Low Numbers of Vascular Vessels Correlate to Progression in Hormone-Naïve Prostate Carcinomas Undergoing Radical Prostatectomy

 ,
, 
Abstract
:1. Introduction
2. Results
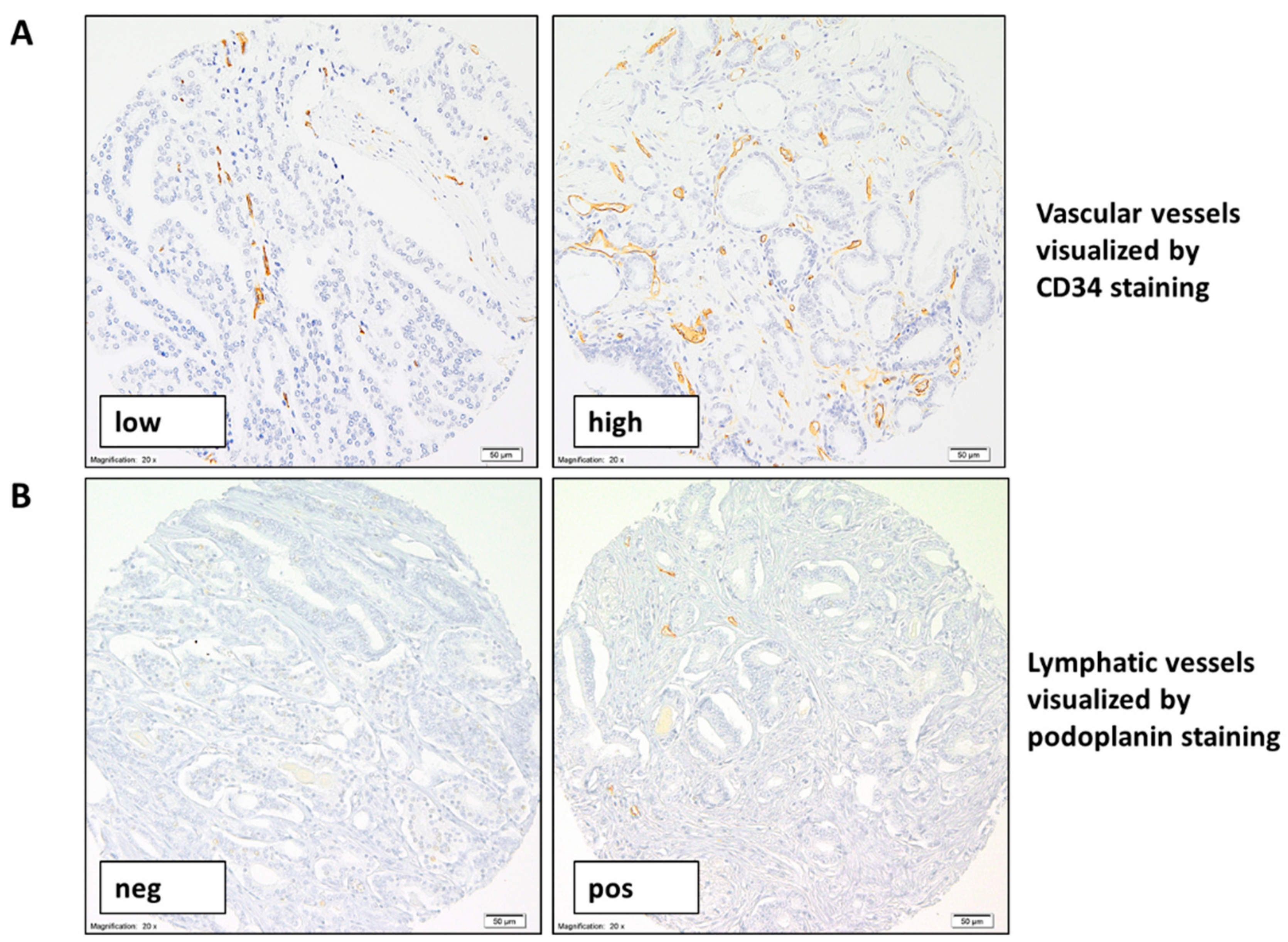
2.1. High Variability of Numbers of Vascular and Lymphatic Vessels in Prostate Carcinoma
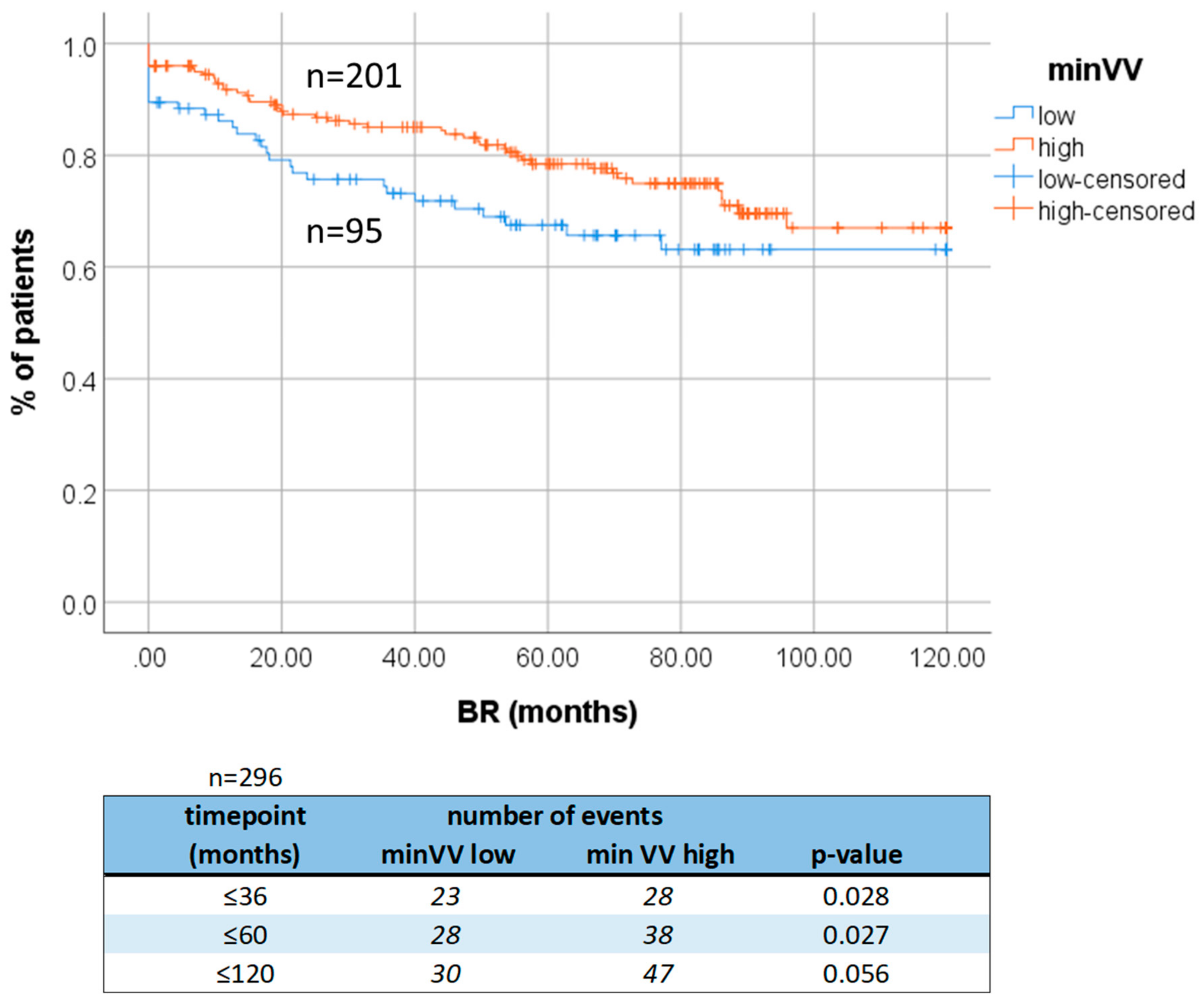
2.2. Clinical Relevance of Low Number of Vascular Vessels
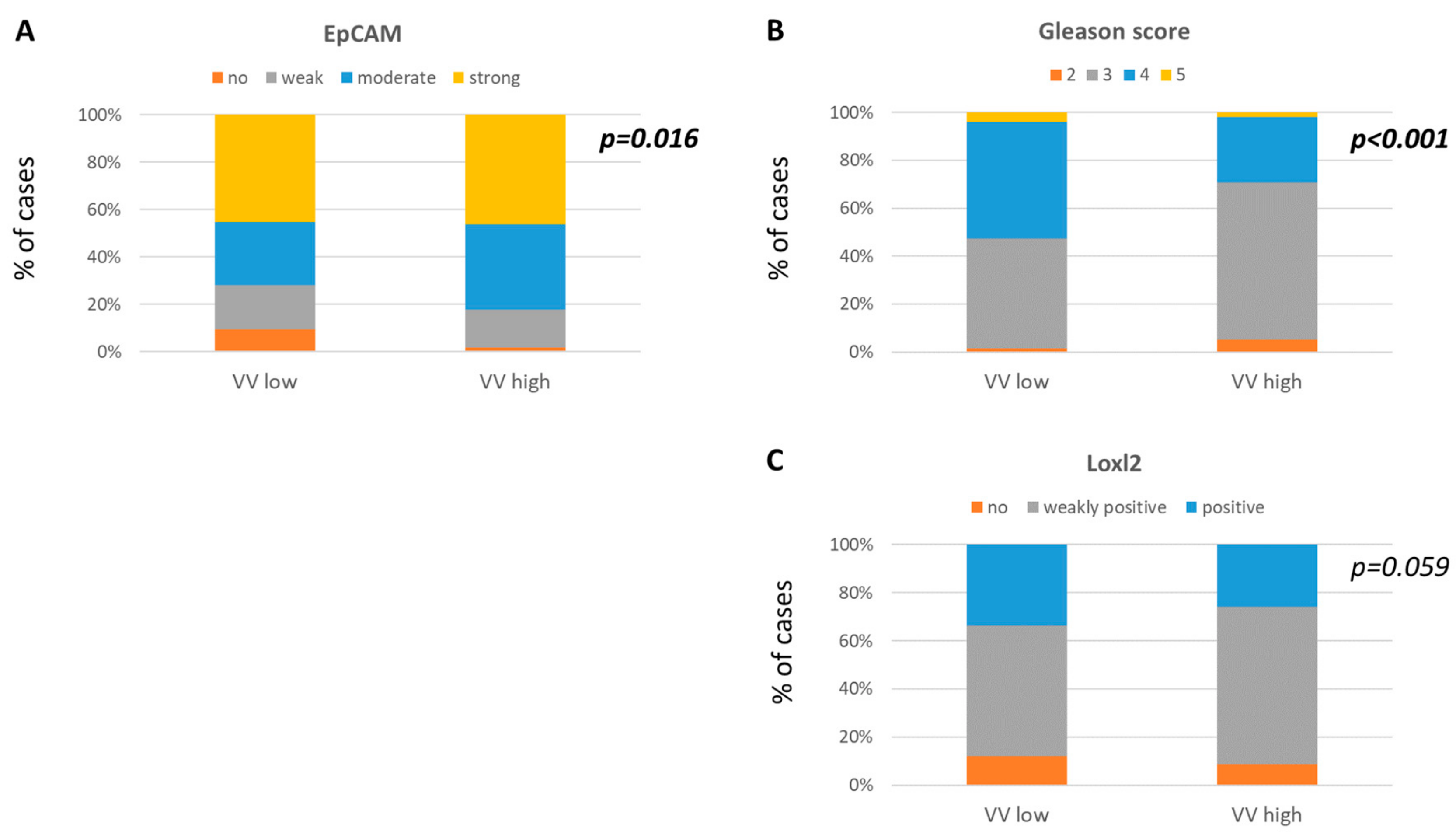
2.3. Signatures of Aggressive Molecular Phenotype in Tumors Characterized by Low Number of Vascular Vessels
3. Discussion
4. Material and Methods
4.1. Patient Cohort
4.2. Immunohistochemistry for CD34 and Podoplanin
4.3. The Evaluation of VV and LV Density
4.4. Immunohistochemistry for Tumor Cell Markers
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Pernar, C.H.; Ebot, E.M.; Wilson, K.M.; Mucci, L.A. Epidemiology of Prostate Cancer. CSH Perspect. Med. 2018. [Google Scholar] [CrossRef] [PubMed]
- Freedland, S.J.; Humphreys, E.B.; Mangold, L.A.; Eisenberger, M.; Dorey, F.J.; Walsh, P.C.; Partin, A.W. Risk of Prostate Cancer–Specific Mortality Following Biochemical Recurrence After Radical Prostatectomy. JAMA 2005, 294, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Matsuyama, K.; Chiba, Y.; Sasaki, M.; Tanaka, H.; Muraoka, R.; Tanigawa, N. Tumor Angiogenesis As a Prognostic Marker in Operable Non-Small Cell Lung Cancer. Ann. Thorac. Surg. 1998, 65, 1405–1409. [Google Scholar] [CrossRef]
- Frank, R.E.; Saclarides, T.J.; Leurgans, S.; Speziale, N.J.; Drab, E.A.; Rubin, D.B. Tumor Angiogenesis As a Predictor of Recurrence and Survival in Patients with Node-Negative Colon Cancer. Ann. Surg. 1995, 222, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Fontanini, G.; Bigini, D.; Vignati, S.; Basolo, F.; Mussi, A.; Lucchi, M.; Chine, S.; Angeletti, C.A.; Harris, A.L.; Bevilacqua, G. Microvessel Count Predicts Metastatic Disease and Survival in Non-Small Cell Lung Cancer. J. Pathol. 