Hyperthermic Intraperitoneal Chemotherapy for Primary or Recurrent Adrenocortical Carcinoma. A Single Center Study

 ,
,  , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Chemotherapy
2.2. Surgical Technique
2.3. HIPEC
2.4. Outcome
2.5. Statistics
3. Results
3.1. Surgery for Primary
3.2. Surgery for Recurrence
4. Discussion
4.1. Safety Considerations
4.2. HIPEC in the Prophylactic and Therapeutic Setting
4.3. Survival Performances
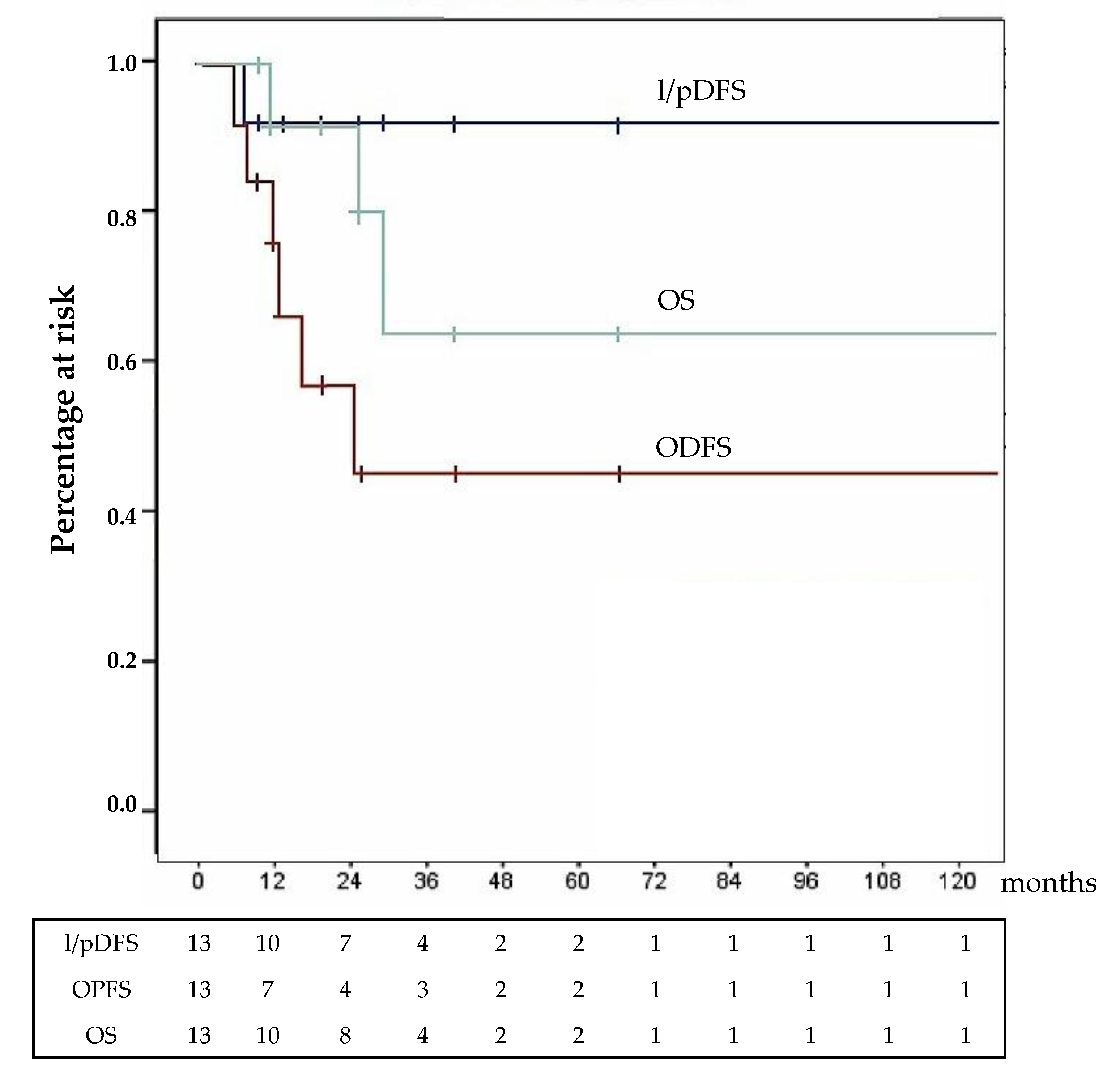
4.3.1. Surgery for Primary
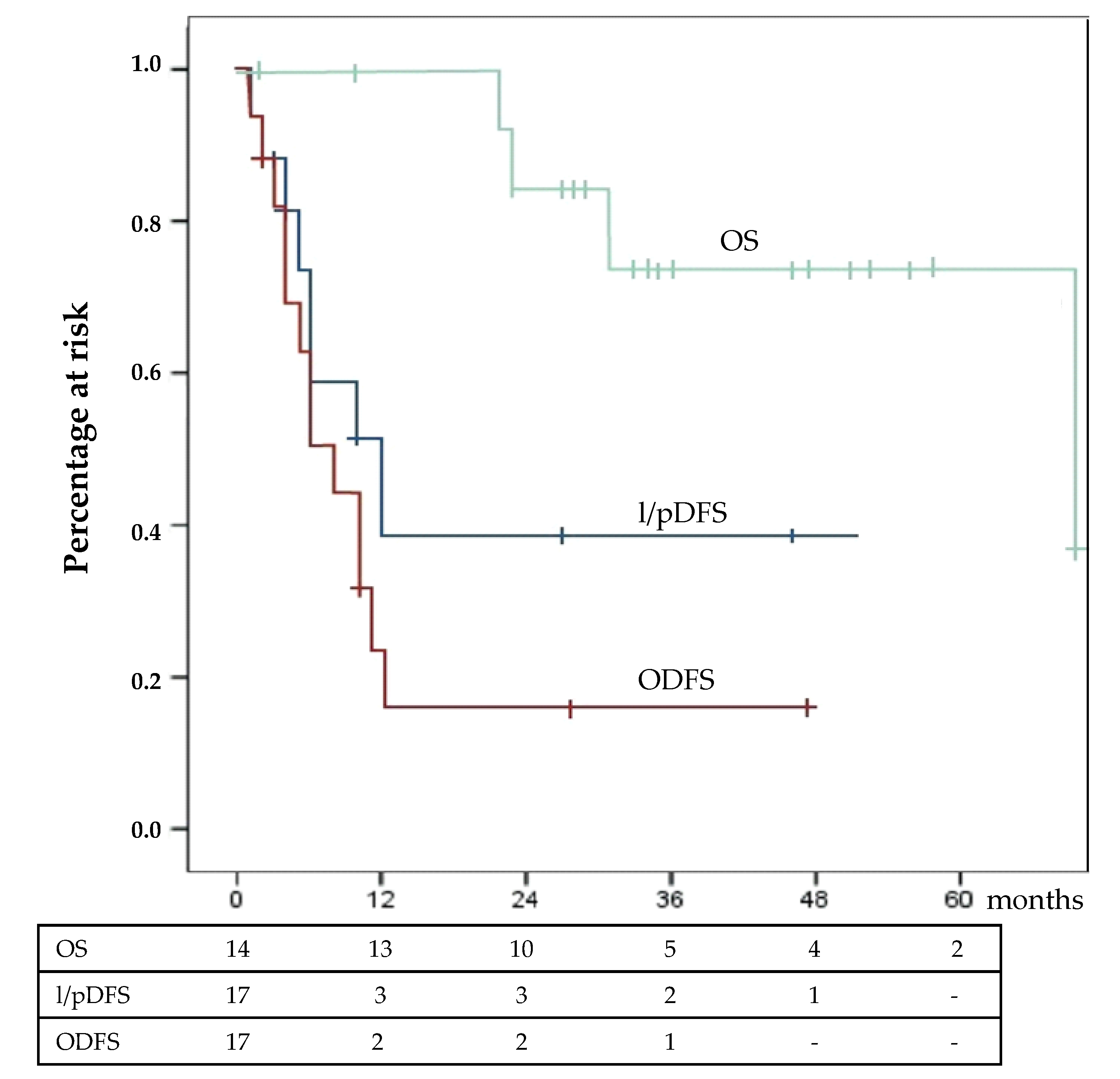
4.3.2. Surgery for Recurrence
4.4. Limits of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fassnacht, M.; Dekkers, O.M.; Else, T.; Baudin, E.; Berruti, A.; De Krijger, R.R.; Haak, H.R.; Mihai, R.; Assie, G.; Terzolo, M. European Society of Endocrinology Clinical Practice Guidelines on the management of adrenocortical carcinoma in adults, in collaboration with the European Network for the Study of Adrenal Tumors. Eur. J. Endocrinol. 2018, 179, G1–G46. [Google Scholar] [CrossRef] [PubMed]
- Glenn, J.A.; Else, T.; Hughes, D.T.; Cohen, M.S.; Jolly, S.; Giordano, T.; Worden, F.P.; Gauger, P.G.; Hammer, G.D.; Miller, B.S. Longitudinal patterns of recurrence in patients with adrenocortical carcinoma. Surgery 2019, 165, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Sidhu, S.; Glover, A.; Ip, J.C.Y.; Zhao, J.T.; Soon, P.S.H.; Robinson, B.G. Current management options for recurrent adrenocortical carcinoma. OncoTargets Ther. 2013, 6, 635–643. [Google Scholar] [CrossRef] [PubMed]
- Bilimoria, K.Y.; Shen, W.T.; Elaraj, D.; Bentrem, D.J.; Winchester, D.J.; Kebebew, E.; Sturgeon, C. Adrenocortical carcinoma in the United States. Cancer 2008, 113, 3130–3136. [Google Scholar] [CrossRef] [PubMed]
- Bellantone, R.; Ferrante, A.M.R.; Boscherini, M.; Lombardi, C.P.; Crucitti, P.; Crucitti, F.; Favia, G.; Borrelli, D.; Boffi, L.; Capussotti, L.; et al. Role of reoperation in recurrence of adrenal cortical carcinoma: Results from 188 cases collected in the Italian National Registry for Adrenal Cortical Carcinoma. Surgery 1997, 122, 1212–1218. [Google Scholar] [CrossRef]
