Therapy of Sporadic and NF2-Related Vestibular Schwannoma


Abstract
:1. Introduction
2. Pathophysiology of VS
2.1. The Normal Structure and Function of the NF2 Gene
2.2. Pathophysiology of Sporadic Form
2.3. Pathophysiology of NF2 VS
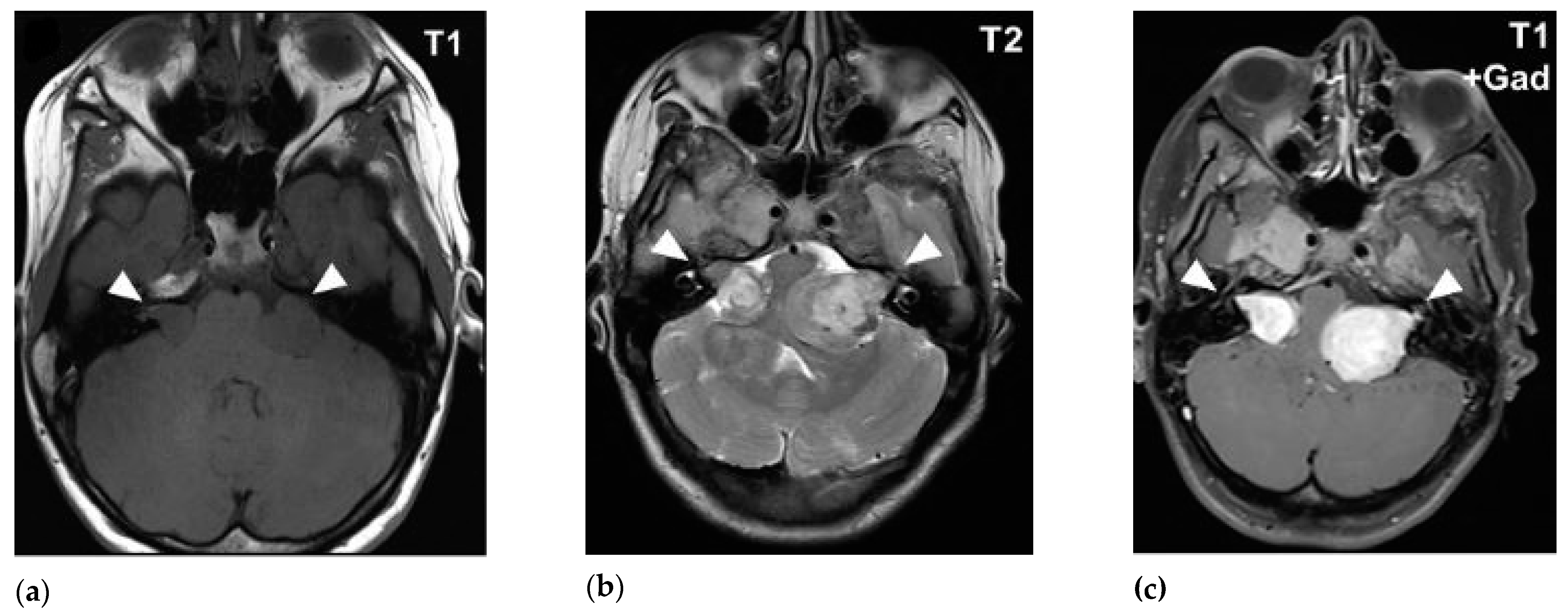
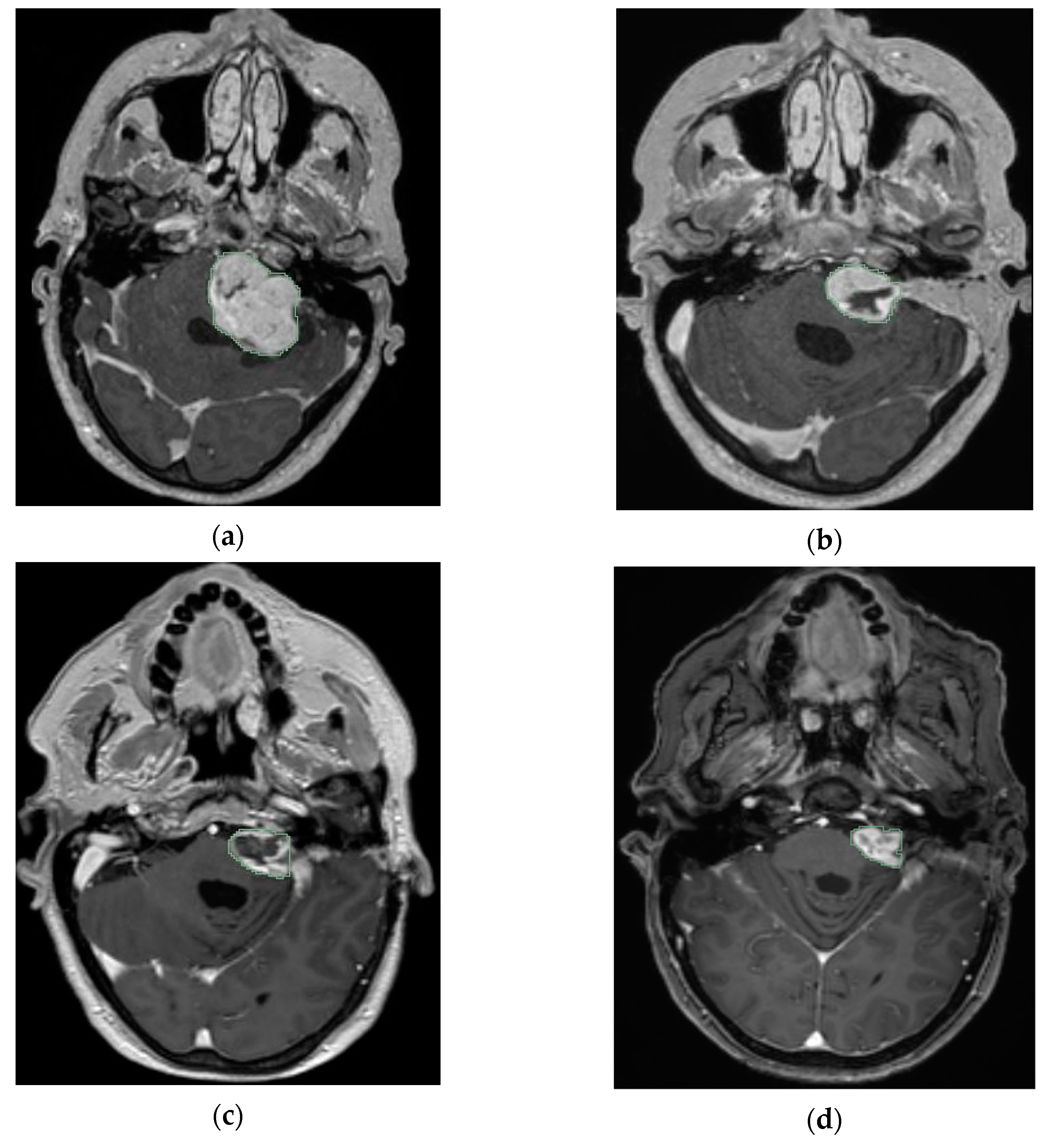
3. Imaging of VS
4. Management of Sporadic VS and NF2 VS
4.1. Sporadic VS
4.2. NF2 VS
5. Radiotherapy
5.1. NF2 VS and Radiotherapy
5.2. Sporadic VS and Radiotherapy
5.2.1. Primary Radiotherapy in Small to Medium VS
5.2.2. Primary Radiotherapy in Large VS
5.3. Planned Radiotherapy After Subtotal Resection in Large VS
5.4. Radiation-Induced Effects After Radiotherapy in Both VS and NF2 VS
6. Medical Therapy and NF2 VS
7. Conclusions
Funding
Conflicts of Interest
References
- Niknafs, Y.S.; Wang, A.C.; Than, K.D.; Etame, A.B.; Thompson, B.G.; Sullivan, S.E. Hemorrhagic vestibular schwannoma: review of the literature. World Neurosurg. 2014, 82, 751–756. [Google Scholar] [CrossRef] [PubMed]
- Halliday, J.; Rutherford, S.A.; McCabe, M.G.; Evans, D.G. An update on the diagnosis and treatment of vestibular schwannoma. Expert Rev. Neurother. 2018, 18, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Kaul, V.; Cosetti, M.K. Management of Vestibular Schwannoma (Including NF2): Facial nerve considerations. Otolaryngol. Clin. N. Am. 2018, 51, 1193–1212. [Google Scholar] [CrossRef] [PubMed]
- Greene, J.; Al-Dhahir, M.A. Acoustic Neuroma (Vestibular Schwannoma). In StatPearls, Treasure Island (FL): StatPearls. Available online: https://www.ncbi.nlm.nih.gov/books/NBK470177/ (accessed on 16 December 2019).