1995, 177, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Taverna, G.; Grizzi, F.; Colombo, P.; Graziotti, P. Is Angiogenesis a Hallmark of Prostate Cancer? Front. Oncol. 2013, 3, 15. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R.A.; West, C.M.L.; Wilks, D.P.; Logue, J.P.; Davidson, S.E.; Roberts, S.A.; Hunter, R.D. Tumour Vascularity is a Significant Prognostic Factor for Cervix Carcinoma Treated with Radiotherapy: Independence from Tumour Radiosensitivity. Br. J. Cancer 1999, 81, 354–358. [Google Scholar] [CrossRef] [PubMed]
- Ellis, L.M.; Takahashi, Y.; Fenoglio, C.J.; Cleary, K.R.; Bucana, C.D.; Evans, D.B. Vessel Counts and Vascular Endothelial Growth Factor Expression in Pancreatic Adenocarcinoma. Eur. J. Cancer 1998, 34, 337–340. [Google Scholar] [CrossRef]
- Deep, G.; Panigrahi, G.K. Hypoxia-Induced Signaling Promotes Prostate Cancer Progression: Exosomes Role as Messenger of Hypoxic Response in Tumor Microenvironment. Crit. Rev. Oncog. 2015, 20, 419–434. [Google Scholar] [CrossRef]
- Muz, B.; de la Puente, P.; Azab, F.; Azab, A.K. The Role of Hypoxia in Cancer Progression, Angiogenesis, Metastasis, and Resistance to Therapy. Hypoxia 2015, 3, 83–92. [Google Scholar] [CrossRef]
- Miyata, Y.; Sakai, H. Reconsideration of the Clinical and Histopathological Significance of Angiogenesis in Prostate Cancer: Usefulness and Limitations of Microvessel Density Measurement. Int. J. Urol. 2015, 22, 806–815. [Google Scholar] [CrossRef] [PubMed]
- Erbersdobler, A.; Isbarn, H.; Dix, K.; Steiner, I.; Schlomm, T.; Mirlacher, M.; Sauter, G.; Haese, A. Prognostic Value of Microvessel Density in Prostate Cancer: A Tissue Microarray Study. World J. Urol. 2010, 28, 687–692. [Google Scholar] [CrossRef] [PubMed]
- Miyata, Y.; Mitsunari, K.; Asai, A.; Takehara, K.; Mochizuki, Y.; Sakai, H. Pathological Significance and Prognostic Role of Microvessel Density, Evaluated Using CD31, CD34, and CD105 in Prostate Cancer Patients After Radical Prostatectomy with Neoadjuvant Therapy. Prostate 2015, 75, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zheng, D.; Zhou, T.; Song, H.; Hulsurkar, M.; Su, N.; Liu, Y.; Wang, Z.; Shao, L.; Ittmann, M.; et al. Androgen Deprivation Promotes Neuroendocrine Differentiation and Angiogenesis Through CREB-EZH2-TSP1 Pathway in Prostate Cancers. Nat. Commun. 2018, 9, 4080. [Google Scholar] [CrossRef] [PubMed]
