Increased Soluble CMG2 Serum Protein Concentration Is Associated with the Progression of Prostate Carcinoma



Abstract
:1. Introduction
2. Results
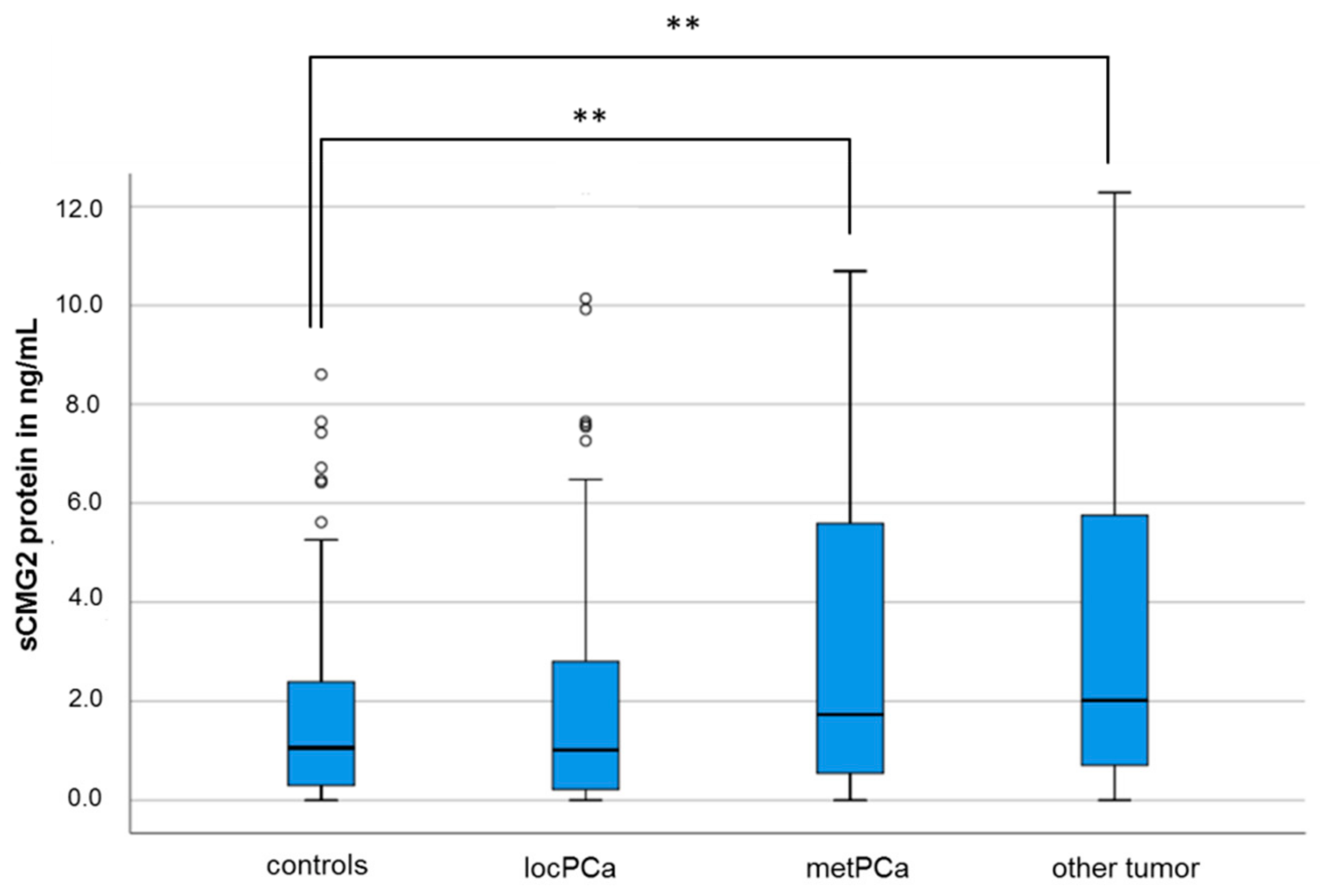
2.1. sCMG2 Concentration in the Serum of Control Subjects and PCa Patients
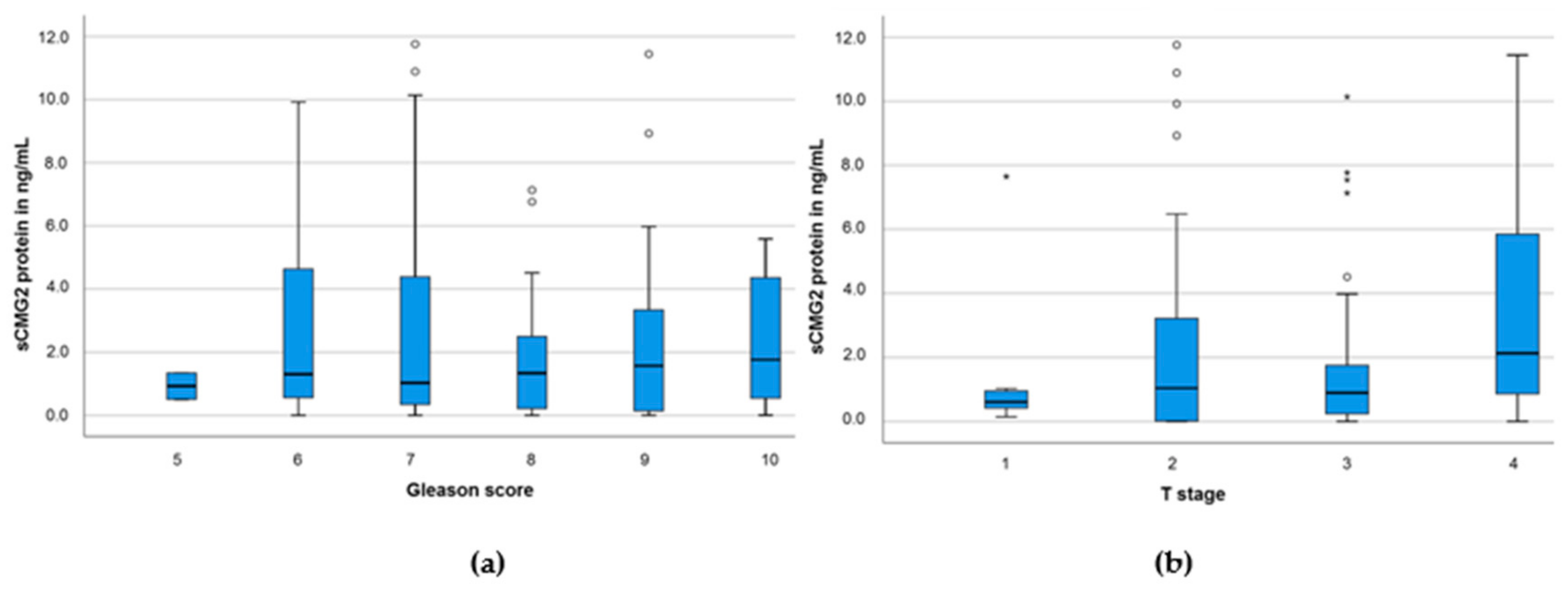
2.2. sCMG2 Concentration and PCa Clinical Parameters
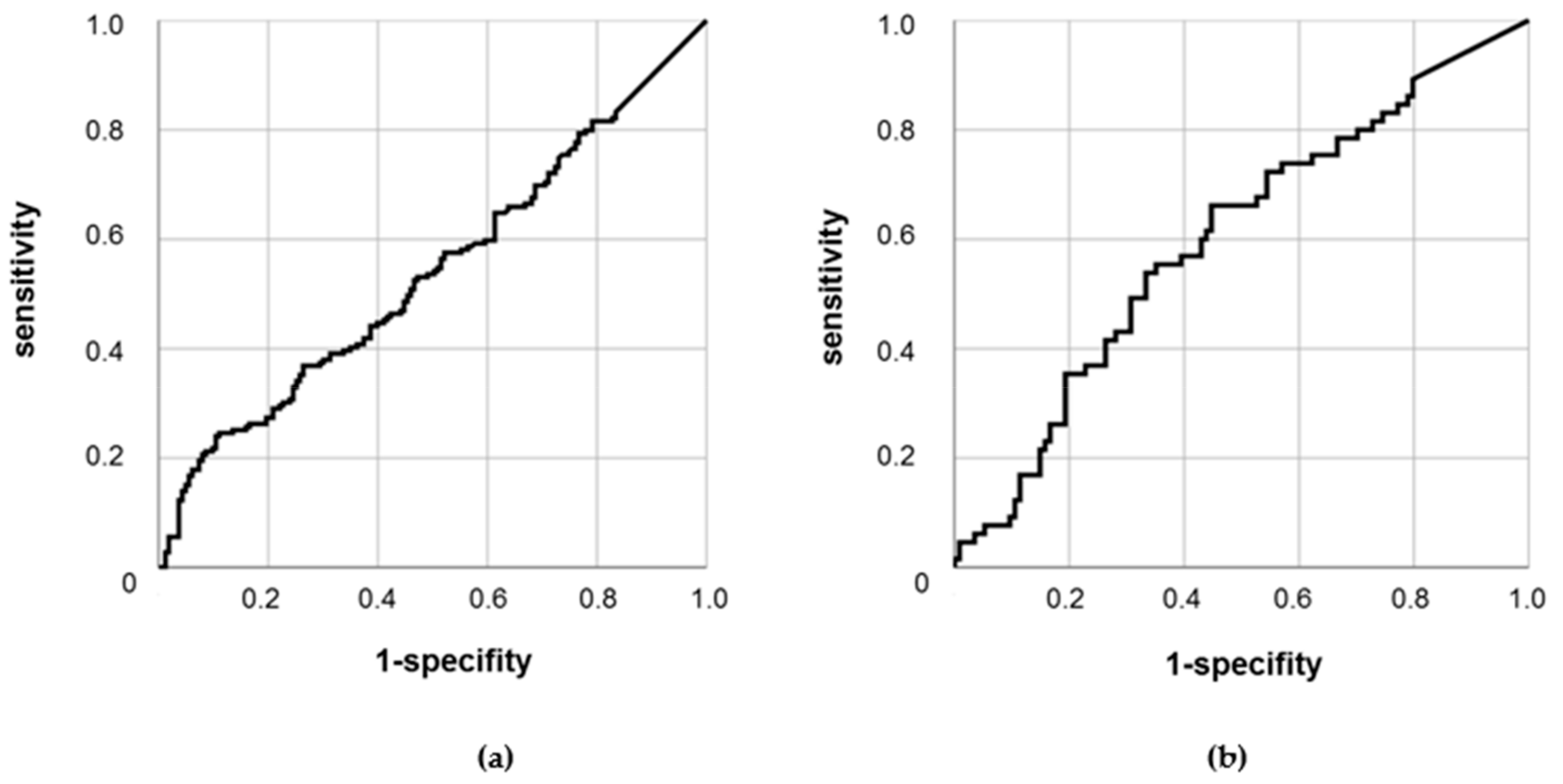
2.3. Diagnostic Capability of sCMG2
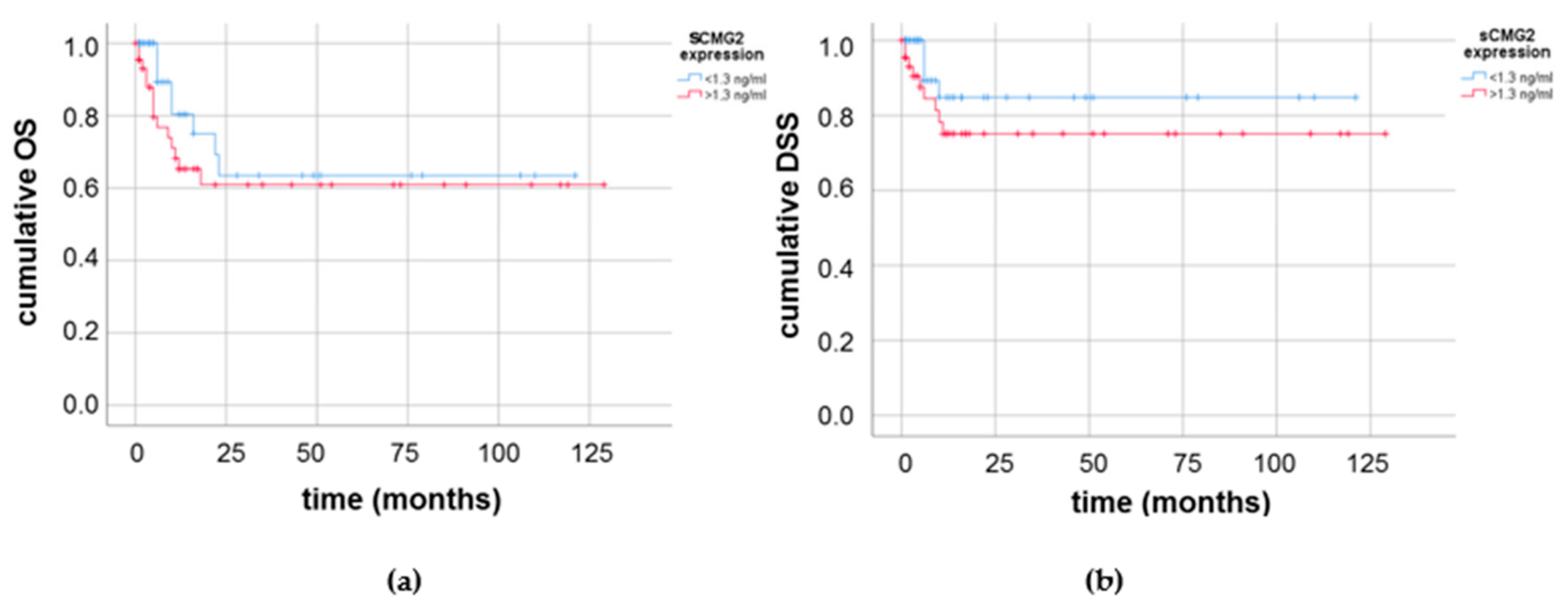
2.4. Prognostic Value of sCMG2 in the Serum of PCa Patients
3. Discussion
4. Materials and Methods
4.1. Study Subjects and Blood Sampling
4.2. ELISA Measurements
4.3. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Zheng, R.; Baade, P.D.; Zhang, S.; Zeng, H.; Bray, F.; Jemal, A.; Yu, X.Q.; He, J. Cancer statistics in China, 2015. CA Cancer J. Clin. 2016, 66, 115–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, L.; Montironi, R.; Bostwick, D.G.; Lopez-Beltran, A.; Berney, D.M. Staging of prostate cancer. Histopathology 2012, 60, 87–117. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, D.T.; Lee, R.J. Cell-free and circulating tumor cell-based biomarkers in men with metastatic prostate cancer: Tools for real-time precision medicine? Urol. Oncol. 2016, 34, 490–501. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, J.K.; Magi-Galluzzi, C. Unfavorable pathology, tissue biomarkers and genomic tests with clinical implications in prostate cancer management. Adv. Anat. Pathol. 2018, 25, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Kontos, C.K.; Adamopoulos, P.G.; Scorilas, A. Prognostic and predictive biomarkers in prostate cancer. Expert Rev. Mol. Diagn. 2015, 15, 1567–1576. [Google Scholar] [CrossRef] [Green Version]
- Pezaro, C.; Woo, H.H.; Davis, I.D. Prostate cancer: Measuring PSA. Intern. Med. J. 2014, 44, 433–440. [Google Scholar] [CrossRef]
- Bussemakers, M.J.; van Bokhoven, A.; Verhaegh, G.W.; Smit, F.P.; Karthaus, H.F.; Schalken, J.A.; Debruyne, F.M.; Ru, N.; Isaacs, W.B. DD3: A new prostate-specific gene, highly overexpressed in prostate cancer. Cancer Res. 1999, 59, 5975–5979. [Google Scholar]
- Mao, Z.; Ji, A.; Yang, K.; He, W.; Hu, Y.; Zhang, Q.; Zhang, D.; Xie, L. Diagnostic performance of PCA3 and hK2 in combination with serum PSA for prostate cancer. Medicine 2018, 97, e12806. [Google Scholar] [CrossRef]
- Newcomb, L.F.; Zheng, Y.; Faino, A.V.; Bianchi-Frias, D.; Cooperberg, M.R.; Brown, M.D.; Brooks, J.D.; Dash, A.; Fabrizio, M.D.; Gleave, M.E.; et al. Performance of PCA3 and TMPRSS2:ERG urinary biomarkers in prediction of biopsy outcome in the Canary Prostate Active Surveillance Study (PASS). Prostate Cancer Prostatic Dis. 2019. [Google Scholar] [CrossRef] [PubMed]
