Circulating Tumor Cell Enumeration and Characterization in Metastatic Castration-Resistant Prostate Cancer Patients Treated with Cabazitaxel

 , , , ,
, , , , 

Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Circulating Tumor Cells at Baseline
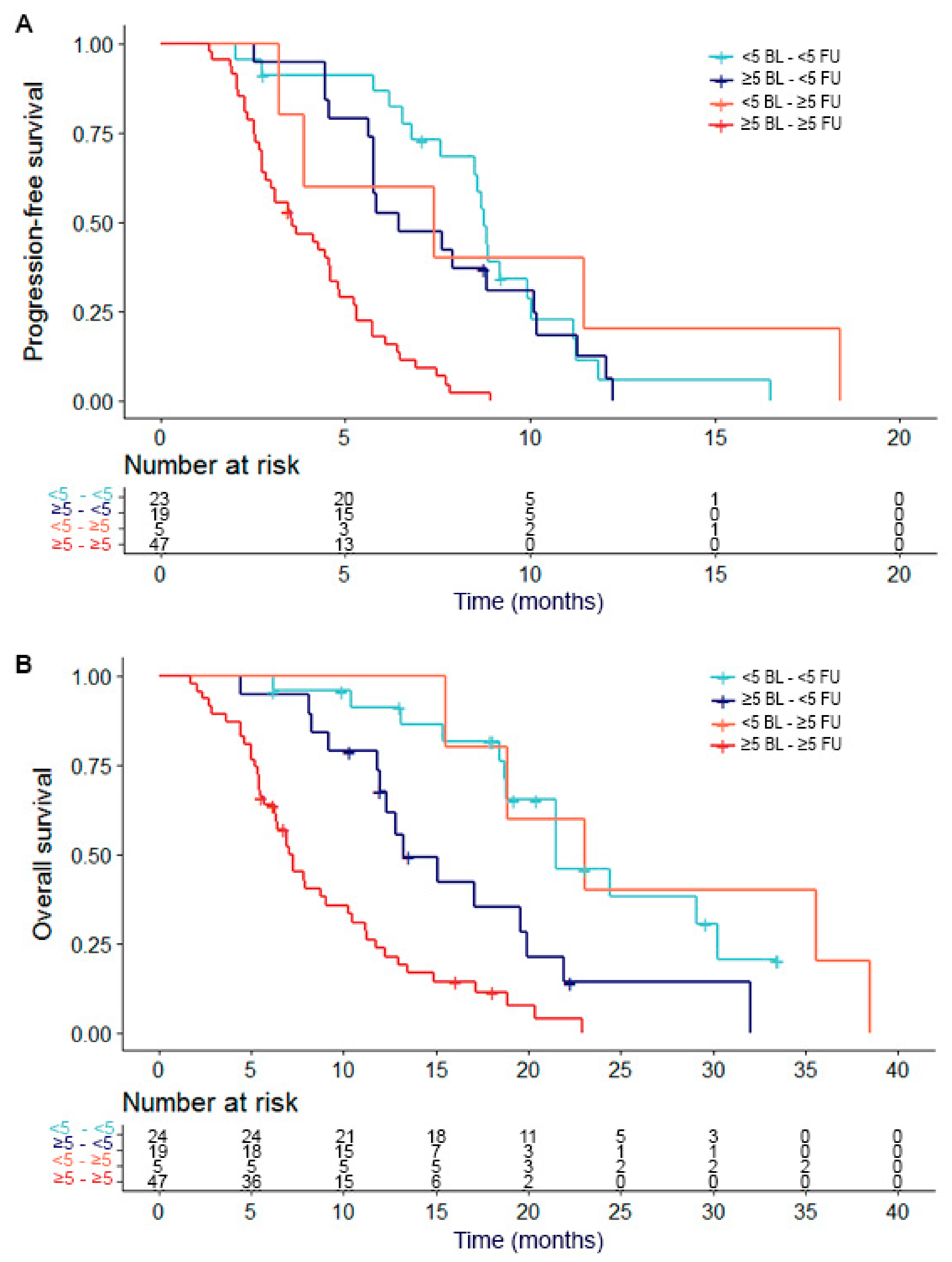
2.3. Circulating Tumor Cell Dynamics at Baseline and Follow-Up
2.4. Gene Expression Profiles of CTC-Specific Genes
2.5. Gene Expression Profiles in Relation to Outcome to Cabazitaxel Therapy
2.6. Cox Regression Analysis
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. CTC Enumeration and mRNA Isolation
4.3. Sample Processing and Normalization
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Gillessen, S.; Omlin, A.; Attard, G.; de Bono, J.S.; Efstathiou, E.; Fizazi, K.; Halabi, S.; Nelson, P.S.; Sartor, O.; Smith, M.R.; et al. Management of patients with advanced prostate cancer: Recommendations of the St Gallen Advanced Prostate Cancer Consensus Conference (APCCC) 2015. Ann Oncol. 2015, 26, 1589–1604. [Google Scholar] [CrossRef]
- De Bono, J.S.; Oudard, S.; Ozguroglu, M.; Hansen, S.; Machiels, J.P.; Kocak, I.; Gravis, G.; Bodrogi, I.; Mackenzie, M.J.; Shen, L.; et al. Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: A randomised open-label trial. Lancet 2010, 376, 1147–1154. [Google Scholar] [CrossRef]
- Tannock, I.F.; de Wit, R.; Berry, W.R.; Horti, J.; Pluzanska, A.; Chi, K.N.; Oudard, S.; Théodore, C.; James, N.D.; Turesson, I.; et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. NEJM 2004, 351, 1502–1512. [Google Scholar] [CrossRef] [PubMed]
- Basch, E.; Autio, K.; Ryan, C.J.; Mulders, P.; Shore, N.; Kheoh, T.; Fizazi, K.; Logothetis, C.J.; Rathkopf, D.; Smith, M.R.; et al. Abiraterone acetate plus prednisone versus prednisone alone in chemotherapy-naive men with metastatic castration-resistant prostate cancer: Patient-reported outcome results of a randomised phase 3 trial. Lancet Oncol. 2013, 14, 1193–1199. [Google Scholar] [CrossRef]
- Beer, T.M.; Armstrong, A.J.; Rathkopf, D.E.; Loriot, Y.; Sternberg, C.N.; Higano, C.S.; Iversen, P.; Bhattacharya, S.; Carles, J.; Chowdhury, S.; et al. Enzalutamide in metastatic prostate cancer before chemotherapy. NEJM 2014, 371, 424–433. [Google Scholar] [CrossRef] [PubMed]
- De Bono, J.S.; Logothetis, C.J.; Molina, A.; Fizazi, K.; North, S.; Chu, L.; Chi, K.N.; Jones, R.J.; Goodman, O.B.; Saad, F.; et al. Abiraterone and increased survival in metastatic prostate cancer. NEJM 2011, 364, 1995–2005. [Google Scholar] [CrossRef]
- Scher, H.I.; Fizazi, K.; Saad, F.; Taplin, M.E.; Sternberg, C.N.; Miller, K.; de Wit, R.; Mulders, P.; Chi, K.N.; Shore, N.D.; et al. Increased survival with enzalutamide in prostate cancer after chemotherapy. NEJM 2012, 367, 1187–1197. [Google Scholar] [CrossRef]