- Hadfield, K.D.; Smith, M.J.; Urquhart, J.E.; Wallace, A.J.; Bowers, N.L.; King, A.T.; Rutherford, S.A.; Trump, D.; Newman, W.G.; Evans, D.G. Rates of loss of heterozygosity and mitotic recombination in NF2 schwannomas, sporadic vestibular schwannomas and schwannomatosis schwannomas. Oncogene 2010, 29, 6216–6221. [Google Scholar] [CrossRef] [Green Version]
- De Carvalho, R.M.; Sant’anna, C.D.C.; Pinto, G.R.; Paschoal, E.H.A.; Tuji, F.M.; Borges, B.D.N.; Soares, P.C., Jr.; Rey, J.A.; Chaves, L.C.L.; Burbano, R.R. Frequency of the loss of heterozygosity of the NF2 gene in sporadic spinal schwannomas. Anticancer Res. 2018, 38, 2149–2154. [Google Scholar] [CrossRef]
- Heineman, T.E.; Evans, D.G.; Campagne, F.; Selesnick, S.H. In silico analysis of NF2 gene missense mutations in neurofibromatosis type 2: from genotype to phenotype. Otol. Neurotol. 2015, 36, 908–914. [Google Scholar] [CrossRef]
- Sass, H.C.; Borup, R.; Alanin, M.; Nielsen, F.C.; Caye-Thomasen, P. Gene expression, signal transduction pathways and functional networks associated with growth of sporadic vestibular schwannomas. J. Neurooncol. 2017, 131, 283–292. [Google Scholar] [CrossRef]
- De Vries, M.; Briaire-de Bruijn, I.; Malessy, M.J.; De Bruine, S.F.; Van der Mey, A.G.; Hogendoorn, P.C. Tumor-associated macrophages are related to volumetric growth of vestibular schwannomas. Otol. Neurotol. 2013, 34, 347–352. [Google Scholar] [CrossRef]
- Archibald, D.J.; Neff, B.A.; Voss, S.G.; Splinter, P.L.; Driscoll, C.L.; Link, M.J.; Dong, H.; Kwon, E.D. B7-H1 expression in vestibular schwannomas. Otol. Neurotol. 2010, 31, 991–997. [Google Scholar] [CrossRef] [Green Version]
- Torres-Martin, M.; Lassaletta, L.; de Campos, J.M.; Isla, A.; Pinto, G.R.; Burbano, R.R.; Melendez, B.; Castresana, J.S.; Rey, J.A. Genome-wide methylation analysis in vestibular schwannomas shows putative mechanisms of gene expression modulation and global hypomethylation at the HOX gene cluster. Genes Chromosomes Cancer 2015, 54, 197–209. [Google Scholar] [CrossRef]
- Chen, Y.; Wang, Z.Y.; Wu, H. P14ARF deficiency and its correlation with overexpression of p53/MDM2 in sporadic vestibular schwannomas. Eur. Arch. Otorhinolaryngol. 2015, 272, 2227–2234. [Google Scholar] [CrossRef] [PubMed]
- Taurone, S.; Bianchi, E.; Attanasio, G.; Di Gioia, C.; Ierino, R.; Carubbi, C.; Galli, D.; Pastore, F.S.; Giangaspero, F.; Filipo, R.; et al. Immunohistochemical profile of cytokines and growth factors expressed in vestibular schwannoma and in normal vestibular nerve tissue. Mol. Med. Rep. 2015, 12, 737–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, B.; Cui, Z.; Zhong, Z.; Sun, Y.; Yang, G.Y.; Sun, Q.; Bian, L. The role and regulatory mechanism of IL-1beta on the methylation of the NF2 gene in benign meningiomas and leptomeninges. Mol. Carcinog. 2016, 55, 2268–2277. [Google Scholar] [CrossRef] [PubMed]
- De Vries, W.M.; Briaire-de Bruijn, I.H.; van Benthem, P.P.G.; van der Mey, A.G.L.; Hogendoorn, P.C.W. M-CSF and IL-34 expression as indicators for growth in sporadic vestibular schwannoma. Virchows Arch. 2018. [Google Scholar] [CrossRef] [Green Version]
- Morrow, K.A.; Shevde, L.A. Merlin: the wizard requires protein stability to function as a tumor suppressor. Biochim. Biophys. Acta 2012, 1826, 400–406. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Xue, L.; Wang, H.; Wang, Z.; Wu, H. Differential NF2 Gene Status in Sporadic Vestibular Schwannomas and its Prognostic Impact on Tumour Growth Patterns. Sci. Rep. 2017, 7, 5470. [Google Scholar] [CrossRef] [Green Version]
- Su, F.; Zhou, Z.; Su, W.; Wang, Z.; Wu, Q. A novel alternative splicing isoform of NF2 identified in human Schwann cells. Oncol. Lett. 2016, 12, 977–982. [Google Scholar] [CrossRef] [Green Version]
- Lopez, E.W.; Vue, Z.; Broaddus, R.R.; Behringer, R.R.; Gladden, A.B. The ERM family member Merlin is required for endometrial gland morphogenesis. Dev. Bio. 2018, 442, 301–314. [Google Scholar] [CrossRef]
- Sabra, H.; Brunner, M.; Mandati, V.; Wehrle-Haller, B.; Lallemand, D.; Ribba, A.-S.; Chevalier, G.; Guardiola, P.; Block, M.R.; Bouvard, D. β1 integrin–dependent Rac/group I PAK signaling mediates YAP activation of Yes-associated protein 1 (YAP1) via NF2/merlin. J. Biol. Chem. 2017, 292, 19179. [Google Scholar] [CrossRef] [Green Version]
- Sato, T.; Sekido, Y. NF2/Merlin inactivation and potential therapeutic targets in mesothelioma. Int. J. Mol. Sci. 2018, 19, 988. [Google Scholar] [CrossRef] [Green Version]
- De Vries, M.; van der Mey, A.G.; Hogendoorn, P.C. Tumor biology of vestibular schwannoma: a review of experimental data on the determinants of tumor genesis and growth characteristics. Otol. Neurotol. 2015, 36, 1128–1136. [Google Scholar] [CrossRef] [PubMed]
- Terawaki, S.; Kitano, K.; Aoyama, M.; Mori, T.; Hakoshima, T. MT1-MMP recognition by ERM proteins and its implication in CD44 shedding. Genes Cells 2015, 20, 847–859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morrison, H.; Sperka, T.; Manent, J.; Giovannini, M.; Ponta, H.; Herrlich, P. Merlin/neurofibromatosis type 2 suppresses growth by inhibiting the activation of Ras and Rac. Cancer Res. 2007, 67, 520–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, J.H.; Oh, A.Y.; Park, S.; Kang, S.M.; Yoon, M.H.; Woo, T.G.; Hong, S.D.; Hwang, J.; Ha, N.C.; Lee, H.Y.; et al. Loss of NF2 induces TGF beta receptor 1-mediated noncanonical and oncogenic TGF beta signaling: implication of the therapeutic effect of tgfbeta receptor 1 inhibitor on nf2 syndrome. Mol. Cancer Ther. 2018, 17, 2271–2284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlson, M.L.; Smadbeck, J.B.; Link, M.J.; Klee, E.W.; Vasmatzis, G.; Schimmenti, L.A. Next generation sequencing of sporadic vestibular schwannoma: necessity of biallelic NF2 inactivation and implications of accessory non-NF2 variants. Otol. Neurotol. 2018, 39, e860–e871. [Google Scholar] [CrossRef]
- Lassaletta, L.; Torres-Martín, M.; Peña-Granero, C.; Roda, J.M.; Santa-Cruz-Ruiz, S.; Castresana, J.S.; Gavilan, J.; Rey, J.A. NF2 genetic alterations in sporadic vestibular schwannomas: clinical implications. Otol. Neurotol. 2013, 34, 1355–1361. [Google Scholar] [CrossRef] [Green Version]