- Schulick, R.D.; Brennan, M. Long-term survival after complete resection and repeat resection in patients with adrenocortical carcinoma. Ann. Surg. Oncol. 1999, 6, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Gaujoux, S.; Al-Ahmadie, H.; Allen, P.J.; Gonen, M.; Shia, J.; D’Angelica, M.; DeMatteo, R.; Fong, Y.; Blumgart, L.; Jarnagin, W.R. Resection of Adrenocortical Carcinoma Liver Metastasis: Is it Justified? Ann. Surg. Oncol. 2012, 19, 2643–2651. [Google Scholar] [CrossRef] [PubMed]
- Prendergast, K.M.; Smith, P.M.; Tran, T.B.; Postlewait, L.M.; Maithel, S.K.; Prescott, J.D.; Pawlik, T.M.; Wang, T.S.; Glenn, J.; Hatzaras, I.; et al. Features of synchronous versus metachronous metastasectomy in adrenal cortical carcinoma: Analysis from the US adrenocortical carcinoma database. Surgery 2020, 167, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Di Giorgio, A.; Pinto, E. Treatment of Peritoneal Surface Malignancies: State of the Art and Perspectives; Springer: Milano, Italia, 2015; ISSN 2280-9848. ISBN 978-88-470-5710-4. e-ISBN: 978-88-470-5711-1 (eBook). [Google Scholar]
- Fassnacht, M.; Allolio, B. Reply to Limited prognostic value of the 2004 International Union Against Cancer staging classification for adrenocortical carcinoma. Cancer 2009, 115, 5848. [Google Scholar] [CrossRef]
- Reibetanz, J.; Rinn, B.; Kunz, A.S.; Flemming, S.; Ronchi, C.L.; Kroiss, M.; Deutschbein, T.; Pulzer, A.; Hahner, S.; Kocot, A.; et al. Patterns of Lymph Node Recurrence in Adrenocortical Carcinoma: Possible Implications for Primary Surgical Treatment. Ann. Surg. Oncol. 2018, 26, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Ihemelandu, C.U.; Mcquellon, R.; Shen, P.; Stewart, J.H.; Votanopoulos, K.; Levine, E.A. Predicting Postoperative Morbidity Following Cytoreductive Surgery with Hyperthermic Intraperitoneal Chemotherapy (CS+HIPEC) with Preoperative FACT-C (Functional Assessment of Cancer Therapy) and Patient-Rated Performance Status. Ann. Surg. Oncol. 2013, 20, 3519–3526. [Google Scholar] [CrossRef] [PubMed]
- Gusani, N.J.; Cho, S.W.; Colovos, C.; Seo, S.; Franko, J.; Richard, S.D.; Edwards, R.P.; Brown, C.K.; Holtzman, M.P.; Zeh, H.J.; et al. Aggressive Surgical Management of Peritoneal Carcinomatosis with Low Mortality in a High-Volume Tertiary Cancer Center. Ann. Surg. Oncol. 2007, 15, 754–763. [Google Scholar] [CrossRef] [PubMed]