- De Bono, J.S.; Scher, H.I.; Montgomery, R.B.; Parker, C.; Miller, M.C.; Tissing, H.; Doyle, G.V.; Terstappen, L.W.W.M.; Pienta, K.J.; Raghavan, D. Circulating tumor cells predict survival benefit from treatment in metastatic castration-resistant prostate cancer. Clin. Cancer Res. 2008, 14, 6302–6309. [Google Scholar] [CrossRef] [PubMed]
- Olmos, D.; Arkenau, H.T.; Ang, J.E.; Ledaki, I.; Attard, G.; Carden, C.P.; Reid, A.H.M.; A’Hern, R.; Fong, P.C.; Oomen, N.B.; et al. Circulating tumour cell (CTC) counts as intermediate end points in castration-resistant prostate cancer (CRPC): A single-centre experience. Ann Oncol. 2009, 20, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Scher, H.I.; Jia, X.; de Bono, J.S.; Fleisher, M.; Pienta, K.J.; Raghavan, D.; Heller, G. Circulating tumour cells as prognostic markers in progressive, castration-resistant prostate cancer: A reanalysis of IMMC38 trial data. Lancet Oncol. 2009, 10, 233–239. [Google Scholar] [CrossRef]
- Resel Folkersma, L.; San Jose Manso, L.; Galante Romo, I.; Moreno Sierra, J.; Olivier Gomez, C. Prognostic significance of circulating tumor cell count in patients with metastatic hormone-sensitive prostate cancer. Urology 2012, 80, 1328–1332. [Google Scholar] [CrossRef] [PubMed]
- Climent, M.A.; Perez-Valderrama, B.; Mellado, B.; Fernandez Parra, E.M.; Fernandez Calvo, O.; Ochoa de Olza, M.; Romay, L.M.; Anido, U.; Domenech, M.; Polo, S.H.; et al. Weekly cabazitaxel plus prednisone is effective and less toxic for ‘unfit’ metastatic castration-resistant prostate cancer: Phase II Spanish Oncology Genitourinary Group (SOGUG) trial. Eur. J. Cancer 2017, 87, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Antonarakis, E.S.; Lu, C.; Wang, H.; Luber, B.; Nakazawa, M.; Roeser, J.C.; Chen, Y.; Mohammad, T.A.; Chen, Y.; Fedor, H.L.; et al. AR-V7 and resistance to enzalutamide and abiraterone in prostate cancer. NEJM 2014, 371, 1028–1038. [Google Scholar] [CrossRef] [PubMed]
- Onstenk, W.; Sieuwerts, A.M.; Kraan, J.; Van, M.; Nieuweboer, A.J.; Mathijssen, R.H.; Hamberg, P.; Meulenbeld, H.J.; Laere, B.D.; Dirix, L.Y.; et al. Efficacy of Cabazitaxel in Castration-resistant Prostate Cancer Is Independent of the Presence of AR-V7 in Circulating Tumor Cells. Eur. Urol. 2015, 68, 939–945. [Google Scholar] [CrossRef] [PubMed]
- Antonarakis, E.S.; Lu, C.; Luber, B.; Wang, H.; Chen, Y.; Nakazawa, M.; Nadal, R.; Paller, C.J.; Denmeade, S.R.; Carducci, M.A.; et al. Androgen Receptor Splice Variant 7 and Efficacy of Taxane Chemotherapy in Patients With Metastatic Castration-Resistant Prostate Cancer. JAMA Oncol. 2015, 1, 582–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, D.F.; Cristofanilli, M.; Budd, G.T.; Ellis, M.J.; Stopeck, A.; Miller, M.C.; Matera, J.; Allard, W.J.; Doyle, G.V.; Terstappen, L.W.W.M. Circulating tumor cells at each follow-up time point during therapy of metastatic breast cancer patients predict progression-free and overall survival. Clin. Cancer Res. 2006, 12, 4218–4224. [Google Scholar] [CrossRef] [PubMed]
