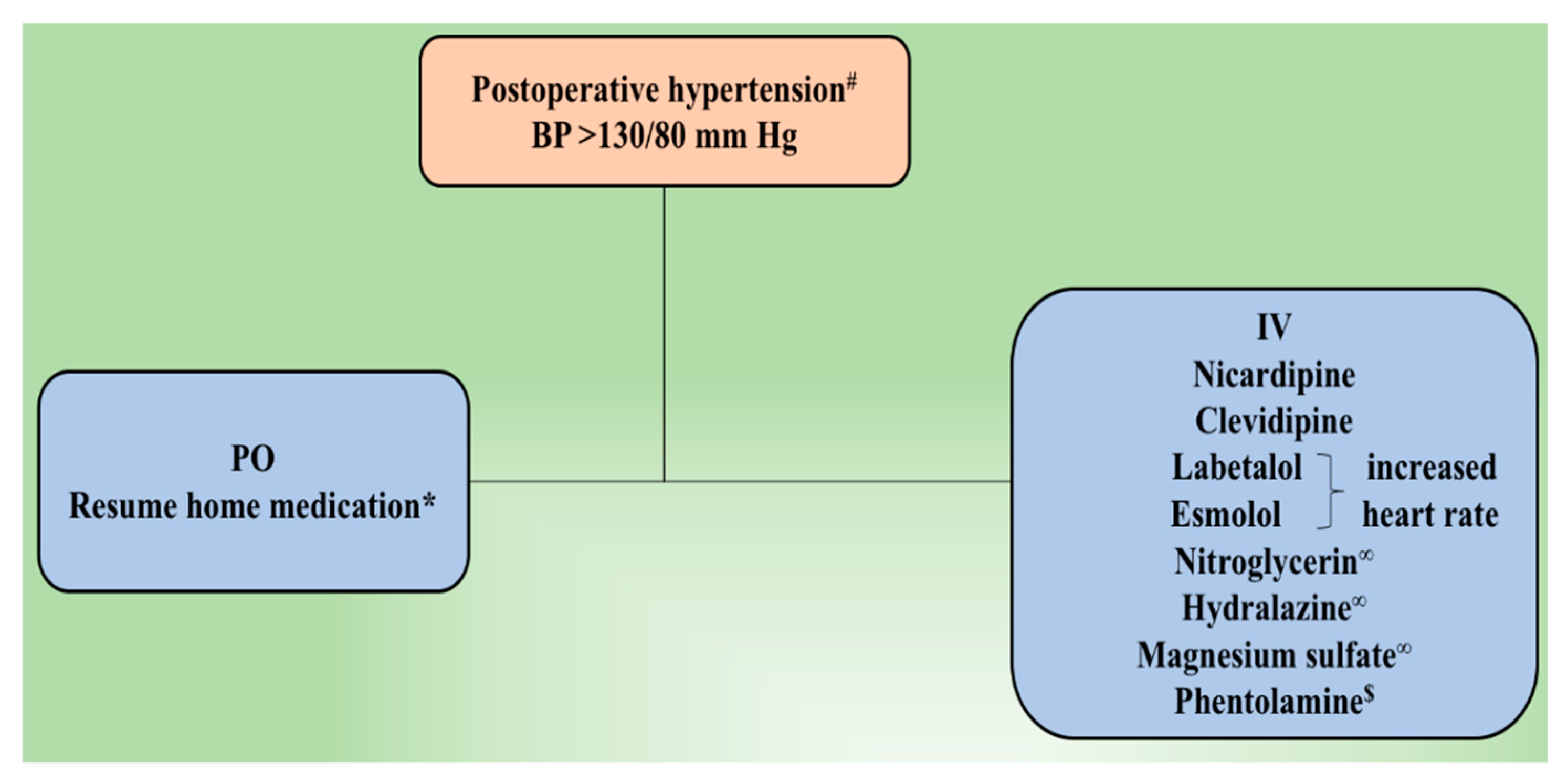
3.1. Hypertension
3.1.1. α- and β-Adrenoceptor Antagonist
3.1.2. Calcium Channel Blockers
3.1.3. Nitroglycerin
3.1.4. Hydralazine
3.1.5. Magnesium Sulfate
3.1.6. Treatment of Underlying Hypertension
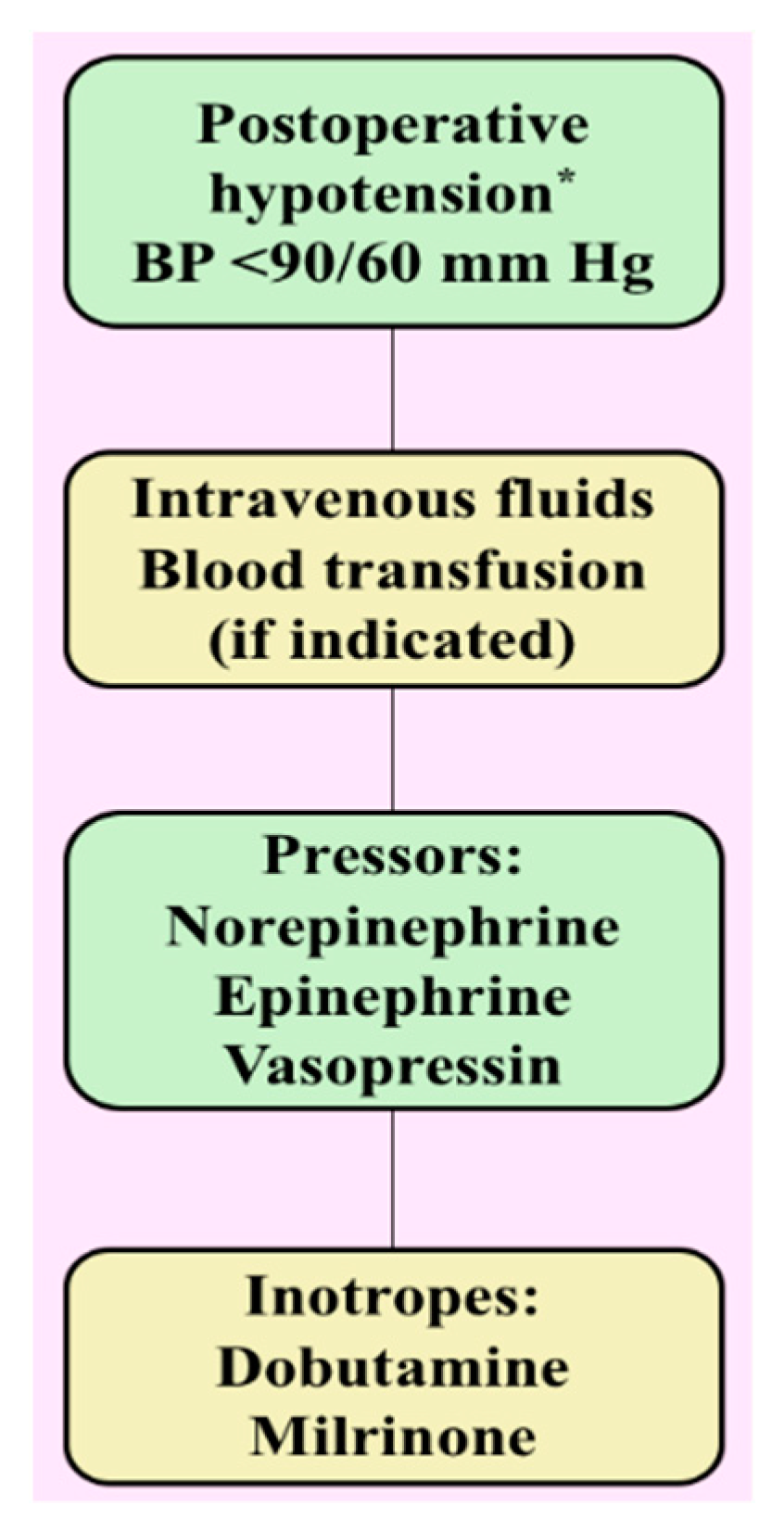
3.2. Hypotension
3.2.1. Intravenous Fluid
3.2.2. Norepinephrine
3.2.3. Epinephrine
3.2.4. Vasopressin
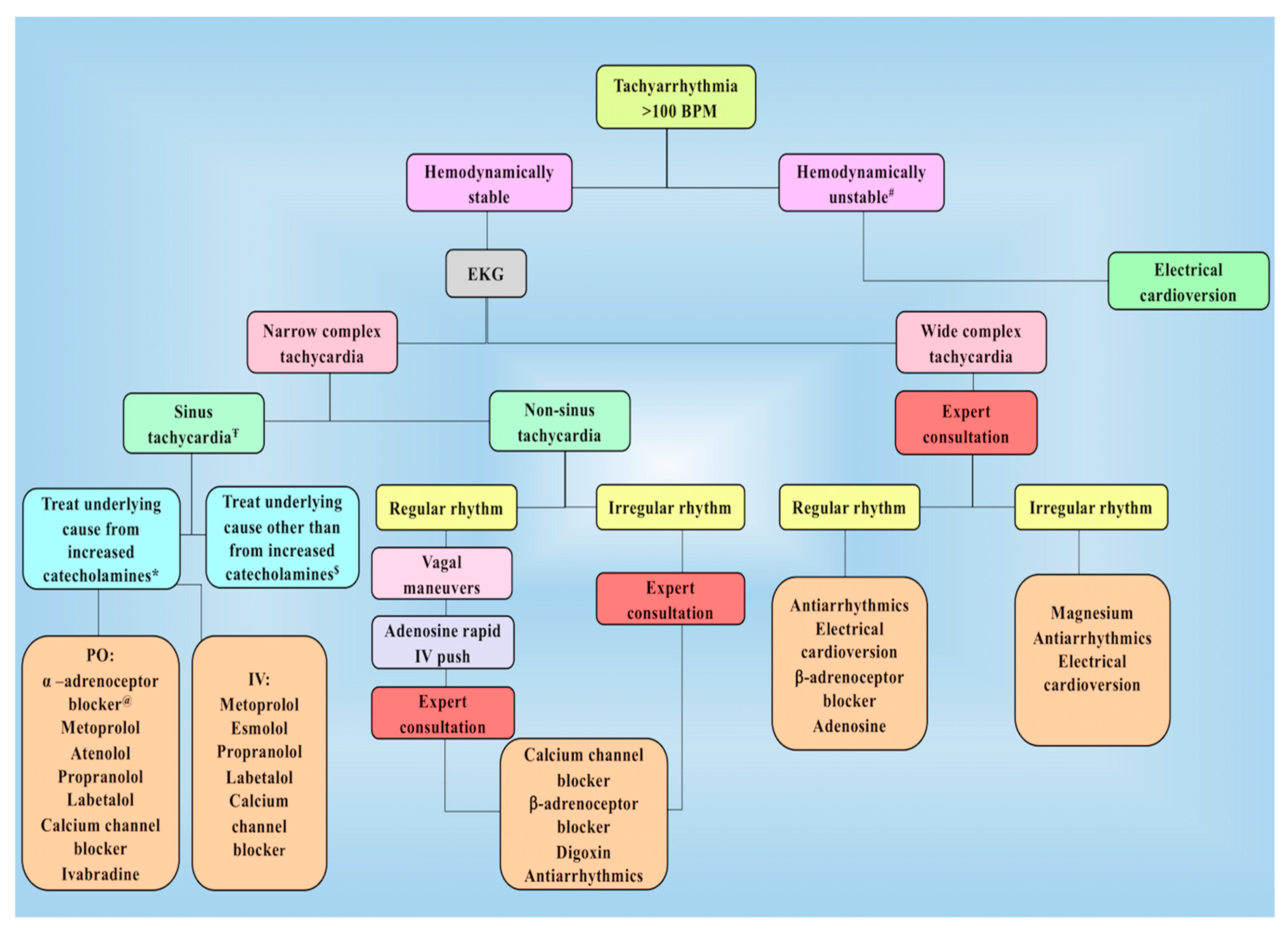
3.3. Arrhythmia
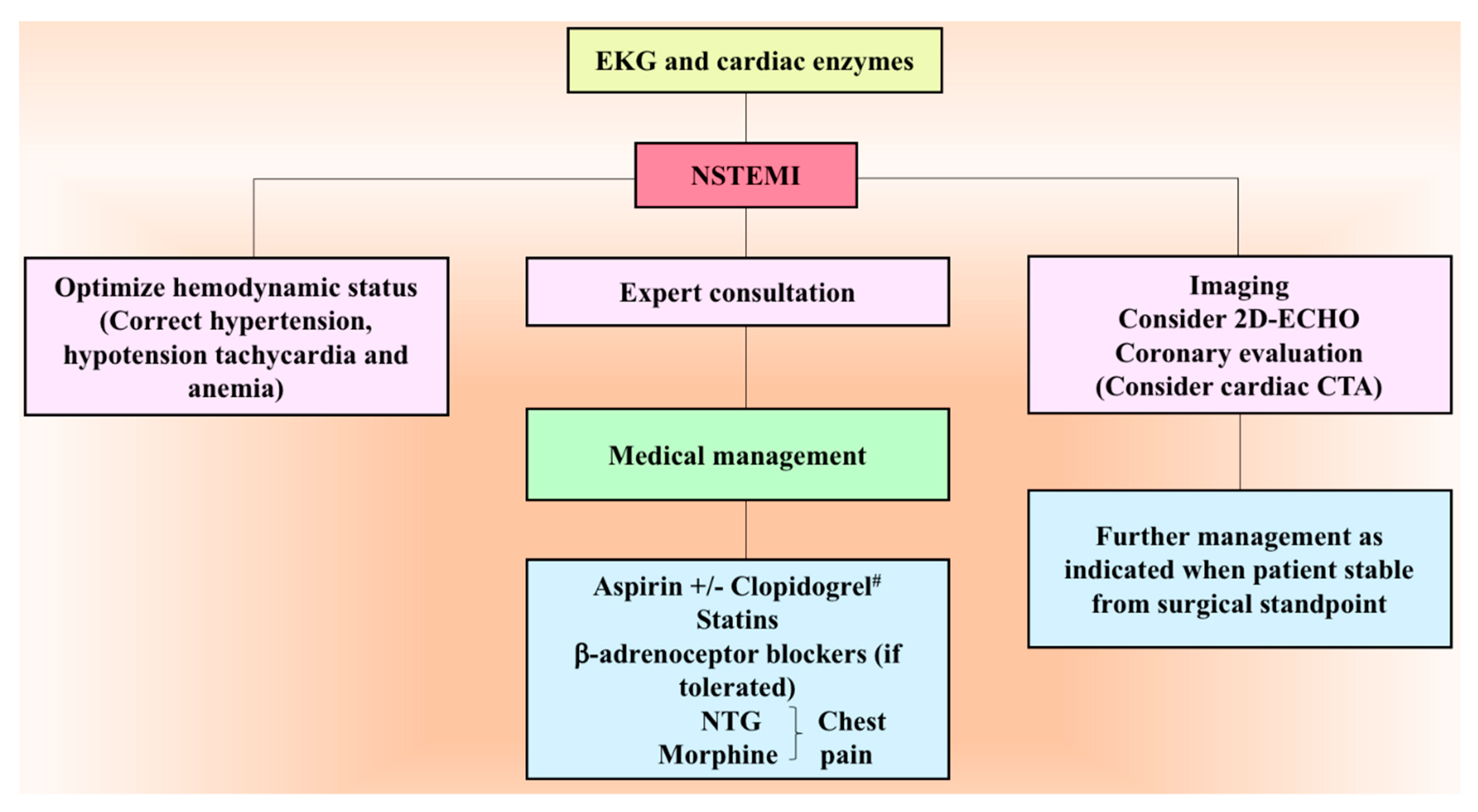
3.4. Myocardial Infarction
3.5. Heart Failure
3.6. Cerebrovascular Accident
4. Other Complications
4.1. Adrenocortical Insufficiency
4.2. Renal Failure
4.3. Hypoglycemia
4.4. Intestinal Pseudo-Obstruction
5. Other Common Surgical Complications
6. Conclusions
Funding
Conflicts of Interest
References
- Martucci, V.L.; Pacak, K. Pheochromocytoma and paraganglioma: Diagnosis, genetics, management, and treatment. Curr. Probl. Cancer 2014, 38, 7–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pacak, K. Preoperative management of the pheochromocytoma patient. J. Clin. Endocrinol. Metab. 2007, 92, 4069–4079. [Google Scholar] [CrossRef] [PubMed]
- Eisenhofer, G.; Peitzsch, M. Laboratory evaluation of pheochromocytoma and paraganglioma. Clin. Chem. 2014, 60, 1486–1499. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishna, H. Pheochromocytoma resection: Current concepts in anesthetic management. J. Anaesthesiol. Clin. Pharmacol. 2015, 31, 317–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pisarska, M.; Pedziwiatr, M.; Budzynski, A. Perioperative hemodynamic instability in patients undergoing laparoscopic adrenalectomy for pheochromocytoma. Gland. Surg. 2016, 5, 506–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiernan, C.M.; Du, L.; Chen, X.; Broome, J.T.; Shi, C.; Peters, M.F.; Solorzano, C.C. Predictors of hemodynamic instability during surgery for pheochromocytoma. Ann. Surg. Oncol. 2014, 21, 3865–3871. [Google Scholar] [CrossRef] [PubMed]
- Domi, R.; Laho, H. Management of pheochromocytoma: Old ideas and new drugs. Niger. J. Clin. Pract. 2012, 15, 253–257. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, R.; Rewari, V. Current perioperative management of pheochromocytomas. Indian. J. Urol. 2017, 33, 19–25. [Google Scholar] [CrossRef]
- Chen, Y.; Hodin, R.A.; Pandolfi, C.; Ruan, D.T.; McKenzie, T.J. Hypoglycemia after resection of pheochromocytoma. Surgery 2014, 156, 1404–1408. [Google Scholar] [CrossRef]
- Cruz, S.R.; Colwell, J.A. Pheochromocytoma and ileus. JAMA 1972, 219, 1050–1051. [Google Scholar] [CrossRef]
- Fee, H.J.; Fonkalsrud, E.W.; Ament, M.E.; Bergstein, J. Enterocolitis with peritonitis in a child with pheochromocytoma. Ann. Surg. 1977, 185, 448–450. [Google Scholar] [CrossRef] [PubMed]
- Gagner, M.; Lacroix, A.; Bolte, E. Laparoscopic adrenalectomy in Cushing’s syndrome and pheochromocytoma. N. Engl. J. Med. 1992, 327, 1033. [Google Scholar] [CrossRef] [PubMed]
- Brunton, L.L.; Hilal-Dandan, R.; Knollmann, B.C. Goodman & Gilman’s: The Pharmacological Basis of Therapeutics, 13th ed.; Mcgraw-Hill: New York, NY, USA, 2018. [Google Scholar]
- Ito, Y.; Fujimoto, Y.; Obara, T. The role of epinephrine, norepinephrine, and dopamine in blood pressure disturbances in patients with pheochromocytoma. World J. Surg. 1992, 16, 759–763. [Google Scholar] [CrossRef] [PubMed]
- Eisenhofer, G.; Kopin, I.J.; Goldstein, D.S. Catecholamine metabolism: A contemporary view with implications for physiology and medicine. Pharmacol. Rev. 2004, 56, 331–349. [Google Scholar] [CrossRef] [PubMed]
- Tsujimoto, G.; Manger, W.M.; Hoffman, B.B. Desensitization of beta-adrenergic receptors by pheochromocytoma. Endocrinology 1984, 114, 1272–1278. [Google Scholar] [CrossRef] [PubMed]
- Tsujimoto, G.; Honda, K.; Hoffman, B.B.; Hashimoto, K. Desensitization of postjunctional alpha 1- and alpha 2-adrenergic receptor-mediated vasopressor responses in rat harboring pheochromocytoma. Circ. Res. 1987, 61, 86–98. [Google Scholar] [CrossRef] [PubMed]
- Eisenhofer, G.; Walther, M.M.; Huynh, T.T.; Li, S.T.; Bornstein, S.R.; Vortmeyer, A.; Mannelli, M.; Goldstein, D.S.; Linehan, W.M.; Lenders, J.W.; et al. Pheochromocytomas in von Hippel-Lindau syndrome and multiple endocrine neoplasia type 2 display distinct biochemical and clinical phenotypes. J. Clin. Endocrinol. Metab. 2001, 86, 1999–2008. [Google Scholar] [CrossRef] [PubMed]
- Bravo, E.L.; Tarazi, R.C.; Fouad, F.M.; Textor, S.C.; Gifford, R.W., Jr.; Vidt, D.G. Blood pressure regulation in pheochromocytoma. Hypertension 1982, 4, 193–199. [Google Scholar] [PubMed]
- Ueda, T.; Oka, N.; Matsumoto, A.; Miyazaki, H.; Ohmura, H.; Kikuchi, T.; Nakayama, M.; Kato, S.; Imaizumi, T. Pheochromocytoma presenting as recurrent hypotension and syncope. Intern. Med. 2005, 44, 222–227. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E., Jr.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 71, 1269–1324. [Google Scholar] [CrossRef] [PubMed]
- Livingstone, M.; Duttchen, K.; Thompson, J.; Sunderani, Z.; Hawboldt, G.; Sarah Rose, M.; Pasieka, J. Hemodynamic Stability During Pheochromocytoma Resection: Lessons Learned Over the Last Two Decades. Ann. Surg. Oncol. 2015, 22, 4175–4180. [Google Scholar] [CrossRef] [PubMed]