- Wach, S.; Nolte, E.; Szczyrba, J.; Stöhr, R.; Hartmann, A.; Ørntoft, T.; Dyrskjøt, L.; Eltze, E.; Wieland, W.; Keck, B.; et al. MicroRNA profiles of prostate carcinoma detected by multiplatform microRNA screening. Int. J. Cancer 2012, 130, 611–621. [Google Scholar] [CrossRef] [PubMed]
- Selth, L.A.; Townley, S.; Gillis, J.L.; Ochnik, A.M.; Murti, K.; Macfarlane, R.J.; Chi, K.N.; Marshall, V.R.; Tilley, W.D.; Butler, L.M. Discovery of circulating microRNAs associated with human prostate cancer using a mouse model of disease. Int. J. Cancer 2012, 131, 652–661. [Google Scholar] [CrossRef] [PubMed]
- Miyake, H.; Hara, I.; Yamanaka, K.; Arakawa, S.; Kamidono, S. Elevation of urokinase-type plasminogen activator and its receptor densities as new predictors of disease progression and prognosis in men with prostate cancer. Int. J. Oncol. 1999, 14, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Lippert, S.; Berg, K.D.; Høyer-Hansen, G.; Lund, I.K.; Iversen, P.; Christensen, I.J.; Brasso, K.; Røder, M.A. Copenhagen uPAR prostate cancer (CuPCa) database: Protocol and early results. Biomark. Med. 2016, 10, 209–216. [Google Scholar] [CrossRef]
- Kachakova, D.; Mitkova, A.; Popov, E.; Popov, I.; Vlahova, A.; Dikov, T.; Christova, S.; Mitev, V.; Slavov, C.; Kaneva, R. Combinations of serum prostate-specific antigen and plasma expression levels of let-7c, miR-30c, miR-141 and miR-375 as potential better diagnostic biomarkers for prostate cancer. DNA Cell Biol. 2015, 34, 189–200. [Google Scholar] [CrossRef]