- Halabi, S.; Lin, C.Y.; Kelly, W.K.; Fizazi, K.S.; Moul, J.W.; Kaplan, E.B.; Morris, M.J.; Small, E.J. Updated prognostic model for predicting overall survival in first-line chemotherapy for patients with metastatic castration-resistant prostate cancer. J. Clin. Oncol. 2014, 32, 671–677. [Google Scholar] [CrossRef]
- Bergmann, P.; Body, J.J.; Boonen, S.; Boutsen, Y.; Devogelaer, J.-P.; Goemaere, S.; Kaufman, J.-M.; Reginster, J.-Y.; Gangji, V. Evidence-based guidelines for the use of biochemical markers of bone turnover in the selection and monitoring of bisphosphonate treatment in osteoporosis: A consensus document of the Belgian Bone Club. Int. J. Clin. Pract. 2009, 63, 19–26. [Google Scholar] [CrossRef]
- Heinrich, D.; Bruland, O.; Guise, T.A.; Suzuki, H.; Sartor, O. Alkaline phosphatase in metastatic castration-resistant prostate cancer: Reassessment of an older biomarker. Future Oncol. 2018, 14, 2543–2556. [Google Scholar] [CrossRef]
- Kani, K.; Malihi, P.D.; Jiang, Y.; Wang, H.; Wang, Y.; Ruderman, D.L.; Agus, D.B.; Mallick, P.; Gross, M.E. Anterior gradient 2 (AGR2): Blood-based biomarker elevated in metastatic prostate cancer associated with the neuroendocrine phenotype. Prostate 2013, 73, 306–315. [Google Scholar] [CrossRef]
- Mostert, B.; Sieuwerts, A.M.; Bolt-de Vries, J.; Kraan, J.; Lalmahomed, Z.; van Galen, A.; van der Spoel, P.; de Weerd, V.; Ramírez-Moreno, R.; Smid, M.; et al. mRNA expression profiles in circulating tumor cells of metastatic colorectal cancer patients. Mol. Oncol. 2015, 9, 920–932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sieuwerts, A.M.; Mostert, B.; Bolt-de Vries, J.; Peeters, D.; de Jongh, F.E.; Stouthard, J.M.L.; Dirix, L.Y.; van Dam, P.A.; Galen, A.V.; de Weerd, V.; et al. mRNA and microRNA expression profiles in circulating tumor cells and primary tumors of metastatic breast cancer patients. Clin. Cancer Res. 2011, 17, 3600–3618. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Forootan, S.S.; Liu, D.; Barraclough, R.; Foster, C.S.; Rudland, P.S.; Ke, Y. Increased expression of anterior gradient-2 is significantly associated with poor survival of prostate cancer patients. Prostate Cancer Prostatic Dis. 2007, 10, 293–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, J.L.; Hickey, T.E.; Warren, A.Y.; Vowler, S.L.; Carroll, T.; Lamb, A.D.; Papoutsoglou, N.; Neal, D.E.; Tilley, W.D.; Carroll, J.S.; et al. Elevated levels of FOXA1 facilitate androgen receptor chromatin binding resulting in a CRPC-like phenotype. Oncogene 2014, 33, 5666–5674. [Google Scholar] [CrossRef]
- Rachner, T.D.; Thiele, S.; Gobel, A.; Browne, A.; Fuessel, S.; Erdmann, K.; Wirth, M.P.; Fröhner, M.; Todenhöfer, T.; Muders, M.H.; et al. High serum levels of Dickkopf-1 are associated with a poor prognosis in prostate cancer patients. BMC Cancer. 2014, 14, 649. [Google Scholar] [CrossRef]