- Sugarbaker, P.H. Peritoneal Metastases from Adrenal Cortical Carcinoma Treated by Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy. Tumori J. 2016, 102, 588–592. [Google Scholar] [CrossRef] [PubMed]
- Glehen, O.; Gilly, F.N.; Boutitie, F.; Bereder, J.M.; Quenet, F.; Sideris, L.; Mansvelt, B.; Lorimier, G.; Msika, S.; Elias, M. Toward curative treatment of peritoneal carcinomatosis from nonovarian origin by cytoreductive surgery combined with perioperative intraperitoneal chemotherapy. Cancer 2010, 116, 5608–5618. [Google Scholar] [CrossRef] [PubMed]
- Hughes, M.S.; Lo, W.M.; Beresnev, T.; Merino, M.; Shutack, Y.; Ripley, R.T.; Hernandez, J.M.; Davis, J.L. A Phase II Trial of Cytoreduction and Hyperthermic Intraperitoneal Chemotherapy for Recurrent Adrenocortical Carcinoma. J. Surg. Res. 2018, 232, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Dy, B.M.; Wise, K.B.; Richards, M.L.; Young, W.F.; Grant, C.S.; Bible, K.C.; Rosedahl, J.; Harmsen, W.S.; Farley, D.R.; Thompson, S.M. Operative intervention for recurrent adrenocortical cancer. Surgery 2013, 154, 1292–1299. [Google Scholar] [CrossRef] [PubMed]
- Erdogan, I.; Deutschbein, T.; Jurowich, C.; Kroiss, M.; Ronchi, C.L.; Quinkler, P.D.M.M.; Waldmann, J.; Willenberg, P.D.M.H.S.; Beuschlein, F.; Fottner, C.; et al. The Role of Surgery in the Management of Recurrent Adrenocortical Carcinoma. J. Clin. Endocrinol. Metab. 2013, 98, 181–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Datrice, N.M.; Langan, R.C.; Ripley, R.T.; Kemp, C.D.; Steinberg, S.M.; Wood, B.J.; Libutti, S.K.; Fojo, T.; Schrump, D.S.; Avital, I. Operative management for recurrent and metastatic adrenocortical carcinoma. J. Surg. Oncol. 2011, 105, 709–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, T.B.; Maithel, S.K.; Pawlik, T.M.; Wang, T.S.; Hatzaras, I.; Phay, J.E.; Fields, R.C.; Weber, S.M.; Sicklick, J.K.; Yopp, A.C.; et al. Clinical Score Predicting Long-Term Survival after Repeat Resection for Recurrent Adrenocortical Carcinoma. J. Am. Coll. Surg. 2016, 223, 794–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, A.; Habra, M.A.; Grubbs, E.G.; Bednarski, B.K.; Ying, A.; Perrier, N.D.; Lee, J.E.; Aloia, T.A. Does laparoscopic adrenalectomy jeopardize oncologic outcomes for patients with adrenocortical carcinoma? Surg. Endosc. 