- Wach, S.; Al-Janabi, O.; Weigelt, K.; Fischer, K.; Greither, T.; Marcou, M.; Theil, G.; Nolte, E.; Holzhausen, H.J.; Stöhr, R.; et al. The combined serum levels of miR-375 and urokinase plasminogen activator receptor are suggested as diagnostic and prognostic biomarkers in prostate cancer. Int. J. Cancer 2015, 137, 1406–1416. [Google Scholar] [CrossRef]
- Bell, S.E.; Mavila, A.; Salazar, R.; Bayless, K.J.; Kanagala, S.; Maxwell, S.A.; Davis, G.E. Differential gene expression during capillary morphogenesis in 3D collagen matrices: Regulated expression of genes involved in basement membrane matrix assembly, cell cycle progression, cellular differentiation and G-protein signaling. J. Cell Sci. 2001, 114, 2755–2773. [Google Scholar]
- Scobie, H.M.; Rainey, G.J.A.; Bradley, K.A.; Young, J.A.T. Human capillary morphogenesis protein 2 functions as an anthrax toxin receptor. Proc. Natl. Acad. Sci. USA 2003, 100, 5170–5174. [Google Scholar] [CrossRef] [Green Version]
- Reeves, C.V.; Dufraine, J.; Young, J.A.T.; Kitajewski, J. Anthrax toxin receptor 2 is expressed in murine and tumor vasculature and functions in endothelial proliferation and morphogenesis. Oncogene 2010, 29, 789–801. [Google Scholar] [CrossRef]