- Bednarz, N.; Eltze, E.; Semjonow, A.; Rink, M.; Andreas, A.; Mulder, L.; Hannemann, J.; Fisch, M.; Pantel, K.; Weier, H.; et al. BRCA1 Loss Preexisting in Small Subpopulations of Prostate Cancer is Associated with Advanced Disease and Metastatic Spread to Lymph Nodes and Peripheral Blood. Clin. Cancer Res. 2010, 16, 3340–3348. [Google Scholar] [CrossRef] [PubMed]
- Nastały, P.; Filipska, M.; Morrissey, C.; Elke, E.; Semjonow, A.; Brandt, B.; Pantel, K.; Bednarz-Knoll, N. ALDH1-Positive Intratumoral Stromal Cells Indicate Differentiated Epithelial-Like Phenotype and Good Prognosis in Prostate Cancer. Transl. Res. 2019, 203, 49–56. [Google Scholar] [CrossRef]
- Omari, A.; Nastały, P.; Stoupiec, S.; Omari, A.; Nastały, P.; Stoupiec, S.; Bałabas, A.; Dąbrowska, M.; Bielińska, B.; Huss, S.; et al. Somatic Aberrations of BRCA1 Gene are Associated with ALDH1, EGFR, and Tumor Progression in Prostate Cancer. Int. J. Cancer 2019, 144, 607–614. [Google Scholar] [CrossRef]
- Smentoch, J.; Szade, J.; Żaczek, A.J.; Eltze, E.; Semjonow, A.; Brandt, B.; Bednarz-Knoll, N.; Medical University of Gdańsk, Gdańsk 80-211, Poland; Institute of Pathology Saarbruecken-Rastpfuhl, Saarbruecken 66113, Germany; University Clinic Münster, Münster 48149, Germany; University Medical Centre Schleswig-Holstein, Kiel 24105, Germany. 2019; Unpublished work.
- Hasan, J.; Byers, R.; Jayson, G.C. Intra-Tumoural Microvessel Density in Human Solid Tumours. Br. J. Cancer 2002, 86, 1566–1577. [Google Scholar] [CrossRef]
- Weidner, N. Current Pathologic Methods for Measuring Intratumoral Microvessel Density within Breast Carcinoma and Other Solid Tumors. Breast Cancer Res. Treat. 1995, 36, 169–180. [Google Scholar] [CrossRef]