- Lassaletta, L.; Aristegui, M.; Medina, M.; Aranguez, G.; Perez-Mora, R.M.; Falcioni, M.; Gavilan, J.; Piazza, P.; Sanna, M. Ipsilateral cochlear implantation in patients with sporadic vestibular schwannoma in the only or best hearing ear and in patients with NF2. Eur. Arch. Otorhinolaryngol. 2016, 273, 27–35. [Google Scholar] [CrossRef]
- Roche, P.H.; Bouvier, C.; Chinot, O.; Figarella-Branger, D. Genesis and biology of vestibular schwannomas. Prog. Neurol. Surg. 2008, 21, 24–31. [Google Scholar] [CrossRef]
- Welling, D.B.; Guida, M.; Goll, F.; Pearl, D.K.; Glasscock, M.E.; Pappas, D.G.; Linthicum, F.H.; Rogers, D.; Prior, T.W. Mutational spectrum in the neurofibromatosis type 2 gene in sporadic and familial schwannomas. Hum. Genet. 1996, 98, 189–193. [Google Scholar] [CrossRef]
- Diebold, R.; Bartelt-Kirbach, B.; Evans, D.G.; Kaufmann, D.; Hanemann, C.O. Sensitive detection of deletions of one or more exons in the neurofibromatosis type 2 (NF2) gene by multiplexed gene dosage polymerase chain reaction. J. Mol. Diagn. 2005, 7, 97–104. [Google Scholar] [CrossRef] [Green Version]
- Hino, O.; Kobayashi, T. Mourning Dr. Alfred, G. Knudson: the two-hit hypothesis, tumor suppressor genes, and the tuberous sclerosis complex. Cancer Sci. 2017, 108, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Xue, L.; Huang, H.; Wang, H.; Zhang, X.; Zhu, W.; Wang, Z.; Wang, Z.; Wu, H.J.E. Synergistic effect of Nutlin-3 combined with MG-132 on schwannoma cells through restoration of merlin and p53 tumour suppressors. EBioMedicine 2018, 36, 252–265. [Google Scholar] [CrossRef] [PubMed]
- Koutsimpelas, D.; Ruerup, G.; Mann, W.J.; Brieger, J. Lack of neurofibromatosis type 2 gene promoter methylation in sporadic vestibular schwannomas. ORL J. Otorhinolaryngol. Relat. Spec. 2012, 74, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Klutstein, M.; Nejman, D.; Greenfield, R.; Cedar, H.J.C.r. DNA methylation in cancer and aging. Cancer Res. 2016, 76, 3446–3450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hexter, A.T.; Evans, D.G. The genetics of vestibular schwannoma. Curr. Otorhinolaryngol. Rep. 2014, 2, 226–234. [Google Scholar] [CrossRef] [Green Version]
- Kino, T.; Takeshima, H.; Nakao, M.; Nishi, T.; Yamamoto, K.; Kimura, T.; Saito, Y.; Kochi, M.; Kuratsu, J.; Saya, H.; et al. Identification of the cis-acting region in the NF2 gene promoter as a potential target for mutation and methylation-dependent silencing in schwannoma. Genes Cells 2001, 6, 441–454. [Google Scholar] [CrossRef]
- Aarhus, M.; Bruland, O.; Sætran, H.A.; Mork, S.J.; Lund-Johansen, M.; Knappskog, P.M. Global gene expression profiling and tissue microarray reveal novel candidate genes and down-regulation of the tumor suppressor gene CAV1 in sporadic vestibular schwannomas. Neurosurgery 2010, 67, 998–1019. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.D.; Kwon, T.J.; Kim, U.K.; Lee, W.S. Genetic and epigenetic alterations of the NF2 gene in sporadic vestibular schwannomas. PLoS ONE 2012, 7, e30418. [Google Scholar] [CrossRef]
- Kresak, J.L.; Walsh, M. Neurofibromatosis: A review of NF1, NF2, and schwannomatosis. J. Pediatr. Genet. 2016, 5, 98–104. [Google Scholar]
- Evans, D.G. Neurofibromatosis type 2 (NF2): A clinical and molecular review. Orphanet J. Rare Dis. 2009, 4, 16. [Google Scholar] [CrossRef] [Green Version]
- Asthagiri, A.R.; Parry, D.M.; Butman, J.A.; Kim, H.J.; Tsilou, E.T.; Zhuang, Z.; Lonser, R.R. Neurofibromatosis type 2. Lancet 2009, 373, 1974–1986. [Google Scholar] [CrossRef] [Green Version]
- Ardern-Holmes, S.; Fisher, G.; North, K. Neurofibromatosis type 2: Presentation, major complications, and management, with a focus on the pediatric age group. J. Child Neurol. 2017, 32, 9–22. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.G.R.; Sainio, M.; Baser, M.E. Neurofibromatosis type 2. J. Med. Genet. 2000, 37, 897–904. [Google Scholar] [CrossRef] [PubMed]
- Bijlsma, EK.; Wallace, AJ.; Evans, DG. Misleading linkage results in an NF2 presymptomatic test owing to mosaicism. J. Med. Genet. 1997, 34, 934–936. [Google Scholar] [CrossRef] [Green Version]
- Bourn, D.; Carter, SA.; Evans, DG.; Goodship, J.; Coakham, H.; Strachan, T. A mutation in the neurofibromatosis type 2 tumor-suppressor gene, giving rise to widely different clinical phenotypes in two unrelated individuals. Am. J. Hum. Genet. 1994, 55, 69–73. [Google Scholar] [PubMed]
- Bonne, N.X.; Aboukais, R.; Baroncini, M.; Hochart, A.; Leblond, P.; Broly, F.; Dubrulle, F.; Lejeune, J.P.; Vincent, C. Pediatric neurofibromatosis type 2: Clinical and molecular presentation, management of vestibular schwannomas, and hearing rehabilitation. Childs Nerv. Syst. 2016, 32, 2403–2413. [Google Scholar] [CrossRef]
- Evans, D.G.; Ramsden, R.T.; Gokhale, C.; Bowers, N.; Huson, S.M.; Wallace, A. Should NF2 mutation screening be undertaken in patients with an apparently isolated vestibular schwannoma? Clin. Genet. 2007, 71, 354–358. [Google Scholar] [CrossRef]
- Dombi, E.; Ardern-Holmes, S.L.; Babovic-Vuksanovic, D.; Barker, F.G.; Connor, S.; Evans, D.G.; Fisher, M.J.; Goutagny, S.; Harris, G.J.; Jaramillo, D.; et al. Recommendations for imaging tumor response in neurofibromatosis clinical trials. Neurology 2013, 19, S33–S40. [Google Scholar] [CrossRef] [Green Version]
- Kocaoglu, M.; Bulakbasi, N.; Ucoz, T.; Ustunsoz, B.; Pabuscu, Y.; Tayfun, C.; Somuncu, I. Comparison of contrast-enhanced T1-weighted and 3D constructive interference in steady state images for predicting outcome after hearing-preservation surgery for vestibular schwannoma. Neuroradiology 2003, 45, 476–481. [Google Scholar] [CrossRef]
- Forgues, M.; Mehta, R.; Anderson, D.; Morel, C.; Miller, L.; Sevy, A.; Son, L.; Arriaga, M. Non-contrast magnetic resonance imaging for monitoring patients with acoustic neuroma. J. Laryngol. Otol. 2018, 132, 780–785. [Google Scholar] [CrossRef]