- Weingarten, T.N.; Cata, J.P.; O’Hara, J.F.; Prybilla, D.J.; Pike, T.L.; Thompson, G.B.; Grant, C.S.; Warner, D.O.; Bravo, E.; Sprung, J. Comparison of two preoperative medical management strategies for laparoscopic resection of pheochromocytoma. Urology 2010, 76, 508.e6–508.e11. [Google Scholar] [CrossRef] [PubMed]
- Lord, M.S.; Augoustides, J.G. Perioperative management of pheochromocytoma: Focus on magnesium, clevidipine, and vasopressin. J. Cardiothorac. Vasc. Anesth. 2012, 26, 526–531. [Google Scholar] [CrossRef] [PubMed]
- Kinney, M.A.; Warner, M.E.; vanHeerden, J.A.; Horlocker, T.T.; Young, W.F., Jr.; Schroeder, D.R.; Maxson, P.M.; Warner, M.A. Perianesthetic risks and outcomes of pheochromocytoma and paraganglioma resection. Anesth. Analg. 2000, 91, 1118–1123. [Google Scholar] [PubMed]
- Bruynzeel, H.; Feelders, R.A.; Groenland, T.H.; van den Meiracker, A.H.; van Eijck, C.H.; Lange, J.F.; de Herder, W.W.; Kazemier, G. Risk Factors for Hemodynamic Instability during Surgery for Pheochromocytoma. J. Clin. Endocrinol. Metab. 2010, 95, 678–685. [Google Scholar] [CrossRef] [Green Version]
- Aksakal, N.; Agcaoglu, O.; Sahbaz, N.A.; Albuz, O.; Saracoglu, A.; Yavru, A.; Barbaros, U.; Erbil, Y. Predictive Factors of Operative Hemodynamic Instability for Pheochromocytoma. Am. Surg. 2018, 84, 920–923. [Google Scholar] [PubMed]
- Zelinka, T.; Eisenhofer, G.; Pacak, K. Pheochromocytoma as a catecholamine producing tumor: Implications for clinical practice. Stress 2007, 10, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Aronow, W.S. Treatment of hypertensive emergencies. Ann. Transl. Med. 2017, 5, S5. [Google Scholar] [CrossRef]
- Rhoney, D.; Peacock, W.F. Intravenous therapy for hypertensive emergencies, part 1. Am. J. Health Syst. Pharm. 2009, 66, 1343–1352. [Google Scholar] [CrossRef] [Green Version]
- Gray, R.J. Managing critically ill patients with esmolol. An ultra short-acting beta-adrenergic blocker. Chest 1988, 93, 398–403. [Google Scholar] [CrossRef]
- Varon, J.; Marik, P.E. Clinical review: The management of hypertensive crises. Crit. Care 2003, 7, 374–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sibal, L.; Jovanovic, A.; Agarwal, S.C.; Peaston, R.T.; James, R.A.; Lennard, T.W.; Bliss, R.; Batchelor, A.; Perros, P. Phaeochromocytomas presenting as acute crises after beta blockade therapy. Clin. Endocrinol. 2006, 65, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Bravo, E.L. Pheochromocytoma: An approach to antihypertensive management. Ann. N. Y. Acad. Sci. 2002, 970, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lund-Johansen, P. Pharmacology of combined alpha-beta-blockade. II. Haemodynamic effects of labetalol. Drugs 1984, 28, 35–50. [Google Scholar] [CrossRef] [PubMed]
- Kanto, J.; Allonen, H.; Kleimola, T.; Mantyla, R. Pharmacokinetics of labetalol in healthy volunteers. Int. J. Clin. Pharmacol. Ther. Toxicol. 1981, 19, 41–44. [Google Scholar] [PubMed]
- Poopalalingam, R.; Chin, E.Y. Rapid preparation of a patient with pheochromocytoma with labetolol and magnesium sulfate. Can. J. Anaesth. 2001, 48, 876–880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cressman, M.D.; Vidt, D.G.; Gifford, R.W., Jr.; Moore, W.S.; Wilson, D.J. Intravenous labetalol in the management of severe hypertension and hypertensive emergencies. Am. Heart J. 1984, 107, 980–985. [Google Scholar] [CrossRef]
- Hecht, J.P.; Mahmood, S.M.; Brandt, M.M. Safety of high-dose intravenous labetalol in hypertensive crisis. Am. J. Health Syst. Pharm. 2019, 76, 286–292. [Google Scholar] [CrossRef]
- Bravo, E.L. Pheochromocytoma. Cardiol. Rev. 2002, 10, 44–50. [Google Scholar] [CrossRef]
- Lehmann, H.U.; Hochrein, H.; Witt, E.; Mies, H.W. Hemodynamic effects of calcium antagonists. Review. Hypertension 1983, 5, II66–II73. [Google Scholar] [CrossRef]
- Nordlander, M.; Sjoquist, P.O.; Ericsson, H.; Ryden, L. Pharmacodynamic, pharmacokinetic and clinical effects of clevidipine, an ultrashort-acting calcium antagonist for rapid blood pressure control. Cardiovasc. Drug. Rev. 2004, 22, 227–250. [Google Scholar] [CrossRef]
- Awad, A.S.; Goldberg, M.E. Role of clevidipine butyrate in the treatment of acute hypertension in the critical care setting: A review. Vasc. Health Risk Manag. 2010, 6, 457–464. [Google Scholar]
- Kieler-Jensen, N.; Jolin-Mellgard, A.; Nordlander, M.; Ricksten, S.E. Coronary and systemic hemodynamic effects of clevidipine, an ultra-short-acting calcium antagonist, for treatment of hypertension after coronary artery surgery. Acta. Anaesthesiol. Scand. 2000, 44, 186–193. [Google Scholar] [CrossRef]
- Powroznyk, A.V.; Vuylsteke, A.; Naughton, C.; Misso, S.L.; Holloway, J.; Jolin-Mellgard, A.; Latimer, R.D.; Nordlander, M.; Feneck, R.O. Comparison of clevidipine with sodium nitroprusside in the control of blood pressure after coronary artery surgery. Eur. J. Anaesthesiol. 2003, 20, 697–703. [Google Scholar] [CrossRef]
- Bussmann, W.D.; Kenedi, P.; von Mengden, H.J.; Nast, H.P.; Rachor, N. Comparison of nitroglycerin with nifedipine in patients with hypertensive crisis or severe hypertension. Clin. Investig. 1992, 70, 1085–1088. [Google Scholar] [CrossRef] [PubMed]