- Bono, A.V.; Celato, N.; Cova, V.; Salvadore, M.; Chinetti, S.; Novario, R. Microvessel Density in Prostate Carcinoma. Prostate Cancer Prostatic Dis. 2002, 5, 123–127. [Google Scholar] [CrossRef]
- Bettencourt, M.C.; Bauer, J.J.; Sesterhenn, I.A.; Connelly, R.R.; Moul, J.W. CD34 Immunohistochemical Assessment of Angiogenesis As a Prognostic Marker for Prostate Cancer Recurrence after Radical Prostatectomy. J. Urol. 1998, 160, 459–465. [Google Scholar] [CrossRef]
- Revelos, K.; Petraki, C.; Scorilas, A.; Stefanakis, S.; Malovrouvas, D.; Alevizopoulos, N.; Kanellis, G.; Halapas, A.; Koutsilieris, M. Correlation of Androgen Receptor Status, Neuroendocrine Differentiation and Angiogenesis with Time-to-Biochemical Failure after Radical Prostatectomy in Clinically Localized Prostate Cancer. Anticancer Res. 2007, 27, 3651–3660. [Google Scholar] [PubMed]
- Ambrosio, M.R.; Rocca, B.J.; Barone, A.; Ginori, A.; Crivelli, F.; Pirtoli, L.; Del Vecchio, M.T. Lymphatic Vascularization in Prostate Adenocarcinoma: Correlation with Tumor Grade, Androgen Withdrawal and Prognosis. Anticancer Res. 2015, 35, 5595–5600. [Google Scholar]
- Foroozan, M.; Roudi, R.; Abolhasani, M.; Gheytanchi, E.; Mehrazma, M. Clinical Significance of Endothelial Cell Marker CD34 and Mast Cell Marker CD117 in Prostate Adenocarcinoma. Pathol. Res. Pract. 2017, 213, 61–618. [Google Scholar] [CrossRef] [PubMed]
- Mucci, L.A.; Powolny, A.; Giovannucci, E.; Liao, Z.; Kenfield, S.A.; Shen, R.; Stampfer, M.J.; Clinton, S.K. Prospective Study of Prostate Tumor Angiogenesis and Cancer-Specific Mortality in the Health Professionals Follow-Up Study. J. Clin. Oncol. 2009, 27, 5627–5633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matic, S.D.; Rakocevic, M.S.; Jocic, T.T.; Todorovic, M.S.; Vuckovic, L.M.; Jancic, S.A.; Knezevic, M.G. Clinical Significance of Microvessel Density and Proliferation in Prostate Cancer Core Biopsy. J. BUON. 2017, 22, 757–765. [Google Scholar] [PubMed]
