30 Years of Experience in the Management of Stage III and IV Epithelial Ovarian Cancer: Impact of Surgical Strategies on Survival

 , ,
, ,  ,
,  ,
,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Population Description
2.2. Clinical and Pathological Features
2.3. Statistical Analysis
3. Results
3.1. Clinical and Pathological Features
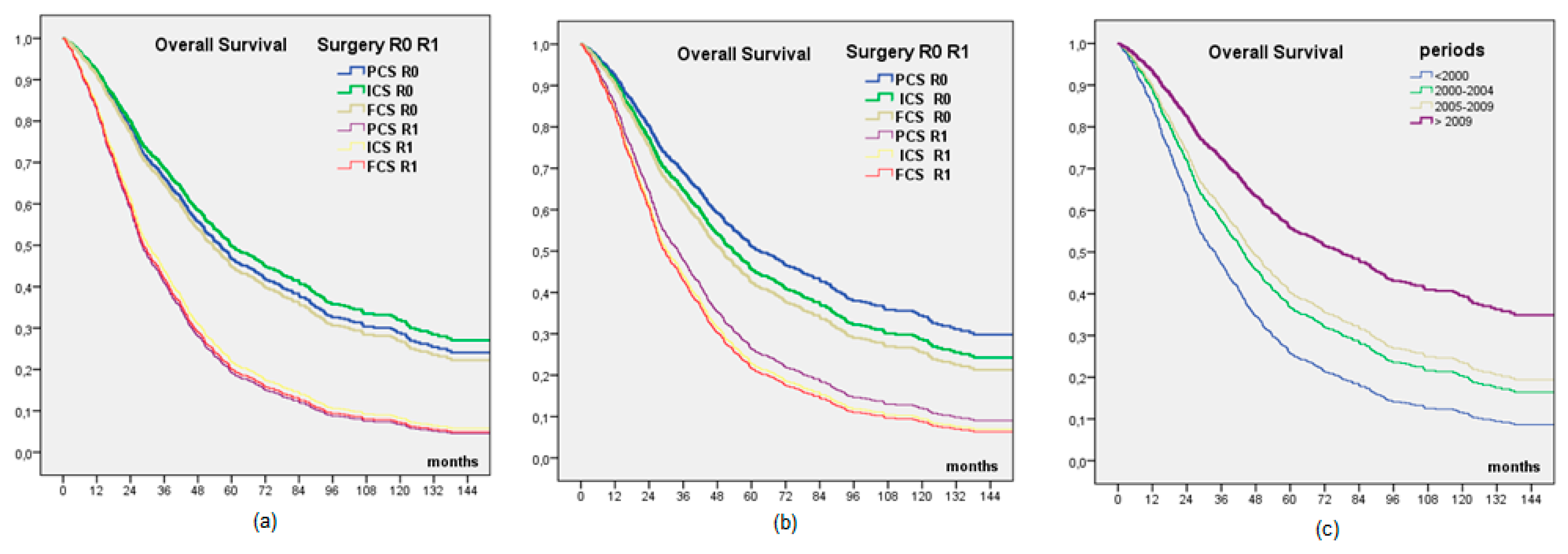
3.2. Survival
3.3. Evolution of Practices
3.4. Multivariate Analysis
4. Discussion
4.1. Residual Disease after Surgery
4.2. Type of Surgery
4.3. Surgical Morbidity
4.4. Limitations
4.5. Future Trials
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

References
- Cancer of the Ovary-SEER Stat Fact Sheets. Available online: http://seer.cancer.gov/statfacts/html/ovary.html (accessed on 6 April 2016).
- Ferlay, J.; Shin, H.-R.; Bray, F.; Forman, D.; Mathers, C.; Parkin, D.M. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int. J. Cancer 2010, 127, 2893–2917. [Google Scholar] [CrossRef] [PubMed]
- Cancer et Environnement. Available online: http://www.ipubli.inserm.fr/handle/10608/76 (accessed on 6 April 2016).
