Beyond Traditional Morphological Characterization of Lung Neuroendocrine Neoplasms: In Silico Study of Next-Generation Sequencing Mutations Analysis across the Four World Health Organization Defined Groups

 , , , , ,
, , , , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Paper and Datasets Selection
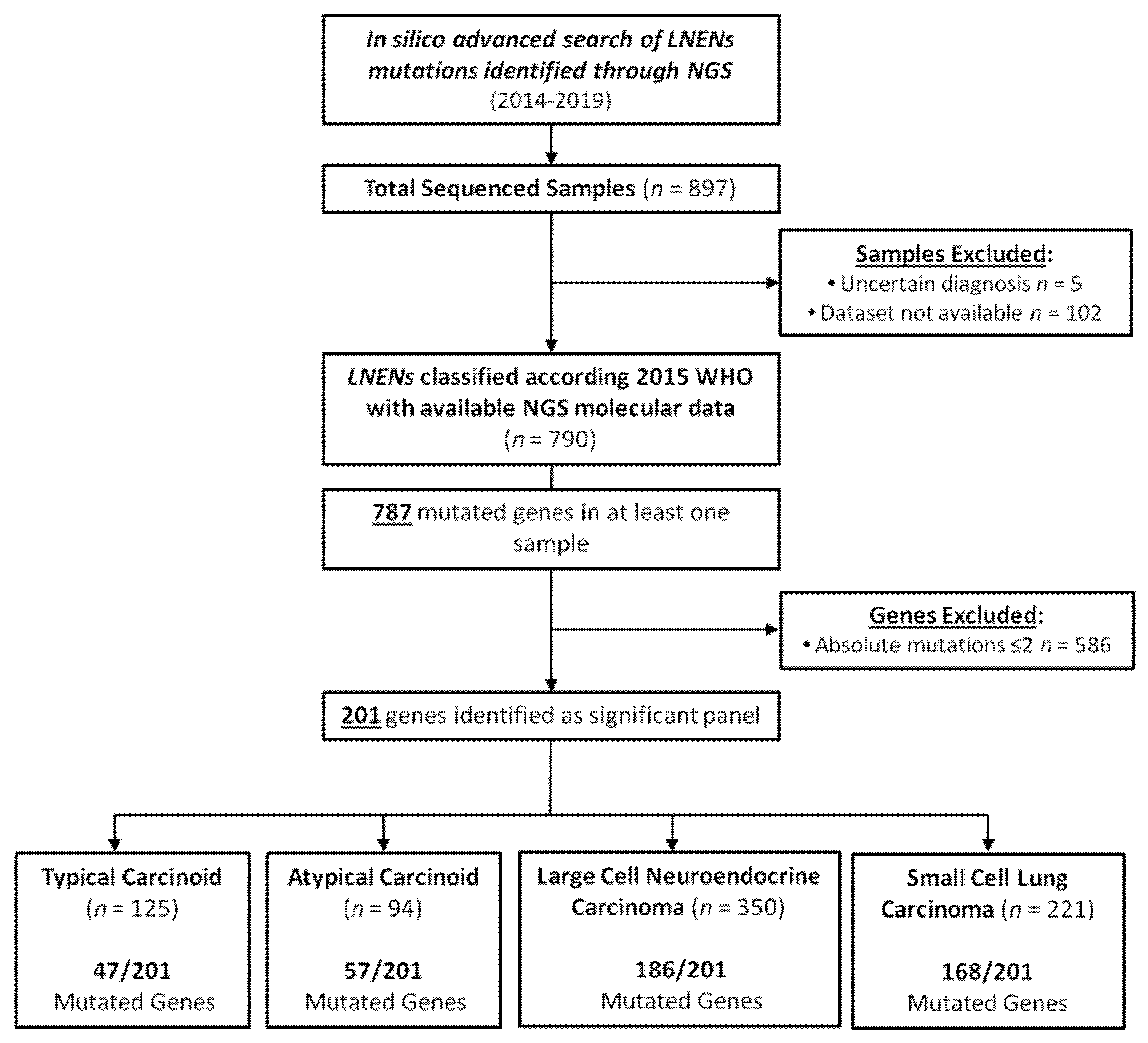
2.3. Samples Selection
2.4. Genes Selection and Dataset Creation
2.5. Mutation Rate
2.6. Statistical Analysis
3. Results
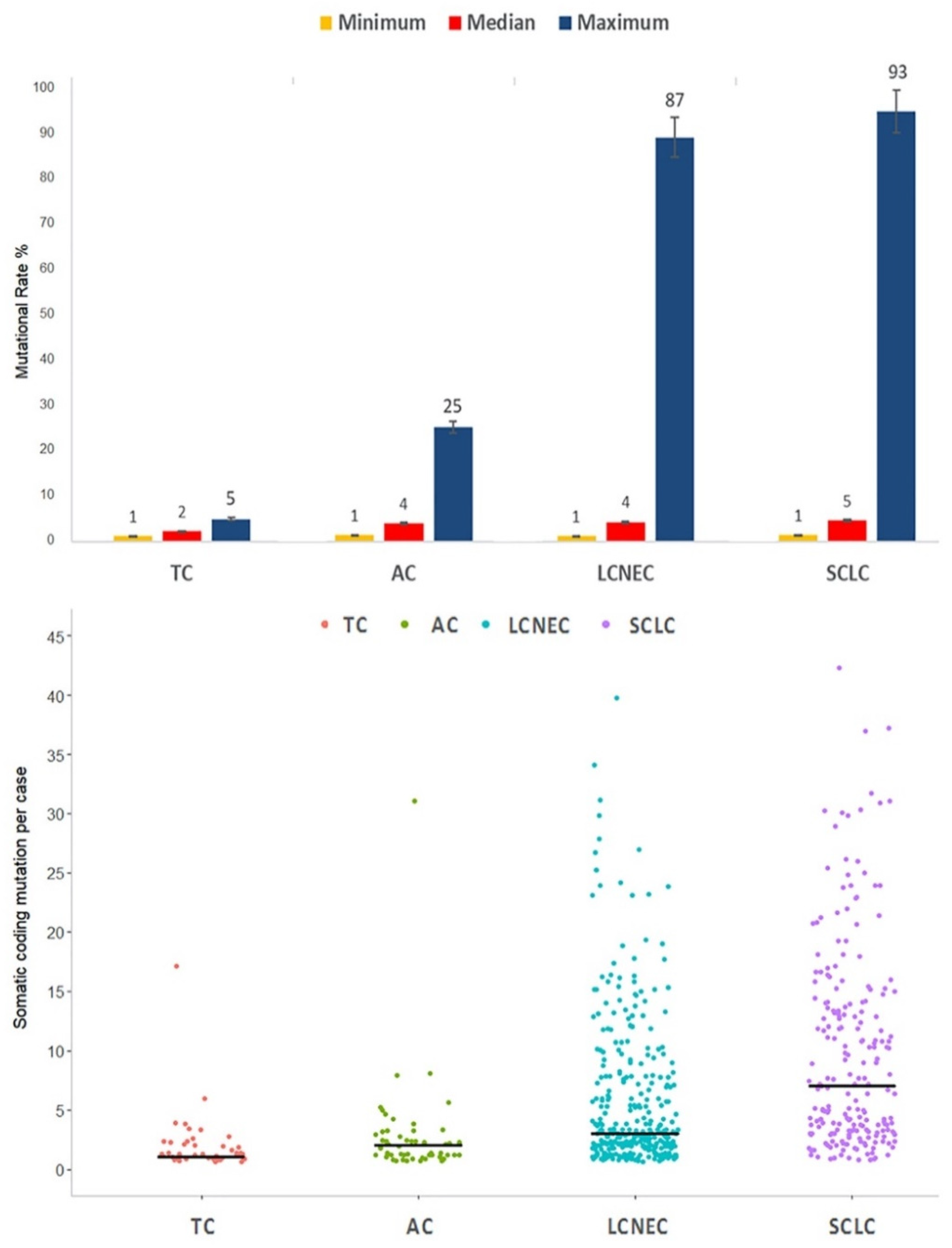
3.1. Number of Samples, Genes and Mutation Rate across WHO Histological Variants
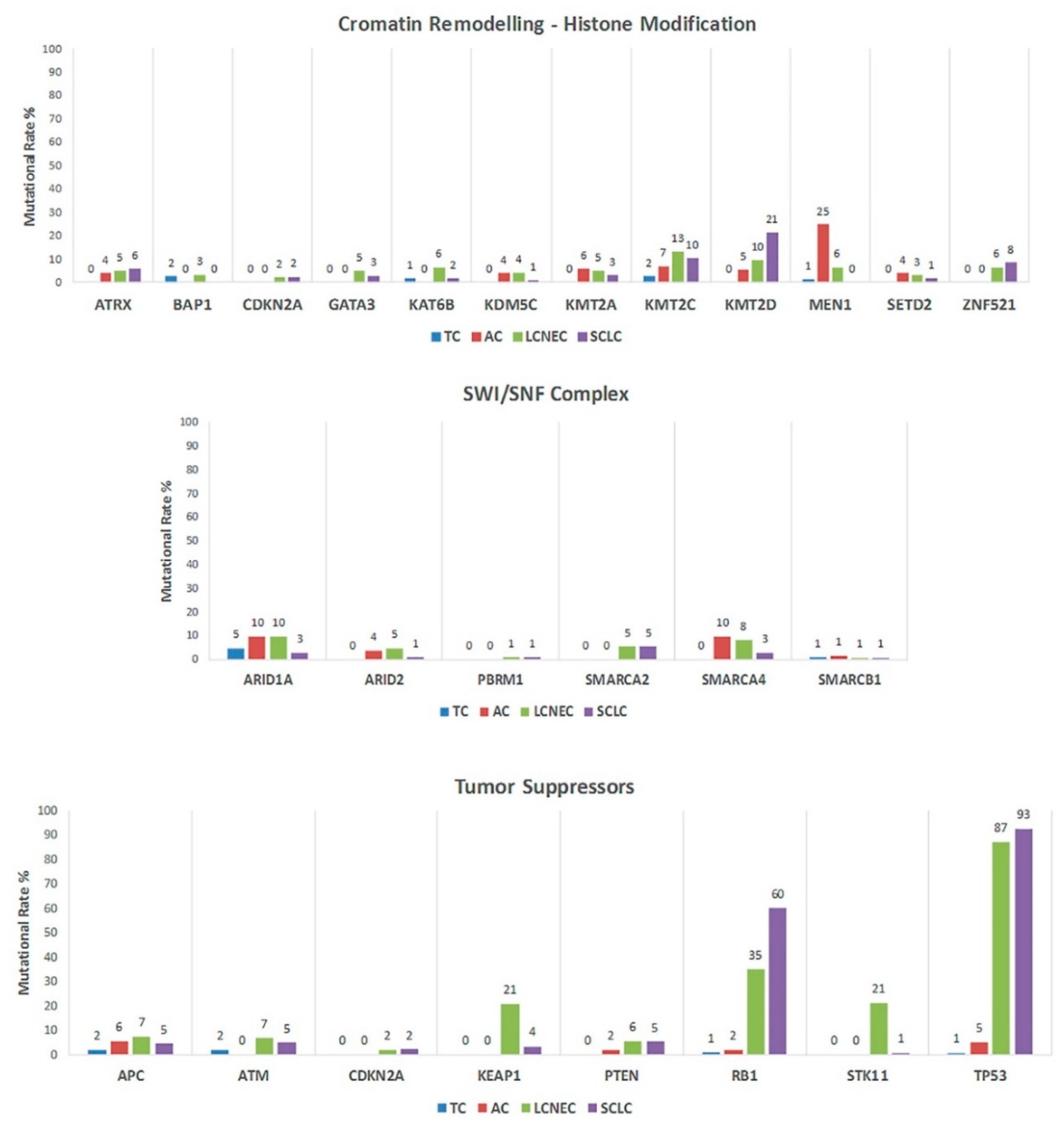
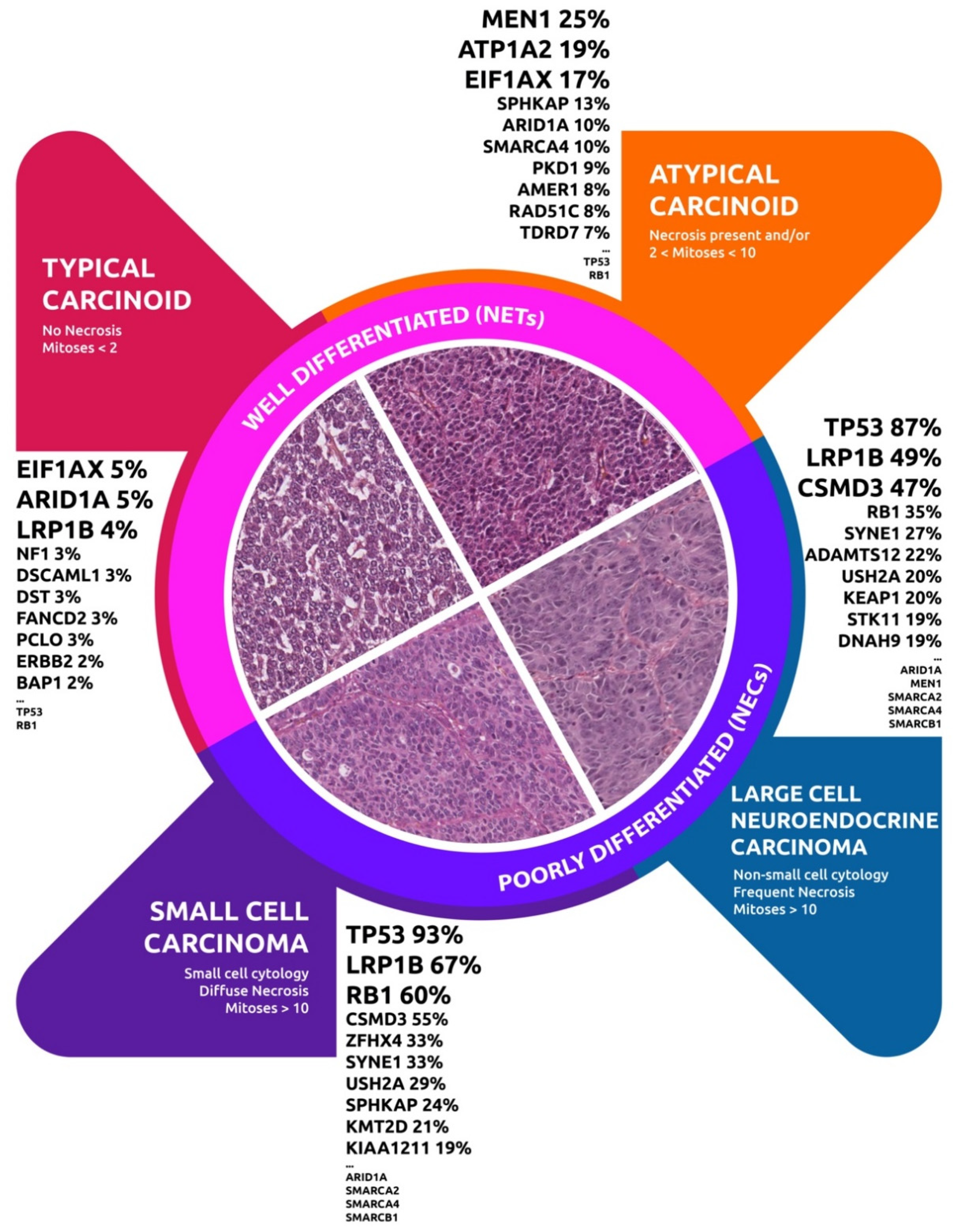
3.2. Altered Genes and Pathways in NETs
3.3. Altered Genes and Pathways in NEC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Travis, W.D.; Brambilla, E.; Burke, A.; Marx, A.; Nicholson, A.G. Who Classification of Tumours of the Lung, Pleura, Thymus and Heart; International Agency for Research on Cancer; International Academy of Pathology: Lyon, France, 2015. [Google Scholar]
- Travis, W.D. Advances in neuroendocrine lung tumors. Ann. Oncol. 2010, 21, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Petursdottir, A.; Sigurdardottir, J.; Fridriksson, B.M.; Johnsen, A.; Isaksson, H.J.; Hardardottir, H.; Jonsson, S.; Gudbjartsson, T. Pulmonary carcinoid tumours: Incidence, histology, and surgical outcome. A population-based study. Gen. Thorac. Cardiovasc. Surg. 2020, 68, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Derks, J.L.; Hendriks, L.E.; Buikhuisen, W.A.; Groen, H.J.M.; Thunnissen, E.; van Suylen, R.-J.; Houben, R.; Damhuis, R.A.; Speel, E.J.M.; Dingemans, A.-M.C. Clinical features of large cell neuroendocrine carcinoma: A population-based overview. Eur. Respir. J. 2016, 47, 615–624. [Google Scholar] [CrossRef] [Green Version]
- Van Meerbeeck, J.P.; Fennell, D.A.; De Ruysscher, D.K. Small-cell lung cancer. Lancet 2011, 378, 1741–1755. [Google Scholar] [CrossRef]
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the incidence, prevalence, and survival outcomes in patients with neuroendocrine tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, B.I.; Kidd, M.; Chan, A.; Malfertheiner, M.V.; Modlin, I.M. Bronchopulmonary neuroendocrine tumors. Cancer 2008, 113, 5–21. [Google Scholar]
- Oronsky, B.; Ma, P.C.; Morgensztern, D.; Carter, C.A. Nothing But NET: A Review of Neuroendocrine Tumors and Carcinomas. Neoplasia 2017, 19, 991–1002. [Google Scholar] [CrossRef]
- Rindi, G.; Klimstra, D.S.; Abedi-Ardekani, B.; Asa, S.L.; Bosman, F.T.; Brambilla, E.; Busam, K.J.; de Krijger, R.R.; Dietel, M.; El-Naggar, A.K.; et al. A common classification framework for neuroendocrine neoplasms: An International Agency for Research on Cancer (IARC) and World Health Organization (WHO) expert consensus proposal. Mod. Pathol. 2018, 31, 1770–1786. [Google Scholar] [CrossRef]