- Varon, J.; Marik, P.E. Perioperative hypertension management. Vasc. Health Risk Manag. 2008, 4, 615–627. [Google Scholar] [CrossRef]
- Bryskin, R.; Weldon, B.C. Dexmedetomidine and magnesium sulfate in the perioperative management of a child undergoing laparoscopic resection of bilateral pheochromocytomas. J. Clin. Anesth. 2010, 22, 126–129. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, B.H.; Telander, R.L.; van Heerden, J.A.; Zimmerman, D.; Sheps, S.G.; Dawson, B. Pheochromocytoma in the pediatric age group: Current status. J. Pediatr. Surg. 1983, 18, 879–884. [Google Scholar] [CrossRef]
- Minami, T.; Adachi, T.; Fukuda, K. An effective use of magnesium sulfate for intraoperative management of laparoscopic adrenalectomy for pheochromocytoma in a pediatric patient. Anesth. Analg. 2002, 95, 1243–1244, table of contents. [Google Scholar] [CrossRef]
- Iseri, L.T.; French, J.H. Magnesium: nature’s physiologic calcium blocker. Am. Heart J. 1984, 108, 188–193. [Google Scholar] [CrossRef]
- Shimosawa, T.; Takano, K.; Ando, K.; Fujita, T. Magnesium inhibits norepinephrine release by blocking N-type calcium channels at peripheral sympathetic nerve endings. Hypertension 2004, 44, 897–902. [Google Scholar] [CrossRef] [PubMed]
- Bierlaire, D.; Pea, D.; Monnier, F.; Delbreil, J.P.; Bessout, L. Phaeochromocytoma and pregnancy: Anaesthetic management about two cases. Ann. Fr. Anesth. Reanim. 2009, 28, 988–993. [Google Scholar] [CrossRef] [PubMed]
- Golshevsky, J.R.; Karel, K.; Teale, G. Phaeochromocytoma causing acute pulmonary oedema during emergency caesarean section. Anaesth. Intensive Care 2007, 35, 423–427. [Google Scholar] [CrossRef] [PubMed]
- Kasaoka, S.; Tsuruta, R.; Nakashima, K.; Soejima, Y.; Miura, T.; Sadamitsu, D.; Tateishi, A.; Maekawa, T. Effect of intravenous magnesium sulfate on cardiac arrhythmias in critically ill patients with low serum ionized magnesium. Jpn. Circ. J. 1996, 60, 871–875. [Google Scholar] [CrossRef] [PubMed]
- Namekawa, T.; Utsumi, T.; Kawamura, K.; Kamiya, N.; Imamoto, T.; Takiguchi, T.; Hashimoto, N.; Tanaka, T.; Naya, Y.; Suzuki, H.; et al. Clinical predictors of prolonged postresection hypotension after laparoscopic adrenalectomy for pheochromocytoma. Surgery 2016, 159, 763–770. [Google Scholar] [CrossRef] [PubMed]
- Kercher, K.W.; Novitsky, Y.W.; Park, A.; Matthews, B.D.; Litwin, D.E.; Heniford, B.T. Laparoscopic curative resection of pheochromocytomas. Ann. Surg. 2005, 241, 919–926. [Google Scholar] [CrossRef] [PubMed]
- Chang, R.Y.; Lang, B.H.; Wong, K.P.; Lo, C.Y. High pre-operative urinary norepinephrine is an independent determinant of peri-operative hemodynamic instability in unilateral pheochromocytoma/paraganglioma removal. World J. Surg. 2014, 38, 2317–2323. [Google Scholar] [CrossRef] [PubMed]
- Cryer, P.E. Physiology and pathophysiology of the human sympathoadrenal neuroendocrine system. N. Engl. J. Med. 1980, 303, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Olson, S.W.; Deal, L.E.; Piesman, M. Epinephrine-secreting pheochromocytoma presenting with cardiogenic shock and profound hypocalcemia. Ann. Intern. Med. 2004, 140, 849–851. [Google Scholar] [CrossRef]
- Bartels, E.C.; Cattell, R.B. Pheochromocytoma; its diagnosis and treatment. Ann. Surg. 1950, 131, 903–916. [Google Scholar] [CrossRef]
- Frang, H.; Cockcroft, V.; Karskela, T.; Scheinin, M.; Marjamaki, A. Phenoxybenzamine binding reveals the helical orientation of the third transmembrane domain of adrenergic receptors. J. Biol. Chem. 2001, 276, 31279–31284. [Google Scholar] [CrossRef] [PubMed]
- Mannelli, M. Management and treatment of pheochromocytomas and paragangliomas. Ann. N. Y. Acad. Sci. 2006, 1073, 405–416. [Google Scholar] [CrossRef] [PubMed]
- Kayilioglu, S.I.; Dinc, T.; Sozen, I.; Bostanoglu, A.; Cete, M.; Coskun, F. Postoperative fluid management. World J. Crit. Care Med. 2015, 4, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Bangash, M.N.; Kong, M.L.; Pearse, R.M. Use of inotropes and vasopressor agents in critically ill patients. Br. J. Pharmacol. 2012, 165, 2015–2033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herget-Rosenthal, S.; Saner, F.; Chawla, L.S. Approach to hemodynamic shock and vasopressors. Clin. J. Am. Soc. Nephrol. 2008, 3, 546–553. [Google Scholar] [CrossRef] [PubMed]
- Maas, J.J.; Pinsky, M.R.; de Wilde, R.B.; de Jonge, E.; Jansen, J.R. Cardiac output response to norepinephrine in postoperative cardiac surgery patients: Interpretation with venous return and cardiac function curves. Crit. Care Med. 2013, 41, 143–150. [Google Scholar] [CrossRef] [PubMed]
- ECC Committee, Subcommittees and Task Forces of the American Heart Association. 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2005, 112, IV1–IV203. [Google Scholar] [CrossRef]
- Sato, Y.; Matsuzawa, H.; Eguchi, S. Comparative study of effects of adrenaline, dobutamine and dopamine on systemic hemodynamics and renal blood flow in patients following open heart surgery. Jpn. Circ. J. 1982, 46, 1059–1072. [Google Scholar] [CrossRef] [PubMed]
- De Backer, D.; Creteur, J.; Silva, E.; Vincent, J.L. Effects of dopamine, norepinephrine, and epinephrine on the splanchnic circulation in septic shock: Which is best? Crit. Care Med. 2003, 31, 1659–1667. [Google Scholar] [CrossRef]