- Tretiakova, M.; Antic, T.; Binder, D.; Kocherginsky, M.; Liao, C.; Taxy, J.B.; Oto, A. Microvessel Density is not Increased in Prostate Cancer: Digital Imaging of Routine Sections and Tissue Microarrays. Hum. Pathol. 2013, 44, 495–502. [Google Scholar] [CrossRef]
- Baeuerle, P.A.; Gires, O. EpCAM (CD326) Finding Its Role in Cancer. Br. J. Cancer 2007, 96, 417–423. [Google Scholar] [CrossRef]
- Yeo, C.D.; Kang, N.; Choi, S.Y.; Kim, B.N.; Park, C.K.; Kim, J.W.; Kim, Y.K.; Kim, S.J. The Role of Hypoxia on the Acquisition of Epithelial-Mesenchymal Transition and Cancer Stemness: A Possible Link to Epigenetic Regulation. Korean J. Intern. Med. 2017, 32, 589–599. [Google Scholar] [CrossRef]
- Richardsen, E.; Andersen, S.; Al-Saad, S.; Rakaee, M.; Nordby, Y.; Pedersen, M.I.; Ness, N.; Grindstad, T.; Movik, I.; Dønnem, T.; et al. Evaluation of the Proliferation Marker Ki-67 in a Large Prostatectomy Cohort. PLoS ONE 2017, 12, e0186852. [Google Scholar] [CrossRef]
- Xie, P.; Yu, H.; Wang, F.; Yan, F.; He, X. Inhibition of LOXL2 Enhances the Radiosensitivity of Castration-Resistant Prostate Cancer Cells Associated with the Reversal of the EMT Process. Biomed. Res. Int. 2019, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Wu, C.; Gao, L.; Qin, F.; Wei, Q.; Yuan, J. Lysyl Oxidase Family Members in Urological Tumorigenesis and Fibrosis. Oncotarget 2018, 9, 20156–20164. [Google Scholar] [CrossRef] [PubMed]
- Higgins, D.F.; Kimura, K.; Bernhardt, W.M.; Shrimanker, N.; Akai, Y.; Hohenstein, B.; Saito, Y.; Johnson, R.S.; Kretzler, M.; Cohen, C.D.; et al. Hypoxia Promotes Fibrogenesis in Vivo via HIF-1 Stimulation of Epithelial-to-Mesenchymal Transition. J. Clin. Invest. 2007, 117, 3810–3820. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Zhao, X.; Zhu, D.; Liu, T.; Liang, X.; Liu, F.; Zhang, Y.; Dong, X.; Sun, B. HIF-1α Promoted Vasculogenic Mimicry Formation in Hepatocellular Carcinoma through LOXL2 Up-Regulation in Hypoxic Tumor Microenvironment. J. Exp. Clin. Cancer Res. 2017, 36, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Park, P.-G.; Jo, S.J.; Kim, M.J.; Kim, H.J.; Lee, J.H.; Park, C.K.; Kim, H.; Lee, K.Y.; Kim, H.; Park, J.H.; et al. Role of LOXL2 in the Epithelial-Mesenchymal Transition and Colorectal Cancer Metastasis. Oncotarget 2017, 8, 80325–80335. [Google Scholar] [CrossRef] [PubMed]