- Simbolo, M.; Mafficini, A.; Sikora, K.O.; Fassan, M.; Barbi, S.; Corbo, V.; Mastracci, L.; Rusev, B.; Grillo, F.; Vicentini, C.; et al. Lung neuroendocrine tumours: Deep sequencing of the four World Health Organization histotypes reveals chromatin-remodelling genes as major players and a prognostic role for TERT, RB1, MEN1 and KMT2D. J. Pathol. 2017, 241, 488–500. [Google Scholar] [CrossRef]
- Fernandez-Cuesta, L.; Peifer, M.; Lu, X.; Sun, R.; Ozretić, L.; Seidel, D.; Zander, T.; Leenders, F.; George, J.; Müller, C.; et al. Frequent mutations in chromatin-remodelling genes in pulmonary carcinoids. Nat. Commun. 2014, 5, 3518. [Google Scholar] [CrossRef]
- George, J.; Walter, V.; Peifer, M.; Alexandrov, L.B.; Seidel, D.; Leenders, F.; Maas, L.; Müller, C.; Dahmen, I.; Delhomme, T.M.; et al. Integrative genomic profiling of large-cell neuroendocrine carcinomas reveals distinct subtypes of high-grade neuroendocrine lung tumors. Nat. Commun. 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- George, J.; Lim, J.S.; Jang, S.J.; Cun, Y.; Ozretić, L.; Kong, G.; Leenders, F.; Lu, X.; Fernández-Cuesta, L.; Bosco, G. Comprehensive genomic profiles of small cell lung cancer. Nature 2015, 524, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Swarts, D.R.A.; Ramaekers, F.C.S.; Speel, E.J.M. Molecular and cellular biology of neuroendocrine lung tumors: Evidence for separate biological entities. Biochim. Biophys. Acta 2012, 1826, 255–271. [Google Scholar] [CrossRef] [PubMed]
- Caplin, M.E.; Baudin, E.; Ferolla, P.; Filosso, P.; Garcia-Yuste, M.; Lim, E.; Oberg, K.; Pelosi, G.; Perren, A.; Rossi, R.E.; et al. Pulmonary neuroendocrine (carcinoid) tumors: European Neuroendocrine Tumor Society expert consensus and recommendations for best practice for typical and atypical pulmonary carcinoids. Ann. Oncol. 2015, 26, 1604–1620. [Google Scholar] [CrossRef] [PubMed]
- Fasano, M.; Della Corte, C.M.; Papaccio, F.; Ciardiello, F.; Morgillo, F. Pulmonary large-cell neuroendocrine carcinoma: From epidemiology to therapy. J. Thorac. Oncol. 2015, 10, 1133–1141. [Google Scholar] [CrossRef] [Green Version]
- Rossi, A.; Tay, R.; Chiramel, J.; Prelaj, A.; Califano, R. Current and future therapeutic approaches for the treatment of small cell lung cancer. Expert Rev. Anticancer Ther. 2018, 18, 473–486. [Google Scholar] [CrossRef]
- Hendifar, A.E.; Marchevsky, A.M.; Tuli, R. Neuroendocrine Tumors of the Lung: Current Challenges and Advances in the Diagnosis and Management of Well-Differentiated Disease. J. Thorac. Oncol. 2017, 12, 425–436. [Google Scholar] [CrossRef] [Green Version]
