Combined wIRA-Hyperthermia and Hypofractionated Re-Irradiation in the Treatment of Locally Recurrent Breast Cancer: Evaluation of Therapeutic Outcome Based on a Novel Size Classification

 , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Notter, M.; Piazena, H.; Vaupel, P. Hypofractionated re-irradiation of large-sized recurrent breast cancer with thermography-controlled, contact-free water-filtered infra-red-A hyperthermia: A retrospective study of 73 patients. Int. J. Hyperth. 2017, 33, 227–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merino, T.; Tran, W.T.; Czarnota, G.J. Re-irradiation for locally recurrent refractory breast cancer. Oncotarget 2015, 6, 35051–35062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oldenborg, S.; Rasch, C.R.N.; Os, R.V.; Kusumanto, Y.H.; Oei, B.S.; Venselaar, J.L.; Heymans, M.W.; Zum Vörde Sive Vörding, P.J.; Crezee, H.; Tienhoven, G.V. Reirradiation + hyperthermia for recurrent breast cancer en cuirasse. Strahlenther. Onkol. 2017, 194, 206–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horsman, M.R.; Overgaard, J. Hyperthermia: A potent enhancer of radiotherapy. Clin. Oncol. (R. Coll. Radiol.) 2007, 19, 418–426. [Google Scholar] [CrossRef]
- Elming, P.B.; Sørensen, B.S.; Oei, A.L.; Franken, N.A.P.; Crezee, J.; Overgaard, J.; Horsman, M.R. Hyperthermia: The optimal treatment to overcome radiation resistant hypoxia. Cancers 2019, 11, 60. [Google Scholar] [CrossRef] [Green Version]
- Vaupel, P.; Höckel, M.; Mayer, A. Detection and characterization of tumor hypoxia using pO2 histography. Antioxid. Redox Signal. 2007, 9, 1221–1235. [Google Scholar] [CrossRef]
- Vaupel, P.; Briest, S.; Höckel, M. Hypoxia in breast cancer: Pathogenesis, characterization and biological/therapeutic implications. Wien. Med. Wschr. 2002, 152, 334–342. [Google Scholar] [CrossRef]
- Thomsen, A.R.; Aldrian, C.; Niedermann, G.; Grosu, A.L.; Vaupel, P.; Lund, P.G. Differential effects of 42 °C-hyperthermia on radiation response of breast cancer spheroids vs. normal human skin explants. In Proceedings of the 36th Annual Meeting of the Society for Thermal Medicine (STM), St. Pete Beach, FL, USA, 28 April–2 May 2019. [Google Scholar]
- Overgaard, J. Simultaneous and sequential hyperthermia and radiation treatment of an experimental tumor and its surrounding normal tissue in vivo. Int. J. Radiat. Oncol. Biol. Phys. 1980, 6, 1507–1517. [Google Scholar] [CrossRef]
- van Leeuwen, C.M.; Oei, A.L.; Chin, K.W.T.K.; Crezee, J.; Bel, A.; Westermann, A.M.; Buist, M.R.; Franken, N.A.P.; Stalpers, L.J.A.; Kok, H.P. A short time interval between radiotherapy and hyperthermia reduces in-field recurrence and mortality in women with advanced cervical cancer. Radiat. Oncol. 2017, 12, 75. [Google Scholar] [CrossRef]
- Oei, A.L.; Kok, H.P.; Oei, S.B.; Horsman, M.R.; Stalpers, L.J.A.; Franken, N.A.P.; Crezee, J. Molecular and biological rationale of hyperthermia as radio-and chemosensitizer. Adv. Drug Deliv. Rev. 2020, S0169–S409. [Google Scholar] [CrossRef]
- Frey, B.; Weiss, E.M.; Rubner, Y.; Wunderlich, R.; Ott, O.J.; Sauer, R.; Fietkau, R.; Gaipl, U.S. Old and new facts about hyperthermia-induced modulations of the immune system. Int. J. Hyperth. 2012, 28, 528–542. [Google Scholar] [CrossRef] [PubMed]
- Dewhirst, M.W.; Vujaskovic, Z.; Jones, E.; Thrall, D. Re-setting the biologic rationale for thermal therapy. Int. J. Hyperth. 2005, 21, 779–790. [Google Scholar] [CrossRef] [PubMed]
- Kötter, B.; Frey, B.; Winderl, M.; Rubner, Y.; Scheithauer, H.; Sieber, R.; Fietkau, R.; Gaipl, U.S. The in vitro immunogenic potential of caspase-3 proficient breast cancer cells with basal low immunogenicity is increased by hypofractionated irradiation. Radiat. Oncol. 2015, 10, 197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Datta, N.R.; Puric, E.; Klingbiel, D.; Gomez, S.; Bodis, S. Hyperthermia and radiation therapy in locoregional recurrent breast cancers: A systematic review and meta-analysis. Int. J. Radiat. Oncol. Biol. Phys. 2016, 94, 1073–1087. [Google Scholar] [CrossRef] [PubMed]