- The tumor suppressor FAT1 modulates WNT activity in multiple cancers. Cancer Discov. 2013, 3, 19. [CrossRef]
- Tomlins, S.A.; Rhodes, D.R.; Perner, S.; Dhanasekaran, S.M.; Mehra, R.; Sun, X.W.; Varambally, S.; Cao, X.; Tchinda, J.; Kuefer, R.; et al. Recurrent fusion of TMPRSS2 and ETS transcription factor genes in prostate cancer. Science 2005, 310, 644–648. [Google Scholar] [CrossRef]
- Iljin, K.; Wolf, M.; Edgren, H.; Gupta, S.; Kilpinen, S.; Skotheim, R.I.; Peltola, M.; Smit, F.; Verhaegh, G.; Schalken, J.; et al. TMPRSS2 fusions with oncogenic ETS factors in prostate cancer involve unbalanced genomic rearrangements and are associated with HDAC1 and epigenetic reprogramming. Cancer Res. 2006, 66, 10242–10246. [Google Scholar] [CrossRef] [PubMed]
- Schneider, J.A.; Logan, S.K. Revisiting the role of Wnt/beta-catenin signaling in prostate cancer. Mol. Cell. Endocrinol. 2018, 462, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Murillo-Garzon, V.; Kypta, R. WNT signalling in prostate cancer. Nat. Rev. Urol. 2017, 14, 683–696. [Google Scholar] [CrossRef] [PubMed]
- Marin-Aguilera, M.; Reig, O.; Lozano, J.J.; Jimenez, N.; Garcia-Recio, S.; Erill, N.; Gaba, L.; Tagliapietra, A.; Ortega, V.; Carrera, G.; et al. Molecular profiling of peripheral blood is associated with circulating tumor cells content and poor survival in metastatic castration-resistant prostate cancer. Oncotarget 2015, 6, 10604–10616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dijkstra, S.; Leyten, G.H.; Jannink, S.A.; de Jong, H.; Mulders, P.F.; van Oort, I.M.; Schalken, J.A. KLK3, PCA3, and TMPRSS2-ERG expression in the peripheral blood mononuclear cell fraction from castration-resistant prostate cancer patients and response to docetaxel treatment. Prostate 2014, 74, 1222–1230. [Google Scholar] [CrossRef] [PubMed]
- Heck, M.M.; Thalgott, M.; Schmid, S.C.; Oh, W.K.; Gong, Y.; Wang, L.; Zhu, J.; Seitz, A.-K.; Porst, D.; Höppner, M.; et al. A 2-Gene Panel Derived from Prostate Cancer-Enhanced Transcripts in Whole Blood Is Prognostic for Survival and Predicts Treatment Benefit in Metastatic Castration-Resistant Prostate Cancer. Prostate 2016, 76, 1160–1168. [Google Scholar] [CrossRef] [PubMed]
- Olmos, D.; Brewer, D.; Clark, J.; Danila, D.C.; Parker, C.; Attard, G.; Fleisher, M.; Reid, A.H.M.; Castro, E.; Sandhu, S.K.; et al. Prognostic value of blood mRNA expression signatures in castration-resistant prostate cancer: A prospective, two-stage study. Lancet Oncol. 2012, 13, 1114–1124. [Google Scholar] [CrossRef]
- Ross, R.W.; Galsky, M.D.; Scher, H.I.; Magidson, J.; Wassmann, K.; Lee, G.S.M.; Katz, L.; KSubudhi, S.; Anand, A.; Fleisher, M.; et al. A whole-blood RNA transcript-based prognostic model in men with castration-resistant prostate cancer: A prospective study. Lancet Oncol. 2012, 13, 1105–1113. [Google Scholar] [CrossRef]