- Pusceddu, S.; Lo Russo, G.; Macerelli, M.; Proto, C.; Vitali, M.; Signorelli, D.; Ganzinelli, M.; Scanagatta, P.; Duranti, L.; Trama, A.; et al. Diagnosis and management of typical and atypical lung carcinoids. Crit. Rev. Oncol. Hematol. 2016, 100, 167–176. [Google Scholar] [CrossRef]
- Lo Russo, G.; Pusceddu, S.; Proto, C.; Macerelli, M.; Signorelli, D.; Vitali, M.; Ganzinelli, M.; Gallucci, R.; Zilembo, N.; Platania, M.; et al. Treatment of lung large cell neuroendocrine carcinoma. Tumour Biol. 2016, 37, 7047–7057. [Google Scholar] [CrossRef]
- Lo Russo, G.; Pusceddu, S.; Prinzi, N.; Imbimbo, M.; Proto, C.; Signorelli, D.; Vitali, M.; Ganzinelli, M.; Maccauro, M.; Buzzoni, R.; et al. Peptide receptor radionuclide therapy: Focus on bronchial neuroendocrine tumors. Tumour Biol. 2016, 37, 12991–13003. [Google Scholar] [CrossRef]
- Lo Russo, G.; Macerelli, M.; Platania, M.; Zilembo, N.; Vitali, M.; Signorelli, D.; Proto, C.; Ganzinelli, M.; Gallucci, R.; Agustoni, F.; et al. Small-Cell Lung Cancer: Clinical Management and Unmet Needs New Perspectives for an Old Problem. Curr. Drug Targets 2017, 18, 341–362. [Google Scholar] [CrossRef] [PubMed]
- Rekhtman, N.; Pietanza, M.C.; Hellmann, M.D.; Naidoo, J.; Arora, A.; Won, H.; Halpenny, D.F.; Wang, H.; Tian, S.K.; Litvak, A.M.; et al. Next-generation sequencing of pulmonary large cell neuroendocrine carcinoma reveals small cell carcinoma-like and non-small cell carcinoma-like subsets. Clin. Cancer Res. 2016, 22, 3618–3629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simbolo, M.; Barbi, S.; Fassan, M.; Mafficini, A.; Ali, G.; Vicentini, C.; Sperandio, N.; Corbo, V.; Rusev, B.; Mastracci, L.; et al. Gene expression profiling of lung atypical carcinoids and large cell neuroendocrine carcinomas identifies three transcriptomic subtypes with specific genomic alterations. J. Thorac. Oncol. 2019, 14, 1651–1661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karlsson, A.; Brunnström, H.; Micke, P.; Botling, J.; Jönsson, M.; Reuterswärd, C. Gene Expression Profiling of Large Cell Lung Cancer Links Transcriptional Phenotypes to the New Histological WHO 2015 Classi fi cation. J. Thorac. Oncol. 2017, 12, 1257–1267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swarts, D.R.A.; Scarpa, A.; Corbo, V.; Criekinge, W.V.; Engeland, M.V.; Gatti, G.; Henfling, M.E.R.; Papotti, M.; Perren, A.; Ramaekers, F.C.S.; et al. MEN1 Gene Mutation and Reduced Expression Are Associated With Poor Prognosis in Pulmonary. J. Clin. Endocrinol. Metab. 2014, 99, 374–378. [Google Scholar] [CrossRef] [Green Version]