- Hentschel, M.; Scholte, M.; Steens, S.; Kunst, H.; Rovers, M. The diagnostic accuracy of non-imaging screening protocols for vestibular schwannoma in patients with asymmetrical hearing loss and/or unilateral audiovestibular dysfunction: a diagnostic review and meta-analysis. Clin. Otolaryngol. 2017, 42, 815–823. [Google Scholar] [CrossRef]
- Coy, S.; Rashid, R.; Stemmer-Rachamimov, A.; Santagata, S. An update on the CNS manifestations of neurofibromatosis type 2. Acta Neuropathol. 2019. [Google Scholar] [CrossRef] [Green Version]
- Carlson, M.L.; Tombers, N.M.; Driscoll, C.L.; Van Gompel, J.J.; Lane, J.I.; Raghunathan, A.; Flemming, K.D.; Link, M.J. Clinically significant intratumoral hemorrhage in patients with vestibular schwannoma. Laryngoscope 2017, 127, 1420–1426. [Google Scholar] [CrossRef]
- Strasilla, C.; Sychra, V. Imaging-based diagnosis of vestibular schwannoma. HNO 2017, 65, 373–380. [Google Scholar] [CrossRef]
- Kulkarni, B.S.N.; Bajwa, H.; Chandrashekhar, M.; Sharma, S.D.; Singareddy, R.; Gudipudi, D.; Ahmad, S.; Kumar, A.; Sresty, N.M.; Raju, A.K. CT-and MRI-based gross target volume comparison in vestibular schwannomas. Rep. Pract. Oncol. Radiother. 2017, 22, 201–208. [Google Scholar] [CrossRef] [Green Version]
- Klijn, S.; Verheul, J.B.; Beute, G.N.; Leenstra, S.; Mulder, J.J.; Kunst, H.P.; Hanssens, P.E. Gamma Knife radiosurgery for vestibular schwannomas: Evaluation of tumor control and its predictors in a large patient cohort in The Netherlands. J. Neurosurg. 2016, 124, 1619–1626. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.; Liu, J.; Zhang, Y.; Richard, S.A. Tumor-associated hemorrhage in patients with vestibular schwannoma. Acta Neurochir. 2018. [Google Scholar] [CrossRef]
- Miki, S.; Ishikawa, E.; Yamamoto, T.; Akutsu, H.; Matsuda, M.; Sakamoto, N.; Matsumura, A. Extreme volume expansion of a vestibular schwannoma due to intratumoral hemorrhage after gamma knife radiosurgery. J. Clin. Neurosci. 2015, 22, 1196–1199. [Google Scholar] [CrossRef]
- Crist, J.; Hodge, J.R.; Frick, M.; Leung, F.P.; Hsu, E.; Gi, M.T.; Venkatesh, S.K. Magnetic resonance imaging appearance of schwannomas from head to toe: A pictorial review. J. Clin. Imaging Sci. 2017, 7, 38. [Google Scholar] [CrossRef]
- Ocak, P.E.; Dogan, I.; Ocak, U.; Dinc, C.; Başkaya, M.K. Facial nerve outcome and extent of resection in cystic versus solid vestibular schwannomas in radiosurgery era. Neurosurg. Focus 2018, 44, E3. [Google Scholar] [CrossRef] [Green Version]
- Chu, M.; Wei, L.L.; Li, G.Z.; Lin, Y.Z.; Zhao, S.G. Bilateral acoustic neurinomas presenting as subarachnoid hemorrhage: case report. Chin. Med. J. 2007, 120, 83–84. [Google Scholar] [CrossRef]
- Coelho, D.H.; Tang, Y.; Suddarth, B.; Mamdani, M. MRI surveillance of vestibular schwannomas without contrast enhancement: Clinical and economic evaluation. Laryngoscope 2018, 128, 202–209. [Google Scholar] [CrossRef]
- Zhang, Z.; Wang, Z.; Huang, Q.; Yang, J.; Wu, H. Removal of large or giant sporadic vestibular schwannomas via translabyrinthine approach: A report of 115 cases. ORL 2012, 74, 271–277. [Google Scholar] [CrossRef]
- Dandinarasaiah, M.; Prasad, S.C.; Piccirillo, E.; Vashishth, A.; Valentina, M.; Grinblat, G.; Codreanu, C.M.; Sanna, M. Facial nerve outcomes following total excision of vestibular schwannoma by the enlarged translabyrinthine approach. Otol. Neurotol. 2019, 40, 226–235. [Google Scholar] [CrossRef]
- Torres, R.; Nguyen, Y.; Vanier, A.; Smail, M.; Ferrary, E.; Sterkers, O.; Kalamarides, M.; Bernardeschi, D. Multivariate analysis of factors influencing facial nerve outcome following microsurgical resection of vestibular schwannoma. Otolaryngol. Head Neck Surg. 2017, 156, 525–533. [Google Scholar] [CrossRef]
- Tawfik, K.O.; Walters, Z.A.; Kohlberg, G.D.; Lipschitz, N.; Breen, J.T.; O’Neal, K.; Zuccarello, M.; Samy, R.N. Impact of Motor-Evoked Potential Monitoring on Facial Nerve Outcomes after Vestibular Schwannoma Resection. Ann. Otol. Rhinol. Laryngol. 2019, 128, 56–61. [Google Scholar] [CrossRef]
- Moffat, D.A.; Parker, R.A.; Hardy, D.G.; Macfarlane, R. Factors affecting final facial nerve outcome following vestibular schwannoma surgery. J. Laryngol. Otol. 2014, 128, 406–415. [Google Scholar] [CrossRef]
- Kunert, P.; Dziedzic, T.; Podgorska, A.; Nowak, A.; Czernicki, T.; Marchel, A. Surgery for sporadic vestibular schwannoma. Part IV. Predictive factors influencing facial nerve function after surgery. Neurol. Neurochir. Pol. 2016, 50, 36–44. [Google Scholar] [CrossRef]
- Bernardeschi, D.; Pyatigorskaya, N.; Vanier, A.; Bielle, F.; Smail, M.; Lamas, G.; Sterkers, O.; Kalamarides, M. Role of electrophysiology in guiding near-total resection for preservation of facial nerve function in the surgical treatment of large vestibular schwannomas. J. Neurosurg. 2018, 128, 903–910. [Google Scholar] [CrossRef] [Green Version]
- Carlson, M.L.; Link, M.J.; Wanna, G.B.; Driscoll, C.L. Management of sporadic vestibular schwannoma. Otolaryngol. Clin. N. Am. 2015, 48, 407–422. [Google Scholar] [CrossRef]
- Wise, S.C.; Carlson, M.L.; Tveiten, O.V.; Driscoll, C.L.; Myrseth, E.; Lund-Johansen, M.; Link, M.J. Surgical salvage of recurrent vestibular schwannoma following prior stereotactic radiosurgery. Laryngoscope 2016, 126, 2580–2586. [Google Scholar] [CrossRef]
- Jiang, N.; Wang, Z.; Chen, W.; Xie, Y.; Peng, Z.; Yuan, J.; Wanggou, S.; Su, Y.; Li, X.; Yuan, X. Microsurgical Outcomes After Gross Total Resection on Vestibular Schwannoma in Elderly Patients: A Matched Cohort Study. World Neurosurg. 2017, 101, 457–465. [Google Scholar] [CrossRef]
- Nakatomi, H.; Jacob, J.T.; Carlson, M.L.; Tanaka, S.; Tanaka, M.; Saito, N.; Lohse, C.M.; Driscoll, C.L.W.; Link, M.J. Long-term risk of recurrence and regrowth after gross-total and subtotal resection of sporadic vestibular schwannoma. J. Neurosurg. 2017, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Jacob, J.T.; Carlson, M.L.; Driscoll, C.L.; Link, M.J. Volumetric analysis of tumor control following subtotal and near-total resection of vestibular schwannoma. Laryngoscope 2016, 126, 1877–1882. [Google Scholar] [CrossRef]