- Cryan, L.M.; Bazinet, L.; Habeshian, K.A.; Cao, S.; Clardy, J.; Christensen, K.A.; Rogers, M.S. 1,2,3,4,6-Penta-O-galloyl-β-D-glucopyranose inhibits angiogenesis via inhibition of capillary morphogenesis gene 2. J. Med. Chem. 2013, 56, 1940–1945. [Google Scholar] [CrossRef] [PubMed]
- G-Doyagüez, E.; Carrero, P.; Madrona, A.; Rodriguez-Salamanca, P.; Martínez-Gualda, B.; Camarasa, M.J.; Jimeno, M.L.; Bennallack, P.R.; Finnell, J.G.; Tsang, T.M.; et al. Galloyl Carbohydrates with Antiangiogenic Activity Mediated by Capillary Morphogenesis Gene 2 (CMG2) Protein Binding. J. Med. Chem. 2019, 62, 3958–3970. [Google Scholar] [CrossRef] [PubMed]
- Zou, J.; Xu, L.; Ju, Y.; Zhang, P.; Wang, Y.; Zhang, B. Cholesterol depletion induces ANTXR2-dependent activation of MMP-2 via ERK1/2 phosphorylation in neuroglioma U251 cell. Biochem. Biophys. Res. Commun. 2014, 452, 186–190. [Google Scholar] [CrossRef] [PubMed]
- Bürgi, J.; Kunz, B.; Abrami, L.; Deuquet, J.; Piersigilli, A.; Scholl-Bürgi, S.; Lausch, E.; Unger, S.; Superti-Furga, A.; Bonaldo, P.; et al. CMG2/ANTXR2 regulates extracellular collagen VI which accumulates in hyaline fibromatosis syndrome. Nat. Commun. 2017, 8, 15861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Available online: https://www.uniprot.org/uniprot/P58335 (accessed on 20 June 2019).