- Prat, J.; FIGO Committee on Gynecologic Oncology. Staging classification for cancer of the ovary, fallopian tube, and peritoneum. Int. J. Gynaecol. Obstet. Off. Organ Int. Fed. Gynaecol. Obstet. 2014, 124, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Chern, J.-Y.; Curtin, J.P. Appropriate Recommendations for Surgical Debulking in Stage IV Ovarian Cancer. Curr. Treat. Options Oncol. 2016, 17, 1. [Google Scholar] [CrossRef] [PubMed]
- Eisenkop, S.M.; Friedman, R.L.; Wang, H.J. Complete cytoreductive surgery is feasible and maximizes survival in patients with advanced epithelial ovarian cancer: A prospective study. Gynecol. Oncol. 1998, 69, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Zivanovic, O.; Eisenhauer, E.L.; Zhou, Q.; Iasonos, A.; Sabbatini, P.; Sonoda, Y.; Abu-Rustum, N.R.; Barakat, R.R.; Chi, D.S. The impact of bulky upper abdominal disease cephalad to the greater omentum on surgical outcome for stage IIIC epithelial ovarian, fallopian tube, and primary peritoneal cancer. Gynecol. Oncol. 2008, 108, 287–292. [Google Scholar] [CrossRef]
- du Bois, A.; Reuss, A.; Pujade-Lauraine, E.; Harter, P.; Ray-Coquard, I.; Pfisterer, J. Role of surgical outcome as prognostic factor in advanced epithelial ovarian cancer: A combined exploratory analysis of 3 prospectively randomized phase 3 multicenter trials: By the Arbeitsgemeinschaft Gynaekologische Onkologie Studiengruppe Ovarialkarzinom (AGO-OVAR) and the Groupe d’Investigateurs Nationaux Pour les Etudes des Cancers de l’Ovaire (GINECO). Cancer 2009, 115, 1234–1244. [Google Scholar]
- Aletti, G.D.; Dowdy, S.C.; Podratz, K.C.; Cliby, W.A. Surgical treatment of diaphragm disease correlates with improved survival in optimally debulked advanced stage ovarian cancer. Gynecol. Oncol. 2006, 100, 283–287. [Google Scholar] [CrossRef]
- Bristow, R.E.; Tomacruz, R.S.; Armstrong, D.K.; Trimble, E.L.; Montz, F.J. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: A meta-analysis. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2002, 20, 1248–1259. [Google Scholar] [CrossRef]
- Chi, D.S.; Eisenhauer, E.L.; Lang, J.; Huh, J.; Haddad, L.; Abu-Rustum, N.R.; Sonoda, Y.; Levine, D.A.; Hensley, M.; Barakat, R.R. What is the optimal goal of primary cytoreductive surgery for bulky stage IIIC epithelial ovarian carcinoma (EOC)? Gynecol. Oncol. 2006, 103, 559–564. [Google Scholar] [CrossRef]
- Olaparib Maintenance Monotherapy in Patients With BRCA Mutated Ovarian Cancer Following First Line Platinum Based Chemotherapy. Available online: https://clinicaltrials.gov/ct2/show/NCT01844986 (accessed on 15 March 2020).
- GOG-0218: Final Overall Survival Results for Addition of Bevacizumab to Chemotherapy in Ovarian Cancer. Available online: https://www.ascopost.com/News/60222 (accessed on 15 March 2020).
- Search of: ICON 7 | Ovarian Cancer-List Results. Available online: https://clinicaltrials.gov/ct2/results?cond=ovarian+cancer&term=ICON+7&cntry=&state=&city=&dist= (accessed on 15 March 2020).