- Chen, Z.; Prasad, S.C.; Di Lella, F.; Medina, M.; Piccirillo, E.; Taibah, A.; Russo, A.; Yin, S.; Sanna, M. The behavior of residual tumors and facial nerve outcomes after incomplete excision of vestibular schwannomas. J. Neurosurg. 2014, 120, 1278–1287. [Google Scholar] [CrossRef]
- Xia, Y.; Zhang, W.; Li, Y.; Ma, X.; Liu, Q.; Shi, J. The transotic approach for vestibular schwannoma: indications and results. Eur. Arch. Otorhinolaryngol. 2017, 274, 3041–3047. [Google Scholar] [CrossRef] [Green Version]
- Broomfield, S.J.; Mandavia, A.K.; Nicholson, J.S.; Mahmoud, O.; King, A.T.; Rutherford, S.A.; Ramsden, R.T. Long-term quality of life following vestibular schwannoma excision via the translabyrinthine approach. Otol. Neurotol. 2017, 38, 1165–1173. [Google Scholar] [CrossRef] [Green Version]
- Arriaga, M.A.; Lin, J. Translabyrinthine approach: indications, techniques, and results. Otolaryngol. Clin. N. Am. 2012, 45, 399–415. [Google Scholar] [CrossRef]
- Obaid, S.; Nikolaidis, I.; Alzahrani, M.; Moumdjian, R.; Saliba, I. Morbidity rate of the retrosigmoid versus translabyrinthine approach for vestibular schwannoma resection. J. Audiol. Otol. 2018, 22, 236–243. [Google Scholar] [CrossRef]
- Zhu, Z.J.; Zhu, W.D.; Chen, H.S.; Wang, Z.Y.; Wu, H. Decision making in dissection range of temporal bone: refinements to enlarged translabyrinthine approach. Eur. Arch. Otorhinolaryngol. 2016, 273, 1115–1121. [Google Scholar] [CrossRef]
- Akakpo, K.; Riggs, W.J.; Harris, M.S.; Dodson, E.E. Hearing preservation after translabyrinthine vestibular schwannoma excision: audiometry and electrocochleography results. Ann. Otol. Rhinol. Laryngol. 2018, 127, 563–567. [Google Scholar] [CrossRef]
- Blakeley, J.O.; Evans, D.G.; Adler, J.; Brackmann, D.; Chen, R.; Ferner, R.E.; Hanemann, C.O.; Harris, G.; Huson, S.M.; Jacob, A.; et al. Consensus recommendations for current treatments and accelerating clinical trials for patients with neurofibromatosis type 2. Am. J. Med. Genet. A 2012, 24–41. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, T.H.; McCormick, P.C. Intramedullary ependymomas: clinical presentation, surgical treatment strategies and prognosis. J. Neurooncol. 2000, 47, 211–218. [Google Scholar] [CrossRef]
- Lloyd, S.K.; Evans, D.G. Neurofibromatosis type 2 (NF2): Diagnosis and management. Handb. Clin. Neurol. 2013, 115, 957–967. [Google Scholar] [CrossRef]
- Nowak, A.; Dziedzic, T.; Czernicki, T.; Kunert, P.; Morawski, K.; Niemczyk, K.; Marchel, A. Strategy for the surgical treatment of vestibular schwannomas in patients with neurofibromatosis type 2. Neurol. Neurochir. Pol. 2015, 49, 295–301. [Google Scholar] [CrossRef]
- Slattery, W.H. Neurofibromatosis 2. Otolaryngol. Clin. N. Am. 2012, 45, 315–332. [Google Scholar] [CrossRef]
- Zhao, F.; Wang, B.; Yang, Z.; Zhou, Q.; Li, P.; Wang, X.; Zhang, J.; Zhang, J.; Liu, P. Surgical treatment of large vestibular schwannomas in patients with neurofibromatosis type 2: Outcomes on facial nerve function and hearing preservation. J. Neurooncol. 2018, 138, 417–424. [Google Scholar] [CrossRef]
- MacNally, S.P.; Rutherford, S.A.; King, A.T.; Freeman, S.; Thorne, J.; Mawman, D.; O'Driscoll, M.P.; Evans, D.G.; Ramsden, R.T. Outcome from surgery for vestibular schwannomas in children. Br. J. Neurosurg. 2009, 23, 226–231. [Google Scholar] [CrossRef]
- Kim, B.S.; Seol, H.J.; Lee, J.I.; Shin, H.J.; Park, K.; Kong, D.S.; Nam, D.H.; Cho, Y.S. Clinical outcome of neurofibromatosis type 2-related vestibular schwannoma: treatment strategies and challenges. Neurosurg. Rev. 2016, 39, 643–653. [Google Scholar] [CrossRef]
- Behr, R.; Colletti, V.; Matthies, C.; Morita, A.; Nakatomi, H.; Dominique, L.; Darrouzet, V.; Brill, S.; Shehata-Dieler, W.; Lorens, A.; et al. New outcomes with auditory brainstem implants in NF2 patients. Otol. Neurotol. 2014, 35, 1844–1851. [Google Scholar] [CrossRef] [PubMed]
- Peng, K.A.; Lorenz, M.B.; Otto, S.R.; Brackmann, D.E.; Wilkinson, E.P. Cochlear implantation and auditory brainstem implantation in neurofibromatosis type 2. Laryngoscope 2018, 128, 2163–2169. [Google Scholar] [CrossRef] [PubMed]
- Moffat, D.; Lloyd, S.; Macfarlane, R.; Mannion, R.; King, A.; Rutherford, S.; Axon, P.; Donnelly, N.; Freeman, S.; Tysome, J.R.; et al. Outcome of translabyrinthine surgery for vestibular schwannoma in neurofibromatosis type 2. Br. J. Neurosurg. 2013, 27, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Jia, H.; El El Sayed, M.; Smail, M.; Mosnier, I.; Wu, H.; Sterkers, O.; Kalamarides, M.; Bernardeschi, D.J.N. Neurofibromatosis type 2: Hearing preservation and rehabilitation. Neurochirurgie 2018, 64, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Hudgins, W.R.; Barker, J.L.; Schwartz, D.E.; Nichols, T.D. Gamma Knife Treatment of 100 Consecutive Meningiomas. Stereotact. Funct. Neurosurg. 1996, 66, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Lunsford, L.D.; Douglas, K.; John, C.F.; David, J.B.; Charles, A.J.; Ann, H.M.; Joseph, A.H.; Robert, J.C. Stereotactic radiosurgery for arteriovenous malformations of the brain. J. Neurosurg. 1991, 75, 512–524. [Google Scholar] [CrossRef] [Green Version]
- Chin, L.S.; Regine, W.F. Principles and Practice of Stereotactic Radiosurgery; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2010. [Google Scholar]
- Owen, H.; Holder, D.; Alonso, J.; Mackay, R. Technologies for delivery of proton and ion beams for radiotherapy. Int. J. Mod. Phys. A 2014, 29, 1441002. [Google Scholar] [CrossRef]
- Leksell, L. A note on the treatment of acoustic tumours. Acta Chir. Scand. 1971, 137, 763–765. [Google Scholar]
- Tsao, M.N.; Sahgal, A.; Xu, W.; De Salles, A.; Hayashi, M.; Levivier, M.; Ma, L.; Martinez, R.; Régis, J.; Ryu, S.; et al. Stereotactic radiosurgery for vestibular schwannoma: international stereotactic radiosurgery society (ISRS) practice guideline. J. Radiosurg. SBRT 2017, 5, 5–24. [Google Scholar]
- Gilkes, C.E.; Evans, D.G. Review of radiation therapy services for neurofibromatosis (NF2) patients in England. Br. J. Neurosurg. 2014, 28, 16–19. [Google Scholar] [CrossRef]
- Rowe, J.G.; Radatz, M.; Walton, L.; Kemeny, A.A. Stereotactic radiosurgery for type 2 neurofibromatosis acoustic neuromas: patient selection and tumour size. Stereotact. Func.t Neurosurg. 2002, 79, 107–116. [Google Scholar] [CrossRef]