- Cai, C.; Che, J.; Xu, L.; Guo, Q.; Kong, Y.; Fu, L.; Xu, J.; Cheng, Y.; Chen, W. Tumor endothelium marker-8 based decoys exhibit superiority over capillary morphogenesis protein-2 based decoys as anthrax toxin inhibitors. PLoS ONE 2011, 6, e20646. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Guo, Q.; Liu, J.; Zhang, J.; Yin, Y.; Dong, D.; Fu, L.; Xu, J.; Chen, W. Recombinant HSA-CMG2 Is a Promising Anthrax Toxin Inhibitor. Toxins 2016, 8, 28. [Google Scholar] [CrossRef] [PubMed]
- Cryan, L.M.; Rogers, M.S. Targeting the anthrax receptors, TEM-8 and CMG-2, for anti-angiogenic therapy. Front. Biosci. (Landmark edition) 2011, 16, 1574–1588. [Google Scholar] [CrossRef]
- Chaudhary, A.; St Croix, B. Selective blockade of tumor angiogenesis. Cell cycle (Georgetown, Tex.) 2012, 11, 2253–2259. [Google Scholar] [CrossRef] [Green Version]
- Cao, S.; Cryan, L.; Habeshian, K.A.; Murillo, C.; Tamayo-Castillo, G.; Rogers, M.S.; Clardy, J. Phenolic compounds as antiangiogenic CMG2 inhibitors from Costa Rican endophytic fungi. Bioorg. Med. Chem. Lett. 2012, 22, 5885–5888. [Google Scholar] [CrossRef]
- Ye, L.; Sun, P.H.; Sanders, A.J.; Martin, T.A.; Lane, J.; Mason, M.D.; Jiang, W.G. Therapeutic potential of capillary morphogenesis gene 2 extracellular vWA domain in tumour-related angiogenesis. Int. J. Oncol. 2014, 45, 1565–1573. [Google Scholar] [CrossRef]
- Ye, L.; Sanders, A.J.; Sun, P.H.; Mason, M.D.; Jiang, W.G. Capillary morphogenesis gene 2 regulates adhesion and invasiveness of prostate cancer cells. Oncol. Lett. 2014, 7, 2149–2153. [Google Scholar] [CrossRef]
- Ji, C.; Yang, L.; Yi, W.; Xiang, D.; Wang, Y.; Zhou, Z.; Qian, F.; Ren, Y.; Cui, W.; Zhang, X.; et al. Capillary morphogenesis gene 2 maintains gastric cancer stem-like cell phenotype by activating a Wnt/β-catenin pathway. Oncogene 2018, 37, 3953–3966. [Google Scholar] [CrossRef]
- Xu, Y.; He, Y.; Xu, W.; Lu, T.; Liang, W.; Jin, W. Promotive effects of capillary morphogenetic protein 2 on glioma cell invasion and the molecular mechanism. Folia Neuropathol. 2019, 57, 6–15. [Google Scholar] [CrossRef]
- Ye, L.; Sun, P.H.; Malik, M.F.A.; Mason, M.D.; Jiang, W.G. Capillary morphogenesis gene 2 inhibits growth of breast cancer cells and is inversely correlated with the disease progression and prognosis. J. Cancer Res. Clin. Oncol. 2014, 140, 957–967. [Google Scholar] [CrossRef]
- Greither, T.; Wedler, A.; Rot, S.; Keßler, J.; Kehlen, A.; Holzhausen, H.J.; Bache, M.; Würl, P.; Taubert, H.; Kappler, M. CMG2 Expression Is an Independent Prognostic Factor for Soft Tissue Sarcoma Patients. Int. J. Mol. Sci. 2017, 18, 2648. [Google Scholar] [CrossRef]