- Dellinger, R.P.; Levy, M.M.; Rhodes, A.; Annane, D.; Gerlach, H.; Opal, S.M.; Sevransky, J.E.; Sprung, C.L.; Douglas, I.S.; Jaeschke, R.; et al. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med. 2013, 39, 165–228. [Google Scholar] [CrossRef]
- Myburgh, J.A.; Higgins, A.; Jovanovska, A.; Lipman, J.; Ramakrishnan, N.; Santamaria, J.; CAT Study Investigators. A comparison of epinephrine and norepinephrine in critically ill patients. Intensive Care Med. 2008, 34, 2226–2234. [Google Scholar] [CrossRef] [PubMed]
- Overgaard, C.B.; Dzavik, V. Inotropes and vasopressors: Review of physiology and clinical use in cardiovascular disease. Circulation 2008, 118, 1047–1056. [Google Scholar] [CrossRef] [PubMed]
- Augoustides, J.G.; Abrams, M.; Berkowitz, D.; Fraker, D. Vasopressin for hemodynamic rescue in catecholamine-resistant vasoplegic shock after resection of massive pheochromocytoma. Anesthesiology 2004, 101, 1022–1024. [Google Scholar] [CrossRef] [PubMed]
- Hollenberg, S.M.; Dellinger, R.P. Noncardiac surgery: Postoperative arrhythmias. Crit. Care Med. 2000, 28, N145–N150. [Google Scholar] [CrossRef] [PubMed]
- Fenster, P.E.; Quan, S.F.; Hanson, C.D.; Coaker, L.A. Suppression of ventricular ectopy with intravenous metoprolol in patients with chronic obstructive pulmonary disease. Crit. Care Med. 1984, 12, 29–32. [Google Scholar] [CrossRef] [PubMed]
- Hilleman, D.E.; Spinler, S.A. Conversion of recent-onset atrial fibrillation with intravenous amiodarone: A meta-analysis of randomized controlled trials. Pharmacotherapy 2002, 22, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Neumar, R.W.; Otto, C.W.; Link, M.S.; Kronick, S.L.; Shuster, M.; Callaway, C.W.; Kudenchuk, P.J.; Ornato, J.P.; McNally, B.; Silvers, S.M.; et al. Part 8: Adult advanced cardiovascular life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2010, 122, S729–S767. [Google Scholar] [CrossRef] [PubMed]
- Savelieva, I.; Camm, A.J. If inhibition with ivabradine: Electrophysiological effects and safety. Drug Saf. 2008, 31, 95–107. [Google Scholar] [CrossRef]
- Swedberg, K.; Komajda, M.; Bohm, M.; Borer, J.S.; Ford, I.; Dubost-Brama, A.; Lerebours, G.; Tavazzi, L.; Investigators, S. Ivabradine and outcomes in chronic heart failure (SHIFT): A randomised placebo-controlled study. Lancet 2010, 376, 875–885. [Google Scholar] [CrossRef]
- Fox, K.; Ford, I.; Steg, P.G.; Tendera, M.; Ferrari, R.; Investigators, B. Ivabradine for patients with stable coronary artery disease and left-ventricular systolic dysfunction (BEAUTIFUL): A randomised, double-blind, placebo-controlled trial. Lancet 2008, 372, 807–816. [Google Scholar] [CrossRef]
- Costa, G.A.; Tannuri, U.; Delgado, A.F. Bradycardia in the early postoperative period of liver transplantation in children. Transplant. Proc. 2010, 42, 1774–1776. [Google Scholar] [CrossRef] [PubMed]
- Habuchi, Y.; Tanaka, H.; Nishio, M.; Yamamoto, T.; Komori, T.; Morikawa, J.; Yoshimura, M. Dopamine stimulation of cardiac beta-adrenoceptors: The involvement of sympathetic amine transporters and the effect of SKF38393. Br. J. Pharmacol. 1997, 122, 1669–1678. [Google Scholar] [CrossRef] [PubMed]
- Brown, H.; Goldberg, P.A.; Selter, J.G.; Cabin, H.S.; Marieb, N.J.; Udelsman, R.; Setaro, J.F. Hemorrhagic pheochromocytoma associated with systemic corticosteroid therapy and presenting as myocardial infarction with severe hypertension. J. Clin. Endocrinol. Metab. 2005, 90, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Galetta, F.; Franzoni, F.; Bernini, G.; Poupak, F.; Carpi, A.; Cini, G.; Tocchini, L.; Antonelli, A.; Santoro, G. Cardiovascular complications in patients with pheochromocytoma: A mini-review. Biomed. Pharmacother. 2010, 64, 505–509. [Google Scholar] [CrossRef] [PubMed]
- Cheng, T.O. Pheochromocytoma as an MI mimic. Hosp. Pract. (Off. Ed.) 1990, 25, 16. [Google Scholar]
- Devereaux, P.J.; Goldman, L.; Yusuf, S.; Gilbert, K.; Leslie, K.; Guyatt, G.H. Surveillance and prevention of major perioperative ischemic cardiac events in patients undergoing noncardiac surgery: A review. CMAJ 2005, 173, 779–788. [Google Scholar] [CrossRef]
- Adams, J.E., 3rd; Sicard, G.A.; Allen, B.T.; Bridwell, K.H.; Lenke, L.G.; Davila-Roman, V.G.; Bodor, G.S.; Ladenson, J.H.; Jaffe, A.S. Diagnosis of perioperative myocardial infarction with measurement of cardiac troponin I. N. Engl. J. Med. 1994, 330, 670–674. [Google Scholar] [CrossRef]
- Landesberg, G.; Beattie, W.S.; Mosseri, M.; Jaffe, A.S.; Alpert, J.S. Perioperative myocardial infarction. Circulation 2009, 119, 2936–2944. [Google Scholar] [CrossRef]
- Adesanya, A.O.; de Lemos, J.A.; Greilich, N.B.; Whitten, C.W. Management of perioperative myocardial infarction in noncardiac surgical patients. Chest 2006, 130, 584–596. [Google Scholar] [CrossRef]
- Fleisher, L.A.; Fleischmann, K.E.; Auerbach, A.D.; Barnason, S.A.; Beckman, J.A.; Bozkurt, B.; Davila-Roman, V.G.; Gerhard-Herman, M.D.; Holly, T.A.; Kane, G.C.; et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014, 130, 2215–2245. [Google Scholar] [CrossRef]