- González-Martín, A.; Pothuri, B.; Vergote, I.; Christensen, R.D.; Graybill, W.; Mirza, M.; McCormick, C.; Lorusso, D.; Hoskins, P.; Freyer, G.; et al. Niraparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2391–2402. [Google Scholar] [CrossRef] [Green Version]
- Vergote, I.; De Wever, I.; Tjalma, W.; Van Gramberen, M.; Decloedt, J.; Van Dam, P. Neoadjuvant chemotherapy or primary debulking surgery in advanced ovarian carcinoma: A retrospective analysis of 285 patients. Gynecol. Oncol. 1998, 71, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Vergote, I.; Tropé, C.G.; Amant, F.; Kristensen, G.B.; Ehlen, T.; Johnson, N.; Verheijen, R.H.; Van Der Burg, M.E.; Lacave, A.J.; Panici, P.B.; et al. Neoadjuvant chemotherapy or primary surgery in stage IIIC or IV ovarian cancer. N. Engl. J. Med. 2010, 363, 943–953. [Google Scholar] [CrossRef] [Green Version]
- Kehoe, S.; Hook, J.; Nankivell, M.; Jayson, G.C.; Kitchener, H.; Lopes, T.; Luesley, D.; Perren, T.; Bannoo, S.; Mascarenhas, M.; et al. Primary chemotherapy versus primary surgery for newly diagnosed advanced ovarian cancer (CHORUS): An open-label, randomised, controlled, non-inferiority trial. Lancet 2015, 386, 249–257. [Google Scholar] [CrossRef]
- van Driel, W.J.; Koole, S.N.; Sikorska, K.; van Leeuwen, J.H.S.; Schreuder, H.W.R.; Hermans, R.H.M.; de Hingh, I.H.J.T.; van der Velden, J.; Arts, H.J.; Massuger, L.F.A.G.; et al. Hyperthermic Intraperitoneal Chemotherapy in Ovarian Cancer. N. Engl. J. Med. 2018, 378, 230–240. [Google Scholar] [CrossRef] [PubMed]
- da Costa Miranda, V.; de Souza Fêde, Â.B.; Dos Anjos, C.H.; da Silva, J.R.; Sanchez, F.B.; da Silva Bessa, L.R.; de Paula Carvalho, J.; Abdo Filho, E.; de Freitas, D.; Diz, M.D. Neoadjuvant chemotherapy with six cycles of carboplatin and paclitaxel in advanced ovarian cancer patients unsuitable for primary surgery: Safety and effectiveness. Gynecol. Oncol. 2014, 132, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Stoeckle, E.; Bourdarias, L.; Guyon, F.; Croce, S.; Brouste, V.; Thomas, L.; Floquet, A. Progress in survival outcomes in patients with advanced ovarian cancer treated by neo-adjuvant platinum/taxane-based chemotherapy and late interval debulking surgery. Ann. Surg. Oncol. 2014, 21, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Classe, J.-M.; Cerato, E.; Boursier, C.; Dauplat, J.; Pomel, C.; Villet, R.; Cuisenier, J.; Lorimier, G.; Rodier, J.F.; Mathevet, P.; et al. Retroperitoneal lymphadenectomy and survival of patients treated for an advanced ovarian cancer: The CARACO trial. J. Gynécologie Obs. Biol. Reprod. 2011, 40, 201–204. [Google Scholar] [CrossRef]
- Luyckx, M.; Leblanc, E.; Filleron, T.; Morice, P.; Darai, E.; Classe, J.M.; Ferron, G.; Stoeckle, E.; Pomel, C.; Vinet, B.; et al. Maximal cytoreduction in patients with FIGO stage IIIC to stage IV ovarian, fallopian, and peritoneal cancer in day-to-day practice: A Retrospective French Multicentric Study. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2012, 22, 1337–1343. [Google Scholar] [CrossRef]
- Winter, W.E.; Maxwell, G.L.; Tian, C.; Sundborg, M.J.; Rose, G.S.; Rose, P.G.; Rubin, S.C.; Muggia, F.; Mcguire, W.P. Tumor residual after surgical cytoreduction in prediction of clinical outcome in stage IV epithelial ovarian cancer: A Gynecologic Oncology Group Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2008, 26, 83–89. [Google Scholar] [CrossRef]