- Tan, J.; Liu, M.; Zhang, J.Y.; Yao, Y.L.; Wang, Y.X.; Lin, Y.; Song, K.; Tan, J.; Wu, J.R.; Cui, Y.H.; et al. Capillary morphogenesis protein 2 is a novel prognostic biomarker and plays oncogenic roles in glioma. J. Pathol. 2018, 245, 160–171. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnosis | n | Age (95% CI) 1 | PSA (95% CI) 2 | |
|---|---|---|---|---|
| Control | BPH | 83 | 66.5 (64.3–68.7) | 3.4 (2.6–4.2) |
| subjects | Kidney-/bladder-related | 41 | 61.4 (57.1–65.7) | 1.9 (1.0–2.8) |
| Testis-related | 9 | 54.2 (47.6–60.8) | 1.9 (0.9–3.0) | |
| PCa-free | 30 | 67.5 (65.2–69.8) | 0.16 (0.03–0.28) | |
| PCa | Localized PCa | 114 | 68.5 (67.2–69.8) | 6.6 (4.9–8.3) |
| Patient | Metastasized PCa | 65 | 70.2 (68.1–72.4) | 186.5 (88.2–284.8) |
| Other | Renal carcinoma | 25 | 72.2 (68.6–75.7) | 2.2 (1.2–3.3) |
| tumor | Urothelial carcinoma | 13 | 75.1 (69.5–76.7) | 9.4 (1.0–26.8) |
| other | 17 | 69.9 (64.7–75.1) | 8.2 (4.3–20.7) |
| Localized PCa (n = 114) | Metastasized PCa (n = 65) | ||
|---|---|---|---|
| 5 | 2 | 0 | |
| 6 | 16 | 0 | |
| Gleason | 7 | 66 | 14 |
| score | 8 | 10 | 11 |
| 9 | 13 | 19 | |
| 10 | 0 | 6 | |
| n.d. | 7 | 15 | |
| 1 | 8 | 0 | |
| T | 2 | 51 | 4 |
| stage | 3 | 33 | 11 |
| 4 | 6 | 37 | |
| n.d. | 16 | 13 | |
| No therapy/active surveillance | 60 | 10 | |
| RP | 54 | 55 | |
| Therapy | Radiotherapy | 24 | 32 |
| Androgen deprivation | 23 | 53 | |
| Chemotherapy | 0 | 26 | |
| No follow-up | 69 | 20 | |
| status | Alive | 43 | 25 |
| deceased | 2 | 20 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Greither, T.; Marcou, M.; Fornara, P.; Behre, H.M. Increased Soluble CMG2 Serum Protein Concentration Is Associated with the Progression of Prostate Carcinoma. Cancers 2019, 11, 1059. https://doi.org/10.3390/cancers11081059
Greither T, Marcou M, Fornara P, Behre HM. Increased Soluble CMG2 Serum Protein Concentration Is Associated with the Progression of Prostate Carcinoma. Cancers. 2019; 11(8):1059. https://doi.org/10.3390/cancers11081059
Chicago/Turabian StyleGreither, Thomas, Marios Marcou, Paolo Fornara, and Hermann M. Behre. 2019. "Increased Soluble CMG2 Serum Protein Concentration Is Associated with the Progression of Prostate Carcinoma" Cancers 11, no. 8: 1059. https://doi.org/10.3390/cancers11081059
APA StyleGreither, T., Marcou, M., Fornara, P., & Behre, H. M. (2019). Increased Soluble CMG2 Serum Protein Concentration Is Associated with the Progression of Prostate Carcinoma. Cancers, 11(8), 1059. https://doi.org/10.3390/cancers11081059