- Mulla, C.M.; Marik, P.E. Pheochromocytoma presenting as acute decompensated heart failure reversed with medical therapy. BMJ Case Rep. 2012, 2012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, J.K.; Cisco, R.M.; Scholten, A.; Mitmaker, E.; Duh, Q.Y. Pheochromocytoma crisis resulting in acute heart failure and cardioembolic stroke in a 37-year-old man. Surgery 2014, 155, 726–727. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Tan, L.Y.R.; Ho, Y.H.; Leow, M.K.S. Giant phaeochromocytoma presenting with an acute stroke: Reappraising phaeochromocytoma surveillance for the neurofibromatosis type 1 phakomatosis. BMJ Case Rep. 2017, 2017. [Google Scholar] [CrossRef] [PubMed]
- Lin, P.C.; Hsu, J.T.; Chung, C.M.; Chang, S.T. Pheochromocytoma underlying hypertension, stroke, and dilated cardiomyopathy. Tex. Heart Inst. J. 2007, 34, 244–246. [Google Scholar] [PubMed]
- Kam, P.C.; Calcroft, R.M. Peri-operative stroke in general surgical patients. Anaesthesia 1997, 52, 879–883. [Google Scholar] [CrossRef] [PubMed]
- Mashour, G.A.; Sharifpour, M.; Freundlich, R.E.; Tremper, K.K.; Shanks, A.; Nallamothu, B.K.; Vlisides, P.E.; Weightman, A.; Matlen, L.; Merte, J.; et al. Perioperative metoprolol and risk of stroke after noncardiac surgery. Anesthesiology 2013, 119, 1340–1346. [Google Scholar] [CrossRef] [PubMed]
- Ng, J.L.; Chan, M.T.; Gelb, A.W. Perioperative stroke in noncardiac, nonneurosurgical surgery. Anesthesiology 2011, 115, 879–890. [Google Scholar] [CrossRef]
- Norris, J.W.; Hachinski, V.C. Misdiagnosis of stroke. Lancet 1982, 1, 328–331. [Google Scholar] [CrossRef]
- Adams, H.P., Jr.; del Zoppo, G.; Alberts, M.J.; Bhatt, D.L.; Brass, L.; Furlan, A.; Grubb, R.L.; Higashida, R.T.; Jauch, E.C.; Kidwell, C.; et al. Guidelines for the early management of adults with ischemic stroke: A guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Circulation 2007, 115, e478–e534. [Google Scholar] [CrossRef]
- Shen, W.T.; Lee, J.; Kebebew, E.; Clark, O.H.; Duh, Q.Y. Selective use of steroid replacement after adrenalectomy: Lessons from 331 consecutive cases. Arch. Surg. 2006, 141, 771–774; discussion 774–776. [Google Scholar] [CrossRef]
- de Graaf, J.S.; Lips, C.J.; Rutter, J.E.; van Vroonhoven, T.J. Subtotal adrenalectomy for phaeochromocytoma in multiple endocrine neoplasia type 2A. Eur J. Surg. 1999, 165, 535–538. [Google Scholar] [CrossRef] [PubMed]
- van Heerden, J.A.; Sizemore, G.W.; Carney, J.A.; Grant, C.S.; ReMine, W.H.; Sheps, S.G. Surgical management of the adrenal glands in the multiple endocrine neoplasia type II syndrome. World J. Surg. 1984, 8, 612–621. [Google Scholar] [CrossRef] [PubMed]
- Lamberts, S.W.; Bruining, H.A.; de Jong, F.H. Corticosteroid therapy in severe illness. N. Engl. J. Med. 1997, 337, 1285–1292. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.M.; Reidy, A.B.; Saatee, S.; Collard, C.D. Perioperative Steroid Management: Approaches Based on Current Evidence. Anesthesiology 2017, 127, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Bornstein, S.R.; Allolio, B.; Arlt, W.; Barthel, A.; Don-Wauchope, A.; Hammer, G.D.; Husebye, E.S.; Merke, D.P.; Murad, M.H.; Stratakis, C.A.; et al. Diagnosis and Treatment of Primary Adrenal Insufficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2016, 101, 364–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortiz, D.I.; Findling, J.W.; Carroll, T.B.; Javorsky, B.R.; Carr, A.A.; Evans, D.B.; Yen, T.W.; Wang, T.S. Cosyntropin stimulation testing on postoperative day 1 allows for selective glucocorticoid replacement therapy after adrenalectomy for hypercortisolism: Results of a novel, multidisciplinary institutional protocol. Surgery 2016, 159, 259–265. [Google Scholar] [CrossRef]
- Arlt, W. The approach to the adult with newly diagnosed adrenal insufficiency. J. Clin. Endocrinol. Metab. 2009, 94, 1059–1067. [Google Scholar] [CrossRef]
- Grossman, A.B. Clinical Review#: The diagnosis and management of central hypoadrenalism. J. Clin. Endocrinol. Metab. 2010, 95, 4855–4863. [Google Scholar] [CrossRef] [PubMed]
- Celik, H.; Celik, O.; Guldiken, S.; Inal, V.; Puyan, F.O.; Tugrul, A. Pheochromocytoma presenting with rhabdomyolysis and acute renal failure: A case report. Ren. Fail. 2014, 36, 104–107. [Google Scholar] [CrossRef]
- Jin, Y.S.; Fan, M.X. Pheochromocytoma Characterizing Both Fever and Acute Renal Failure. Chin. Med. J. 2017, 130, 617–618. [Google Scholar] [CrossRef]
- Pickard, J.L.; Ross, G., Jr.; Silver, D. Coexisting extraadrenal pheochromocytoma and renal artery stenosis: A case report and review of the pathophysiology. J. Pediatr. Surg. 1995, 30, 1613–1615. [Google Scholar] [CrossRef]
- Kaufman, J.J. Pheochromocytoma and stenosis of the renal artery. Surg. Gynecol. Obstet. 1983, 156, 11–15. [Google Scholar] [PubMed]
- Stanley, J.C.; Gewertz, B.L.; Bove, E.L.; Sottiurai, V.; Fry, W.J. Arterial fibrodysplasia. Histopathologic character and current etiologic concepts. Arch. Surg. 1975, 110, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Kota, S.K.; Kota, S.K.; Meher, L.K.; Jammula, S.; Panda, S.; Modi, K.D. Coexistence of pheochromocytoma with uncommon vascular lesions. Indian J. Endocrinol. Metab. 2012, 16, 962–971. [Google Scholar] [CrossRef] [PubMed]
- Burns, A.P.; O’Connell, P.R.; Murnaghan, D.J.; Brady, M.P. Bilateral adrenal phaeochromocytomas associated with unilateral renal artery stenosis. Postgrad. Med. J. 1989, 65, 943–947. [Google Scholar] [CrossRef]