- Bristow, R.E.; Chi, D.S. Platinum-based neoadjuvant chemotherapy and interval surgical cytoreduction for advanced ovarian cancer: A meta-analysis. Gynecol. Oncol. 2006, 103, 1070–1076. [Google Scholar] [CrossRef]
- van Meurs, H.S.; Tajik, P.; Hof, M.H.P.; Vergote, I.; Kenter, G.G.; Mol, B.W.J.; Buist, M.R.; Bossuyt, P.M. Which patients benefit most from primary surgery or neoadjuvant chemotherapy in stage IIIC or IV ovarian cancer? An exploratory analysis of the European Organisation for Research and Treatment of Cancer 55971 randomised trial. Eur. J. Cancer 2013, 49, 3191–3201. [Google Scholar] [CrossRef] [PubMed]
- Vergote, I.; Amant, F.; Kristensen, G.; Ehlen, T.; Reed, N.S.; Casado, A. Primary surgery or neoadjuvant chemotherapy followed by interval debulking surgery in advanced ovarian cancer. Eur. J. Cancer 2011, 47, S88–S92. [Google Scholar] [CrossRef]
- Chi, D.S.; Musa, F.; Dao, F.; Zivanovic, O.; Sonoda, Y.; Leitao, M.M.; Levine, D.A.; Gardner, G.J.; Abu-Rustum, N.R.; Barakat, R.R. An analysis of patients with bulky advanced stage ovarian, tubal, and peritoneal carcinoma treated with primary debulking surgery (PDS) during an identical time period as the randomized EORTC-NCIC trial of PDS vs neoadjuvant chemotherapy (NACT). Gynecol. Oncol. 2012, 124, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Saint Paul de Vence. Available online: http://www.arcagy.org/arcagy-organisation-et-recherche/assets/files/espace-recherche-pdf/saint-paul-de-vence-2016/1-prise-en-charge-multidisciplinaire-premiere-ligne-recommandations.pdf (accessed on 10 April 2016).
- Aletti, G.D.; Eisenhauer, E.L.; Santillan, A.; Axtell, A.; Aletti, G.; Holschneider, C.; Chi, D.S.; Bristow, R.E.; Cliby, W.A. Identification of patient groups at highest risk from traditional approach to ovarian cancer treatment. Gynecol. Oncol. 2011, 120, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Mahner, S.; Eulenburg, C.; Staehle, A.; Wegscheider, K.; Reuss, A.; Pujade-Lauraine, E.; Harter, P.; Ray-Coquard, I.; Pfisterer, J.; du Bois, A. Prognostic impact of the time interval between surgery and chemotherapy in advanced ovarian cancer: Analysis of prospective randomised phase III trials. Eur. J. Cancer 2013, 49, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Tewari, K.S.; Java, J.J.; Eskander, R.N.; Monk, B.J.; Burger, R.A. Early initiation of chemotherapy following complete resection of advanced ovarian cancer associated with improved survival: NRG Oncology/Gynecologic Oncology Group study. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. ESMO 2016, 27, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Eskander, R.; Chang, J.; Ziogas, A.; Anton-Culver, H.; Bristow, R.E. Evaluation of 30-day hospital readmission after surgery for advanced-stage ovarian cancer in a medicare population. J. Clin. Oncol. 2014, 32, 4113–4119. [Google Scholar] [CrossRef] [Green Version]
- Shalowitz, D.I.; Epstein, A.J.; Ko, E.M.; Giuntoli, R.L. Non-surgical management of ovarian cancer: Prevalence and implications. Gynecol. Oncol. 2016, 142, 30–37. [Google Scholar] [CrossRef]
- Kyrgiou, M.; Salanti, G.; Pavlidis, N.; Paraskevaidis, E.; Ioannidis, J.P. Survival benefits with diverse chemotherapy regimens for ovarian cancer: Meta-analysis of multiple treatments. J. Natl. Cancer Inst. 2006, 98, 1655–1663. [Google Scholar] [CrossRef] [Green Version]
- Trial on Radical Upfront Surgery in Advanced Ovarian Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT02828618 (accessed on 12 March 2020).