- Derks, J.L.; Leblay, N.; Thunnissen, E.; van Suylen, R.J.; den Bakker, M.; Groen, H.J.M.; Smit, E.F.; Damhuis, R.; van den Broek, E.C.; Charbrier, A.; et al. Molecular Subtypes of Pulmonary Large-cell Neuroendocrine Carcinoma Predict Chemotherapy Treatment Outcome. Clin. Cancer Res. 2018, 24, 33–42. [Google Scholar] [CrossRef] [Green Version]
- Cerami, E.; Gao, J.; Dogrusoz, U.; Gross, B.E.; Sumer, S.O.; Aksoy, B.A.; Jacobsen, A.; Byrne, C.J.; Heuer, M.L.; Larsson, E.; et al. The cBio cancer genomics portal: An open platform for exploring multidimensional cancer genomics data. Cancer Discov. 2012, 2, 401–404. [Google Scholar] [CrossRef] [Green Version]
- Armengol, G.; Sarhadi, V.K.; Rönty, M.; Tikkanen, M.; Knuuttila, A.; Knuutila, S. Driver Gene Mutations of Non-Small-Cell Lung Cancer are Rare in Primary Carcinoids of the Lung: NGS Study by Ion Torrent. Lung 2015, 193, 303–308. [Google Scholar] [CrossRef]
- Karlsson, A.; Brunnström, H.; Lindquist, K.E.; Jirström, K.; Jönsson, M.; Rosengren, F.; Reuterswärd, C.; Cirenajwis, H.; Borg, Å.; Jönsson, P.; et al. Mutational and gene fusion analyses of primary large cell and large cell neuroendocrine lung cancer. Oncotarget 2015, 6, 22028–22037. [Google Scholar] [CrossRef] [Green Version]
- Vollbrecht, C.; Werner, R.; Walter, R.F.H.; Christoph, D.C.; Heukamp, L.C.; Peifer, M.; Hirsch, B.; Burbat, L.; Mairinger, T.; Schmid, K.W.; et al. Mutational analysis of pulmonary tumours with neuroendocrine features using targeted massive parallel sequencing: A comparison of a neglected tumour group. Br. J. Cancer 2015, 113, 1704–1711. [Google Scholar] [CrossRef] [Green Version]
- Miyoshi, T.; Umemura, S.; Matsumura, Y.; Mimaki, S.; Tada, S.; Makinoshima, H.; Ishii, G.; Udagawa, H.; Matsumoto, S.; Yoh, K.; et al. Genomic profiling of large-cell neuroendocrine carcinoma of the lung. Clin. Cancer Res. 2017, 23, 757–765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asiedu, M.K.; Thomas, C.F.; Dong, J.; Schulte, S.C.; Khadka, P.; Sun, Z.; Kosari, F.; Jen, J.; Molina, J.; Vasmatzis, G.; et al. Pathways impacted by genomic alterations in pulmonary carcinoid tumors. Clin. Cancer Res. 2018, 24, 1691–1704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laddha, S.V.; da Silva, E.M.; Robzyk, K.; Untch, B.R.; Ke, H.; Rekhtman, N.; Poirier, J.T.; Travis, W.D.; Tang, L.H.; Chan, C.S. Integrative Genomic Characterization Identifies Molecular Subtypes of Lung Carcinoids. Cancer Res. 2019, 79, 4339–4347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Subramanian, A.; Tamayo, P.; Mootha, V.K.; Mukherjee, S.; Ebert, B.L.; Gillette, M.A.; Paulovich, A.; Pomeroy, S.L.; Golub, T.R.; Lander, E.S.; et al. Gene set enrichment analysis: A knowledge-based approach for interpreting genome-wide expression profiles. Proc. Natl. Acad. Sci. USA 2005, 102, 15545–15550. [Google Scholar] [CrossRef] [Green Version]