- Marta, G.N.; Hijal, T.; Carvalho, H.D.A. Reirradiation for locally recurrent breast cancer. Breast 2017, 33, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Wadasadawala, T.; Vadgaonkar, R.; Bajpai, J. Management of isolated locoregional recurrences in breast cancer: A review of local and systemic modalities. Clin. Breast Cancer 2017, 17, 493–502. [Google Scholar] [CrossRef]
- Kaidar-Person, O.; Oldenborg, S.; Poortmans, P. Re-irradiation and hyperthermia in breast cancer. Clin. Oncol. 2018, 30, 73–84. [Google Scholar] [CrossRef]
- Arslan, S.A.; Ozdemir, N.; Sendur, M.A.; Eren, T.; Ozturk, H.F.; Aral, I.P.; Delikgoz, E.D.; Inan, G.A. Hyperthermia and radiotherapy combination for locoregional recurrences of breast cancer: A review. Breast Cancer Manag. 2018, 6, 117–126. [Google Scholar] [CrossRef] [Green Version]
- Youssef, I. Hyperthermia for Chest Wall Recurrences; StatPearls Publishing: Treasure Island, FL, USA, 2019; Bookshelf ID: NBK513294. [Google Scholar] [PubMed]
- De-Colle, C.; Weidner, N.; Heinrich, V.; Brucker, S.; Hahn, M.; Macmillan, K.; Lamprecht, U.; Gaupp, S.; Voigt, O.; Zips, D. Hyperthermic chest wall re-irradiation in recurrent breast cancer: A prospective observational study. Strahlenther. Onkol. 2019, 195, 318–326. [Google Scholar] [CrossRef]
- Oldenborg, S.; Os, R.V.; Oei, B.; Poortmans, P. Impact of technique and schedule of reirradiation plus hyperthermia on outcome after surgery for patients with recurrent breast cancer. Cancers 2019, 11, 782. [Google Scholar] [CrossRef] [Green Version]
- Linthorst, M.; Geel, A.N.V.; Baaijens, M.; Ameziane, A.; Ghidey, W.; Rhoon, G.C.V.; van der Zee, J. Re-irradiation and hyperthermia after surgery for recurrent breast cancer. Radiother. Oncol. 2013, 109, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Oldenborg, S.; Griesdoorn, V.; Os, R.V.; Kusumanto, Y.H.; Oei, B.S.; Venselaar, J.L.; Paul, J.; Vörding, Z.V.S.; Heymans, M.W.; Kolff, M.W.; et al. Reirradiation and hyperthermia for irresectable locoregional recurrent breast cancer in previously irradiated area: Size matters. Radiother. Oncol. 2015, 117, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Vaupel, P.; Piazena, H.; Müller, W.; Notter, M. Biophysical and photobiological basics of water-filtered infrared-A hyperthermia of superficial tumors. Int. J. Hyperth. 2018, 35, 26–36. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.K.; Antell, A.G.; Perez, C.A.; Straube, W.L.; Ramachandran, G.; Myerson, R.J.; Emami, B.; Molmenti, E.P.; Buckner, A.; Lockett, M.A. Superficial hyperthermia and irradiation for recurrent breast carcinoma of the chest wall: Prognostic factors in 196 tumors. Int. J. Radiat. Oncol. Biol. Phys. 1998, 40, 365–375. [Google Scholar] [CrossRef]
- Dharmaiah, S.; Zeng, J.; Rao, V.S.; Zi, O.; Ma, T.; Yu, K.; Bhatt, H.; Shah, C.; Godley, A.; Xia, P.; et al. Clinical and dosimetric evaluation of recurrent breast cancer patients treated with hyperthermia and radiation. Int. J. Hyperth. 2019, 36, 986–992. [Google Scholar] [CrossRef] [Green Version]
- Notter, M.; Vaupel, P. Re-irradiation and wIRA-hyperthermia for superficial widespread breast cancer recurrences: An update. In Proceedings of the 31st Annual Meeting of the European Society for Hyperthermic Oncology (ESHO), Athens, Greece, 21–23 June 2017. Abstract OP-04. [Google Scholar]
- Notter, M.; Vaupel, P. Water-filtered infrared-A hyperthermia & re-irradiation in the treatment of recurrent breast cancer. Strahlenther. Onkol. 2018, 194, S60. [Google Scholar]
- AGO (Arbeitsgemeinschaft Gynäkologische Onkologie) Innerhalb Der Deutschen Gesellschaft Für Gynäkologie Und Geburtshilfe (DGGG) Und Der Deutschen Krebsgesellschaft e.V. (DKG). Guidelines Breast 2019, Version 2019.1, Loco-Regional Recurrence, Page 17 and 19. Available online: https://www.ago-online.de/fileadmin/ago-online/downloads/_leitlinien/2019/PDF_EN/2019E_17_Loco-Regional_Recurrence_with_References.pdf (accessed on 2 March 2020).