{kind=link}
{kind=link}
| (a) Comparison of patients depending on surgical strategy. | ||||||||||
| Surgical Strategy | Total | Surgery | No Surgery | |||||||
| PCS | ICS | FCS | Chi 2 | |||||||
| Nb (%) | Nb (%*) | Nb (%*) | Nb (%*) | Nb (%) | p | |||||
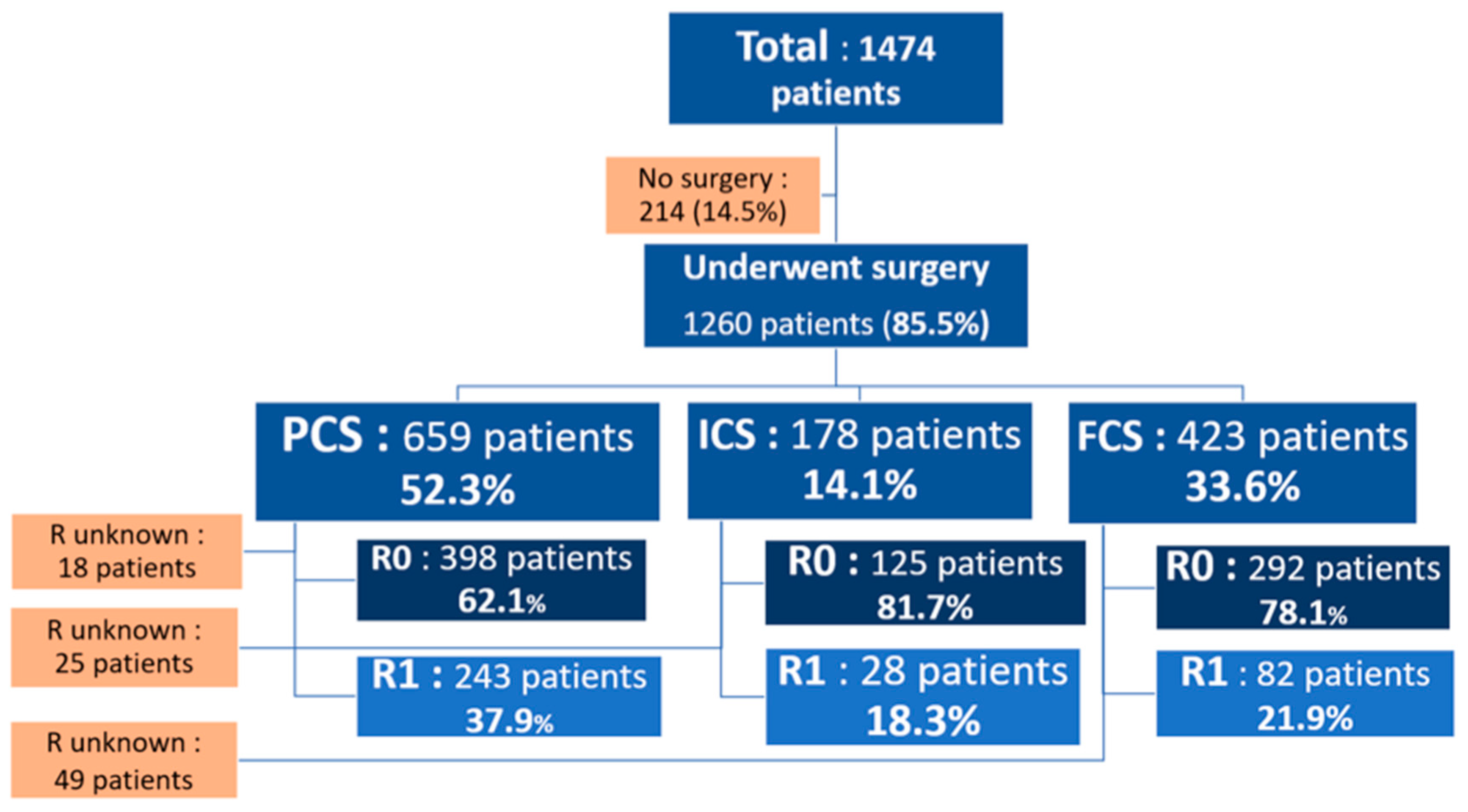
| Number of patients | 1474 | 659 (44.7) | 178 (12.1) | 423(28.7) | 214 (14.5) | |||||
| Age | <50 | 271 (18.4) | 153 (56.6) | 25 (9.2) | 72 (26.6) | 21 (7.7) | <0.0001 | |||
| 50–74 | 1028 (69.7) | 438 (42.6) | 144 (14) | 314 (30.5) | 132 (12.8) | |||||
| > = 75 | 175 (11.9) | 68 (38.9) | 9 (5.1) | 37 (21.1) | 61 (34.9) | |||||
| FIGO Stage | III | 1170 (79.4) | 562 (48) | 149 (12.7) | 317 (27.1) | 142(12.1) | <0.0001 | |||
| IV | 304 (20.6) | 97 (31.9) | 29 (9.5) | 106 (34.9) | 72(23.7) | |||||
| Histological type | Serous | 958 (65.2) | 405 (42.3) | 138 (14.4) | 286 (29.9) | 129(13.5) | <0.0001 | |||
| Mucinous | 90 (6.1) | 59 (65.6) | 3 (3.3) | 12 (13.3) | 16 (17.8) | |||||
| Endometrioid | 105 (7.1) | 68 (64.8) | 7 (6.7) | 24 (22.9) | 6 (5.7) | |||||
| Clear cells | 49 (3.3) | 28 (57.1) | 2 (4.1) | 15 (30.6) | 4 (8.2) | |||||
| other | 124 (8.4) | 32 (25.8) | 20 (16.1) | 44 (35.5) | 28 (22.6) | |||||
| undifferentiated | 113 (7.7) | 47 (41.6) | 7 (6.2) | 30 (26.5) | 29 (25.7) | |||||
| carcinosarcoma | 20 (1.4) | 12 (60) | 1 (5) | 5 (25) | 2 (10) | |||||
| Mixed | 11 (0.7) | 6 (54.5) | 0 (0) | 5 (45.5) | 0 (0) | |||||
| CA 125** | <500 | 125 (40.5) | 85 (48.3) | 12 (28.6) | 28 (30.8) | DM | 0.004 | |||
| 500–1000 | 64 (20.7) | 32 (18.2) | 10 (23.8) | 22 (24.2) | DM | |||||
| >1000 | 120 (38.8) | 59 (33.5) | 20 (47.6) | 41 (45.1) | DM | |||||
| DM | 1165 | |||||||||
| Chemotherapy protocol | Platinum + Taxanes | 1076 (73.0) | 391 (61.8) | 161 (90.4) | 355 (85.5) | 169 (79.3) | <0.0001 | |||
| Other | 363 (24.6) | 242 (38.2) | 17 (9.6) | 60 (14.5) | 44 (20.7) | |||||
| DM | 35 (2.4) | |||||||||
| Cancer Institute | 1 | 685 (46.5) | 189 (27.6) | 128 (18.7) | 271 (39.6) | 97(14.2) | <0.0001 | |||
| 2 | 789 (53.5) | 470 (59.6) | 50 (6.3) | 152 (19.3) | 117(14.8) | |||||