- Schumacher, T.N.; Schreiber, R.D. Neoantigens in cancer immunotherapy. Science 2015, 348, 69–74. [Google Scholar] [CrossRef] [Green Version]
- Nebot-Bral, L.; Brandao, D.; Verlingue, L.; Rouleau, E.; Caron, O.; Despras, E.; El-Dakdouki, Y.; Champiat, S.; Aoufouchi, S.; Leary, A.; et al. Hypermutated tumours in the era of immunotherapy: The paradigm of personalised medicine. Eur. J. Cancer 2017, 84, 290–303. [Google Scholar] [CrossRef]
- Strosberg, J.; Mizuno, N.; Doi, T.; Grande, E.; Delord, J.-P.; Shapira-Frommer, R.; Bergsland, E.; Shah, M.; Fakih, M.; Takahashi, S.; et al. Efficacy and Safety of Pembrolizumab in Previously Treated Advanced Neuroendocrine Tumors: Results From the Phase II KEYNOTE-158 Study. Clin. Cancer Res. 2020, 26, 2124–2130. [Google Scholar] [CrossRef]
- Yao, J.C.; Strosberg, J.; Fazio, N.; Pavel, M.E.; Ruszniewski, P.; Bergsland, E.; Li, D.; Tafuto, S.; Raj, N.; Campana, D. 1308O Activity & safety of spartalizumab (PDR001) in patients (pts) with advanced neuroendocrine tumors (NET) of pancreatic (Pan), gastrointestinal (GI), or thoracic (T) origin, & gastroenteropancreatic neuroendocrine carcinoma (GEP NEC) who have progress. Ann. Oncol. 2018, 29 (Suppl. 8), VIII467–VIII468. [Google Scholar]
- Remon, J.; Passiglia, F.; Ahn, M.-J.; Barlesi, F.; Forde, P.M.; Garon, E.B.; Gettinger, S.; Goldberg, S.B.; Herbst, R.S.; Horn, L.; et al. Immune Checkpoint Inhibitors in Thoracic Malignancies: Review of the Existing Evidence by an IASLC Expert Panel and Recommendations. J. Thorac. Oncol. 2020, 15, 914–947. [Google Scholar] [CrossRef]
- Sherman, S.; Rotem, O.; Shochat, T.; Zer, A.; Moore, A.; Dudnik, E. Efficacy of immune check-point inhibitors (ICPi) in large cell neuroendocrine tumors of lung (LCNEC). Lung Cancer 2020, 143, 40–46. [Google Scholar] [CrossRef]
- Goodrich, D.W. The retinoblastoma tumor-suppressor gene, the exception that proves the rule. Oncogene 2006, 25, 5233–5243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Leary, B.; Finn, R.S.; Turner, N.C. Treating cancer with selective CDK4/6 inhibitors. Nat. Rev. Clin. Oncol. 2016, 13, 417–430. [Google Scholar] [CrossRef] [PubMed]
- Polley, E.; Kunkel, M.; Evans, D.; Silvers, T.; Delosh, R.; Laudeman, J.; Ogle, C.; Reinhart, R.; Selby, M.; Connelly, J.; et al. Small Cell Lung Cancer Screen of Oncology Drugs, Investigational Agents, and Gene and microRNA Expression. J. Natl. Cancer Inst. 2016, 108, djw122. [Google Scholar] [CrossRef] [Green Version]
- Barretina, J.; Caponigro, G.; Stransky, N.; Venkatesan, K.; Margolin, A.A.; Kim, S.; Wilson, C.J.; Lehár, J.; Kryukov, G.V.; Sonkin, D.; et al. The Cancer Cell Line Encyclopedia enables predictive modelling of anticancer drug sensitivity. Nature 2012, 483, 603–607. [Google Scholar] [CrossRef] [PubMed]