- Wang, L.; Gong, Y.; Chippada-Venkata, U.; Heck, M.M.; Retz, M.; Nawroth, R.; Galsky, M.; Tsao, C.-K.; Schadt, E.; de Bono, J.; et al. A robust blood gene expression-based prognostic model for castration-resistant prostate cancer. BMC Med. 2015, 13, 201. [Google Scholar] [CrossRef] [PubMed]
- Singhal, U.; Wang, Y.; Henderson, J.; Niknafs, Y.S.; Qiao, Y.; Gursky, A.; Zaslavsky, A.; Chung, J.-S.; Smith, D.C.; Karnes, R.J.; et al. Multigene Profiling of CTCs in mCRPC Identifies a Clinically Relevant Prognostic Signature. Mol. Cancer Res. 2018, 16, 643–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leon-Mateos, L.; Casas, H.; Abalo, A.; Vieito, M.; Abreu, M.; Anido, U.; Gómez-Tato, A.; López, R.; Abal, M.; Muinelo-Romay, L. Improving circulating tumor cells enumeration and characterization to predict outcome in first line chemotherapy mCRPC patients. Oncotarget 2017, 8, 54708–54721. [Google Scholar] [CrossRef]
- Gupta, S.; Li, J.; Kemeny, G.; Bitting, R.L.; Beaver, J.; Somarelli, J.A.; Ware, K.E.; Gregory, S.; Armstrong, A.J. Whole Genomic Copy Number Alterations in Circulating Tumor Cells from Men with Abiraterone or Enzalutamide-Resistant Metastatic Castration-Resistant Prostate Cancer. Clin. Cancer Res. 2017, 23, 1346–1357. [Google Scholar] [CrossRef]
- Chung, J.S.; Wang, Y.; Henderson, J.; Singhal, U.; Qiao, Y.; Zaslavsky, A.B.; Hovelson, D.H.; Spratt, D.E.; Reichert, Z.; Palapattu, G.S.; et al. Circulating Tumor Cell-Based Molecular Classifier for Predicting Resistance to Abiraterone and Enzalutamide in Metastatic Castration-Resistant Prostate Cancer. Neoplasia 2019, 21, 802–809. [Google Scholar] [CrossRef]
- Miyamoto, D.T.; Zheng, Y.; Wittner, B.S.; Lee, R.J.; Zhu, H.; Broderick, K.T.; Desai, R.; Fox, D.B.; Brannigan, B.W.; Trautwein, J.; et al. RNA-Seq of single prostate CTCs implicates noncanonical Wnt signaling in antiandrogen resistance. Science 2015, 349, 1351–1356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyamoto, D.T.; Lee, R.J.; Kalinich, M.; LiCausi, J.A.; Zheng, Y.; Chen, T.; Milner, J.D.; Emmons, E.; Ho, U.; Broderick, K.; et al. An RNA-Based Digital Circulating Tumor Cell Signature Is Predictive of Drug Response and Early Dissemination in Prostate Cancer. Cancer Discov. 2018, 8, 288–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skerenova, M.; Mikulova, V.; Capoun, O.; Svec, D.; Kolostova, K.; Soukup, V.; Honová, H.; Hanuš, T.; Zima, T. Gene Expression Analysis of Immunomagnetically Enriched Circulating Tumor Cell Fraction in Castration-Resistant Prostate Cancer. Mol. Diagn Ther. 2018, 22, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Sieuwerts, A.M.; Kraan, J.; Bolt, J.; van der Spoel, P.; Elstrodt, F.; Schutte, M.; Martens, J.W.M.; Gratama, J.-W.; Sleijfer, S.; Foekens, J.A. Anti-epithelial cell adhesion molecule antibodies and the detection of circulating normal-like breast tumor cells. J. Natl. Cancer Instit. 2009, 101, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Nieuweboer, A.J.; de Graan, A.M.; Hamberg, P.; Bins, S.; van Soest, R.J.; van Alphen, R.J.; Bergman, A.M.; Beeker, A.; van Halteren, H.; ten Tije, A.J.; et al. Effects of Budesonide on Cabazitaxel Pharmacokinetics and Cabazitaxel-Induced Diarrhea: A Randomized, Open-Label Multicenter Phase II Study. Clin. Cancer Res. 2017, 23, 1679–1683. [Google Scholar] [PubMed]