- Cuevas, E.P.; Eraso, P.; Mazón, M.J.; Santos, V.; Moreno-Bueno, G.; Cano, A.; Portillo, F. LOXL2 Drives Epithelial-Mesenchymal Transition via Activation of IRE1-XBP1 Signalling Pathway. Sci. Rep. 2017, 7, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Heßling, S. Prognostische Relevanz in Bezug auf die Expression von LOXL2 bei den verschiedenen Manifestationsformen des Prostatakarzinoms (Prognostic relevance with respect to the expression of LOXL2 in the different manifestations of prostate cancer). Ph.D. Thesis, University of Münster, Münster, Germany, 2007. [Google Scholar]
- Schmidt, H.; Semjonow, A.; Csiszar, K.; Korsching, E.; Brandt, B.; Eltze, E. Mapping Eines Deletionsintervalls auf 8p21-22 beim Prostatakarzionom mittels Gendosis-PCR (Mapping of a Deletion Interval on 8p21-22 in the Prostate Carcinoma Using Gene-Dose PCR). Verh. Dtsch. Ges. Pathol. 2007, 91, 302–307. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| 5 Years | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| p-Value | HR | 95% CI | p-Value | HR | 95% Cl | |
| T3–4 vs. T1–2 | <0.001 | 3.734 | 2.068–6.742 | <0.001 | 3.337 | 1.815–6.136 |
| N1–2 vs. N0 | 0.260 | 1.691 | 0.678–4.251 | - | - | - |
| Preoperative PSA ≥ 4 ng/mL vs. < 4 ng/mL | 0.076 | 5.971 | 0.829–43.030 | - | - | - |
| Age (≥ 64 vs. < 64) | 0.515 | 1.174 | 0.724–1.903 | - | - | - |
| Gleason scale ≥ 7 vs. < 7 | 0.010 | 2.796 | 1.277–6.120 | 0.190 | 1.716 | 0.765–3.849 |
| minVVlow vs. minVVhigh | 0.031 | 0.584 | 0.358–0.951 | 0.046 | 0.607 | 0.372–0.991 |
| Clinical and Pathological Parameters | Status | n | % |
|---|---|---|---|
| Age (years) | <median (64) | 208 | 52.00 |
| ≥median (64) | 192 | 48.00 | |
| total | 400 | ||
| T status | T2 | 3 | 0.80 |
| T3a | 184 | 46.10 | |
| T3b | 190 | 47.60 | |
| T4 | 22 | 5.50 | |
| total | 399 | ||