- Sazonova, O.; Manem, V.; Orain, M.; Khoshkrood-Mansoori, B.; Gaudreault, N.; Desmeules, P.; Bossé, Y.; Joubert, P. Transcriptomic data helps refining classification of pulmonary carcinoid tumors with increased mitotic counts. Mod. Pathol. 2020, 33, 1712–1721. [Google Scholar] [CrossRef] [PubMed]
- Milione, M.; Maisonneuve, P.; Grillo, F.; Mangogna, A.; Centonze, G.; Prinzi, N.; Pusceddu, S.; Garzone, G.; Cattaneo, L.; Busico, A.; et al. Ki-67 index of 55% distinguishes two groups of bronchopulmonary pure and composite large cell neuroendocrine carcinomas with distinct prognosis. Neuroendocrinology 2020. [Google Scholar] [CrossRef] [PubMed]
- Alcala, N.; Leblay, N.; Gabriel, A.A.G.; Mangiante, L.; Hervas, D.; Giffon, T.; Sertier, A.S.; Ferrari, A.; Derks, J.; Ghantous, A. Integrative and comparative genomic analyses identify clinically relevant pulmonary carcinoid groups and unveil the supra-carcinoids. Nat. Commun. 2019, 10, 1–21. [Google Scholar] [CrossRef]
- Shen, J.; Ju, Z.; Zhao, W.; Wang, L.; Peng, Y.; Ge, Z.; Nagel, Z.D.; Zou, J.; Wang, C.; Kapoor, P.; et al. ARID1A deficiency promotes mutability and potentiates therapeutic antitumor immunity unleashed by immune checkpoint blockade. Nat. Med. 2018, 24, 556–562. [Google Scholar] [CrossRef]
- Wu, J.N.; Roberts, C.W.M. ARID1A mutations in cancer: Another epigenetic tumor suppressor? Cancer Discov. 2013, 3, 35–43. [Google Scholar] [CrossRef] [Green Version]
- Williamson, C.T.; Miller, R.; Pemberton, H.N.; Jones, S.E.; Campbell, J.; Konde, A.; Badham, N.; Rafiq, R.; Brough, R.; Gulati, A.; et al. ATR inhibitors as a synthetic lethal therapy for tumours deficient in ARID1A. Nat. Commun. 2016, 7, 13837. [Google Scholar] [CrossRef]
- Bitler, B.G.; Aird, K.M.; Garipov, A.; Li, H.; Amatangelo, M.; Kossenkov, A.V.; Schultz, D.C.; Liu, Q.; Shih, I.-M.; Conejo-Garcia, J.R.; et al. Synthetic lethality by targeting EZH2 methyltransferase activity in ARID1A-mutated cancers. Nat. Med. 2015, 21, 231–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samartzis, E.P.; Gutsche, K.; Dedes, K.J.; Fink, D.; Stucki, M.; Imesch, P. Loss of ARID1A expression sensitizes cancer cells to PI3K- and AKT-inhibition. Oncotarget 2014, 5, 5295–5303. [Google Scholar] [CrossRef] [PubMed]
- Okamura, R.; Kato, S.; Lee, S.; Jimenez, R.E.; Sicklick, J.K.; Kurzrock, R. ARID1A alterations function as a biomarker for longer progression-free survival after anti-PD-1/PD-L1 immunotherapy. J. Immunother. Cancer 2020, 8, e000438. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Author | Sequenced Samples (n) | Sample Histotype (n) | WGS (n) | WES (n) | t-NGS (n) | Genes Analyzed | Sequencing | Selected Samples (n) |