| (b) Comparison of patients depending on residual disease at the end of surgery. | ||||||||||
| Population’s Characteristics | Residual Disease | |||||||||
| No | Yes | Chi 2 | ||||||||
| Missing data (n = 92, 7.3%) | Nb (%) | Nb (%) | p | |||||||
| Surgery | PCS | 18 (2.7%) | 398 (62.1) | 243 (37.9) | <0.0001 | |||||
| ICS | 25 (14%) | 125 (81.7) | 28 (18.3) | |||||||
| FCS | 49 (11.6%) | 292 (78.1) | 82 (21.9) | |||||||
| FIGO Stage | III | 684 (71.2) | 277 (28.8) | 0.016 | ||||||
| IV | 131 (63.3) | 76 (36.7) | ||||||||
| Histological type | Serous | 566 (74.2) | 197 (25.8) | <0.0001 | ||||||
| Mucinous | 30 (42.9) | 40 (57.1) | ||||||||
| Endometrioid | 61 (62.2) | 37 (37.8) | ||||||||
| Clear cells | 29 (72.5) | 11 (27.5) | ||||||||
| other | 63 (73.3) | 23 (27.5) | ||||||||
| undifferentiated | 47 (59.5) | 32 (26.7) | ||||||||
| carcinosarcoma | 10 (55.6) | 8 (44.4) | ||||||||
| Mixed | 6 (60) | 4 (40) | ||||||||
| Periods | <2000 | 165 (49.7) | 167 (50.3) | <0.0001 | ||||||
| 2000–2004 | 144 (64.6) | 79 (35.4) | ||||||||
| 2005–2009 | 193 (77.5) | 56 (22.5) | ||||||||
| >2009 | 313 (86) | 51 (14) | ||||||||
| Age | <50 | 166 (73.1) | 61 (26.9) | 0.167 | ||||||
| 50–74 | 579 (69.8) | 251 (30.2) | ||||||||
| > = 75 | 70 (63.1) | 41 (36.9) | ||||||||
| CA 125 | <500 | 83 (67.5) | 40 (32.5) | 0.368 | ||||||
| 500–1000 | 44 (69.8) | 19 (30.2) | ||||||||
| >1000 | 87 (75.7) | 28 (24.3) | ||||||||
| Survival Outcome | Overall Survival | Progression Free Survival | ||||||
|---|---|---|---|---|---|---|---|---|
| Characteristics | n* | Median of Survival (months) | p | n* | n** PFS < 12 m (%*) | n** PFS > 12m (%*) | p | |
| R0 | 815 | 55.1 | 770 | |||||
| Surgery | PCS | 398 | 59.7 | 0.136 | 376 | 169 (45) | 207 (55) | <0.001 |
| ICS | 125 | 56.0 | 112 | 40 (36) | 72 (64) | |||
| FCS | 292 | 48.6 | 282 | 163 (58) | 119 (42) | |||
| Age | < 50 | 166 | 78.1 | 0.002 | 158 | 65 (41) | 93 (59) | 0.089 |
| 50–74 | 579 | 53.6 | 543 | 269 (50) | 274 (50) | |||
| >= 75 | 70 | 41.7 | 69 | 38 (55) | 31 (45) | |||
| FIGO | III | 684 | 57.2 | 0.005 | 654 | 294 (45) | 360 (55) | <0.001 |