| N status | N0 | 367 | 94.60 |
| N1 | 21 | 5.40 | |
| total | 388 | ||
| Gleason score sum | <7 | 102 | 25.50 |
| 7 | 253 | 63.20 | |
| >7 | 45 | 11.30 | |
| total | 400 | ||
| Preoperative PSA | <4 ng/mL | 42 | 10.80 |
| 4–10 ng/mL | 171 | 44.00 | |
| 10–20 ng/mL | 118 | 30.30 | |
| >20 ng/mL | 58 | 14.90 | |
| total | 389 | ||
| d’Amico scale | low risk | 15 | 3.90 |
| intermediate low risk | 91 | 23.50 | |
| intermediate high risk | 246 | 63.60 | |
| high risk | 35 | 9.00 | |
| total | 387 | ||
| Preoperative ADT | neg | 331 | 82.80 |
| pos | 69 | 17.30 | |
| total | 400 | ||
| Biochemical recurrence | no | 293 | 73.60 |
| yes | 105 | 26.40 | |
| total | 398 | ||
| Tumor focality | monofocal | 69 | 17.30 |
| multifocal | 329 | 82.70 | |
| total | 398 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smentoch, J.; Szade, J.; Żaczek, A.J.; Eltze, E.; Semjonow, A.; Brandt, B.; Bednarz-Knoll, N. Low Numbers of Vascular Vessels Correlate to Progression in Hormone-Naïve Prostate Carcinomas Undergoing Radical Prostatectomy. Cancers 2019, 11, 1356. https://doi.org/10.3390/cancers11091356
Smentoch J, Szade J, Żaczek AJ, Eltze E, Semjonow A, Brandt B, Bednarz-Knoll N. Low Numbers of Vascular Vessels Correlate to Progression in Hormone-Naïve Prostate Carcinomas Undergoing Radical Prostatectomy. Cancers. 2019; 11(9):1356. https://doi.org/10.3390/cancers11091356
Chicago/Turabian StyleSmentoch, Julia, Jolanta Szade, Anna J. Żaczek, Elke Eltze, Axel Semjonow, Burkhard Brandt, and Natalia Bednarz-Knoll. 2019. "Low Numbers of Vascular Vessels Correlate to Progression in Hormone-Naïve Prostate Carcinomas Undergoing Radical Prostatectomy" Cancers 11, no. 9: 1356. https://doi.org/10.3390/cancers11091356
APA StyleSmentoch, J., Szade, J., Żaczek, A. J., Eltze, E., Semjonow, A., Brandt, B., & Bednarz-Knoll, N. (2019). Low Numbers of Vascular Vessels Correlate to Progression in Hormone-Naïve Prostate Carcinomas Undergoing Radical Prostatectomy. Cancers, 11(9), 1356. https://doi.org/10.3390/cancers11091356