|---|---|---|---|---|---|---|---|---|---|
| 2014 | Fernandez-Cuesta et al. [11] | 44 | TC (34) | TC (24) | TC (10) | 0 | All | WGS and WES | 34 TC 5 AC |
| AC (5) | AC (1) | AC (4) | |||||||
| CA NAS (5) | CA NAS (4) | CA NAS (1) | |||||||
| 2015 | Armengol et al. [29] | 25 | TC (21) | 0 | 0 | TC (21) | 22 (t-NGS) | Ion AmpliSeq Colon and Lung Cancer Research Panel v2 (Thermofisher) | TC (21) |
| AC (4) | AC (4) | AC (4) | |||||||
| 2015 | Karlsson et al. [30] | 32 | LCNEC (32) | 0 | 0 | LCNEC (32) | 26 (t-NGS) | Illumina TruSight Tumor 26-gene next-generation sequencing (NGS) panel (Illumina). LCNEC cases were screened for retinoblastoma 1 gene (RB1) mutations by using a custom-designed bidirectional NGS panel (Illumina). | LCNEC (32) |
| 2015 | Vollbrecht et al. [31] | 70 | TC (17) | 0 | 0 | TC (17) | 48 (t-NGS) | TruSeq Amplicon–Cancer Panel (Illumina, San Diego, CA, USA) | TC (17) |
| AC (17) | AC (17) | AC (17) | |||||||
| LCNEC (19) | LCNEC (19) | LCNEC (19) | |||||||
| SCLC (17) | SCLC (17) | SCLC (17) | |||||||
| 2015 | George et al. [13] | 110 | SCLC (110) | SCLC (110) | 0 | 0 | All | WGS | 110 SCLC |
| 2016 | Rekhtman et al. [23] | 45 | LCNEC (45) | 0 | 0 | LCNEC (45) | 241 (t-NGS) | Memorial Sloan Kettering-Integrated Mutation Profiling of Actionable Cancer Targets (MSK-IMPACT) platform | 45 LCNEC |
| 2017 | Miyoshi et al. [32] | 168 | LCNEC (78) | 0 | 0 | LCNEC (78) | 244 (t-NGS) | Custom target-capturing panel (SureSelect XT custom 0.5–2.9 Mb, Agilent Technologies) containing all the coding exons of 244 genes | LCNEC (78) |
| SCLC (90) | SCLC (90) | SCLC (90) | |||||||
| 2017 | Simbolo et al. [10] | 148 | TC (53) | 0 | TC (10) | TC (43) | All (WES) | WES and Ion AmpliSeq Comprehensive Cancer Panel (ThermoFisher) | TC (23) |
| AC (35) | AC (4) | AC (31) | 418 (HCTS) * | AC (14) | |||||
| LCNEC (27) | LCNEC (3) | LCNEC (24) | 88 (t-NGS) | LCNEC (5) | |||||
| SCLC (33) | SCLC (3) | SCLC (30) | SCLC (4) | ||||||
| 2018 | Derks et al. [27] | 79 | LCNEC (79) | 0 | 0 | LCNEC (79) | 4 (t-NGS) | Qiagen GeneRead DNAseq Custom V2 Builder (TP53, RB1, STK11, and KEAP1) | LCNEC (79) |
| 2018 | Asiedu et al. [33] | 20 | TC (14) | TC (3) | TC (14) | 0 | All | WGS and WES | TC (14) |
| AC (6) | AC (2) | AC (6) | AC (6) | ||||||
| 2018 | George et al. [12] | 60 | LCNEC (60) | LCNEC (11) | LCNEC (55) | 0 | All | WGS and WES | 60 LCNEC |
| 2019 | Simbolo et al. [24] | 67 | AC (35) | 0 | 0 | AC (35) | 409 (HCTS) * | Ampliseq Transcriptome Human Gene Expression Kit (ThermoFisher); Ampliseq Comprehensive Cancer Panel (ThermoFisher) | AC (14) HTCS AC (21) t-NGS LCNEC (14) HTCS LCNEC (18) t-NGS |
| LCNEC (32) | LCNEC (32) | 13 (t-NGS) | |||||||
| 2019 | Saurabh V. Laddha et al. [34] | 29 | TC (16) AC (13) | 0 | 0 | TC (16) AC (13) | 354 (t-NGS) | MSK-IMPACT | TC (16) AC (13) |