- McCormick, B. Counterpoint: Hyperthermia with radiation therapy for chest wall recurrences. J. Natl. Compr. Cancer Netw. 2007, 5, 345–348. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Subgroups | No. of Patients |
|---|---|---|
| Median age (years) | 54 (range: 28–91) | 201 |
| Menopausal status | premenopausal | 57 |
| perimenopausal | 29 | |
| postmenopausal | 113 | |
| n.a. | 2 | |
| T-stage | T1 | 58 |
| T2 | 78 | |
| T3 | 30 | |
| T4 | 34 | |
| TX | 1 | |
| Lymph node involvement | N0 | 65 |
| N1 | 71 | |
| N2 | 35 | |
| N3 | 28 | |
| NX | 2 | |
| Distant metastasis | M1 | 185 |
| M1 | 16 | |
| Histological grading | G1 | 16 |
| G2 | 80 | |
| G3 | 105 | |
| Resection status | R0 | 186 |
| R1 | 15 | |
| Estrogen receptor expression | positive | 124 |
| negative | 27 | |
| Progesterone receptor expression | positive | 109 |
| negative | 42 | |
| Her2/new expression | amplified | 47 |
| missing | 74 | |
| unknown | 30 | |
| Triple negative | 50 |
| Characteristics | Median (Range) | No. of Patients |
|---|---|---|
| Total number of patients | 201 | |
| No. of tumor regions treated | 284 | |
| Age (years) | 65 (31–102) | |
| Interval between initial RT and re-RT (months) | 47 (0–389) | |
| Presence of distant metastasis | 91 | |
| Number of previous recurrences | 2 (1–11) | |
| Previous RT-dose (Gy) | 60 (20–139) | |
| Re-irradiation dose (Gy) | ||
| 4 | 1 | |
| 8 | 2 | |
| 12 | 6 | |
| 16 | 8 | |
| 20 | 177 | |
| 24 | 5 | |
| 25 | 1 | |
| 28 | 1 | |
| No. of previous chemotherapies | ||
| 0 | 32 | |
| 1 | 20 | |
| 2 | 33 | |
| >2 | 116 | |
| No. of previous hormone therapies | ||
| 0 | 83 | |
| 1 | 34 | |
| 2 | 27 | |
| >2 | 57 | |
| No. of previous resections | ||
| 0 | 10 | |
| 1 | 88 | |
| 2 | 59 | |
| >2 | 44 | |
| Tissue transfer | ||
| None | 157 | |
| Meshgraft/skin transplants/reconstruction, etc. | 44 | |
| Anatomic site at the time of recurrence | ||
| Breast | 18 | |
| Chest wall | 131 | |
| Regional lymph nodes | 22 | |
| Regional lymph nodes and chest wall | 30 | |
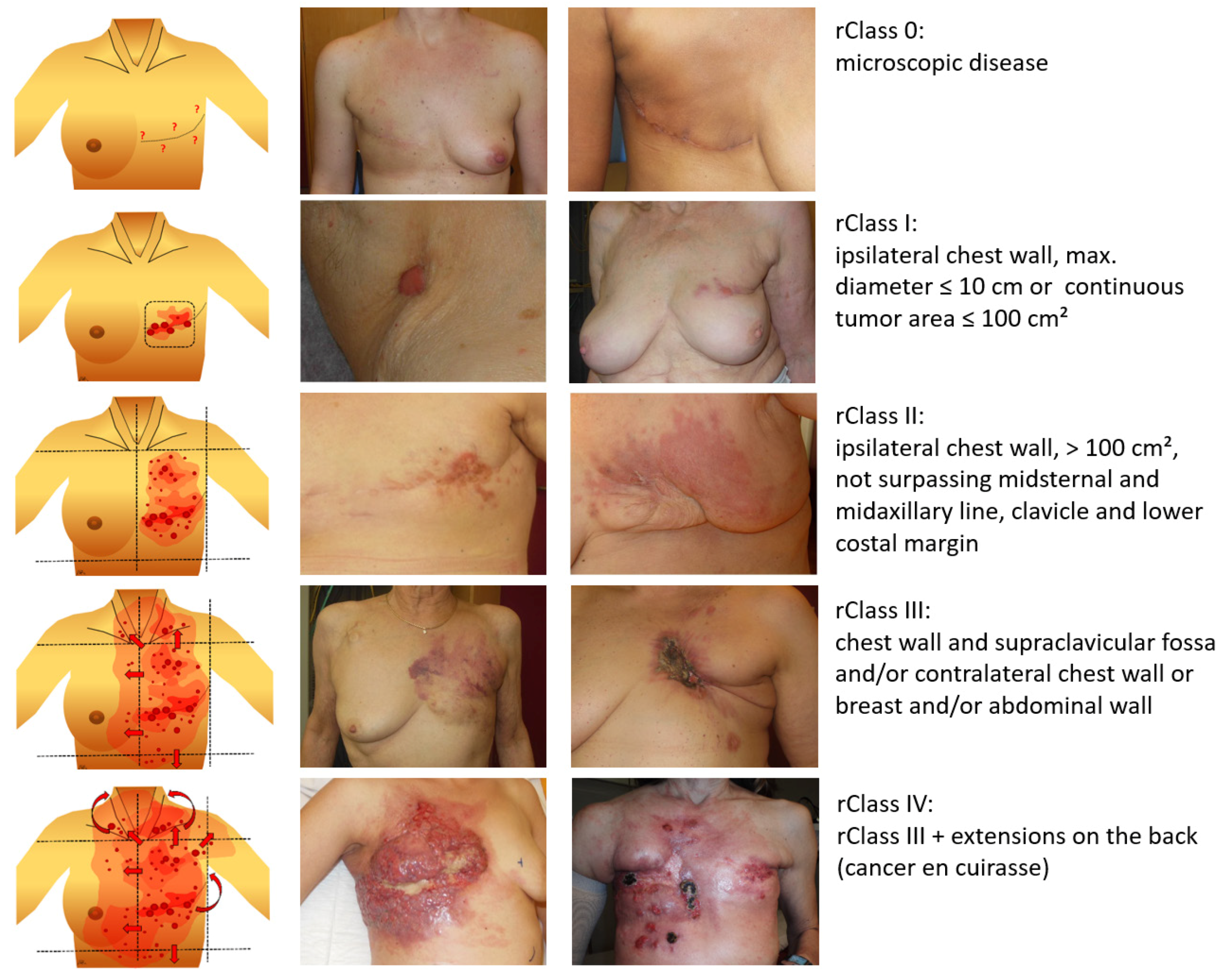
| LRBC extension (classification) | ||
| Microscopic disease: | ||
| rClass 0 | 31 | |
