Muscle Loss after Chemoradiotherapy as a Biomarker of Distant Failures in Locally Advanced Cervical Cancer

 , ,
, , 
Abstract
:1. Introduction
2. Results
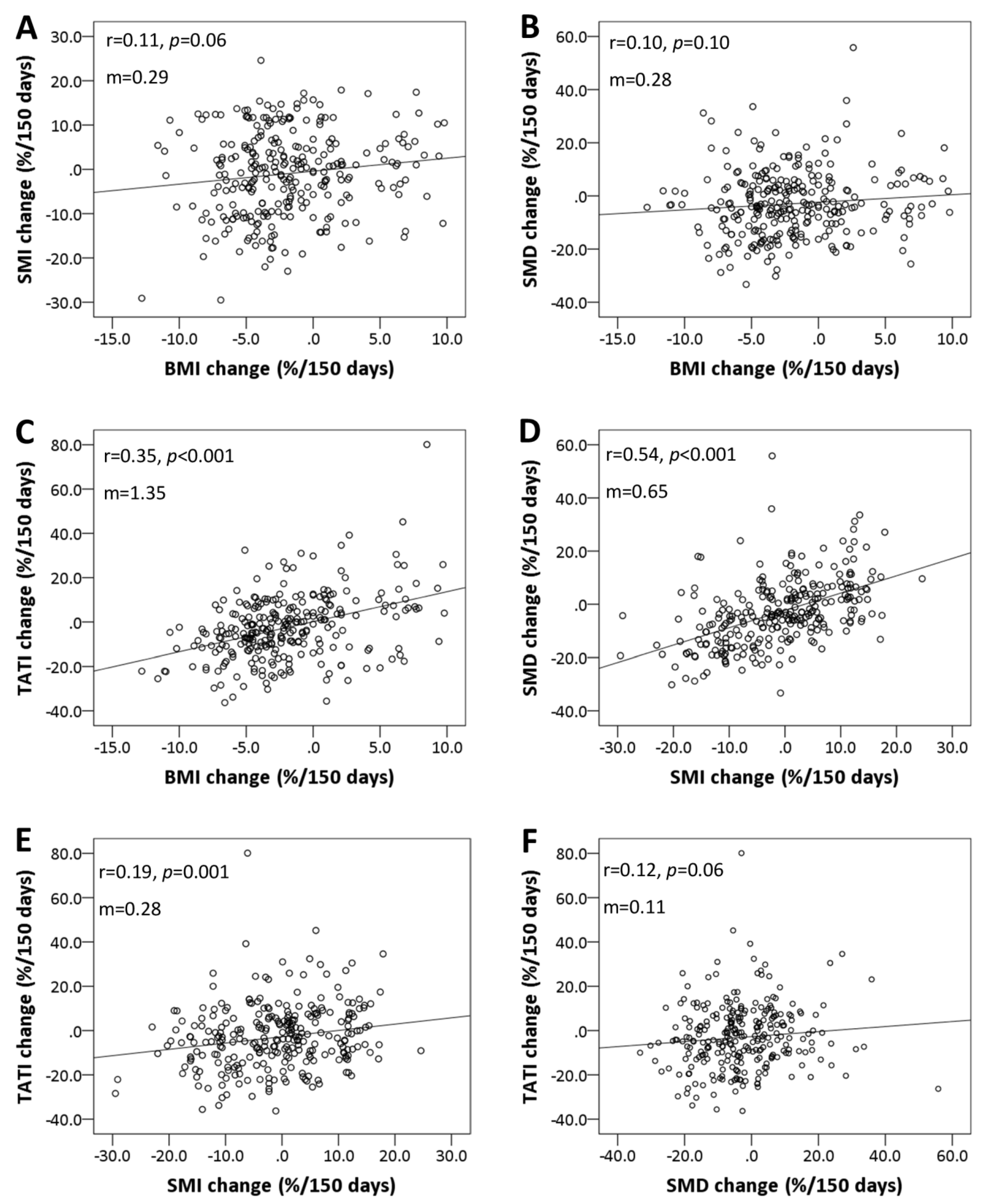
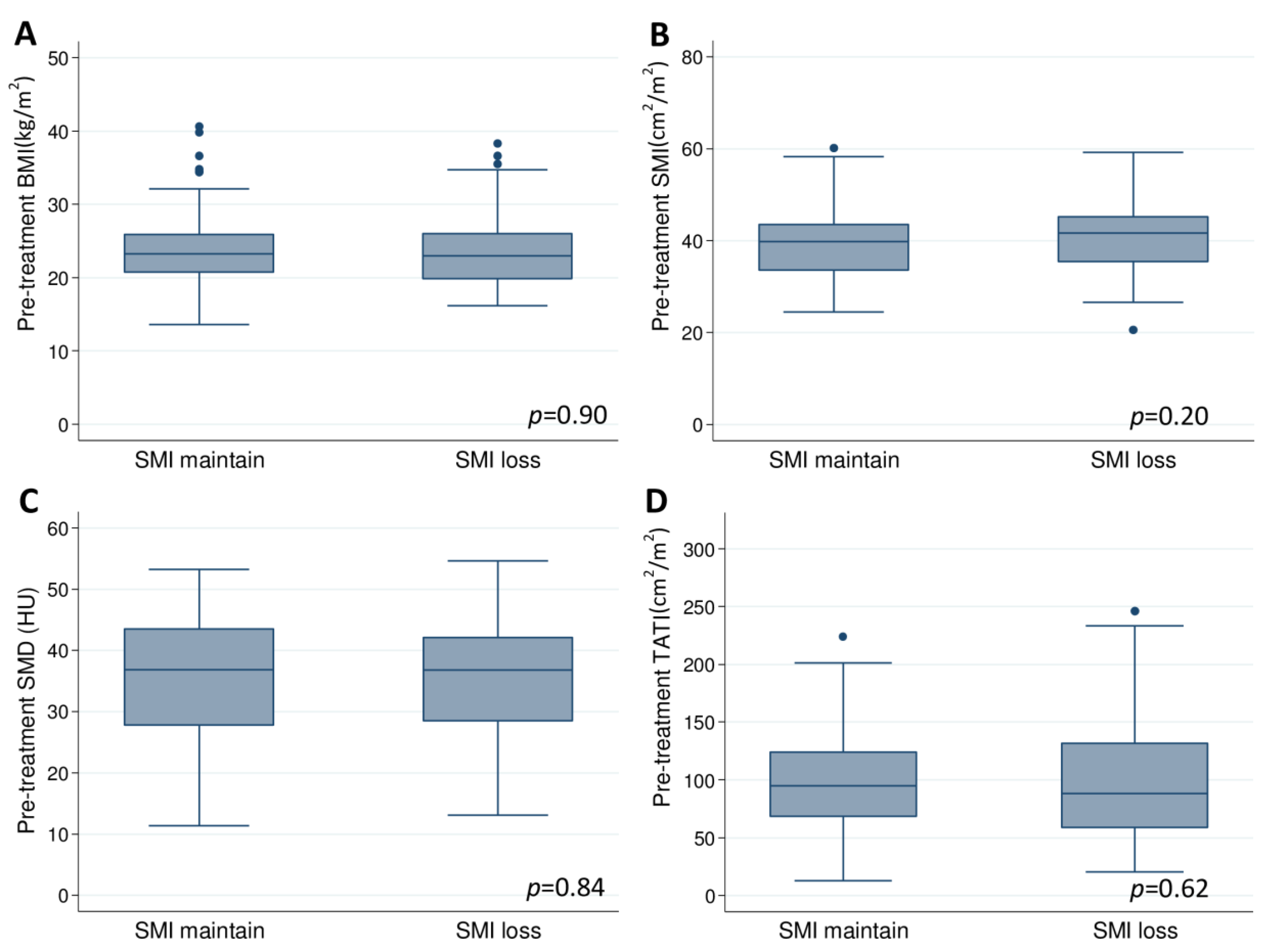
2.1. Body Composition at the Baseline and Change after Treatment
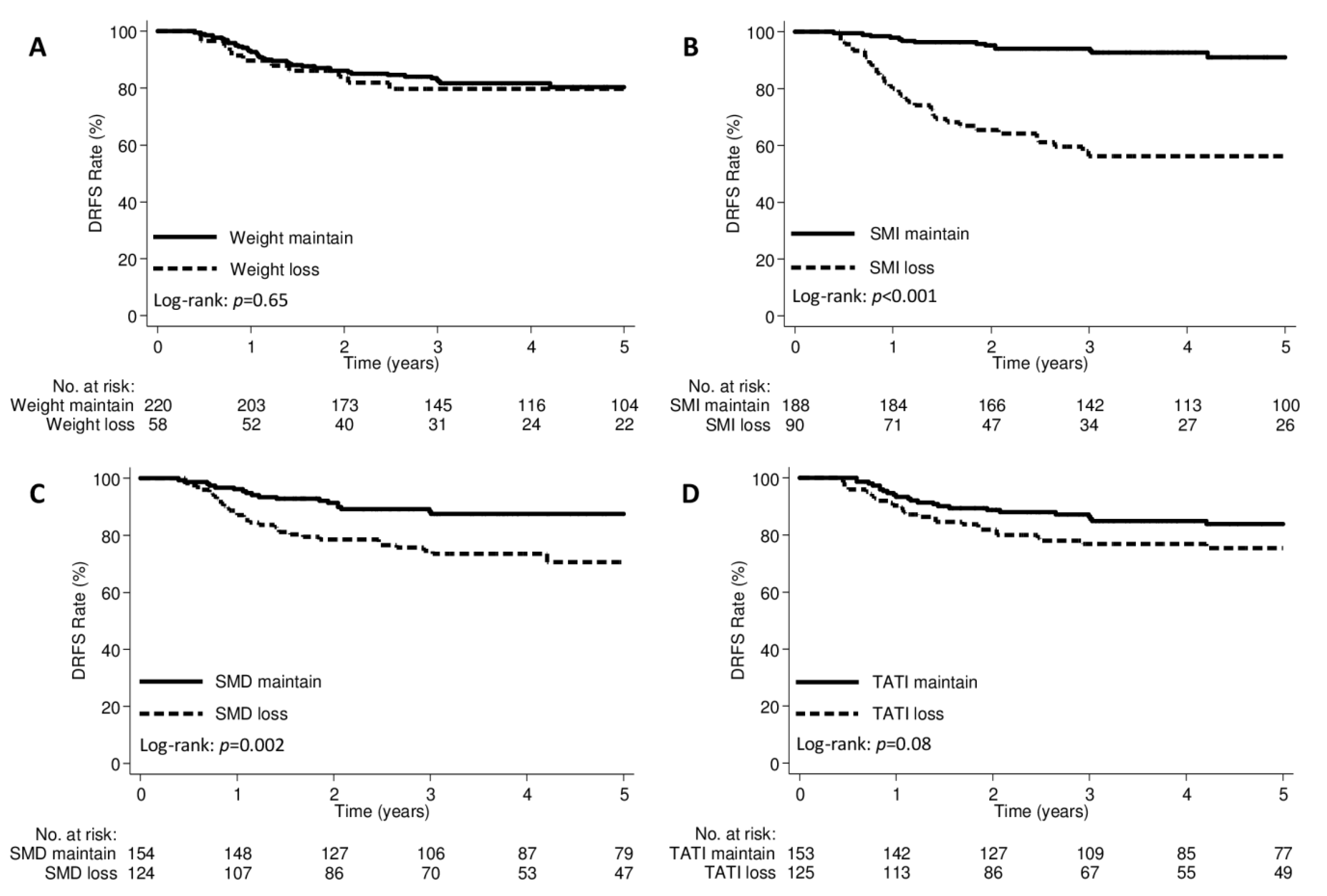
2.2. Body Composition and Distant Failures
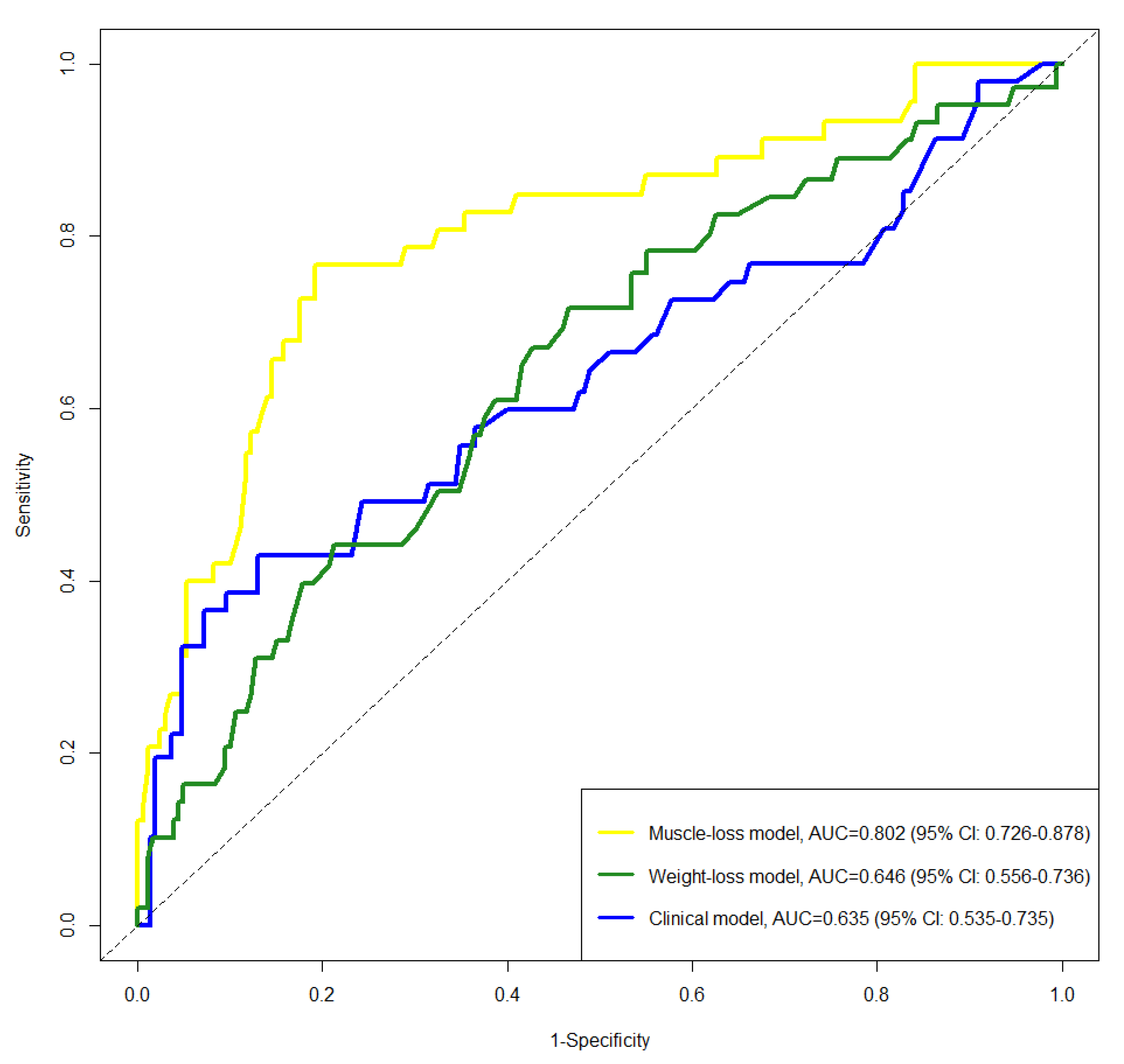
2.3. Comparison of Clinical, Weight-Loss, and Muscle-Loss Models
3. Discussion
4. Materials and Methods
4.1. Patients
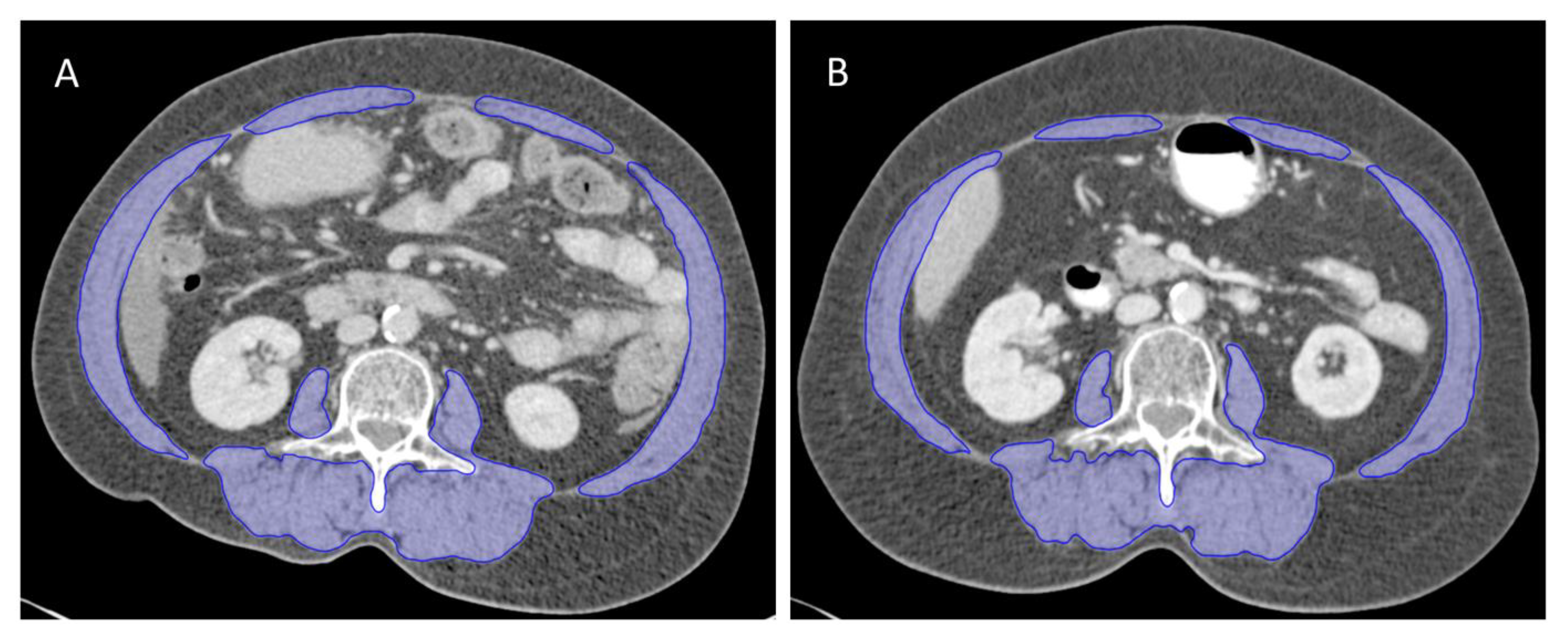
4.2. Computed Tomography-Based Body Composition Analysis
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Sturdza, A.; Potter, R.; Fokdal, L.U.; Haie-Meder, C.; Tan, L.T.; Mazeron, R.; Petric, P.; Segedin, B.; Jurgenliemk-Schulz, I.M.; Nomden, C.; et al. Image guided brachytherapy in locally advanced cervical cancer: Improved pelvic control and survival in RetroEMBRACE, a multicenter cohort study. Radiother. Oncol. 2016, 120, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Lin, J.B.; Chang, C.L.; Jan, Y.T.; Sun, F.J.; Wu, M.H.; Chen, Y.J. Prophylactic lower para-aortic irradiation using intensity-modulated radiotherapy mitigates the risk of para-aortic recurrence in locally advanced cervical cancer: A 10-year institutional experience. Gynecol. Oncol. 2017, 146, 20–26. [Google Scholar] [CrossRef]
- Lee, J.; Lin, J.B.; Chang, C.L.; Sun, F.J.; Wu, M.H.; Jan, Y.T.; Chen, Y.J. Impact of para-aortic recurrence risk-guided intensity-modulated radiotherapy in locally advanced cervical cancer with positive pelvic lymph nodes. Gynecol. Oncol. 2018, 148, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Liang, J.A.; Chen, S.W.; Hung, Y.C.; Yeh, L.S.; Chang, W.C.; Lin, W.C.; Chang, Y.Y. Low-dose, prophylactic, extended-field, intensity-modulated radiotherapy plus concurrent weekly cisplatin for patients with stage IB2-IIIB cervical cancer, positive pelvic lymph nodes, and negative para-aortic lymph nodes. Int. J. Gynecol. Cancer 2014, 24, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Tan, L.T.; Potter, R.; Sturdza, A.; Fokdal, L.; Haie-Meder, C.; Schmid, M.; Gregory, D.; Petric, P.; Jurgenliemk-Schulz, I.; Gillham, C.; et al. Change in Patterns of Failure After Image-Guided Brachytherapy for Cervical Cancer: Analysis from the RetroEMBRACE Study. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 895–902. [Google Scholar] [CrossRef] [PubMed]
- Yavas, G.; Yavas, C.; Sen, E.; Oner, I.; Celik, C.; Ata, O. Adjuvant carboplatin and paclitaxel after concurrent cisplatin and radiotherapy in patients with locally advanced cervical cancer. Int. J. Gynecol. Cancer 2019, 29, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Tangjitgamol, S.; Katanyoo, K.; Laopaiboon, M.; Lumbiganon, P.; Manusirivithaya, S.; Supawattanabodee, B. Adjuvant chemotherapy after concurrent chemoradiation for locally advanced cervical cancer. Cochrane Database Syst. Rev. 2014, CD010401. [Google Scholar] [CrossRef] [Green Version]
- National Comprehensive Cancer Network. Clinical Practice Guidelines in Oncology: Cervical Cancer (Version 1.2018). Available online: https://www.nccn.org/professionals/physician_gls/pdf/cervical.pdf (accessed on 1 February 2018).
- Jurgenliemk-Schulz, I.M.; Beriwal, S.; de Leeuw, A.A.C.; Lindegaard, J.C.; Nomden, C.N.; Potter, R.; Tanderup, K.; Viswanathan, A.N.; Erickson, B. Management of Nodal Disease in Advanced Cervical Cancer. Semin. Radiat. Oncol. 2019, 29, 158–165. [Google Scholar] [CrossRef]
- Kiyotoki, T.; Nakamura, K.; Haraga, J.; Omichi, C.; Ida, N.; Saijo, M.; Nishida, T.; Kusumoto, T.; Masuyama, H. Sarcopenia Is an Important Prognostic Factor in Patients With Cervical Cancer Undergoing Concurrent Chemoradiotherapy. Int. J. Gynecol. Cancer 2018, 28, 168–175. [Google Scholar] [CrossRef]