| Features | All | TCs | ACs | LCNECs | SCLCs | p-Value * |
|---|---|---|---|---|---|---|
| Total Mutated Genes † | 201 | 47 | 57 | 186 | 168 | - |
| Mutational Rate % | ||||||
| Median [range] | 4.00 (1.14–92.76) | 2.17 (1.18–4.84) | 3.85 (1.37–24.66) | 4.22 (1.14–87.14) | 4.55 (1.36–92.76) | <0.0001 |
| Somatic coding mutation per case | ||||||
| Median [range] | 3 (1–42) | 1 (1–17) | 2 (1–31) | 3 (1–40) | 7 (1–42) | <0.0001 |
| Type of Mutations | ||||||
| Missense | 2958 (69.8) | 66 (75.9) | 107 (73.8) | 1299 (68.8) | 1486 (70.1) | |
| Nonsense | 553 (13.05) | 6 (6.9) | 10 (6.9) | 284 (15.1) | 253 (11.9) | |
| Frameshift | 503 (11.9) | 7 (8) | 24 (16.5) | 204 (10.8) | 268 (12.7) | |
| Splice | 222 (5.2) | 8 (9.2) | 4 (2.8) | 100 (5.3) | 110 (5.2) | |
| Non-Stop | 2 (0.05) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (0.1) | 0.004 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Centonze, G.; Biganzoli, D.; Prinzi, N.; Pusceddu, S.; Mangogna, A.; Tamborini, E.; Perrone, F.; Busico, A.; Lagano, V.; Cattaneo, L.; et al. Beyond Traditional Morphological Characterization of Lung Neuroendocrine Neoplasms: In Silico Study of Next-Generation Sequencing Mutations Analysis across the Four World Health Organization Defined Groups. Cancers 2020, 12, 2753. https://doi.org/10.3390/cancers12102753
Centonze G, Biganzoli D, Prinzi N, Pusceddu S, Mangogna A, Tamborini E, Perrone F, Busico A, Lagano V, Cattaneo L, et al. Beyond Traditional Morphological Characterization of Lung Neuroendocrine Neoplasms: In Silico Study of Next-Generation Sequencing Mutations Analysis across the Four World Health Organization Defined Groups. Cancers. 2020; 12(10):2753. https://doi.org/10.3390/cancers12102753
Chicago/Turabian StyleCentonze, Giovanni, Davide Biganzoli, Natalie Prinzi, Sara Pusceddu, Alessandro Mangogna, Elena Tamborini, Federica Perrone, Adele Busico, Vincenzo Lagano, Laura Cattaneo, and et al. 2020. "Beyond Traditional Morphological Characterization of Lung Neuroendocrine Neoplasms: In Silico Study of Next-Generation Sequencing Mutations Analysis across the Four World Health Organization Defined Groups" Cancers 12, no. 10: 2753. https://doi.org/10.3390/cancers12102753
APA StyleCentonze, G., Biganzoli, D., Prinzi, N., Pusceddu, S., Mangogna, A., Tamborini, E., Perrone, F., Busico, A., Lagano, V., Cattaneo, L., Sozzi, G., Roz, L., Biganzoli, E., & Milione, M. (2020). Beyond Traditional Morphological Characterization of Lung Neuroendocrine Neoplasms: In Silico Study of Next-Generation Sequencing Mutations Analysis across the Four World Health Organization Defined Groups. Cancers, 12(10), 2753. https://doi.org/10.3390/cancers12102753