| Macroscopic disease: | 170 | |
| rClass I | 29 | |
| rClass II | 56 | |
| rClass III | 44 | |
| rClass IV | 41 | |
| Gross tumor volume (cm3) | 36 (3–2100) | 39 |
| Tumor size (cm2) | 555 (12–4200) | 142 |
| Lymphangiosis carcinomatosa | ||
| no | 86 | |
| yes | 115 | |
| Ulceration | ||
| no | 131 | |
| yes | 70 |
| Patients | rClass 0 | Macroscopic All | Macroscopic/Size | Macroscopic/Other Factors | ||||
|---|---|---|---|---|---|---|---|---|
| rClass I | rClass II | rClass III | rClass IV | Lymphang | Ulceration | |||
| 31 (100%) | 170 (100%) | 29 (100%) | 56 (100%) | 44 (100%) | 41 (100%) | 115 (100%) | 70 (100%) | |
| CR | 73 (43%) | 22 (76%) | 34 (61%) | 16 (36%) | 1 (2%) | 41 (36%) | 12 (17%) | |
| PR | 88 (52%) | 7 (24%) | 20 (36%) | 27 (61%) | 34 (83%) | 68 (59%) | 52 (74%) | |
| NC | 6 (4%) | 2 (3%) | 4 (10%) | 4 (3%) | 4 (6%) | |||
| PD | 3 (2%) | 1 (2%) | 2 (5%) | 2 (2%) | 2 (3%) | |||
| Patients | rClass 0 | Macroscopic All | Macroscopic/Size Classes | Macroscopic/Other Factors | ||||
|---|---|---|---|---|---|---|---|---|
| rClass I | rClass II | rClass III | rClass IV | Lymphang | Ulceration | |||
| 31 (100%) | 73 (100%) | 22 (100%) | 34 (100%) | 16 (100%) | 1 (100%) | 41 (100%) | 12 (100%) | |
| LC | 21 (68%) | 49 (67%) | 17 (77%) | 21 (62%) | 11 (69%) | 24 (59%) | 7 (58%) | |
| Local re-rec | 2 (6%) | 21 (29%) | 2 (9%) | 13 (38%) | 5 (31%) | 1 (100%) | 17 (41%) | 5 (42%) |
| LFU | 8 (26%) | 3 (4%) | 3 (14%) | |||||
| Patients | Macroscopic All | Macroscopic/Size | Macroscopic/Other Factors | ||||
|---|---|---|---|---|---|---|---|
| rClass I | rClass II | rClass III | rClass IV | Lymphang | Ulceration | ||
| 88 (100%) | 7 (100%) | 20 (100%) | 27 (100%) | 34 (100%) | 68 (100%) | 52 (100%) | |
| Locally progression-free New local progression | 48 (55%) 40 (45%) | 3 (43%) 4 (57%) | 8 (40%) 12 (60%) | 14 (52%) 13 (48%) | 23 (71%) 11 (29%) | 37 (56%) 31 (44%) | 27 (54%) 25 (46%) |
| Characteristics | Re-Recurrences after CR | New Local Progression after PR |
|---|---|---|
| Number of patients | 21 | 40 |
| Number of re-recurrences (fields) | 25 | 53 |
| infield border | 7 18 | 27 26 |