| IV | 131 | 44.9 | 116 | 78 (67) | 38 (33) | |||
| Histological type° | Serous | 566 | 55.8 | 0.012 | 541 | 263 (49) | 278 (51) | 0.163 |
| Mucinous | 30 | 67.1 | 28 | 13 (46) | 15 (54) | |||
| Endometrioid | 61 | 57.9 | 56 | 24 (43) | 32 (57) | |||
| Clear cells | 29 | 33.2 | 26 | 17 (65) | 9 (35) | |||
| other | 63 | 77.8 | 58 | 23 (40) | 35 (60) | |||
| undifferentiated | 47 | 51.8 | 44 | 20 (45) | 24 (55) | |||
| carcinosarcoma | 10 | 49.3 | 10 | 6 (60) | 4 (40) | |||
| Mixed | 6 | 9.6 | 4 | 4 (100) | 0 (0) | |||
| Periods | <2000 | 165 | 47.7 | 0.015 | 154 | 80 (52) | 74 (48) | 0.169 |
| 2000–2004 | 144 | 54.3 | 135 | 54 (40) | 81 (60) | |||
| 2005–2009 | 193 | 59.0 | 189 | 91 (48) | 98 (52) | |||
| >2009 | 313 | 59.3 | 292 | 147 (50) | 145 (50) | |||
| Cancer Institute | 1 | 388 | 61.5 | 0.002 | 366 | 152 (42) | 214 (58) | <0.001 |
| 2 | 427 | 50.6 | 404 | 220 (54) | 184 (46) | |||
| Periods | ||||||
|---|---|---|---|---|---|---|
| <2000 | 2000–2004 | 2005–2009 | >2009 | |||
| Nb (%*) | Nb (%) | Nb (%) | Nb (%) | p | ||
| Surgery | Yes | 401 (89.9) | 240 (90.2) | 253 (87.5) | 366 (77.4) | <0.001 |
| No | 45 (10.1) | 26 (9.8) | 36 (12.5) | 107 (22.6) | ||
| Strategy | PCS | 311 (69.7) | 131 (49.2) | 98 (33.9) | 119 (25.2) | <0.001 |
| ICS | 22 (4.9) | 39 (14.7) | 27 (9.3) | 90 (19.0) | ||
| FCS | 68 (15.2) | 70 (16.5) | 128 (44.3) | 157 (33.2) | ||
| No surgery | 45 (10.1) | 26 (9.8) | 36 (12.5) | 107 (22.6) | ||
| Residual Disease | Yes | 281 (63.0) | 122 (45.9) | 96 (33.2) | 160 (33.8) | <0.001 |
| No | 165 (37.0) | 144 (54.1) | 193 (66.8) | 313 (66.2) | ||
| Chemotherapy protocol | Platinum + Taxanes | 94 (21.1) | 233 (87.9) | 282 (97.5) | 467 (98.7) | <0.001 |
| Other | 329 (73.7) | 25 (9.4) | 6 (2) | 3 (0.1) | ||
| (a) Factors influencing overall survival among R0 patients. | ||||
| Overall Survival | ||||
| HR | IC95% | p | ||
| Surgery | PCS | 1 | ||
| ICS | 1.001 | 0.734–1.366 | 0.994 | |
| FCS | 1.123 | 0.906–1.393 | 0.289 | |
| FIGO Stage | III | 1 | ||
| IV | 1.298 | 0.995–1.694 | 0.054 | |
| Age | < 50 | 1 | ||