- Gill, I.S.; Meraney, A.M.; Bravo, E.L.; Novick, A.C. Pheochromocytoma coexisting with renal artery lesions. J. Urol. 2000, 164, 296–301. [Google Scholar] [CrossRef]
- Spergel, G.; Bleicher, S.J.; Ertel, N.H. Carbohydrate and fat metabolism in patients with pheochromocytoma. N. Engl. J. Med. 1968, 278, 803–809. [Google Scholar] [CrossRef]
- Reynolds, C.; Wilkins, G.E.; Schmidt, N.; Doll, W.A.; Blix, P.M. Hyperinsulinism after removal of a pheochromocytoma. Can. Med. Assoc. J. 1983, 129, 349–353. [Google Scholar]
- Auer, R.N. Hypoglycemic brain damage. Metab. Brain Dis. 2004, 19, 169–175. [Google Scholar] [CrossRef]
- Levin, H.; Heifetz, M. Phaeochromocytoma and severe protracted postoperative hypoglycaemia. Can. J. Anaesth. 1990, 37, 477–478. [Google Scholar] [CrossRef] [Green Version]
- Cryer, P.E.; Axelrod, L.; Grossman, A.B.; Heller, S.R.; Montori, V.M.; Seaquist, E.R.; Service, F.J.; Endocrine, S. Evaluation and management of adult hypoglycemic disorders: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2009, 94, 709–728. [Google Scholar] [CrossRef] [PubMed]
- Elliott, M.B.; Schafers, S.J.; McGill, J.B.; Tobin, G.S. Prediction and prevention of treatment-related inpatient hypoglycemia. J. Diabetes Sci. Technol. 2012, 6, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Brutsaert, E.; Carey, M.; Zonszein, J. The clinical impact of inpatient hypoglycemia. J. Diabetes Complicat. 2014, 28, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Fischer, K.F.; Lees, J.A.; Newman, J.H. Hypoglycemia in hospitalized patients. Causes and outcomes. N. Engl. J. Med. 1986, 315, 1245–1250. [Google Scholar] [CrossRef] [PubMed]
- Meeke, R.I.; O’Keeffe, J.D.; Gaffney, J.D. Phaeochromocytoma removal and postoperative hypoglycaemia. Anaesthesia 1985, 40, 1093–1096. [Google Scholar] [CrossRef]
- Eiland, L.; Goldner, W.; Drincic, A.; Desouza, C. Inpatient hypoglycemia: A challenge that must be addressed. Curr. Diabetes Rep. 2014, 14, 445. [Google Scholar] [CrossRef]
- Hulkower, R.D.; Pollack, R.M.; Zonszein, J. Understanding hypoglycemia in hospitalized patients. Diabetes Manag. 2014, 4, 165–176. [Google Scholar] [CrossRef] [Green Version]
- Araque, K.A.; Kadayakkara, D.K.; Gigauri, N.; Sheehan, D.; Majumdar, S.; Buller, G.; Flannery, C.A. Reducing severe hypoglycaemia in hospitalised patients with diabetes: Early outcomes of standardised reporting and management. BMJ Open Qual. 2018, 7, e000120. [Google Scholar] [CrossRef] [Green Version]
- Kek, P.C.; Ho, E.T.; Loh, L.M. Phaeochromocytoma presenting with pseudo-intestinal obstruction and lactic acidosis. Singap. Med. J. 2015, 56, e131–e133. [Google Scholar] [CrossRef]
- Osinga, T.E.; Kerstens, M.N.; van der Klauw, M.M.; Koornstra, J.J.; Wolffenbuttel, B.H.; Links, T.P.; van der Horst-Schrivers, A.N. Intestinal pseudo-obstruction as a complication of paragangliomas: Case report and literature review. Neth. J. Med. 2013, 71, 512–517. [Google Scholar]
- Wu, H.W.; Liou, W.P.; Chou, C.C.; Chen, Y.H.; Loh, C.H.; Wang, H.P. Pheochromocytoma presented as intestinal pseudo-obstruction and hyperamylasemia. Am. J. Emerg. Med. 2008, 26, 971.e1–971.e4. [Google Scholar] [CrossRef] [PubMed]
- Sohn, C.I.; Kim, J.J.; Lim, Y.H.; Rhee, P.L.; Koh, K.C.; Paik, S.W.; Rhee, J.C.; Chung, J.H.; Lee, M.S.; Yang, J.H. A case of ischemic colitis associated with pheochromocytoma. Am. J. Gastroenterol. 1998, 93, 124–126. [Google Scholar] [CrossRef] [PubMed]
- Saunders, M.D. Acute colonic pseudo-obstruction. Best Pract. Res. Clin. Gastroenterol. 2007, 21, 671–687. [Google Scholar] [CrossRef] [PubMed]
- Loftus, C.G.; Harewood, G.C.; Baron, T.H. Assessment of predictors of response to neostigmine for acute colonic pseudo-obstruction. Am. J. Gastroenterol. 2002, 97, 3118–3122. [Google Scholar] [CrossRef] [PubMed]
- Eisen, G.M.; Baron, T.H.; Dominitz, J.A.; Faigel, D.O.; Goldstein, J.L.; Johanson, J.F.; Mallery, J.S.; Raddawi, H.M.; Vargo, J.J.; Waring, J.P.; et al. Acute colonic pseudo-obstruction. Gastrointest. Endosc. 2002, 56, 789–792. [Google Scholar] [CrossRef]
- Yamaguchi, I.; Kopin, I.J. Differential inhibiton of alpha-1 and alpha-2 adrenoceptor-mediated pressor responses in pithed rats. J. Pharmacol. Exp. Ther. 1980, 214, 275–281. [Google Scholar] [PubMed]
- Khafagi, F.A.; Lloyd, H.M.; Gough, I.R. Intestinal pseudo-obstruction in pheochromocytoma. Aust. N. Z. J. Med. 1987, 17, 246–248. [Google Scholar] [CrossRef]
- Hashimoto, Y.; Motoyoshi, S.; Maruyama, H.; Sakakida, M.; Yano, T.; Yamaguchi, K.; Goto, K.; Sugihara, S.; Takano, S.; Kambara, T.; et al. The treatment of pheochromocytoma associated with pseudo-obstruction and perforation of the colon, hepatic failure, and DIC. Jpn. J. Med. 1990, 29, 341–346. [Google Scholar] [CrossRef]
- Marik, P.E.; Rivera, R. Hypertensive emergencies: An update. Curr. Opin. Crit. Care 2011, 17, 569–580. [Google Scholar] [CrossRef]
- Young, P.Y.; Khadaroo, R.G. Surgical site infections. Surg. Clin. N. Am. 2014, 94, 1245–1264. [Google Scholar] [CrossRef]
- Darrah, D.M.; Griebling, T.L.; Silverstein, J.H. Postoperative urinary retention. Anesthesiol. Clin. 2009, 27, 465–484, table of contents. [Google Scholar] [CrossRef] [PubMed]