- Mathieu, D.; Kondziolka, D.; Flickinger, J.C.; Niranjan, A.; Williamson, R.; Martin, J.J.; Lunsford, L.D. Stereotactic radiosurgery for vestibular schwannomas in patients with neurofibromatosis type 2: an analysis of tumor control, complications, and hearing preservation rates. Neurosurgery 2007, 60, 460–468. [Google Scholar] [CrossRef] [PubMed]
- Meijer, O.W.; Vandertop, W.P.; Lagerwaard, F.J.; Slotman, B.J. Linear accelerator-based stereotactic radiosurgery for bilateral vestibular schwannomas in patients with neurofibromatosis type 2. Neurosurgery 2008, 62, A37–A42. [Google Scholar] [CrossRef] [PubMed]
- Phi, J.H.; Kim, D.G.; Chung, H.T.; Lee, J.; Paek, S.H.; Jung, H.W. Radiosurgical treatment of vestibular schwannomas in patients with neurofibromatosis type 2: Tumor control and hearing preservation. Cancer 2009, 115, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Chung, L.K.; Nguyen, T.P.; Sheppard, J.P.; Lagman, C.; Tenn, S.; Lee, P.; Kaprealian, T.; Chin, R.; Gopen, Q.; Yang, I. A Systematic review of radiosurgery versus surgery for neurofibromatosis type 2 vestibular schwannomas. World Neurosurg. 2018, 109, 47–58. [Google Scholar] [CrossRef]
- Wolbers, J.G.; Dallenga, A.H.; Mendez Romero, A.; van Linge, A. What intervention is best practice for vestibular schwannomas? A systematic review of controlled studies. BMJ 2013, 3. [Google Scholar] [CrossRef] [Green Version]
- Golfinos, J.G.; Hill, T.C.; Rokosh, R.; Choudhry, O.; Shinseki, M.; Mansouri, A.; Friedmann, D.R.; Thomas Roland, J., Jr.; Kondziolka, D. A matched cohort comparison of clinical outcomes following microsurgical resection or stereotactic radiosurgery for patients with small—And medium-sized vestibular schwannomas. J. Neurosurg. 2016, 125, 1472–1482. [Google Scholar] [CrossRef] [Green Version]
- Carlson, M.L.; Vivas, E.X.; McCracken, D.J.; Sweeney, A.D.; Neff, B.A.; Shepard, N.T.; Olson, J.J. Congress of neurological surgeons systematic review and evidence-based guidelines on hearing preservation outcomes in patients with sporadic vestibular schwannomas. Neurosurgery 2018, 82, e35–e39. [Google Scholar] [CrossRef] [Green Version]
- Langenberg, R.v.d.; Hanssens, P.E.J.; Verheul, J.B.; Overbeeke, J.J.v.; Nelemans, P.J.; Dohmen, A.J.C.; Bondt, B.J.d.; Stokroos, R.J. Management of large vestibular schwannoma. Part II. primary gamma knife surgery: radiological and clinical aspects. J. Neurosurg. 2011, 115, 885. [Google Scholar] [CrossRef]
- Bailo, M.; Boari, N.; Franzin, A.; Gagliardi, F.; Spina, A.; Del Vecchio, A.; Gemma, M.; Bolognesi, A.; Mortini, P. Gamma knife radiosurgery as primary treatment for large vestibular schwannomas: Clinical results at long-term follow-up in a series of 59 patients. World Neurosurg. 2016, 95, 487–501. [Google Scholar] [CrossRef]
- Lefranc, M.; Da Roz, L.M.; Balossier, A.; Thomassin, J.M.; Roche, P.H.; Regis, J. Place of gamma knife stereotactic radiosurgery in grade 4 vestibular schwannoma based on case series of 86 patients with long-term follow-up. World Neurosurg. 2018, 114, e1192–e1198. [Google Scholar] [CrossRef]
- Valentino, V.; Raimondi, A.J. Tumour response and morphological changes of acoustic neurinomas after radiosurgery. Acta Neurochir. 1995, 133, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Vakilian, S.; Souhami, L.; Melançon, D.; Zeitouni, A. Volumetric measurement of vestibular schwannoma tumour growth following partial resection: predictors for recurrence. J. Neurol. Surg. B Skul.l Base 2012, 73, 117–120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van De Langenberg, R.; Hanssens, P.E.J.; Van Overbeeke, J.J.; Verheul, J.B.; Nelemans, P.J.; De Bondt, B.J.; Stokroos, R.J. Management of large vestibular schwannoma. Part I. Planned subtotal resection followed by gamma knife surgery: Radiological and clinical aspects—Clinical article. J. Neurosurg. 2011, 115, 875–884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brokinkel, B.; Sauerland, C.; Holling, M.; Ewelt, C.; Horstmann, G.; van Eck, A.T.C.J.; Stummer, W. Gamma Knife radiosurgery following subtotal resection of vestibular schwannoma. J. Clin. Neurosci. 2014, 21, 2077–2082. [Google Scholar] [CrossRef]
- Iwai, Y.; Ishibashi, K.; Watanabe, Y.; Uemura, G.; Yamanaka, K. Functional preservation after planned partial resection followed by gamma knife radiosurgery for large vestibular schwannomas. World Neurosurg. 2015, 84, 292–300. [Google Scholar] [CrossRef]
- Iwai, Y.; Yamanaka, K.; Ishiguro, T. Surgery combined with radiosurgery of large acoustic neuromas. Surg. Neurol. 2003, 59, 283–289. [Google Scholar] [CrossRef]
- Park, C.K.; Jung, H.W.; Kim, J.E.; Son, Y.J.; Paek, S.H.; Kim, D.G. Therapeutic strategy for large vestibular schwannomas. J. Neurooncol. 2006, 77, 167–171. [Google Scholar] [CrossRef]
- Yang, S.-Y.; Kim, D.G.; Chung, H.-T.; Park, S.-H.; Paek, S.H.; Jung, H.-W. Evaluation of tumor response after gamma knife radiosurgery for residual vestibular schwannomas based on MRI morphological features. J. Neurol. Neurosurg. Psychiatry 2007. [Google Scholar] [CrossRef]
- Fuentes, S.; Arkha, Y.; Pech-Gourg, G.; Grisoli, F.; Dufour, H.; Regis, J. Management of large vestibular schwannomas by combined surgical resection and gamma knife radiosurgery. Prog. Neurol. Surg. 2008, 21, 79–82. [Google Scholar] [CrossRef]
- Pan, H.C.; Sheehan, J.; Sheu, M.L.; Chiu, W.T.; Yang, D.Y. Intracapsular decompression or radical resection followed by Gamma Knife surgery for patients harboring a large vestibular schwannoma. J. Neurosurg. 2012, 117, 69–77. [Google Scholar] [CrossRef] [Green Version]
- Daniel, R.T.; Tuleasca, C.; George, M.; Pralong, E.; Schiappacasse, L.; Zeverino, M.; Maire, R.; Levivier, M. Preserving normal facial nerve function and improving hearing outcome in large vestibular schwannomas with a combined approach: Planned subtotal resection followed by gamma knife radiosurgery. Acta Neurochir. 2017, 159, 1197–1211. [Google Scholar] [CrossRef] [PubMed]