- Lee, J.; Chang, C.L.; Lin, J.B.; Wu, M.H.; Sun, F.J.; Jan, Y.T.; Hsu, S.M.; Chen, Y.J. Skeletal Muscle Loss Is an Imaging Biomarker of Outcome after Definitive Chemoradiotherapy for Locally Advanced Cervical Cancer. Clin. Cancer Res. 2018, 24, 5028–5036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez, M.; Castro-Eguiluz, D.; Luvian-Morales, J.; Jimenez-Lima, R.; Aguilar-Ponce, J.L.; Isla-Ortiz, D.; Cetina, L. Deterioration of nutritional status of patients with locally advanced cervical cancer during treatment with concomitant chemoradiotherapy. J. Hum. Nutr. Diet 2019, 32, 480–491. [Google Scholar] [CrossRef] [PubMed]
- Mourtzakis, M.; Prado, C.M.; Lieffers, J.R.; Reiman, T.; McCargar, L.J.; Baracos, V.E. A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl. Physiol. Nutr. Metab. 2008, 33, 997–1006. [Google Scholar] [CrossRef] [PubMed]
- Shen, W.; Punyanitya, M.; Wang, Z.; Gallagher, D.; St-Onge, M.P.; Albu, J.; Heymsfield, S.B.; Heshka, S. Total body skeletal muscle and adipose tissue volumes: Estimation from a single abdominal cross-sectional image. J. Appl. Physiol. 2004, 97, 2333–2338. [Google Scholar] [CrossRef] [Green Version]
- Chung, E.; Lee, H.S.; Cho, E.S.; Park, E.J.; Baik, S.H.; Lee, K.Y.; Kang, J. Changes in Body Composition During Adjuvant FOLFOX Chemotherapy and Overall Survival in Non-Metastatic Colon Cancer. Cancers 2019, 12, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le-Rademacher, J.G.; Storrick, E.M.; Jatoi, A. Remarks on the design and analyses of longitudinal studies for cancer patients with anorexia and weight loss. J. Cachexia Sarcopenia Muscle 2019, 10, 1175–1182. [Google Scholar] [CrossRef] [PubMed]
- Naumann, P.; Eberlein, J.; Farnia, B.; Liermann, J.; Hackert, T.; Debus, J.; Combs, S.E. Cachectic Body Composition and Inflammatory Markers Portend a Poor Prognosis in Patients with Locally Advanced Pancreatic Cancer Treated with Chemoradiation. Cancers 2019, 11, 1655. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Chang, C.L.; Lin, J.B.; Wu, M.H.; Sun, F.J.; Wu, C.J.; Tai, H.C.; Hsu, S.M.; Chen, Y.J. The Effect of Body Mass Index and Weight Change on Late Gastrointestinal Toxicity in Locally Advanced Cervical Cancer Treated With Intensity-modulated Radiotherapy. Int. J. Gynecol. Cancer 2018, 28, 1377–1386. [Google Scholar] [CrossRef]