- Pavlin, D.J.; Pavlin, E.G.; Gunn, H.C.; Taraday, J.K.; Koerschgen, M.E. Voiding in patients managed with or without ultrasound monitoring of bladder volume after outpatient surgery. Anesth. Analg. 1999, 89, 90–97. [Google Scholar] [PubMed]
- Sarasin, S.M.; Walton, M.J.; Singh, H.P.; Clark, D.I. Can a urinary tract symptom score predict the development of postoperative urinary retention in patients undergoing lower limb arthroplasty under spinal anaesthesia? A prospective study. Ann. R. Coll. Surg. Engl. 2006, 88, 394–398. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Adrenoceptor Subtype | Agonists | Tissue | Responses |
|---|---|---|---|
| α1 * | EPI≥NE>>Iso Phenylephrine | Vascular smooth muscle | Vasoconstriction |
| Liver Ŧ | Glycogenolysis, gluconeogenesis | ||
| Intestinal smooth muscle | Hyperpolarization and relaxation | ||
| Heart | Chronotropic, arrhythmias | ||
| α2 * | EPI≥NE>>Iso Clonidine | Pancreatic islets (/cells) | Decreased insulin secretion |
| Platelets | Aggregation | ||
| Nerve terminals | Decreased release of NE | ||
| Vascular smooth muscle | Vasoconstriction | ||
| β1 | Iso>EPI=NE Dobutamine | Heart | Chronotropic and inotropic |
| β2 | Iso>EPI>>NE Terbutaline | Juxtaglomerular cells Smooth muscle (vascular, bronchial, and gastrointestinal) Skeletal muscle Liver Ŧ | Increased renin secretion Relaxation |
| β3 ŧ | Iso=NE>EPI | Adipose tissue | Glycogenolysis, uptake of K+ Glycogenolysis, gluconeogenesis lipolysis |
| Effector Organs | Adrenergic Impulses | Cholinergic Impulses | |
|---|---|---|---|
| Receptor Type * | Responses Ŧ | Responses Ŧ | |
| Heart ŧ | |||
| SA node | β1, β2 | Chronotropic ++ | Chronotrophy −−, vagal arrest +++ |
| Atria | β1, β2 | Inotropic and chronotropic ++ | Inotropic −−, shortened AP duration ++ |
| AV node | β1, β2 | Increase in automaticity and chronotropic ++ | Chronotropic −−, AV block +++ |
| His-Purkinje system | β1, β2 | Increase in automaticity and chronotropic +++ | Little effect |
| Ventricles | β1, β2 | inotropic, chronotropic automaticity, and rate of idioventricular pacemakers +++ | Slight decrease in contractility |
| Arterioles | |||
| Coronary | α1, α2, β2 | Constriction +, dilations § ++ | Constriction + |
| Skin and mucosa | α1, α2 | Constriction +++ | Dilation || |
| Skeletal muscle | α1, β2 | Constriction +, dilation § ++, $++ | Dilation **+ |
| Cerebral | α1 | Constriction (slight) | Dilation || |
| Pulmonary | α1, β2 | Constriction +, dilations § | Dilation || |
| Abdominal viscera | α1; β2 | Constriction +++, dilation $+ | − |
| Salivary glands | α1, α2 | Constriction +++, | Dilation++ |
| Renal | α1, α2, β1, β2 | Constriction +++, dilation $+ | − |
| Veins (systemic) | |||
| Veins | α1, α2, β2 | Constriction ++, dilation++ | − |
| Lung | |||
| Tracheal and bronchial muscle | β2 | Relaxation + | Contraction ++ |
| Bronchial glands | α1, β2 | Decreased secretion, increased secretion | Stimulation +++ |
| Stomach | |||
| Mobility and tone | α1, α2, β2 | Decrease (usually) ŦŦ+ | Increase +++ |
| Sphincters | α1 | Contraction (usually) + | Relaxation (usually) + |
| Secretion | Inhibition | Stimulation +++ | |
| Intestine | |||
| Mobility and tone | α1, α2, β1, β2 | Decrease (usually)+ | Increase +++ |
| Sphincters | α1 | Contraction (usually) + | Relaxation (usually) + |
| Secretion | α2 | Inhibition | Stimulation ++ |
| Gallbladder and ducts | |||
| β2 | Relaxation + | Contraction + | |
| Kidney | |||
| Renin Secretion | α1, β1 | Decrease +, increase ++ | − |
| Urinary bladder | |||
| Detrusor | β2 | Relaxation (usually) + | Contraction +++ |
| Trigone and sphincter | α1 | Contraction ++ | Relaxation ++ |
| Ureter | |||
| Mobility and tone | α1 | Increase | Increase (+) |
| Adrenal medulla | |||
| − | Secretion of epinephrine and norepinephrine (primarily nicotinic and secondarily muscarinic) | ||
| Skeletal muscle | |||
| β2 | Increased contractility, glycogenolysis, K+ uptake | − | |
| Liver | |||
| α1, β2 | Glycogenolysis and gluconeogenesis $$ +++ | − | |
| Pancreas | |||
| Acini | α | Decreased secretion + | Secretion ++ |
| Islets (β cells) | α2 | Decreased secretion +++ | − |
| β2 | Increased secretion + | − | |
| Anti-Hypertensive Medication | Mechanism of Action | Route of Administration | Dose |
|---|---|---|---|
| α- and β-adrenoceptor blockers | |||
| Phentolamine | Competitive α1- and α2-adrenoceptor blocker | IV | Bolus dose 5 g Maintenance dose 0.5 mg/min |
| Esmolol | β1-adrenoceptor antagonist | IV | Starting dose 0.5 ml/kg Maintenance dose 50–300 µg/kg/min |
| Metoprolol | β1-adrenoceptor antagonist | IV | 5 mg every 5 mins as tolerated up to 15 mg total dose |
| Labetalol | Selective α1- and nonselective β-adrenoceptor antagonist | IV | Loading dose 10–20 mg, double initial dose every 10 mins until target blood pressure is attained |
| Calcium channel blockers | |||
| Nicardipine | NE mediated transmembrane calcium influx into vascular smooth muscles | IV | Starting dose 5 mg/h, dose increased by 2.5 mg/h every 5mins to a maximum of 15 mg/h |
| Clevidepine | Increase cardiac output Decrease afterload | IV | Starting dose 1–2 mg/h Maintenance dose 4–6 mg/h |
| Others | |||