2013, 27, 4026–4032. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Measure |
|---|---|
| ECOG: | |
| 0 | 10 |
| 1 | 2 |
| 2 | 1 |
| ASA score: | 8 |
| 2 | |
| 3 | 4 |
| 4 | 1 |
| Right/Left adrenal tumor | 2/11 |
| Hyperfunction: | 4 |
| cortisol | |
| androgen | 2 |
| cortisol and androgen | 1 |
| Tumor diameter (cm, median ± SD) | 10.5 ± 7.1 |
| Ensat stage: | 3 |
| II | |
| III | 3 |
| IV | 7 |
| Positive regional nodes (pts) | 3 |
| Variable | Measure |
|---|---|
| Neoadjuvant CHT | 9 (69%) |
| Duration of surgery | 410’ (325’–630’) |
| Associated resections: | 9 (69%) |
| Kidney/Spleen/Colon/Liver | 7/2/1/1 |
| Abdominal R0 resection | 13 (100%) |
| Intraop. blood transfusion | 5 (38%) |
| Units: median (range) | 2 (2–4) |
| Postop. blood transfusion | 6 (46%) |
| Units: median (range) | 4 (2–54) |
| Postop. 90 days mortality | 0 (0 %) |
| Postop. morbidity | 6 (46%) |
| Grade 2:3 (23%) | Anemia: 3 |
| Pancreatic fistula: 1 | |
| Grade 3a: 2 (15%) | Pleural effusion: 2 |
| Pancreatic fistula: 1 | |
| Grade 4b: 1 (8%) | Septic shock Haemoperitoneum |
| Postop. relief of hyperfunction | 7/7 (100%) |
| Hospital stay | 14 days (7–109) |
| Adjuvant Mitotane | 11/13 (84%) |
| Variables | Measure |
|---|---|
| ECOG: | |
| 0 | 7 |
| 1 | 5 |
| 2 | 2 |
| ASA score: | |
| 2 | 5 |
| 3 | 7 |
| 4 | 2 |
| Recurrence | n = 14 |
| Loco-regional | 8 |
| Loco-regional and peritoneal | 3 |
| Peritoneal | 2 |
| Peritoneal and hepatic | 1 |
| II Recurrence | n = 3 |
| Peritoneal | 2 |
| Loco-regional and peritoneal | 1 |
| Peritoneal Cancer Index: | n = 9 |
| median (range) | 7 (2–9) |
| Variable | Measure |
|---|---|
| Neoadjuvant CHT | 16/17 (94%) |
| Duration of surgery (minutes) | 445’ (288–600) |
| Associated resections | 17/17 (100%) |
| Omentectomy: | 9 |
| Splenectomy: | 7 |
| Cholecystectomy: | 5 |
| Nephrectomy: | 4 |
| Hemicolectomy: | 4 |
| Left Pancreatectomy: | 3 |