- Martin, L.; Birdsell, L.; Macdonald, N.; Reiman, T.; Clandinin, M.T.; McCargar, L.J.; Murphy, R.; Ghosh, S.; Sawyer, M.B.; Baracos, V.E. Cancer cachexia in the age of obesity: Skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J. Clin. Oncol. 2013, 31, 1539–1547. [Google Scholar] [CrossRef]
- Kays, J.K.; Shahda, S.; Stanley, M.; Bell, T.M.; O’Neill, B.H.; Kohli, M.D.; Couch, M.E.; Koniaris, L.G.; Zimmers, T.A. Three cachexia phenotypes and the impact of fat-only loss on survival in FOLFIRINOX therapy for pancreatic cancer. J. Cachexia Sarcopenia Muscle 2018, 9, 673–684. [Google Scholar] [CrossRef]
- Brown, J.C.; Cespedes Feliciano, E.M.; Caan, B.J. The evolution of body composition in oncology-epidemiology, clinical trials, and the future of patient care: Facts and numbers. J. Cachexia Sarcopenia Muscle 2018, 9, 1200–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.Y.; Yang, Y.C.; Chen, T.C.; Chen, J.R.; Chen, Y.J.; Wu, M.H.; Jan, Y.T.; Chang, C.L.; Lee, J. Muscle loss during primary debulking surgery and chemotherapy predicts poor survival in advanced-stage ovarian cancer. J. Cachexia Sarcopenia Muscle 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonald, A.M.; Swain, T.A.; Mayhew, D.L.; Cardan, R.A.; Baker, C.B.; Harris, D.M.; Yang, E.S.; Fiveash, J.B. CT Measures of Bone Mineral Density and Muscle Mass Can Be Used to Predict Noncancer Death in Men with Prostate Cancer. Radiology 2017, 282, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.Y.; Sun, F.J.; Lee, J. Prognostic value of muscle measurement using the standardized phase of computed tomography in patients with advanced ovarian cancer. Nutrition 2019, 72, 110642. [Google Scholar] [CrossRef]
- Cohen, S.; Nathan, J.A.; Goldberg, A.L. Muscle wasting in disease: Molecular mechanisms and promising therapies. Nat. Rev. Drug Discov. 2015, 14, 58–74. [Google Scholar] [CrossRef]
- Gallot, Y.S.; Durieux, A.C.; Castells, J.; Desgeorges, M.M.; Vernus, B.; Plantureux, L.; Remond, D.; Jahnke, V.E.; Lefai, E.; Dardevet, D.; et al. Myostatin gene inactivation prevents skeletal muscle wasting in cancer. Cancer Res. 2014, 74, 7344–7356. [Google Scholar] [CrossRef] [Green Version]