- Andrews, D.W.; Suarez, O.; Goldman, H.W.; Downes, M.B.; Bednarz, G.; Corn, B.W.; Werner-Wasik, M.; Rosenstock, J.; Curran, W.J. Stereotactic radiosurgery and fractionated stereotactic radiotherapy for the treatment of acoustic schwannomas: Comparative observations of 125 patients treated at one institution. Int. J. Radiat. Oncol. Biol. Phys. 2001, 50, 1265–1278. [Google Scholar] [CrossRef]
- Chin, L.S.; Ma, L.; DiBiase, S. Radiation necrosis following gamma knife surgery: A case-controlled comparison of treatment parameters and long-term clinical follow up. J. Neurosurg. 2001, 94, 899–904. [Google Scholar] [CrossRef]
- Kim, J.H.; Jung, H.H.; Chang, J.H.; Chang, J.W.; Park, Y.G.; Chang, W.S. Predictive factors of unfavorable events after gamma knife radiosurgery for vestibular schwannoma. World Neurosurg. 2017, 107, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Kurita, H.; Sugasawa, K.; Mizuno, M.; Sasaki, T. Analyses of neuro-otological complications after radiosurgery for acoustic neurinomas. Int. J. Radiat. Oncol. Biol. Phys. 1997, 39, 983–988. [Google Scholar] [CrossRef]
- Shin, M.; Ueki, K.; Kurita, H.; Kirino, T. Malignant transformation of a vestibular schwannoma after gamma knife radiosurgery. Lancet 2002, 360, 309–310. [Google Scholar] [CrossRef]
- Carlson, M.L.; Babovic-Vuksanovic, D.; Messiaen, L.; Scheithauer, B.W.; Neff, B.A.; Link, M.J. Radiation-induced rhabdomyosarcoma of the brainstem in a patient with neurofibromatosis type 2. J. Neurosurg. 2010, 112, 81–87. [Google Scholar] [CrossRef] [Green Version]
- Evans, D.G.R.; Baser, M.E.; O'Reilly, B.; Rowe, J.; Gleeson, M.; Saeed, S.; King, A.; Huson, S.M.; Kerr, R.; Thomas, N.; et al. Management of the patient and family with neurofibromatosis 2: a consensus conference statement. Br. J. Neurosurg. 2005, 19, 5–12. [Google Scholar] [CrossRef]
- Cahan, W.G.; Woodard, H.Q.; Higinbotham, N.L.; Stewart, F.W.; Coley, B.L. Sarcoma in irradiated bone. Report of eleven cases. Cancer 1948, 1, 3–29. [Google Scholar] [CrossRef]
- Patel, T.R.; Chiang, V.L. Secondary neoplasms after stereotactic radiosurgery. World Neurosurg. 2014, 81, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Carlson, M.L.; Glasgow, A.E.; Jacob, J.T.; Habermann, E.B.; Link, M.J. The Short-Term and Intermediate-Term Risk of Second Neoplasms After Diagnosis and Treatment of Unilateral Vestibular Schwannoma: Analysis of 9460 Cases. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 1149–1157. [Google Scholar] [CrossRef]
- Balasubramaniam, A.; Shannon, P.; Hodaie, M.; Laperriere, N.; Michaels, H.; Guha, A. Glioblastoma multiforme after stereotactic radiotherapy for acoustic neuroma: case report and review of the literature. Neuro. Oncol. 2007, 9, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Rowe, J.; Grainger, A.; Walton, L.; Radatz, M.; Kemeny, A. Safety of radiosurgery applied to conditions with abnormal tumor suppressor genes. Neurosurg. 2007, 60, 860–864. [Google Scholar] [CrossRef] [PubMed]
- Tripathi, M.; Deora, H.; Kumar, N.; Batish, A.; Dutta, P.; Gurnani, J.; Mohindra, S.; Hussain Shahid, A.; Kataria, K.; Agrahari, A.; et al. Role of Bevacizumab as a prophylactic and rehabilitative treatment modality in cases of sporadic and syndromic vestibular schwannoma: Fifty shades of grey! Interdiscip. Neurosurg. 2020, 19, 100607. [Google Scholar] [CrossRef]
- Plotkin, S.R.; Stemmer-Rachamimov, A.O.; Barker, F.G.; Halpin, C.; Padera, T.P.; Tyrrell, A.; Sorensen, A.G.; Jain, R.K.; di Tomaso, E. Hearing Improvement after Bevacizumab in Patients with Neurofibromatosis Type 2. N. Engl. J. Med. 2009, 361, 358–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mautner, V.-F.; Nguyen, R.; Kutta, H.; Fuensterer, C.; Bokemeyer, C.; Hagel, C.; Friedrich, R.E.; Panse, J. Bevacizumab induces regression of vestibular schwannomas in patients with neurofibromatosis type 2†. Neuro. Oncol. 2009, 12, 14–18. [Google Scholar] [CrossRef] [Green Version]
- Eminowicz, G.K.; Raman, R.; Conibear, J.; Plowman, P.N. Bevacizumab treatment for vestibular schwannomas in neurofibromatosis type two: Report of two cases, including responses after prior gamma knife and vascular endothelial growth factor inhibition therapy. J. Laryngol. Otol. 2012, 126, 79–82. [Google Scholar] [CrossRef]
- Subbiah, V.; Slopis, J.; Hong, D.S.; Ketonen, L.M.; Hamilton, J.; McCutcheon, I.E.; Kurzrock, R. Treatment of patients with advanced neurofibromatosis type 2 with novel molecularly targeted therapies: from bench to bedside. J. Clin. Oncol. 2012, 30, e64–e68. [Google Scholar] [CrossRef]
- Van Gompel, J.J.; Agazzi, S.; Carlson, M.L.; Adewumi, D.A.; Hadjipanayis, C.G.; Uhm, J.H.; Olson, J.J. Congress of Neurological Surgeons Systematic Review and Evidence-Based Guidelines on Emerging Therapies for the Treatment of Patients With Vestibular Schwannomas. Neurosurgery 2017, 82, E52–E54. [Google Scholar] [CrossRef] [Green Version]
- Lu, V.M.; Ravindran, K.; Graffeo, C.S.; Perry, A.; Van Gompel, J.J.; Daniels, D.J.; Link, M.J. Efficacy and safety of bevacizumab for vestibular schwannoma in neurofibromatosis type 2: a systematic review and meta-analysis of treatment outcomes. J. Neuro. Oncol. 2019, 144, 239–248. [Google Scholar] [CrossRef]
- Miller, C.; Sudhoff, H.; Jacob, A. Vestibular Schwannoma Drug Development: Current State-of-the Art. Curr. Otorhinolaryngol. Rep. 2014, 2, 217–225. [Google Scholar] [CrossRef] [Green Version]
- James, M.F.; Han, S.; Polizzano, C.; Plotkin, S.R.; Manning, B.D.; Stemmer-Rachamimov, A.O.; Gusella, J.F.; Ramesh, V. NF2/Merlin Is a Novel Negative Regulator of mTOR Complex 1, and Activation of mTORC1 Is Associated with Meningioma and Schwannoma Growth. Mol. Cell. Biol. 2009, 29, 4250–4261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curto, M.; Cole, B.K.; Lallemand, D.; Liu, C.-H.; McClatchey, A.I. Contact-dependent inhibition of EGFR signaling by Nf2/Merlin. J. Cell. Biol. 2007, 177, 893–903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goutagny, S.; Raymond, E.; Esposito-Farese, M.; Trunet, S.; Mawrin, C.; Bernardeschi, D.; Larroque, B.; Sterkers, O.; Giovannini, M.; Kalamarides, M. Phase II study of mTORC1 inhibition by everolimus in neurofibromatosis type 2 patients with growing vestibular schwannomas. Neuro. Oncol. 2015, 122, 313–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sagers, J.E.; Beauchamp, R.L.; Zhang, Y.; Vasilijic, S.; Wu, L.; DeSouza, P.; Seist, R.; Zhou, W.; Xu, L.; Ramesh, V.; et al. Combination therapy with mTOR kinase inhibitor and dasatinib as a novel therapeutic strategy for vestibular schwannoma. Sci. Rep. 2020, 10, 4211. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Sporadic VS | NF2 VS |