- Sieuwerts, A.M.; Kraan, J.; Bolt-de Vries, J.; van der Spoel, P.; Mostert, B.; Martens, J.W.; Sleijfer, S.; Foekens, J.A. Molecular characterization of circulating tumor cells in large quantities of contaminating leukocytes by a multiplex real-time PCR. Breast Cancer Res. Treat. 2009, 118, 455–468. [Google Scholar] [CrossRef]
- Zheng, Y.; Zhang, C.; Wu, J.; Cheng, G.; Yang, H.; Hua, L.; Wang, Z. Prognostic Value of Circulating Tumor Cells in Castration Resistant Prostate Cancer: A Meta-analysis. Urol. J. 2016, 13, 2881–2888. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Category | N | % | < 5 CTC | ≥ 5 CTC | p-Value |
|---|---|---|---|---|---|
| Age | 0.968 | ||||
| < 65 years | 31 | 26 | 10 | 19 | |
| ≥ 65 years | 89 | 74 | 27 | 58 | |
| WHO performance score | 0.045 | ||||
| 0 | 61 | 51 | 24 | 33 | |
| 1 | 59 | 49 | 13 | 44 | |
| Type of castration | 1.000 | ||||
| Surgical | 15 | 13 | 5 | 10 | |
| LHRH agonist | 105 | 88 | 32 | 67 | |
| Prior chemotherapy lines | |||||
| 1 (only docetaxel) | 119 | 99 | 37 | 76 | |
| 2 | 1 | 1 | 0 | 1 | |
| Prior antiandrogen therapy for mCRPC * | 0.326 | ||||
| Abiraterone | 23 | 19 | 10 | 12 | |
| Enzalutamide | 9 | 8 | 2 | 7 | |
| Orteronel | 12 | 10 | 3 | 9 | |
| None | 77 | 64 | 23 | 49 | |
| Baseline chemistry | Median | Range | Median (range) | Median (range) | |
| LDH U/L (n = 118) | 312 | 141–1843 | 237.5 (151–531) | 353 (141–1843) | 0.001 |
| ALP U/L (n = 119) | 128 | 39–909 | 105 (43–409) | 174 (39–909) | <0.001 |
| PSA μg/L (n = 120) | 152 | 4.5–5300 | 120 (45–2000) | 175 (7–5300) | 0.519 |
| CTC count (n = 114) | 15.5 | 0–1025 | 1 (0–4) | 51 (5–1025) |
| (A) | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| Variable | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| 5-gene profile | 1.325 | 0.80–2.20 | 0.279 | |||
| CTC count | 1.001 | 1.00–1.00 | 0.011 | 1.001 | 1.00–1.00 | 0.023 |
| Age | 0.988 | 0.95–1.02 | 0.508 | |||
| PSA | 1.000 | 1.00–1.00 | 0.777 | |||
| ALP | 1.001 | 1.00–1.00 | 0.101 | |||
| LDH | 1.000 | 0.99–1.00 | 0.248 | |||
| Albumin | 0.954 | 0.91–1.00 | 0.070 | |||
| Hemoglobin | 0.709 | 0.54–0.93 | 0.011 | 0.731 | 0.56–0.95 | 0.020 |
| (B) | Univariate Analysis | Multivariate Analysis | ||||
| Variable | HR | 95% CI | p-Value | HR | 95%CI | p-Value |
| 5-gene profile | 1.743 | 1.02–2.98 | 0.042 | |||
| CTC count | 1.002 | 1.00–1.00 | 0.006 | 1.002 | 1.00–1.00 | 0.009 |
| Age | 1.015 | 0.98–1.05 | 0.418 | |||
| PSA | 1.000 | 1.00–1.00 | 0.090 | |||