- Van Dijk, D.P.J.; Horstman, A.M.H.; Smeets, J.S.J.; den Dulk, M.; Grabsch, H.I.; Dejong, C.H.C.; Rensen, S.S.; Olde Damink, S.W.M.; van Loon, L.J.C. Tumour-specific and organ-specific protein synthesis rates in patients with pancreatic cancer. J. Cachexia Sarcopenia Muscle 2019, 10, 549–556. [Google Scholar] [CrossRef] [Green Version]
- Wen, Y.F.; Cheng, T.T.; Chen, X.L.; Huang, W.J.; Peng, H.H.; Zhou, T.C.; Lin, X.D.; Zeng, L.S. Elevated circulating tumor cells and squamous cell carcinoma antigen levels predict poor survival for patients with locally advanced cervical cancer treated with radiotherapy. PLoS ONE 2018, 13, e0204334. [Google Scholar] [CrossRef]
- Pin, F.; Barreto, R.; Kitase, Y.; Mitra, S.; Erne, C.E.; Novinger, L.J.; Zimmers, T.A.; Couch, M.E.; Bonewald, L.F.; Bonetto, A. Growth of ovarian cancer xenografts causes loss of muscle and bone mass: A new model for the study of cancer cachexia. J. Cachexia Sarcopenia Muscle 2018, 9, 685–700. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.L.; Lee, D.E.; Rosa-Caldwell, M.E.; Brown, L.A.; Perry, R.A.; Haynie, W.S.; Huseman, K.; Sataranatarajan, K.; Van Remmen, H.; Washington, T.A.; et al. Protein imbalance in the development of skeletal muscle wasting in tumour-bearing mice. J. Cachexia Sarcopenia Muscle 2018, 9, 987–1002. [Google Scholar] [CrossRef]
- Baracos, V.E.; Arribas, L. Sarcopenic obesity: Hidden muscle wasting and its impact for survival and complications of cancer therapy. Ann. Oncol. 2018, 29, ii1–ii9. [Google Scholar] [CrossRef]
- Caan, B.J.; Cespedes Feliciano, E.M.; Kroenke, C.H. The Importance of Body Composition in Explaining the Overweight Paradox in Cancer-Counterpoint. Cancer Res. 2018, 78, 1906–1912. [Google Scholar] [CrossRef] [Green Version]
- Fearon, K.; Strasser, F.; Anker, S.D.; Bosaeus, I.; Bruera, E.; Fainsinger, R.L.; Jatoi, A.; Loprinzi, C.; MacDonald, N.; Mantovani, G.; et al. Definition and classification of cancer cachexia: An international consensus. Lancet Oncol. 2011, 12, 489–495. [Google Scholar] [CrossRef]