|---|---|---|
| Mutation in the NF2 gene | 60% | 90% |
| Common type of mutation | Point mutations and small deletions | Truncating mutations |
| The “hit”hypothesis | One hit, two hits | One hit, two hits, four hits |
| Family history | No | Approximately 50% of individuals with NF2 have an affected parent |
| Tumor location | Unilateral | Bilateral |
| New cases | 95% | 5% |
| Concomitant tumors | No | Meningiomas, astrocytomas and ependymomas |
| Standard diagnosis technology | MRI | MRI |
| Age of onset | Middle-age | Childhood |
| The preferred management | medium- or small-sized: wait and scan, radiotherapy and/or surgery large size: surgery | medium- or small-sized: wait and scan, radiotherapy and/or surgery large size: surgery |
| Ophthalmological lesions | No | Cataracts, epiretinal membranes, retinal hamartomas |
| Cutaneous lesions | No | Skin tumors, skin plaques, subcutaneous tumors |
| Author | Patient Number | Tumor Diameter OR Volume Before Surgery | Tumor Diameter OR Volume After Surgery | RS Type | Prescribed Dose | Interval between S and RS (Months) | Follow Up (Months) | Control Rate | Regrowth | Time to Manifestation (Months) | RS Side Effect | FN Function (Preservation) | Hearing Function (Preservation) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Iawi Y Yamanaka, and Ishiguro (2003) | 14 | Diameter ≥ 30 mm | Mean diameters = 18.9 mm (9.8–36.1 mm) | GK | Mean = 12.1 Gy (10 - 14.1 Gy) | 1–6 months (mean = 2.9 months) | Mean = 32 months (12–72 months) | 79% | 3 (2 with NF2 and 1 with extra-large VS | 1NM | No complications | 85.70% | Among 3 patients with useful hearing (with G&R Class 1 and 2 preoperatively), postoperatively useful hearing was preserved in only 1 patient. |
| Park et al.(2006) | 8 | Volume ≥ 3 cm3 | Mean volume = 4.6 cm3 | GK | Mean = 12 Gy | 1 Week- 6 months | 68.8 | 100% | 0 | NM | No complications | 31 patients underwent R-STR and 8 of them received GK. The overall FN preservation rate = 87% | NM |
| Yang et al. (2007) | 61 | Mean volume = 20.6 ± 11.1 mL (range: 18–67) | Mean volume = 3.68 mL (range: 0.52–15.50 mL) | GK | Marginal doses 9–14 Gy (mean: 12.5 GY) | Median = 5.8 months | After KG, median follow up = 53.7 months (range 24.1–102.2) | The 4- and 8-year actuarial tumor control rates were 96.5% ± 2.4% and 93.5% ± 3.7%, respectively | 3 patients | Within 4 years after GK | No complications | 95% | Before surgery, only 10 out of 61 patients had serviceable hearing (grade 1 and 2). After surgery, 5 out of 10 had serviceable hearing. At the last follow up and after GK, 3 of the 5 patients had serviceable hearing (30% : 3/10) |
| Fuentes et al. (2008) | 8 | Mean diameter = 40 mm (35–45) | Mean volume = 1.16 cm3 (0.3 - 2.2 cm3) | GK | The mean peripheral dose = 11.8 Gy (range: 11–13 Gy). Mean dose to the tumor center = 23.75 GY (22–26 Gy). | Mean = 9 months (6–12 months) | Mean follow-up time after the GK = 46 (range: 12–73) months. | 100% | 0 | NM | No complications | 87.5% | NM |
| Van De Langenberg et al. (2011) | 50 | Mean volume = 14.9 cm3 (4.1–36.1) | Mean volume = 3.34 cm3 (0.22–11.8 cm3) | GK | Mean dose prescribed to the isodose covering 90% of the tumor = 12.9 Gy (12 - 13). Mean maximum dose = 21.1 Gy (18–26). The mean tumor margin dose = 11 Gy (9.4 - 11.9). | Mean = 8.5 (2 - 24) | Median = 33.8 (12 - 84) | Clinical tumor control = 92%, radiological tumor control = 90% | 4 | Mean = 31.5 months ( 22–49) | HB Grade II transient facial paresis developed in 2 patients. One patient developed transient trigeminal hypesthesia. One patient experienced persisting FN spasms. | 94% | Before surgery: All patients reported hearing loss, and only 4 (8%) of the 50 patients presented with serviceable hearing, all Class B. |
| Pan et al. (2012) | 18 | Mean volume = 17.5 cm3 | Mean volume = 9.35 cm3 | GK | 12 Gy | Mean = 3.6 | Mean = 57.7 (at least 3 years) | 100% | 0 | NM | 1 patient had transient hearing loss following GK. | 89% | 100%/Before surgery, 11 patients had serviceable hearing and all were preserved. |
| Iwai et al. (2015) | 40 | Median diameter = 18.6 mm (9.1–27.1) | Median volume = 3.3 cm3 (0.4–10.4) | GK | Median dose = 12 Gy (10–12 Gy) | Median = 3 (1–12) | Median = 65 (18–156) | At 3 years = 92%, at 5 years = 86%, at 10 years = 86% | 4 | After 12, 27, 34 and 40 months | • 2 patients suffered transient facial spasms. • 2 patients experienced transient trigeminal neuropathy | 95% | Before surgery: 29 patients had some hearing preservation. At the last follow-up: 42.9% (6/14) preserved their hearing |
| Daniel et al. (2017) | 32 | Mean volume = 12.5 cm3 | Mean volume = 3.5 cm3 | GK | Mean dose = 12 Gy | Mean = 6.3 | Mean = 29 | 91.6% | 3 | After 2.6, 2 and 1.2 years | No complications | 100% | Before surgery: 13 had normal hearing, After treatment 10 preserved hearing functions 76.9% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yao, L.; Alahmari, M.; Temel, Y.; Hovinga, K. Therapy of Sporadic and NF2-Related Vestibular Schwannoma. Cancers 2020, 12, 835. https://doi.org/10.3390/cancers12040835
Yao L, Alahmari M, Temel Y, Hovinga K. Therapy of Sporadic and NF2-Related Vestibular Schwannoma. Cancers. 2020; 12(4):835. https://doi.org/10.3390/cancers12040835
Chicago/Turabian StyleYao, Longping, Mohammed Alahmari, Yasin Temel, and Koos Hovinga. 2020. "Therapy of Sporadic and NF2-Related Vestibular Schwannoma" Cancers 12, no. 4: 835. https://doi.org/10.3390/cancers12040835
APA StyleYao, L., Alahmari, M., Temel, Y., & Hovinga, K. (2020). Therapy of Sporadic and NF2-Related Vestibular Schwannoma. Cancers, 12(4), 835. https://doi.org/10.3390/cancers12040835