| Nitroglycerin | Venous dilator Decrease preload | IV | Starting dose 5–10 µg/min (increase the dose by 5 µg/min every 5 mins until desired effect is achieved) |
| Hydralazine | Decrease arterial vascular resistance | IV | 10 mg over 2 mins, additional doses as needed |
| Magnesium sulfate | •Inhibition of release catecholamines •Direct inhibition of catecholamines receptors •Endogenous calcium antagonist | IV | Bolus dose 2–4 g over 2 mins Maintenance dose 1–2 g/h, dose adjusted on magnesium blood levels |
| Medications | Dosage | Goal of Treatment |
|---|---|---|
| Aspirin | 325 mg PO | Inhibition of platelet aggregation and activation |
| High-intensity Statin | Lowers LDL cholesterol levels in blood by approximately ≥ 50%, atherosclerotic plaque stabilization | |
| Atorvastatin | 40–80 mg PO | |
| Rosuvastatin | 20–40 mg PO | |
| β-adrenoceptor blocker | Lowering heart rate, pain resolution, ST-segment normalization | |
| Metoprolol | 1–5 mg IV, incrementally repeat as needed up to 15 mg total dose 25–50 mg PO three to four times a day | |
| Esmolol | 10–50 mg IV bolus, infusion up to 200 µg/kg/min | |
| Morphine sulfate | 2–5 mg IV, repeat as needed | Pain control |
| Nitroglycerin | 0.4 mg sublingual every five minutes up to a total of three doses. Transdermal patch starting at 0.2 mg/h and increasing to 0.6 mg/h with drug-free period from 6 to 8 PM 50 µg/min IV, titrate upwards as mean arterial pressure tolerates | Pain elimination by coronary vasodilation and ST-segment normalization |
| Complication | Reason | Recommended First Line Management |
|---|---|---|
| Hypertension | •Incomplete tumor removal •Tumor present at unknown location •Metastatic tumor •Excessive vasopressor use •Surplus IV fluids administration •Pain medication •Underlying essential hypertension | Nicardipine Labetalol |
| Hypotension | •Chronically low circulating plasma volume •Prolonged (preoperative) α-adrenoceptor blockade action •Abrupt decrease in serum catecholamines levels •Downregulation of adrenoceptors •Blood loss | IV fluids # |
| Arrhythmia | Tachyarrhythmia: •Elevated sympathetic activity from increased catecholamines levels and pain •Use of inotropes for postoperative hypotension •Rebound effect of preoperative discontinuation of β-adrenoceptor blockers | Stable narrow complex sinus tachycardia: Treat underlying cause Stable regular narrow complex non-sinus tachycardia: Vagal maneuvers- adenosine, expert consultation Stable irregular narrow complex tachycardia: Expert consultation. Stable wide complex tachycardia: Expert consultation Hemodynamically unstable tachycardia: Electrical cardioversion |
| Bradyarrhythmia: •Progression of native conduction disease •Electrolyte disturbance •Sinus node dysfunction •Heart block •Excessive medication used such as β-adrenoceptor blockers | Treatment of underlying abnormalities Atropine Dopamine Epinephrine | |
| Myocardial infarction | Increased catecholamines causes myocyte injury by: •Hemodynamic compromise •Tachycardia •Increased oxygen consumption •Coronary artery vasoconstriction | 12-lead EKG Expert consultation |
| Heart failure | •Desensitized adrenoceptors on myocardium •Cardiomyopathy | Expert consultation |
| Cerebrovascular accident | •Uncontrolled hypertension •Thrombotic or embolic occlusion of cerebral artery •Rupture of intracranial artery leading to hemorrhage | Expert consultation |
| Adrenocortical insufficiency | •PHEO resection with concomitant cortisol hypersecretion | Hydrocortisone Fludrocortisone |
| •Bilateral adrenalectomy | ||
| Renal Failure | •Hypoperfusion of renal bed (hypotension, hypertension and massive bleeding) •Secondary to rhabdomyolysis | Antihypertensive medication (if hypertension exits) IV fluid therapy based on electrolytes Hemodialysis |
| Hypoglycemia | •Hyperinsulinemia from increased catecholamine secretion (predominantly β-adrenergic) •Sudden withdrawal of catecholamines | 50% Dextrose (0.5 ml ampules) Maintenance fluid must include 5–20% dextrose. |
| Intestinal pseudo-obstruction | •Hypomotility from increased catecholamines •Mesenteric vasoconstriction (predominantly α-adrenergic) •Use of opioid analgesics | Laxatives diet with high fiber content, enema |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mamilla, D.; Araque, K.A.; Brofferio, A.; Gonzales, M.K.; Sullivan, J.N.; Nilubol, N.; Pacak, K. Postoperative Management in Patients with Pheochromocytoma and Paraganglioma. Cancers 2019, 11, 936. https://doi.org/10.3390/cancers11070936
Mamilla D, Araque KA, Brofferio A, Gonzales MK, Sullivan JN, Nilubol N, Pacak K. Postoperative Management in Patients with Pheochromocytoma and Paraganglioma. Cancers. 2019; 11(7):936. https://doi.org/10.3390/cancers11070936
Chicago/Turabian StyleMamilla, Divya, Katherine A. Araque, Alessandra Brofferio, Melissa K. Gonzales, James N. Sullivan, Naris Nilubol, and Karel Pacak. 2019. "Postoperative Management in Patients with Pheochromocytoma and Paraganglioma" Cancers 11, no. 7: 936. https://doi.org/10.3390/cancers11070936
APA StyleMamilla, D., Araque, K. A., Brofferio, A., Gonzales, M. K., Sullivan, J. N., Nilubol, N., & Pacak, K. (2019). Postoperative Management in Patients with Pheochromocytoma and Paraganglioma. Cancers, 11(7), 936. https://doi.org/10.3390/cancers11070936