- Ubachs, J.; Ziemons, J.; Minis-Rutten, I.J.G.; Kruitwagen, R.; Kleijnen, J.; Lambrechts, S.; Olde Damink, S.W.M.; Rensen, S.S.; Van Gorp, T. Sarcopenia and ovarian cancer survival: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2019, 10, 1165–1174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.; Lin, J.B.; Wu, M.H.; Jan, Y.T.; Chang, C.L.; Huang, C.Y.; Sun, F.J.; Chen, Y.J. Muscle radiodensity loss during cancer therapy is predictive for poor survival in advanced endometrial cancer. J. Cachexia Sarcopenia Muscle 2019, 10, 814–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, M.H.; Yoon, S.B.; Lee, K.; Song, M.; Lee, I.S.; Lee, M.A.; Hong, T.H.; Choi, M.G. Preoperative sarcopenia and post-operative accelerated muscle loss negatively impact survival after resection of pancreatic cancer. J. Cachexia Sarcopenia Muscle 2018, 9, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Kang, L.; Chen, W.; Petrick, N.A.; Gallas, B.D. Comparing two correlated C indices with right-censored survival outcome: A one-shot nonparametric approach. Stat. Med. 2015, 34, 685–703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanche, P.; Kattan, M.W.; Gerds, T.A. The c-index is not proper for the evaluation of t-year predicted risks. Biostatistics 2019, 20, 347–357. [Google Scholar] [CrossRef]
- Kamarudin, A.N.; Cox, T.; Kolamunnage-Dona, R. Time-dependent ROC curve analysis in medical research: Current methods and applications. BMC Med. Res. Methodol. 2017, 17, 53. [Google Scholar] [CrossRef] [Green Version]
- Blanche, P.; Dartigues, J.F.; Jacqmin-Gadda, H. Estimating and comparing time-dependent areas under receiver operating characteristic curves for censored event times with competing risks. Stat. Med. 2013, 32, 5381–5397. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Overall (n = 278) | SMI loss (n = 90) | SMI Maintained (n = 188) | p-Value |
|---|---|---|---|---|