| ALP | 1.001 | 1.00–1.00 | 0.038 | |||
| LDH | 1.001 | 1.00–1.00 | 0.006 | |||
| Albumin | 0.949 | 0.90–1.00 | 0.056 | |||
| Hemoglobin | 0.631 | 0.48–0.84 | 0.002 | 0.642 | 0.48–0.85 | 0.002 |
| (A) | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| Variable | HR | 95% CI | p-Value | HR | 95%CI | p-Value |
| CTC count | 1.002 | 1.00–1.00 | <0.001 | 1.002 | 1.00–1.00 | <0.001 |
| Age | 0.989 | 0.96–1.02 | 0.453 | |||
| PSA | 1.000 | 1.00–1.00 | 0.732 | |||
| ALP | 1.002 | 1.00–1.00 | <0.001 | 1.002 | 1.00–1.00 | 0.014 |
| LDH | 1.001 | 1.00–1.00 | 0.007 | |||
| Albumin | 0.983 | 0.94–1.03 | 0.490 | |||
| Hemoglobin | 0.694 | 0.57–0.85 | <0.001 | 0.749 | 0.61–0.92 | 0.005 |
| (B) | Univariate Analysis | Multivariate Analysis | ||||
| Variable | HR | 95% CI | p-Value | HR | 95%CI | p-Value |
| CTC count | 1.003 | 1.00–1.00 | <0.001 | 1.002 | 1.00–1.00 | <0.001 |
| Age | 1.017 | 0.99–1.05 | 0.276 | |||
| PSA | 1.000 | 1.00–1.00 | 0.112 | |||
| ALP | 1.002 | 1.00–1.00 | <0.001 | 1.002 | 1.00–1.00 | 0.006 |
| LDH | 1.002 | 1.00–1.00 | <0.001 | |||
| Albumin | 0.952 | 0.91–0.99 | 0.044 | |||
| Hemoglobin | 0.551 | 0.44–0.68 | <0.001 | 0.591 | 0.47–0.74 | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Kruijff, I.E.; Sieuwerts, A.M.; Onstenk, W.; Kraan, J.; Smid, M.; Van, M.N.; van der Vlugt-Daane, M.; Oomen-de Hoop, E.; Mathijssen, R.H.J.; Lolkema, M.P.; et al. Circulating Tumor Cell Enumeration and Characterization in Metastatic Castration-Resistant Prostate Cancer Patients Treated with Cabazitaxel. Cancers 2019, 11, 1212. https://doi.org/10.3390/cancers11081212
de Kruijff IE, Sieuwerts AM, Onstenk W, Kraan J, Smid M, Van MN, van der Vlugt-Daane M, Oomen-de Hoop E, Mathijssen RHJ, Lolkema MP, et al. Circulating Tumor Cell Enumeration and Characterization in Metastatic Castration-Resistant Prostate Cancer Patients Treated with Cabazitaxel. Cancers. 2019; 11(8):1212. https://doi.org/10.3390/cancers11081212
Chicago/Turabian Stylede Kruijff, Ingeborg E., Anieta M. Sieuwerts, Wendy Onstenk, Jaco Kraan, Marcel Smid, Mai N. Van, Michelle van der Vlugt-Daane, Esther Oomen-de Hoop, Ron H.J. Mathijssen, Martijn P. Lolkema, and et al. 2019. "Circulating Tumor Cell Enumeration and Characterization in Metastatic Castration-Resistant Prostate Cancer Patients Treated with Cabazitaxel" Cancers 11, no. 8: 1212. https://doi.org/10.3390/cancers11081212
APA Stylede Kruijff, I. E., Sieuwerts, A. M., Onstenk, W., Kraan, J., Smid, M., Van, M. N., van der Vlugt-Daane, M., Oomen-de Hoop, E., Mathijssen, R. H. J., Lolkema, M. P., de Wit, R., Hamberg, P., Meulenbeld, H. J., Beeker, A., Creemers, G.-J., Martens, J. W. M., & Sleijfer, S. (2019). Circulating Tumor Cell Enumeration and Characterization in Metastatic Castration-Resistant Prostate Cancer Patients Treated with Cabazitaxel. Cancers, 11(8), 1212. https://doi.org/10.3390/cancers11081212