| 50–74 | 1.355 | 1.061–1.729 | 0.015 | |
| >= 75 | 1.951 | 1.318–2.888 | 0.001 | |
| Histological type | Serous | 1 | ||
| Mucinous | 0.911 | 0.549–1.513 | 0.719 | |
| Endometrioid | 0.984 | 0.692–1.400 | 0.929 | |
| Clear cells | 1.668 | 1.055–2.638 | 0.029 | |
| other | 0.673 | 0.446–1.014 | 0.058 | |
| undifferentiated | 1.178 | 0.805–1.722 | 0.399 | |
| carcinosarcoma | 1.042 | 0.463–2.344 | 0.921 | |
| Mixed | 2.996 | 1.222–7.344 | 0.016 | |
| (b) Factors influencing progression free survival among R0 patients. | ||||
| PFS | PFS <12 vs. >12 months | |||
| OR | IC95% | p | ||
| Surgery | PCS | 1 | ||
| ICS | 1.526 | 0.982–2.373 | 0.060 | |
| FCS | 0.669 | 0.486–0.921 | 0.014 | |
| FIGO Stage | III | 1 | ||
| IV | 0.441 | 0.288–0.677 | <0.001 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Delga, B.; Classe, J.-M.; Houvenaeghel, G.; Blache, G.; Sabiani, L.; El Hajj, H.; Andrieux, N.; Lambaudie, E. 30 Years of Experience in the Management of Stage III and IV Epithelial Ovarian Cancer: Impact of Surgical Strategies on Survival. Cancers 2020, 12, 768. https://doi.org/10.3390/cancers12030768
Delga B, Classe J-M, Houvenaeghel G, Blache G, Sabiani L, El Hajj H, Andrieux N, Lambaudie E. 30 Years of Experience in the Management of Stage III and IV Epithelial Ovarian Cancer: Impact of Surgical Strategies on Survival. Cancers. 2020; 12(3):768. https://doi.org/10.3390/cancers12030768
Chicago/Turabian StyleDelga, Berenice, Jean-Marc Classe, Gilles Houvenaeghel, Guillaume Blache, Laura Sabiani, Houssein El Hajj, Nicole Andrieux, and Eric Lambaudie. 2020. "30 Years of Experience in the Management of Stage III and IV Epithelial Ovarian Cancer: Impact of Surgical Strategies on Survival" Cancers 12, no. 3: 768. https://doi.org/10.3390/cancers12030768
APA StyleDelga, B., Classe, J. -M., Houvenaeghel, G., Blache, G., Sabiani, L., El Hajj, H., Andrieux, N., & Lambaudie, E. (2020). 30 Years of Experience in the Management of Stage III and IV Epithelial Ovarian Cancer: Impact of Surgical Strategies on Survival. Cancers, 12(3), 768. https://doi.org/10.3390/cancers12030768