| Age (years), median (IQR) | 62 (53–73) | 64 (54–75) | 62 (52–71) | 0.11 |
| ECOG performance status | 0.08 | |||
| 0 | 253 (91.0) | 78 (86.7) | 175 (93.1) | |
| 1 | 25 (9.0) | 12 (13.3) | 13 (6.9) | |
| FIGO stage | 0.28 | |||
| IB-II | 203 (73.0) | 62 (68.9) | 141 (75.0) | |
| III-IVA | 75 (27.0) | 28 (31.1) | 47 (25.0) | |
| Pathology | 0.002 | |||
| Squamous cell carcinoma | 246 (88.5) | 72 (80.0) | 174 (92.6) | |
| Adenocarcinoma | 32 (11.5) | 18 (20.0) | 14 (7.4) | |
| Pelvic lymph node | 0.80 | |||
| Positive | 136 (48.9) | 45 (50.0) | 91 (48.4) | |
| Negative | 142 (51.1) | 45 (50.0) | 97 (51.6) | |
| SCC-Ag level, median (IQR) | 7.6 (3.3–15.0) | 8.6 (2.8–20.4) | 6.9 (3.3–14.3) | 0.29 |
| Radiation field | 0.09 | |||
| Extended-field radiotherapy | 147 (52.9) | 41 (45.6) | 106 (56.4) | |
| Pelvic radiotherapy | 131 (47.1) | 49 (54.4) | 82 (43.6) | |
| Chemotherapy | 0.07 | |||
| Yes | 243 (87.4) | 74 (82.2) | 169 (89.9) | |
| No | 35 (12.6) | 16 (17.8) | 19 (10.1) | |
| Chemotherapy cycles | n = 243 | n = 74 | n = 169 | 0.78 |
| 5–6 | 181 (74.5) | 56 (75.7) | 125 (74.0) | |
| 1–4 | 62 (25.5) | 18 (24.3) | 44 (26.0) | |
| Overall treatment duration (day), median (IQR) | 58 (54–61) | 59 (52–61) | 58 (54–61) | 0.89 |
| Median (IQR) duration between CT scans, days | 143 (135–150) | 141 (133–149) | 143 (135–151) | 0.38 |
| Variable | First CT Scan | Second CT Scan | Relative Change Per 150 Days (%) | ||
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean | 95% CI | p-Value | |
| BMI (kg/m2) | 23.4 ± 4.3 | 23.0 ± 4.3 | −1.9 | −2.4 to −1.4 | <0.001 |
| SMI (cm2/m2) | 39.8 ± 7.3 | 39.3 ± 7.6 | −1.0 | −2.1 to 0.2 | 0.09 |
| SMD (HU) | 35.6 ± 9.5 | 34.5 ± 9.6 | −2.9 | −4.4 to −1.5 | <0.001 |
| TATI (cm2/m2) | 97.7 ± 44.5 | 93.7 ± 41.8 | −3.0 | −4.9 to −1.2 | 0.001 |
| Variable | Clinical Model | Weight-Loss Model | Muscle-Loss Model | |||
|---|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| FIGO stage | ||||||
| IB-II | Reference | Reference | Reference | |||
| III-IVA | 2.30 (1.21–4.37) | 0.01 | 2.36 (1.24–4.47) | 0.01 | 1.98 (1.05–3.74) | 0.04 |