| Diaphragm resection: | 3 |
| Appendectomy: | 2 |
| Oophorectomy: | 2 |
| Contra lateral Adrenalectomy: | 2 |
| Hepatectomy: | 1 |
| Intraop. blood transfusion | 6/17 (35%) |
| Units: median (range) | 2 (1–4) |
| R0 resection rate | 14/17 (82%) |
| Postop. blood transfusion | 9/17 (53%) |
| Units: median (range) | 2 (2–4) |
| Postop. 90 days mortality | 0/17 (0 %) |
| Postop. morbidity | 13/17 (77%) |
| Grade 2: 10/17 (59%) | Severe anemia: 6 |
| Pleural effusion: 5 | |
| Pneumonitis: 2 | |
| Pancreatic fistula: 2 | |
| Sepsis: 2 | |
| Ileus: 1 | |
| Grade 3b: 2/17 (12%) | Haemoperitoneum: 2 |
| Grade 4b: 1/17 (6%) | Pancreatic fistula, Septic shock Addison and Guillan–Barré |
| Hospital stay (17 procedures) | 14 days (8–78) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tiberio, G.A.M.; Ferrari, V.; Ballarini, Z.; Casole, G.; Laganà, M.; Gritti, M.; Arici, E.; Grisanti, S.; Nascimbeni, R.; Sigala, S.; et al. Hyperthermic Intraperitoneal Chemotherapy for Primary or Recurrent Adrenocortical Carcinoma. A Single Center Study. Cancers 2020, 12, 969. https://doi.org/10.3390/cancers12040969
Tiberio GAM, Ferrari V, Ballarini Z, Casole G, Laganà M, Gritti M, Arici E, Grisanti S, Nascimbeni R, Sigala S, et al. Hyperthermic Intraperitoneal Chemotherapy for Primary or Recurrent Adrenocortical Carcinoma. A Single Center Study. Cancers. 2020; 12(4):969. https://doi.org/10.3390/cancers12040969
Chicago/Turabian StyleTiberio, Guido Alberto Massimo, Vittorio Ferrari, Zeno Ballarini, Giovanni Casole, Marta Laganà, Michele Gritti, Elisa Arici, Salvatore Grisanti, Riccardo Nascimbeni, Sandra Sigala, and et al. 2020. "Hyperthermic Intraperitoneal Chemotherapy for Primary or Recurrent Adrenocortical Carcinoma. A Single Center Study" Cancers 12, no. 4: 969. https://doi.org/10.3390/cancers12040969
APA StyleTiberio, G. A. M., Ferrari, V., Ballarini, Z., Casole, G., Laganà, M., Gritti, M., Arici, E., Grisanti, S., Nascimbeni, R., Sigala, S., Berruti, A., & Coniglio, A. (2020). Hyperthermic Intraperitoneal Chemotherapy for Primary or Recurrent Adrenocortical Carcinoma. A Single Center Study. Cancers, 12(4), 969. https://doi.org/10.3390/cancers12040969