| Number of patients treated with re-HT/re-re-RT | 19 | 24 |
| CR after first re-HT/re-re-RT | 13 | 2 |
| PR after first re-HT/re-re-RT | 6 | 16 |
| NC after first re-HT/re-re-RT | 0 | 4 |
| PD after first re-HT/re-re-RT | 0 | 2 |
| No. of Patients | 201 (100%) |
|---|---|
| No acute side effects Acute side effects Radiodermatitis Grade I Radiodermatitis Grade II Scurfs Hyperpigmentation Burn with blistering | 114 (57%) 87 (43%) 65 4 10 64 1 |
| No chronic side effects Chronic side effects Grade 1: hyperpigmentation Grade 2: new teleangiectasia | 145 (72%) 56 (28%) 53 7 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Notter, M.; Thomsen, A.R.; Nitsche, M.; Hermann, R.M.; Wolff, H.A.; Habl, G.; Münch, K.; Grosu, A.-L.; Vaupel, P. Combined wIRA-Hyperthermia and Hypofractionated Re-Irradiation in the Treatment of Locally Recurrent Breast Cancer: Evaluation of Therapeutic Outcome Based on a Novel Size Classification. Cancers 2020, 12, 606. https://doi.org/10.3390/cancers12030606
Notter M, Thomsen AR, Nitsche M, Hermann RM, Wolff HA, Habl G, Münch K, Grosu A-L, Vaupel P. Combined wIRA-Hyperthermia and Hypofractionated Re-Irradiation in the Treatment of Locally Recurrent Breast Cancer: Evaluation of Therapeutic Outcome Based on a Novel Size Classification. Cancers. 2020; 12(3):606. https://doi.org/10.3390/cancers12030606
Chicago/Turabian StyleNotter, Markus, Andreas R. Thomsen, Mirko Nitsche, Robert M. Hermann, Hendrik A. Wolff, Gregor Habl, Karin Münch, Anca-L. Grosu, and Peter Vaupel. 2020. "Combined wIRA-Hyperthermia and Hypofractionated Re-Irradiation in the Treatment of Locally Recurrent Breast Cancer: Evaluation of Therapeutic Outcome Based on a Novel Size Classification" Cancers 12, no. 3: 606. https://doi.org/10.3390/cancers12030606
APA StyleNotter, M., Thomsen, A. R., Nitsche, M., Hermann, R. M., Wolff, H. A., Habl, G., Münch, K., Grosu, A. -L., & Vaupel, P. (2020). Combined wIRA-Hyperthermia and Hypofractionated Re-Irradiation in the Treatment of Locally Recurrent Breast Cancer: Evaluation of Therapeutic Outcome Based on a Novel Size Classification. Cancers, 12(3), 606. https://doi.org/10.3390/cancers12030606