| PLNs involvement | ||||||
| Negative | Reference | Reference | Reference | |||
| Positive | 1.75 (0.87–3.50) | 0.12 | 1.81 (0.90–3.63) | 0.10 | 2.31 (1.24–4.30) | 0.01 |
| Pathology | ||||||
| SCC | Reference | Reference | Reference | |||
| Adenocarcinoma | 4.43 (2.30–8.53) | <0.001 | 4.63 (2.40–8.94) | <0.001 | 3.03 (1.54–5.95) | 0.001 |
| SCC-Ag | 1.02 (1.01–1.02) | <0.001 | 1.02 (1.01–1.02) | <0.001 | 1.02 (1.01–1.02) | 0.001 |
| Weight change | ||||||
| Weight maintain | - | - | Reference | - | - | |
| Weight loss | - | - | 1.51 (0.76–3.02) | 0.24 | - | - |
| SMI change | ||||||
| SMI maintain | - | - | - | - | Reference | |
| SMI loss | - | - | - | - | 6.31 (3.18–12.53) | <0.001 |
| SMD change | ||||||
| SMD maintain | - | - | - | - | Reference | |
| SMD loss | - | - | - | - | 1.00 (0.53–1.87) | 0.99 |
| TATI change | ||||||
| TATI maintain | - | - | - | - | Reference | |
| TATI loss | - | - | - | - | 1.32 (0.73–2.38) | 0.36 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.; Lin, J.-B.; Wu, M.-H.; Chang, C.-L.; Jan, Y.-T.; Chen, Y.-J. Muscle Loss after Chemoradiotherapy as a Biomarker of Distant Failures in Locally Advanced Cervical Cancer. Cancers 2020, 12, 595. https://doi.org/10.3390/cancers12030595
Lee J, Lin J-B, Wu M-H, Chang C-L, Jan Y-T, Chen Y-J. Muscle Loss after Chemoradiotherapy as a Biomarker of Distant Failures in Locally Advanced Cervical Cancer. Cancers. 2020; 12(3):595. https://doi.org/10.3390/cancers12030595
Chicago/Turabian StyleLee, Jie, Jhen-Bin Lin, Meng-Hao Wu, Chih-Long Chang, Ya-Ting Jan, and Yu-Jen Chen. 2020. "Muscle Loss after Chemoradiotherapy as a Biomarker of Distant Failures in Locally Advanced Cervical Cancer" Cancers 12, no. 3: 595. https://doi.org/10.3390/cancers12030595
APA StyleLee, J., Lin, J. -B., Wu, M. -H., Chang, C. -L., Jan, Y. -T., & Chen, Y. -J. (2020). Muscle Loss after Chemoradiotherapy as a Biomarker of Distant Failures in Locally Advanced Cervical Cancer. Cancers, 12(3), 595. https://doi.org/10.3390/cancers12030595